Vol 9, No 3, July
-
September 2000 Cancer in Cipto Mangunkusumo Hospilal Jakartal8l
Hospital
based
cancer
registry in
Cipto Mangunkusumo hospital Jakarta
Wilfried
Herdin Sibuea', R
Rukmini
Mangunkusumo#,Nurul
Akbar', Abidin
Wi-djanarko', Djajadiman
Gatoy', EndangWindiastuti/, Mochtar
Hamzah*,Sonar
Soni Panigoroo, JoedoPrihartono', Ening
Krisnuhono#, Lisnawati#, SriMulya
SekarUtamiv, Irwan Ramliv,
A
rerdiRoezin*, Sigit
Pribadin,Iik
Wilarsoe,I
Made Nasar#, Santoso Cornain#Abstrak
Règistrasi kanker berbasis rumah sakit di RSUPN Cipto Mangunkusumo, Fakultas Kedokteran Ilniversitas Indonesia, telah dimulai tahun 1997, bertujuan untuk memberi data bagi program pengendalian kanker dan membantu perencanaan rumah sakit. Makalah ini menyajikan registrasi kanker sepanjang tahun 1997-1998. Data
dari
semua pasien kanker yang baru terdiagnosis dicatat padaFormulir
RegistrasiKanker.
Yangdidata
ialah
identitas pasien, demografidan kultur, penilaian tumor dan usia,
serta penatalaksanaan. Terdapat 2144 (0.45%ù penderita kanker diantara 444.178 pasien baru yang berobat ke RSCM. Perbandingan perempuan dan laki-laki adalah 1.7: L
Ilsia terbanyak pada perempuan adalah 35-44 tahun, pada laki-laki 45-54 tahun. Usia rata-rata saat terdiagnosis umumnya lebih muda dibanding senter lainnya. Pada perempuan, kanker terbanyak adalah kçnker servil<s, disusul oleh payudara dan nasofaring sedang pada lakiJaki terbanyak nasofaring, sumsum tulang dan hati. Pada anak, terbanyak adalah leukemia limfositik akut, leukemia non limfositik akut, retinoblastoma dan nefroblastoma. Pendidikan penderita perempuan lebih rendah dibanding laki-laki. Perempuan penderita kanker serviks, kuli!, sumsum tulang, kelenjar getah bening dan laki-laki penderita kanker sumsum tulang, kelenjar getah bening dan mata mempunyai pendidikan yang lebih rendah. Sebanyak 85% diagnosis ditegakkan secara mikroskopik. Jumlah kanker stadium awal lebih rendah dibanding stadium lanjut (47% vs 53%o). Pada tahun 1998terapi awal yang
paling
banyak diberikan adalah berturut-turut radiolerapi, bedah dan kemoterapi. Hanya 45oÀ pasien yang memperoleh terapi dalam 3 bulan perlama setelah diagnosis.Abstract
The Hospital Based Cancer Registry in Registry
in
Cipto Mangunkusumo National Center General Hospital (RSCM), the teaching hospilal ol the Faculty of Medicine University of Indonesia, was set up in I 997. Its aims were to provide information on lhe magnilude of cartcer problems, and data for focussing cancer control programs, to facilitate thefollow
up and to help plan hospital facilities. This paper presents a summary ofthe cancer registry data collected during the period of 1997-1998. Datafrom al newly diagnosed cancer patients was recorded in Cancer Registration Forms by the oncologt doctors. The collected items of information were patient's identification, demographic and cultural items, the tumor and its investigalions, and the treatment. There were 2144 (0.48%o) cancer patients among 444,178 new patients treated in RSCM hospilal. The female to male palientsralio
was 1.7:
1. The age peaked in females within 35-44 years, and in males within 45-54 years. In general, the mean age al diagnosis ofvarious cancer was younger compared to other centers. Infemales, the most common cancers were cervical, breast, and nasophayngeal, and in males, they were nasopharyngeal, bone maruow, and liver cancers. In children, the most common cancers were acute lymphocytic leukemia, acute non-lymphocytic leukemia, acute non-non-lymphocytic leukemia, retinoblastoma, and nephroblastoma. Female patients had lower educational level than males. Females with cervical, skin, bone maruow, lymph nodes cancer and males with bone maruow, lymph nodes and eye malignancy had lower educational level. There were 85oÀpalients
diagnosedby
microscopic examinalion. The number of early slage cancer was lower comed to late stage cases (47o% vs 53%o).In
1998, the mostfrequen! initial treatment was radiotherapy,followed by surgery and chemotherapy, and only 45% patients received treatments within 3 months after diagnosis.Keywords: Cancer registry, site, ape, education, staging, diagnosis, trealmenl
v Department of Radiologt, Faculty of Medicine University of Indonesia,
Jokarta.
Indonesia
The incidence
of
cancer
in
Indonesia
has
been* Departmenrof ENT,Facuttyof Medicine(Jniversityof
Indonesia,
observed
to
increase
every year. According
to
theJakarta,
Indonesia
estimation of
theMinistry of
Health
the incidence rate'o;i,ï:::;',f,fl!;:::';:r:#,fl,T:;:"!:y,;o*
ttvorMedicine
of
cancerwas about
looper
100.000 people-rAs
thet co^put", Sii*ce Center, IJniversity of Indones'a,
Jakarta
people's
awareness
about this dreaded
disease
is'
Department of Internal Medicine, Faculty of Medicine University ofI ndo nes ia, Jakarta, I ndo nes ia
n Department of Anatomic Pathologt, Faculty of Medicine IJniversity of I ndo nes ia, Jaka rta, I ndo nes ia
I
Department of Pediatric, Faculty of Medicine [Jniversity of Indonesia, Jakarla, Indonesia- Department of Dermalologt, Faculty of Medicine University of
I ndo nes ia, J ako rta, I ndo nes ia
t
Department of Surgery, Faculty of Mediéine University of Indonesia, Jakarta, Indonesia182
Sibuea et algrowing,
it
is of
interest
to
see
that
several
socialorganization
for
cancercontrol
have been established such asNederlands Indische Kanker
Instituut
in
1933in
Bandung, Cancer foundationsin
severalcities
in
In-donesia, Wisnuwardhana
Cancer
Foundation in
Surabaya, and Indonesian Cancer Foundation (Yayasan
Kanker Indonesia)
in
1977
in
Jakarta,
followed
by
establishment
of
its
branches
in
27
provinces in
Indonesia.2Since
1989
the Ministry
of
Health
has
actively
par-ticipated
in
CancerControl
andinstructed to
establisha
hospital-based Integrated
Cancer
Control
Team(ICCT) in
everybig hospital.
In
1996, such a team hasbeen
established
in
Cipto
Mangunkusumo National
Center General
Hospital (RSCM) which
functions
asthe
teaching hospital
of
Medical Faculty
of University
of
Indonesia
and
the top
referral hospital
in
theWestern
part
of
Indonesia
by
the
director
of
thehospital
andwith
theapproval of
the Deanof
Medical
Faculty,
University
of
Indonesia. One
of
the
tasksof
this
teamis
to
perform hospital
based cancerregistry,
which
will
provide information on the
magnitude
of
cancer problems
and
data
for
focussing
cancercontrol,
i.e.
thetotal number
of
patients annually,
siteof
cancers,
data
on
survival
of
patients,
the
ratio
between
localized
and
advanced casesat
the
time
of
diagnosis.3In
addition,
to
facilitate the
follow
up
of
all
patients
and
to
furnish
information about
thedemands
made
by
cancer patients
on
the
facilities,
equipment and human resourcesof
the hospital.This
paper presentsa summary
of
the
cancerregistry
data
collected during
the period
of
1997-1998.
Ten mostfrequent tumors were given according to
gender.The
data was analyzed against age,clinical
andhisto-pathological diagnosis, extent
of diseases
and
thenature
of initial
treatment
given to
cancer patients
in
1998.
They were
also evaluated against demographical datain particular
educationalbackground
and age.MATERIALS
AND METHODS
The
Hospital
Based CancerRegistry
in
Cipto
Mangun-kusumo
Hospital was
officially
established
in
1997.To
enasurean
easycollection
of
data
from
different
department
which
were treating cancer,
a Cancer
Registration
Form
(CRF)
was developed based on theform
issuedby
theMinistry
of Health
in
1995.Data from
all
newly
diagnosed cancer patients who
visited Cipto
Mangunkusumo
Hospital from
Januaryl,
1997
until
December
31,
1998
was
recorded in
Med J Indones
CRF.
Table
1 shows
the
items
of
information
which
should be collected.aTable l. Items of Patients Information which should be collected in
the Registration Form
No. Items of Information No. Items of Information
l.
