EVALUASI TIPE DNA HPV KANKER SERVIKS
PASCARADIASI/ KEMORADIASI DI RSUP H. ADAM MALIK MEDAN
Deri Edianto, M. Fauzie Sahil, Christoffel L. Tobing, Edy