Name of Hospital2. Code of Hospital 3. Medical Record Number
4. Cancer Registry Number 5. Name of Patient 6. Number of Identity Card 7. Gender
8. Date of Birth
9. Address
10. Racial Group I
l.
Religion12. Marital Status
13. Education
14. Occupation
15. Type ofPatient 16. Incidence Date
17. Most Valid Diagnosis
18. Clinical Diagnosis
19. Primary Site: Topography (ICD-O) 20. Histological Diagnosis 21. Morphology (ICD-O)
22. Clinical Extent of Disease before Treatment
23. Multiple Primary Neoplasm 24. Dateof Death
25. Cause of Death (ICD)
26
Name of Oncologist27
Name ofSupervisorThe
form
were sentto
cancertreating
departments andwere
filled
and
completed
by
the treating
medical,surgical
or radiation oncology
doctors
and
approvedby their
supervisors. Then theseforms
were forwarded to theHospital
CancerRegistry
for further
pJocessing:coding,
verification, analyiis
and reporting.s'6For
thecoding
of all
registeredtumors, the
secondedition of
the
International Classification
of
the
Diseases
for
Oncology
(ICD-O)
was used.7In
this
study the
level
of
education
from
all
patients was recorded and was usedto
examine whether
there was adifferential
changein
cancerprevalence
acrosseducational categories.
It
was
categorized
into
illiterate
(unable
to
read and
write),
able
to
read
andwrite,
elementary
school
graduate
(six
years
of
schooling completed),
junior high
school
(9
years
of
schooling completed), senior
high
school
graduate(twelve
years
of
schooling completed),
academy or
university
graduate(more
than
15 yearsof
schooling
completed). Beginning
from
1998on, the information
about the nature
of
initial
therapy and
the data
onwhich
therapy commenced were alsocollected.
RESTJLTS
AND DISCUSSION
A
descriptive study
was
completed
from January
I,
1997
until
December
31,
1998. There were 444.178
new
patients suffered
from
various
diseases who
visited Cipto
Mangunkusumo
Hospital,
among
them2144
(O.48Vo)were
cancerpatients, consisting
of
798(0.l8Vo)
males
and
1346
(0.30Vo)females.
Sukardjareported
2.957o casesof
the total admitted
patien-ts')Vol 9, No 3, July
-
September 2000was
l.2Vo.
The
female
to
male
ratio
was
3.4:2(1346:798),
thesimilar ratiorwas
reportedby
Sukardjabut it
was 2:3in Singapore."
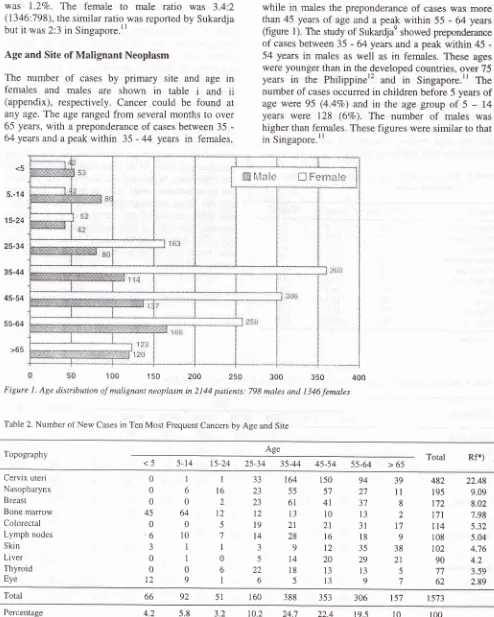
Age and Site of Malignant Neoplasm
The
number
of
cases
by
primary site and age
in
females
and
males
are
shown
in
table
i
and
ii
(appendix), respectively. Cancer could
be
found
atany
age.The
age rangedfrom
severalmonths to
over65
years,with
a preponderanceof
cases between35
-64 years and a peakwithin
35 -44
years
in
females,<5
5.-14
15-24
25-34
35-44
45-54
55-64
>65
[image:3.595.77.571.88.705.2]100 1
50
200
2s0 FigureI.
Age distribution of malignant neoplasm in 2 I 44 patients.Cancer'in Cipto Mangunkusumo Hospital
Jakarta
183while
in
malesthe
preponderanceof
caseswas
more than45
yearsof
age and apea\ within 55
-
64
years(figure
1). The studyof
Sukar-djae showed preponderanceof
cases between 35-
64 years and apeak within
45
-54 years
in
males as well as
in
females. These
ages were younger thanin
the developedcountries, over
75years
in
the
Philippiner2
and
in
Singapore."
The numberof
cases occurredin children before
5 yearsof
age
were
95
(4.4Vo)and
in
the
agegroup
of
5
-
14years
were
128 (6Vo).
The
number
of
males
was higher than females. Thesefigures
weresimilar to
thatin
Singapore.rr300
350798 males and l346females 400
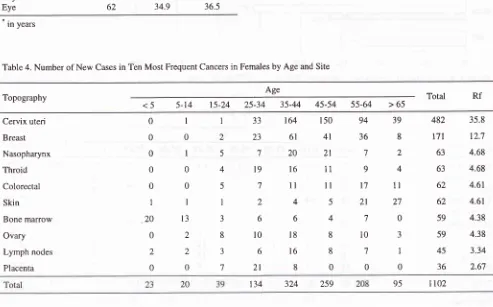
Table 2. Number of New Cases in Ten Most Frequent Cancers by Age and Site
ffi
h{al*
{],JFenr*ie
Age
Topography Total Rf*)
<5 5-14
t5-24
25-3435-44 45-54
5s-64 >65Cervix uteri
Nasopharynx
Breast
Bone marrow Colorectal Lymph nodes
Skin Liver Thyroid Eye
0 0 0 45 0
,6
3
0 0
t2
I 6
0 64 0
10
I
I
0
9
I t6 2 t2 5 7 I
0
6 1
JJ
23
^/.3 12
19 t4 3 5
22
6
94 27 JI
13
3l
l8
35
29
13
9
39
ll
8
2
1',l
9
38
21
5
7
164
15055
5761
4113
1021
2128
16912
14
2018
135
13482
22.48195
9.09172
8.02171
7.98114
5.32108
5.04102
4.7690
4.2't7
3.5962
2.89Total 66 92 51 160
388 353
306 157 t573Percentage
*) Rf = Relative frequency
184
Sibuea etal
The number
of
ten most frequent cancers was
1573 cases, representing 73Vo(1573
:2144) of
all cancers
(table 2). The most frequent
canber encountered wascervical (22.5Vo),
followed by naso-pharyngeal
(9Vo),breast (87o),
bone marrow (8Vo), colore*tal
(5.3Vo),lymph nodes (57o),
skin (4.87o),
liver
(4.2Vo), thyroid (3.67o) and eye (2.9Vo).Cervical carcinoma and breast
cancers were more frequentin the age group of 35-44
years, nasopharyngeal
cancer
in
45-54 years,
bonemarrow
in
0-15
years and
colorectal
in
55-64 years.
The data
collected
by Sukardja
in
East Java shpwed
that
the
most frequent cancer was cervical
cancer,followed by liver
and breast"ancer.n
Table
3.
Mean and Median Age at Diagnosis in Ten Most Frequent CancersCancer
TotalCases
Mean Median' Cervix uteriNasopharynx Breast Bone marrow Colorectal Lymph nodes Skin Liver Thyroid Eye
[image:4.595.80.573.400.707.2]ln years
Table 4. Number of New Cases in Ten Most Frequent Cancers in Females by Age and Site
Med J Indones
The mean age at diagnosis
of cervical
cancer was 47.8years and breast cancer was 45.5
years (table 3). In
USA
these cancerswere diagnosed at older
age,la'lswhile the
mean age
of
cervical cancer and
breastcancer
was
54
years
and
57
years
respectively.
According to Ramli,le the mean age
of
breast cancerwas 46.9 years. The median age
of
nasopharyngealcarcinoma was 43 years, younger than
the study
of
Sudipto
et al who found 50years as the median age.r6In
females
the total
number
of ten
most frequent
cancers was 1102 (82Vo), and the mostfrequent cancer
encounteredwas cervical cancer and
the second was
breast cancer (table4). In other countries of Asia like
the
ast,cervical
rs were
the
ones,
and
y
werecer
esophageal
iupunt3and
USA,
cancer
of
the cervix
has been steadily
decreased.In
USA,
it
only ranked
as cancer number eight.raIn Japanl3
and Singaporell
breastcancer was
also increasing
while
in
USA
it
was
32Vo
of
all
cancers in females.15482
47.8
47195
42.9
43r72
45.5
44t7
|
18.5
l0
tt4
48.5
49.5I
l0
39.3
42r02
58.2
6090
54.2
5'l77
41.6
3962
34.9
36.5Age
Topography Total
Rf
<5
5-14 t5-24
25-34 35-44 45-54
55-64
> 65 Cervix uteriBreast Nasopharynx Throid
Colorectal
Skin
Bone marrow Ovary Lymph nodes Placenta
0
0 0
0 0
I 20 0 2
0 I 0 I 0 0 I
l3
22
0
33
23
7
l9
t64
6l
20l6
ll
46
l8
l6
8
150
4l
2l
11
ll
594 36 7
9
t7
2l
7
l0
7
0 39
8
2
4
1l
27 0
J I
0
482
t7l
63 63
62 62 59 59
35.8 12.7 4.68
4.68 4.6t
4.61 4.38
4.38 1
2
5
4
5
I
3
8
3
7
4
8
8
0 ,|
2 6
t0
6
21
45
3.3436
2.6',1Vol 9, No 3, July
-
September 2000 Cancer in Cipto Mangunkusumo HospitalJakarta
185Table 5. Number of New Cases in Ten Most Frequent Cancers in Males by Age and Site
Age
Topography Total
Rf
<5
5-t4
15-24
25-3435-44
45-54 55-64 >65Nasopharynx Bone marrow Liver Lymph nodes Colorectal Skin Eye Bladder Prostate giand Kidney
0 25 0 4 t, 2
9 0 0 5
5
5l
I 8 0 0 70 0 I
36 6
18 8
10 7 6
8 2
2 20
6
l8
ll
14 14
7
t4
7
3
9 2
l9
8
6
l1
4
,7
20 2
16.5
l4
8.77 '1.89 6.52 5.01 4.64 4.51 3.63 2.26
il
9 0 4 0 0
I I 0 0
132 112 70 63 52 40 37 36 29
l8
16
3567
4
l0
812
t2
10l5
I.J J
33
00
32
589 88
88
l14
87 53
26 73
45
Total
The number
of
ten most frequent
cancers
in
maleswas 589
represented 14Vo
of all
cancers
in
males(table
5).
Nasopharyngeal carcinoma
(NPC)
was
themost frequent cancer
encountered,followed by
bonemarrow
and
liver
malignancy.
Nasopharyngealmalignancy
was morefrequent
in
the age groupof
45-54
years,bone marrow
in 0-14
years andliver
in the
age
group
of >65
years.The
number
of NPC's
casesTabel 6. Number of New Cases in Four Most Frequent Cancers in Children by Age and Site
ICD-O
Site
cD2t
BoneMarrow
Acute leukemia, NOS Acute lymphocytic Acute non-lymphocytic Chronic lymphocytic Chronic myelogenous
Lymph nodes
Burkitt's lymphoma, NOS Hodgkin's disease, NOS Non Hodgkin's lymphoma Carcinoma, unditïeren ti ated Squamous cell carcinoma Eye
Neuroblastoma
Squamous cell carcinoma Rhabdomyosarcoma Retinoblastoma
Kidney
Nephroblastoma, NOS Neoplasma, malignant Carcinoma, NOS
Clear cell sarcoma of kidney c770-779
in
maleswere
132 andin
females were 63 cases.Male
to
female
ratio
was 2.1:1.
Accordrng to the
study
of
Sutjipto
etal,
thenumber
of
NPC
in
the yearof
1980-l98l
in
our hospital
was 219 cases, 154 males and 65females,l6
but the male
to
female ratio was
similar.
This
cancer
ranks number
five
in
Singapore
andnumber
sevenin
the Philippines but
in
Indonesia
it
remains the most
fiequent
cancerin
males.Total
All
M
All
<5
M Age
c690-699
20 25
45000
t2 23
35628
000
202
246
000
000
t45
t0l
000
39t2
000
000
0ll
38il
358
257
l0l
000
000
33
760l
20
6l
ll
1200
22
4t2
1t
02
28
l0
0l
165
02
00
t5
ll
269
'75
l0
0l
0l
109 I
8l
23 0 4
t6
2 2
l0
I I
2t
2
0
6
l3
15
l2
13 51
64011
83846
5 r0
15000
022
2810
lt2
022
t45
000
0ll
279
022
000
055
202
617
4t5
000
r05
t0t
[image:5.595.72.578.101.274.2] [image:5.595.79.571.389.714.2]186
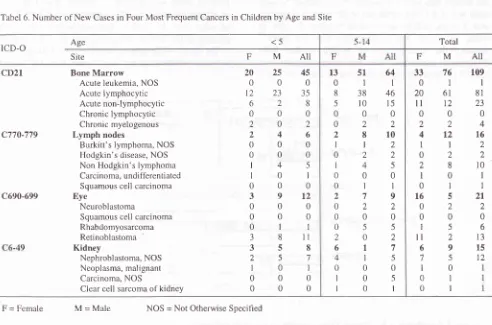
Sibuea et alIn
children, malignancy
of
the bone marrow,
eye,lymph
nodes
and
kidney
were
the
most common
cancers
[table 6
andtable
iii
(appendix)]. The male of
female
ratio was 1.6
:
1. Among 109
casesof
bonemarrow malignancy,
therewere lO5
(96.3Va) casesof
acute leukemia consisting
of
8l
(74.3Vo) cases of
acute
lymphocytic leukemia,
and23 (2l.l%o)
casesof
acutenon-lymphocytic leukemia. There were 4
casesof
chronic myelocytic leukemia.
Thirty
five
(35) patientsof
acutelymphocytic leukemia
aged less than5 years and 48
caseswere
in
the
agegroup
of
5-14years (table
6).
Male
to
female
ratio
was
3:l;
the mean ageat the time
of
diagnosis was 6
years (table7\.
These
fisures were similar
to
dala
in
thePirilippines'2
u"nous,q..'o The most common tumor
of
the
eye wasretinoblastoma
(62Vo)in which
female
tomale ratio was 5.5:1, and
the mean ageat
thetime of
diagnosis was
4
years.There were
ll
(84.6Vo) patientsaged
below
5
years.
In
Surabaya,
the
number
of
retinoblaçtoma patients
were 29.5Voof all
eye cancersand female
to
male
ratio
was
1.5:1.2rIn
USA,
thenumber
of
females was higher than males,
the
age peakedat
l7
months,
and 90Voof
the
cases occurredbelow
5 years
of
age.22The most frequent
cancerof
thekidney
was nephroblastoma (80Vo), femaleto
maleratio was
1.4:1, the mean age atthe time of
diagnosiswas 3
years,and the
age peaked less than5
years. InUSA, the
mean age
at
diagnosis was
2.5
yeurr."
Among
the
malignancy
of
lymph
nodes,
non-Hodgkin's
lymphoma
was
the
most frequent
one (22.2Vo).The
mean ag_e at thetime of
diagnosis was 5Med J Indones
years
andmale to female ratio
was 4:1.
In
USA,
theag
andit
was2.5 times
greaterin
Table 7. Mean
andMedian
Age
atDiagnosis
in Four
Most
Frequent CancersCancer Total
cases Mean*
Median'Acute lymphocytic Acute non-lymphocytic Retinoblastoma Nephroblastoma, NOS Non-Hodgki n's lymphoma * in years
[image:6.595.96.538.455.695.2]Education
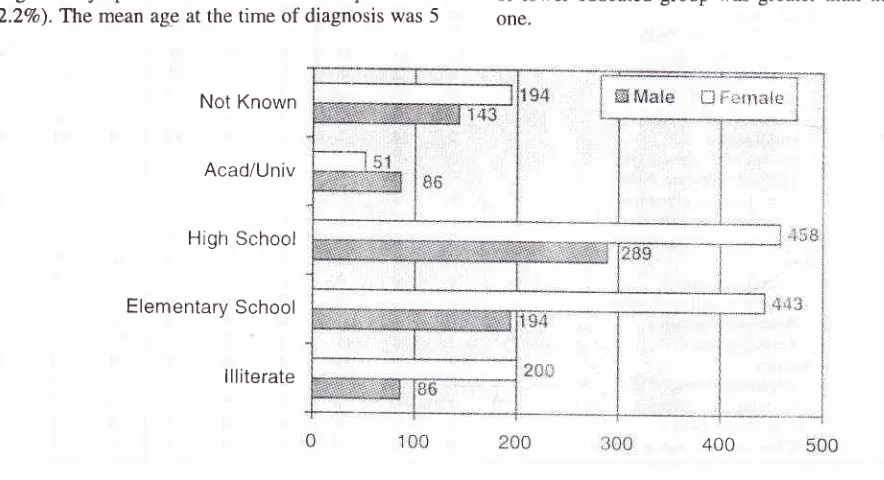
Figure
2
presentsthe number
of new
casesaccording
to educational level and gender in 2144 patients,
798 malesand
1346 females.There were 280
(35Vo)mgle
patients
who
belonged
to
lower
educated
group(illiterate-elementary)
and 375
(477o)
to
higher
educated
group
(high
school-university),
but
in
females, thera
were
643 (48Vo) patientswith low level
of
education and
509
(38Vo)parients with high level
of
education.
It
is
clear
that the
number
of
male patientsin
thehigher
educatedgroup
was greater thanin
thelower,
while
amongfemale
patients thenumber
of
lower
educatedgroup was
greaterthan the higher
one.
81
23
13
t2
l0
65
66
43
JJ
54
Not
KnownAcad/Univ
High School
Elementary School
llliterate
lJ {::ctnair
Figure 2. Distribution of New Cancer Cases according to education and greater
Vol 9, No 3, July
-
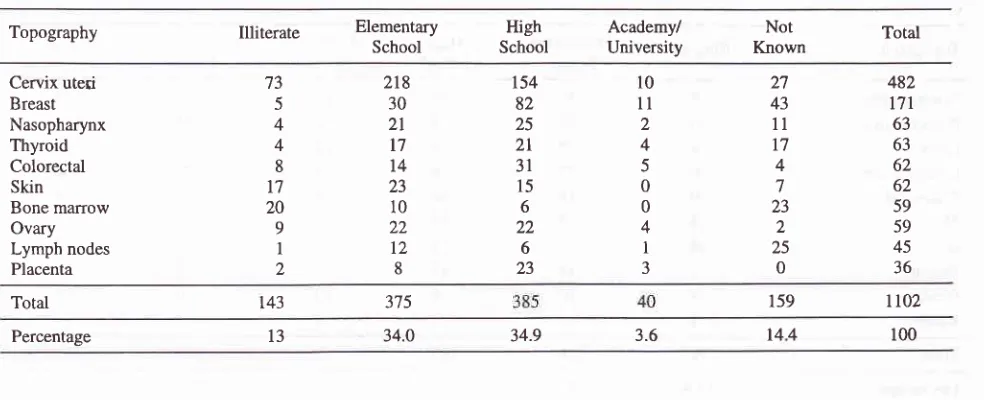
September 2000Table 8. Education Level in Ten Most Frequent Cancers in Females
Cancer in Cipto Mangunkusumo Hospital Jalcarta 187
Topography Illiterate Elemertary
School
Academy/
University KnownNot High
School Total
482
t7t
63 63 62 62 59 59 45 36 27
43
ll
t7
4 7 23
2 25
0 10
1l 2 4 5 0 0 4
I
3154 82 25
2l
3l
15 6 22
6 23 218
30
2t
17
t4
23 10 22
t2
8
'13
5
4 4
8 t7
20 9
I
2 Cervix uteri
Breast Nasopharynx Thyroid Colorectal Skin Bone marrow Ovary Lymph nodes Placenta
Total t43 375 159
lt02
Percentage t3 34.0 34.9 3.6
144
100ln
females,
the
number
of
patients
with
cervical
(60Vo),
skin
(64Vo),
ovary
(52Vo)and bone
marrow
(5OVo) cancer washigher
in
lower
educated group,but
more patients
with
breast, thyroid,
nasopharyngealand
colorectal
cancerswere found
in
higher
educated group (tableiv
and 8). Figure 3 shows the most frequent cancersin females
with low level
of education.
Low
educational
level
of cancer patients was
a
significant
risk factor
for
cervicalls
and breast cancers.reTable
v
andtable 9
show thenumber
of
new
casesby
primary
sites
and
education
in all
and ten
mostCeruix uteri
frequent cancers
in
malesrespectively. The number of
patients
with
bone marrow,
lymph
nodes
and
eyemalignancies
was higher
in
lower educated
group,while the
other numbers were
in
higher
educated group.Most
of patientswith
bonemarrow malignancy
were
acuteleukemia
(l}4lll2 -
93Vo)with
the
mean age atdiagnosis
wasin
the preschool
period (6
yearsof
age),
so they
could
not be
included
in
lower
educated
group.
The similar fact
also occurred
in
eyemalignancy.
[)
Lriv
r'"ifrir;rriiçrrli ievûi ffi i llr".11edLitliili"lrtl
ietrÇ,1Bone
marrow
Ovary
350
300
250
200
150
100
50
0
[image:7.595.78.570.100.300.2] [image:7.595.145.561.498.696.2]I
88
Sibuea et aITable 9. Education lævel in Ten Most Frequent Cancers in Males
Med J Indones
Topography Illiterate Elementary
School SchoolHigh
Academy/
University KnownNot Total Nasopharynx
Bone marrow Liver Lymph nodes Colorectal Skin Eye Bladder Prostate Kidney
5 30 4 6 0 4 24 I
1
4
31 36 9
13
l4
I22 1l
l0
I60
t4
23l4
30
I7
8 l'7 8 8
t4
Il0
2 4
5
1 6 t0 4
22
3l
24 28 42 2 I 0 l
132 112 70 63 52 40 37 36 29
t8
589 115
57
le9
139 79
Total
Percentage 13.4 23.6 33.8 9'7 19.5 100
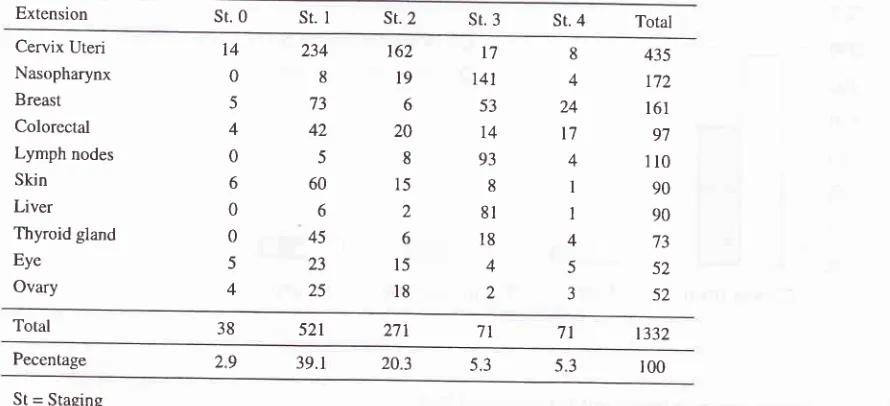
Clinical Extent
of the
DiseaseTable
vi
presents
the
number
of 1617
new cases
by
primary sites and staging.
The number
of
cancerpatients
with
stage
0
I
(localized)
43.85Vo,
)22.02Vo, stage
trI
(regio
)2l.83Vo
and stage
fV
There were
i71
casesof
bone
mzrrrow malignancy
consisting
of 131
(76.6Vo) casesof acute
leukemia,
24Table 10. Primary site and staging in ten most frequent cancers
(l4%o) cases
of chronic leukemia,
I
(0.6Vo)leukemia
NOS,
6
(3.5Vo)
multiple
myeloma,
6
(3.5Vo)polycythemia vera
and3 (l.8Vo)
others.
The
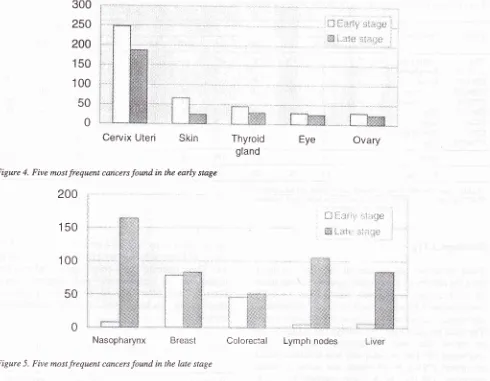
data
of
ten most frequent
cancers
as
presented
in
table
l0
showedtwo different
patterns,namely tumors mostly
found
in the
early
stage (stage 0-I) andtumors mostly
found in
the
late stage (stage
II-IV).
The former
oneconsisted
of
cervical, skin, thyroid, ovary and
eye(figure 4), while the latter
were nasopharynx,
breast,colorectal, lymph
nodes and liver cancers(figure
5).Extension
sr.0
st. I sr. 2 sr. 3 sr. 4 Total Cervix UteriNasopharynx Breast Colorectal Lymph nodes Skin Liver Thyroid gland Eye
Ovary
14 0
5
4 0 6 0 0 5 4
234
8 73 42
5 60 6 45 23 25
162
l9
6 20 8 15
2 6
l5
l8
t'7
14t
53 14 93 8
8l
l8
4 28
4 24 t7 4 I I 4 5 J
435 t72
161 97 110 90 90 t3 52 52
Total 38 521 271 7t 71 t332
Pecentage
St = Staging
[image:8.595.72.517.510.713.2]Vol 9, No
j,
July-
September 2000300
250
200
[image:9.595.83.573.85.466.2]Ceryix
Uteri
Skin
Figure 4. Five most frequent cancers found in the early stage
200
150
100
50
0
Nasopharynx
BreastFigure 5. Five most frequent cancers found in the late stage
Table
vii
showsthe number
of
all cancer
patients by
sites, education and staging.
The
number
of
stage 0and
II
caseswith low
educational
level
was
greaterthan the
high
one
(3.2Vovs lVo,
l3%ovs l07o), while
the number
of
stageI,
III
andfV
caseswere
lower
in
patients
with low
educated
group
compared
to
thehigh
educated
one
(2l%o
vs
22.9Vo, 8.7Vovs
l2%o,4.lVo
vs 5.6Vo).Table
11 shows thecorrelation
of low
andhigh
educational
level
and staging
in
1015 casesof the
nine most frequent
cancers.The number
of late
stage cases (stageII-IV)
in
cervical
cancer washigher
in
the lower
educatedgroup
compared
to
the
higher
educated
group (122
vs
55). The
same
comparison was found in lymphnodes (20
vs 8), skin
(11
vs
10) and eyemalignancies (21 vs 3).
This
condition might
be related
to the fact that a great
number
of
patientshad
low
level
of
education.
Good
education would
contribute
to a good
knowledge
abouthealth
care andto
a
greater chance
for
having
a
job.
On the other
hand, low educationallevel would result
in
unemploy-Cancer in Cipto Mangunkusumo Hospital Jal<orta 189
i-J
firriri
:;ilrrJciij
i-,,ricjïi:riiÊi
,Thyroid
gland
Eye
Ovary
|-"1 il-1.,t ;,,,, ..-i.i f:t:
ËËi l- itli{,, ;i.:-r il{..
Colorectal
Lymph nodesment
andlow
socio-economical
status. Consequently,the
health care
including
cancer screening
would
be neglected.The
Most
Valid
Basis of Diagnosis
of Cancer
Table
viii
showsthe most
valid basis
of
diagnosis
for
selectedsites,
1366 (63.7Vo) caseswere
diagnosedby
histopathology
of
primary
tumor, 251
(ll.7Vo)
by
histopathology
of
metastases,
265
(12.480) were
diagnosed
by
cytology/hematology,
72
(3.3Vo) were
diagnosed
by
clinical only,
173 (8.lVo)
by
clinical
investigations
(X-ray,
USG etc),
11
(0.1Vo)
by
exploratory surgery,
and 6 (O.O3Vo)by
bochemical or
immunological
test. Thus,there were
88Vo caeswhich
were
diagnosedby
microscopic
examinations_and, in
fact,
was higher than
in
Singapore
(76.4Vo),11and in
the
Philippines (52.5Vo
in
males
and
63.2Vo
in
females).''
150
'100
190
Sibuea et alTable I
l.
Nine most frequent cancers by staging and educational levelMed J Indones
St-0 St.III St-IV
ICD.O Description
LEG* HEG** LEG HEG LEG HEG LEG HEG HEG
C539
Cervix UteriCl l0-l
l9
NasopharynxC500-509
BreastCl80-218
ColorectalC77O-7'|O
Lymph nodesCM0-449
SkinC2200
LiverC739
Thyroid glandC690-699
Eye75134
002
I
3
t3l3t4
003
4t14
002
0010
32t4
9l
4 45
2'l I 2l
4
2t
7
108
4
I 5
4
9 0
4
l3
47
t2
4
l4
4 6 2 I 2
l0 -50 t3
) l3
2
0
5
4
5 '74 26
l2
3
4
2
l0
0
-t
3 15
l0
I
0
4t4
150 125
94
32
8l t4 5-5 -50
4
I
4
6 3 0 3
.J 4
35
t48
221
226
l4 l6
100
34 28
134 98
9l
t522 22.3
l4
l6
Percentage
* LEG = [,ow educated group (illiterate, able to write and read, elementary) ** HEG = High educated group (unior and senior high school, academy)
Histological
Types
Table
ix
shows
the
number
of
cases
in
ten
most frequent cancersby histological
type.As
the diagnosisof
the
hepatoma
was merely made
based
on
USG
examination,
it
becameexceptional
and consequently,the
ovarian cancer was
chosen astumor
number
ten.The most frequent
histologic
subtypeof
malignanciesin
cervic the was
keratinizing
squamous
cell
carcinoma
(60.4Vo),in
nasoprahy wasundifferentiated
carcinoma
(79Vo),in
the
breast
was invasive
ductalcarcinoma (58.lVo),
in
the bone marrow was
acutelymphoblastic leukemia
(50.3Vo),in
the
colorectum
was
adenocarcinoma
(68.4Vo),in
the skin
was
basalcell
carcinoma
(50Vo),
in
the thyroid was
papillary
carcinoma
(63.67o)in
eye was squamouscell
carcino-ma
(25.8Vo),and
in
the ovary was
adenocarcinoma (35.6Vo).This tabulation
data can be used as guides onhistological analytical study
or for
future
research purposes.The number
of
squamouscell
carcinoma in
cervical cancer
was
significantly
higher
thanadenocarcinoma
of
the cervix.
In
USA,
the
annualincidence
of
squamouscarcinoma
has beendeelining
steadily
but
adenocarcinoma
has
not. The
declinemight be
related
to
the
increased
utilization
of
PAPsmear,
the
improvement
in
vaginal hygiene,
andchanging
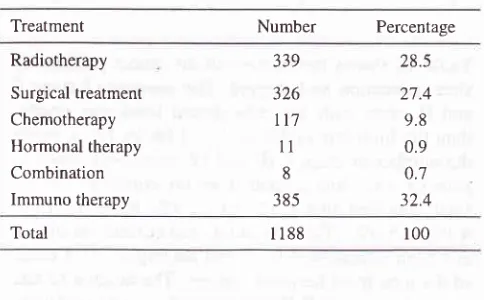
sexual practices.25Initial
Treatment
The
most frequent
initial
treatments among
ll88
cancer patients was radiotherapy
given to
339 (28.580)cases,
followed by
surgical treatment
on
326
(27.4Vo) cases,and chemotherapy
on
117
(9.8Vo) cases (tablel2).
Thesefindings
would
bring
a greatburden
to
thedepartment
of
radiotherapy
and
surgery.
Good
planning
and
effort
should
be
made
to
preventshortage
in
operating theaters
and
radiotherapy equlpment.Table 12. Nature
of
Initial
Treatmenton
ll88
new cancer patientsin
1998Treatment Number Percentage
Radiotherapy
Surgical treatment Chemotherapy Hormonal therapy Combination Immuno therapy
339
326
lt7
11 8
385
28.5
27.4 9.8 0.9 0.7 32.4
Total I 188
From figure 6,
it
can
be
seenthan
49I
(417o)
caseswere treated
within than
I
month,
29
(2Va)
caseswithin
I
month,
ll
(l7o)
caseswithin
2
months,
3(0.27o)
cases
within
3
months
and
the
delayedtreatment consisted
more
than
4
months
after
diagnosis.
There were also 602
(517o)
caseswhich
werenot known. The
delayed treatmentgroup
and thenot
known
status
might
be
due
to
the
poor
socio-economical
condition
of
the patients, and
it
would
increase the
risk of
treatmentfailure.
[image:10.595.77.586.105.277.2] [image:10.595.335.577.458.608.2]Vol 9, No 3, July
-
September 200041"/"
CONCLUSION
1.
During
the
period
of
1997-1998
out
of
444.178
patients
of all
patients treated
in
Cipto
Mangun-kusumo hospital
were 2144
(O.48Vo)
cancerpatients.
The
number
of
female patients
was
1.7times greater than the males.
2.
The
age peakedàt
35-44
yearsin
females,
and at45-54
yearsin
males.In
general, themean
age atdiagnosis
of
various
cancers
was
younger
com-pared
to
other centers.3.
In
females
the
most common malignancies
werecervical, breast
and
nasopharyngeal
cancers,while
in
males
they were
nasopharyngeal, bonemarrow and
liver
cancers.
In
children the
mostcommon malignancies were acute
lymphocytic
leukemia, acute non-lymphocytic leukemia,
re-tinoblastoma,
nephroblastoma andnon-Hodgkin's
lymphoma.
4.
The numberof
female patientswith
low
education-al level
was greater
than the male
ones. Femalepatients
with cervical, skin,
bonemarrow,
ovary,lymph
nodesmalignancies
and male patientswith
bone
marrow,
lymph
nodes and eye malignancies hadlower
educational level.5.
The number
of
the
late
stage cancersin
cervical,lymph
nodes,skin
and eye cancers washrgher
inlower
educated
group
compared
to
higher educated group.6.
The
majority of
patients
(857o) was diagnosedby
microscopic examination.
The
number of
theCancer in Cipto Mangunkusumo Hospital Jakarta 191
51%
)
tr<1
month(41%) tr1
month(2%)
û2
months(1%)
E3
months (0.2%) [image:11.595.74.576.72.817.2]tr4
months(1%)
@> 4 months(4%) ENot
known (51%)Figure 6. Time between the riata of diagnosis and the initiation of cancer therapy
early
stage cancers
was lower
compared
to
thelate
stage cancers (47Vo vs 53Vo).7.
The
most
frequent
initial
treatment
given
tocancer patients
was radiotherapy,
followed
by
surgery and chemotherapy.
8.
In
1998, only
45Vopatients received
treatmentswithin
3 monthsafter
diagnosis.Acknowledgement
The
authors
would
like to
thank
Dr.
Helmy
RustamMM,
Dra.
Sri
Sulistyoningsih,
andthe staff
of
depart-ment
of Medical
Record,
all
doctors
from
the
cancertreating
departmentsin Cipto
Mangunkusumo
Hospi-tal
for
their excellent
care and datacollection.
Special thanksto
Dr.
SuzannaNdraha
SpPD andMrs
Maryati
for
their
helpsin
datacomputing
and secretarial works.This
work
was
supported
by
Cipto
Mangunkusumo
National
Center General
Hospital (RSUPNCM) with
the
approval
of
the
Dean,
Faculty
of
Medicine,
University
of
Indonesia,
No.
30/SKB|FKJUU9T,
andwas partially supported
by
the
Indonesian
Cancer Foundation.REFERENCES
1.
Ministry
of
Heaith
of
the
Republic
of
Indonesia.Guidelines
for
Cancer Controlin
Indonesia, 1989. (inI ncicnesian).
2.
Sukardja DG. The Organizationof
cancerin
Indonesia,presented at the National Cancer Seminar
II
held by the192
J,
4.
Sibuea et
al
World
Health
Organization.WHO
Handbook
for Standardized Cancer Registries, Geneva I 976.Maclennan R. Items of patient information which may be
collected
by
registries.In:
JansenOM,
Parkin DM, Maclænnan R, Editors. Cancer Registration:
Principlesand
Methods. International Agencyfor
Research on Cancer, Lyon, France,l99l
:43-63.Muir
CS, Percy
C.
Classificationand coding
of
neoplasms.In:
JansenOM, Parkin
DM,
Maclennan R,Editors. Cancer Registration: Principles and Methods. Intemational Agency
for
Researchon
Cancer, Lyon, France,l99l:64-81.
Jensen
OM, Storm
HH. Reporting of results.In:
JansenOM,
Parkin
DM,
Macl-ennanR,
Editors.
CancerRegistration:
Principles
and
Methods. Intemational
Agency for Research on Cancer, Lyon, France, I 99l:
108-25.Percy C, Holten VV, Muir C. International Classification
of
Diseasesfor
Oncology.World Health Organization,
Geneva, 1990.Sitas F. National Cancer Registry of South Africa. Annual Statistical Report
for
1988. South African Institute for Medical Research, Joharuresburg 1992.Sukardja
IDG.
Morbidity
andmortality
of
cancer in Surabaya, Indonesia.In:
TjokronegoroA,
Himawan S,Jusuf A, Susworo, AzizMF, Djakaria
M (eds). Cancer in
Asia Pacific,vol
1, Yayasan Kanker Indonesia. Jakarta, 1988 : 153-79.Partoatmodjo
M,
RosfeinR,
Gunawan S.A
survey on cancerin
17 hospitalsin
Jakarta.In:
Tjokronegoro A, Himawan S, JusufA,
Susworo, Aziz }..{F, Djakaria M (eds). Cancerin
Asia Pacific,vol
l,
Yayasan Kanker Indonesia, Jakarta, 1988 : 181-94.Lee HP, Day NE, Shanmugaratnam K. Trends
in
Cancer Incidencein
Singapore 1968-1982. Intemational Agency forResearch on Cancer, Lyon, 1988 : 20-1.Laudico
AV,
EstebanD,
ParkinDM.
Cancerin
the Philippines.World
HealthOrganization
International Agency for Research on Cancer, Lyon, 1989.Hisamichi S. Cancer Registry
in
Japan. In: lokronegoroA, Himawan S, Jusuf
A, Susworo, Aziz
MF, DjakariaM
(eds). Cancerin
Asia Pacific,vol
1, Yayasan Kanker
Indonesia, Jakarta, 1988:l 17-40.Fowler J, Montz FJ. Malignancies of the Uterine Cervix.
In:
CameronRB.
Practical Oncology. Prentice HallMed J Indones
International Inc., New Jersey 1994: 364-76.
Fisher B. Malignancies
of
the Breast.In:
Cameron.RB. Practical Oncology, Prentice Hall Intemational Inc., New Jersey 1994: 417-34.Soetjipto
D,
FachruddinD,
Syafril
A.
Nasopharyngeal Carcinoma in Cipto Mangunkusumo General Hospital. In: TjokronegoroA,
Himawan S, JusufA,
Susworo, AzizMF, Djakaria
M
(eds). Cancerin
Asia Pacihc,vol
l,
Yayasan Kanker Indonesi a, Jakarta, I 988 :499-5 1 3.Luthra UK, Pabhakar AK, Ravi S. Cancer Registrarion in India. In: Ijokronegoro A, Himawan S, Jusuf A, Susworo, AzizMF, Djakaria
M
(eds). Cancer in Asia Pacific, vol 1,Yayasan Kanker Indonesia, Jakarta, 1988 : 103-l 15.
Yanagawa H, Fujita Y, Nagai M, Nakamura
Y, Noda
K, TeshimaK,
et al. Comparative epidemiological study of cervical cancer between Japan and Indonesia.In:
Sasaki R, Aoki K, Eds. Epidemiology and prevention of cancer. The University of Nagoya Press, 1990:84-96.Ramli M. Budiningsih S, Ohno
Y.
Comparative study of the two-period of epidemiological analysis of risk factors for breast cancersin Indonesia. Does
it
change ? Med JIndones, 1999;8:90-7 .
Santana
V.
Childhood leukemia.In:
Cameron RB. Practical Oncology. Prentice Hal Intemational Inc., New Jersey 1994 : 581.Priyanto.
Eye cancer
in
Soetomo Hospital, Surabaya, Indonesia.In :
'IjokronegoroA,
Himawan S, Jusuf A, Susworo, AzizMF,
DjakariaM
(eds). Cancerin
AsiaPasihc,
vol l,'
YayasanKanker
Indonesia, Jakarta, 1988:437-41.Mcintosh JK, Cameron RB. Malignancies of the eye. In:
Cameron
RB.
Practical
Oncology.
Prentice
Hall International Inc., New Jersey 1994: 575-80.Nord RG, Filmer RB.
Wilms'
tumor.In:
Cameron RB. Practical Oncology. Prentice Hall International Inc., New Jersey 1994: 593-8.Santana
V.
Childhood lymphoma.In:
Cameron RB. Practical Oncology. Prentice Hall International Inc., New Jersey 1994: 588-92.Ross
RK,
HendersonBE,
Peters
R,
Mack
T. Epidemiology in relation to cancer control in the USA. In: ljokronegoroA.
Himawan S, JusufA,
Susworo, AzizMF, Djakaria
M
(eds). Cancerin
Asia Pacific,vol
1,Yayasan Kanker Indonesia, Jakarta, 1988: 23-36.
5
t5
t6.
17.
t8. 6
7.
8
9
22
23.
24.
25
ll.
12.
t3
l4
19.
20.
2t
Vol 9,
llo
3, July-
September 2000 Cancer in Cipto Mangunkusumo HospitalJakarta 193
Appendix
Table
ia.
Numbers
of
new
cases
by
primary
site and
age
in
females
ICD-O
Description<5
5-14
ls-24
2s-34
3544
45-54 55-64
>65
Totat
Rf
C0l9
Base oftongueCO2O-O29 Oau parts of tongue
C041-049 Floor of mouth
C050-059 Palate
C060-069 Oau parts of mouth COTO-O79 Parotid gland
C080-089 Oau major salivary glands
C090-099 Tonsil
Cl0O-109 Oropahrynx
Cll0-l19
Nasopharynx Cl50-159 Esophagus Cl60-169 StomachCITO-179 Small intestine Cl80-218 Colorectal
C220
LiverC239
GallbladderC24L
Ampulla of VaterC250
Head ofpancrcasC300
Nasal cavityC3l0
Maxillary sinusC340
Bronchus and lungC398
Overlap.lesion ofresp. syst. and intrathoracal organsC4O2
Long bones of lower limbI 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 I 0 0 I 0 0 0 I 0 I 0 I 0 I 0 0 0 0 0 0 0 0 I 0 0 I I I l3 0 I 0 0 0 0 I
)
0 0 0 0 0 0 0 7 0 0 0 7 l 0 I 0 0 I 0 0 0 I 6 0 2 I I 23 I I JJ)
2 l0 2t)
2 6)
0 0 0 I 0 5 0 2 0 5 0 0 0 0 0 3 0 I 0 2 0 0 0 20 0 0 Ill
4 I 0 0 0 0 0 0 0 3 6 0 4 0 0 6l 3 7 t64 0 2 l8 8 0 4 2 0 I I l6 0 I6168
0 6 0 2 2 0 0 0 0 2l 0 0 2ll
2 0 0 I 2 I 0 0 0 l 4 0 5 2 l I I 0 -t 0140.3
I
13
0.970
I
0.070
8
0.59140.3
0
5
0.370
I
0.070
3
0.22000
2 63
4.68I
2
0.150
3
0.22o40.3
l
l
62
4.612 20
1.490
l
0.070
I
0.070
I
0.07040.3
2
8
0.593
5
0.370
I
0.070
3
0.22I
8
0.590 59
4.38000
27 62
4.61l
6
0.4s040.3
0 7
4t
36 8 l7l
12.7333130.97
56423t.1l
150 94 39
482
35.86
9
2 19
l.4l
2t180.59
8
l0 3 59
4.38000362.67
01o120.89
00280.59
7
2
3 25
1.8600020.15
2r07052
00060.45
9
4 63
4.680030.22
1080-59
7
t
45
3.34 20 0 I 0 I 0 3 0 I 0 0 2 0 0 I 0 0 8 7 0 0 0 0 I 0 t7ll
0 0 0 0 2 I 0 0 I 7 0 2l 0 0 C4l0-419 Bone,jointand 4rtilcularcartilage 0of oau sites
C42l
Bone manowC424
Hematopoietic system Czl40-2149 SkinC48O482 Retroperitoneumandperitoneum 2 C49O499 Connective, subcutaneuous
and
2other soft tissues
C500-509 Breast C5l0-519 Vulva
C529
VaginaC539
Cervix uteriC54l-549 Corpus uteri
C559
UterusC569
OvaryC589
PlacentaC&9
KidneyC679
BladderC690-699 Eye C7W-709 Meninges
C710-719 Braiii
C720-729 Spinal cord, cranial nerves, and
othen parts of CNS C73O-739 Thyroià gand
C750-759 Others endocrine glands and rclated structur€s
C76O-768 Other and ill defined sites ,
C778-779 Lymph nodes
00
00
00
0l
00
00
o2
00
36
00
12
00
o2
32
00
l0
23
).,
ll
0 0 t9I
I 4 I 0 3All sites
42
42s2 163 360 306 25E
123 t346
100 Percentage3.1
3.13.9 t2.t 26.7 22.7 t9.2 9.1
100 Oau=
Others and UnspecifiedCNS = Central Nerves System
[image:13.595.102.549.119.807.2]194
Sibuea et alTable
ià.
Numbers
of
new
cases
by
primary
site and
age
in
males
Med J Indones
ICD.O
C0l9
Base of tongueC020-O29 Oau parts
of
tongueC04l-049 Floor of mouth
C050-059 Palate
C060-069 Oau pans of mouth
C070-079 Parotid gland
C080-089 Oau major salivary glands
C090-099 Tonsil
Cl00-109 Oropahrynx
Cll0-ll9
NasopharynxCl50-159 Esophagus
Cl60-169 Stomach
Cl70-179 Small intestine
Cl80-218 Colorectal
C22O
LiverC239
Gall bladderC24l
Ampulla of VaterC250
Head ofpancreasC300
Nasal cavityC3l0
Maxillary sinusC340
Bronchus and lungC398
Overlap.lesion ofresp. syst. andintrathoracal organs
C402
Long bones of lower limbC4l0-41
9
Bone, joint and artilcular cartilage ofoau sites
C42l
Bone marrowC424
Hematopoietic system Cul40-2149 SkinC480-482 Retroperitoneum and peritoneum
C490-499 Connective, subcutaneuous and other soft tissues
C500-509 Breast
C609
PenisC6l9
Prostate glandC629
Descended testisC649
KidneyC6'79
BladderC690-699 Eye
C700-709 Meninges
C7l0-719 Brain
C72O-729 Spinal cord, cranial nerves, and others
pans of CNS
C'7 30-739 ThJroid gland
Others endocrine glands and related
c750-759 skuctures
C760-768 Other and ill dehned sites
C7'78-719 Lymph nodes
<5
5-14
15-24 25-34 35-44 45-54 55-64
>65 Total120100
105
63000
000
000
000
000
000
000
000
0 -s ll
000
000
000
000
010
000
000
00t
002
001
000
000
021
010
0303060.75
0010010.13
2t00140.5
00012i0.38
3
3
I
I
2 t0
1.250
I
0
0
0 I
0.t30031150.63
0300140.5
16 35 36 20 9 132
16.500t2250.63
022509t.13
1100130.38
12 l0
l0
t4 6 52
6.524
l0
18 l8 19 70
8.7'l0002r30.38
0
0
I
0
0 I
0.t300t4170.88
r00328t
0002360.75
0r-s65172.t3
0001010.13
0
0
r060.75
0140.-5
62ltzt4
0
0 l
0.t3t4 ll 40
5.0rI
I -s
0.634
2 18
2.266 0 I I 2
7 0
-5
I 2
6
0
'7
0
2
0
2
0
5 3 3 0
l I
0 0
2
0
3 2 3 3 I 0 0
0 3 2 2 2 8 6
0 4 0
I 2
,7
0 3
t4
7 0
4
I
0 I
0.134 t4
l;7520 29
3.630 14
1.752 t8
2267 36
4.-s t4 31
4.64o 2
0.250 13
1.630 I
0.132
0
t
t2
2 I
4
t l4
t.750050.63
2tl2l.5
lr
8 63
7.89I 8
3 8 25
0 2 I 2
51
9l0
00
00
3l
00
0t
00
ll
l0
0l
7t
00
t3
00
0
0
0 2
-5
0 9 0
0 0
002
012
2tt
484
All sites
53
86 42 80l4
t37 166t20
798 100Percentage
6.6
r0.8 53 l0t4.3
t72 20.8 15
100 [image:14.595.108.554.100.755.2]VoI 9, No 3, JuIy
-
SePtember 2000Table
ii.
Number of
new cancer
cases
by primary
sites and
ageCancer in Cipto Mangunkusumo Hospital
Jakarta
195ICD-O
c0l9 Base of tongue
CO20-029 Oau parts of tongue
C04l-049
Floor of mouthC050-059 Palate
C060-069 Oau parts ofmouth
C070-079 Parotid gland
C080-089 Oau major salivary glands
C090-099 Tonsil
Cl00-109
OropahrynxCl10-l
19
NasopharynxCl50-159
EsophagusCl60-169
StomachCl'10-179
SmallintestineC180-218 Colorectal
C220
LiverC239
Gall bladderC4l0-419
Bone, joint and artilcular cartilage of oau sitesC42l
Bone marrowC500-509 Breast
C5l0-519
VulvaC529
Vaginac539 Cewix uteri
C54l-549
Corpus uteriC559
UtenrsC569
OvaryC589
Placentas-r4
15-24 25-34
35-44
45-54 55-64
>65
Total2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
200
266
00t
222
002
351
0t0
003
030
23 55
57001
o22
122
19 2t
2l51420
010
l0l
002
102
t0l
015
000
l0l
232
t2
13
t0000
3912
2t2
323
23 61
4t133
t75
33 t64
150206
'>))
l0
18
82l
80
223
002
532
522
578
6
5
133r0
rt6
010
22 18
13201
221
14 28
160 t 0 l6 0 2 0 5 0 0 0 I 3 2 I 0 2 0 l2 0 I 0 I 2 0 0 I 0 0 8 7 I 0 I 0 I t 0 4 0 6 3 I 'l 0 0 0 0 0 0 0 0 0 0 2 0 45 2 0 0 I 0 I 0 I 0 6 0 0 0 0 I 0 0 0 I 0 0 I 3 2 64 I I 0 3 0 0 0 I 0 0 2 0 0 0 I 7 0 9 0 3 2 0 I 4 l0 2 4 0 3 I 2 I 2 0 21 3 6 I 3l 29 2 0 4 3 4 7 I I I l3 0 35 I 4 5t 3 6 94 9 I
9
0.4219
0.892
0.o9t2
0.56'1
0.3315
0;l2
0.098
0.374
0.19l
l 195
9.093
7
0.33o
12
0.56I
'1
033t7
I14
5.322t 90
4.2I
4
0.190
2
0.09l
8
0.372 12
0.565 14
0.658 22
1.03o
2
0.090
9
0.422 t2
0.562
l'lI
7.980
I
0.0538 102
4.762 tr
0.512 22
1.038 t72
8.023 13
0.614 23
1.0739 482
22.482 19
0.89r
8
0.3'7C24l
Ampulla ofVater
0C250
HeadofPancreas
0C300
NasalcavitY
0C310
Maxillarysinus
IC340
Bronchus andlung
0C398
Overlap.lesion of resp. syst. and intrathor.organs
0C4O2
t ong bones of lowerlimb
IC424
HematoPoieticsystem
0C44O-449
Skin
3C48O-482 Retroperitoneum and
peritoneum
3C49O-4gg Connective, subcutaneuous and other soft
tissues
4c609
c6l9
C629
Descended testisC649
KidneyC619
BladderC690-699 Eye
C700-709 Meninges
C71O-'I
19
Brainl0 3 59
2.750
0 36
1.682
4 14
0.65'7 20 29
1.350
0 14
0.654230r.4
t4 9 44
2.O59
7 62
2-890040.19
5
0 20
0.93l
0
'l
o.33t3 5 'l'l
3.590080.37
3
I
20
0.9318 9 108
5.04Penis Prostate gland
8 0
t2
0 0 C72O-129 Spinal cord, cranial nerves, and others parts
ofCNS
3C'130-739 Thyroid
gland
0C'15O-759 Others endocrine glands and related
structures
I C760-768 Other and ill definedsites
4C7'18-779 Lymph nodes
All sites r28 94 243
424
243
2144
1004.41
5 97 22.1 20.1 l9 8ll
Percentage
[image:15.595.70.559.106.707.2]196 Sibuea et
al
C4l0-419
Bone,jointandartilculrcarrilageof
0 0
0
I
;
;
;
;
;
oau sites
C42l
Bone marrowMed J Indones
Table
iii.
Numbers
of
ne\4/cases
by
primary
site and
age
in children
IC
Age n-D-o
:g:_î::
Ii'"I:..
0 o 0 I 0 I 0 I
UIU ,:î:î11: larotiderand
0 o 0 I 0 I
0C090-099Tonsil
rl^;:vrt'
-rrnrr^
o o
o
I
o
I
oCllo-llg Nasopharynx
0 0 0 I ;
;
;
i
;
C220 Liver
/r ^ ^
^vLLwLrvËr0000lll0l
9:99
Nasalcaviry
0 0 0 I 0
r
0
I
Iç119
Maxillarysinus
I 0 I 0 0 0 0 I
Ic398
overrap'resionofresp.syst.and
0 0 0 l 0
l
0
I
r
intrathoracaI organs
2î??^,^
3:qTl-":"tlowerlimb I 0 I I 2 3 2 2
4Acute leukemia,
NOS
0
0 Acutelymphocytic
12
23 Acute nonlymphocyric
6
2 Chroniclymphocytic
0
0soft tissues
C539
Cervixuteri
0
0C569
Ovary
0
0C629
Descendedtesris
O
2C649
KidneyNephroblastoma,NOs
2
sNeoplasma,
malignant
I
0Carcinoma,NOS
6
0Clear cell sarcoma of
kidney
0
0c69o-699
ut_",^---^.,-
o
oinoma
0
0Rerinoblastoma
3
ÀCTIO-719
Brain
0
0C72O-729
Spinal cord, cranial nerves, and others3
000lt0ll
3583846206181
8 5 l0 15 l1 12
230000000
2022224
00tll0l
3101224
3000123
4033527
010t011
0202022
2011303
741s7512
100010
010501
010101
000022022
inoma000000000
RerinobrastomaSÀr1
i;iirtrf,
CTl0-7lgBrain00OZl3t23
c72o-729
spinalcord,craniarnerves,andothers3 0 3 2 o 2 0 5
5
parts of CNS
c75o-759
othersendocrineglandsandrelated
l 0 I 0 l
l
r
l
2
structures
C760-768
Otherandilldefinedsites
2 2 4 3 I
4
3
5
8
C77O-779
Lymph nodesBurkitt's
lymph.oma,NOs
0 Hodgkin'sdisease,NOS
0 Non-Hodgkin'slymphoma
1Carsinoma,undifferentiated,NOs
I [image:16.595.78.579.96.761.2]Vol 9, No 3, July
-
September 2000 Cancer in Cipto Mangunkusumo HospitalJalarta
197Table
iv.
Numbers
of
new
cases
by primary
site and education
in
females
ICD-O
DescriptionE
JH
SH Ac NK
Totalc019 c020-029 Cc/.I-0/;9 c050-059 c060-069 c070-o79 c080-089 c090-099 cl00-109
cl
l0-l l9 cl50-159 cl60-169 ct70-179 cl80-218 c220 c239 c24t c250 c300c3l0
c340 c398c402 c4to-4t9
c42l c424 c440-449 c480-482 c490-499
c500-509 c510-519 c529 c539 c54t-549 c559 c569 c589 c649
c6'19
c690-699 c700-709 cTto-719
c720-'129
c730-739 c750-759
Base of tongue
Oau parts of tongue
Floor of mouth
Palate
Oau parts of mouth Parotid gland
Oau major salivary glands
Tonsil
Oropahrynx Nasopharynx
Esophagus
Stomach Small intestine Colorectal
Liver Gall bladder
Ampulla of Vater
Head of pancreas
Nasal cavity Maxillary sinus
Bronchus and lung
Overlap.lesion ofresp. syst. and
intrathoracal organs
Long bones oflower limb
100
016
001
210
210
001
100
001
000
4516
010
001
001
8212
311
000
000
010
002
202
001
100
I
2
6 0
t7
0
I
25
I
.,
t29
6 2
l3
4 0 4
5
I
7
I
l3
0
55
4t
63
73
89L2
t2
99
24
73
00
13
I00
l0
3t
44
l0
I
2
0 4 0
2
0
I
0
8
0 0
2
l0
2
0 0 0 0 0 0 0
I o
l0t4
31013
0001
Bone,joint and artilcular cartilage 0
of oau sites
Bone marrow Hematopoietic system
Skin
204
00
176
1008
1004
l0l5
0001
1003
0000
172tt63
0012
2003
1004
216362
301020
l00l
00ll
0001
0024
1038
t2l5
0001
0003
3ll8
402359
0000
80762
3006
1004
59 lt
42
r7l
2tt13
51123
75 l0
27
482ll4t9
l0l8
134359
t43036
001r2
0308
10225
10.02
llrT
0006
184r763
2003
0018
20 ,1 0
I
24 J 5
79
4 I
8 9
I I
3
0
I I
J
0 Retroperitoneum and
peritoneum
2
|Connective, subcutaneuous
and 0
Iother soft tissues
Brcast
Vulva Vagina Cervix uteri
Corpus uteri Uterus
Ovary
Placenta
Kidney
Bladder Eye Meninges
Brain
Spinal cord, cranial nerves, and others parts of CNS
Thyroid gland
Others endocrine glands and
related structures
C760-768 Other
and ill defined sites501
C778-779
Lymphnodes
I
I
ll
2
4
O 26
45All
sites
199
t52 292 189 27t 5t
lg2
1346Percentage
t5 I1.3 21.7 t4
20t43
100I=iliterate
A=Able to read and write
E=Elementary
JH= Junior High School SH=Senior High School
[image:17.595.121.528.101.668.2]198
Sibuea et alTable v. Numbers
of
new
cases by
primary
site and education
in
males
Med J Indones
ICD-O
Description JHSH Ac
NK
TotalcOl9 Base of tongue 3
0 0 0 0 0 0 0 0 5 0 0 0 0 4 0 0 0 0 0 0 0 0 I 30 0 4 I I 0 0 I 2 4 I t7 0 I 0 I 0 0 0 0 0 0 0 0 4 0 I 0 5 I 0 0 0 I 0 0 0 0 0 t4 0 5 I 2 0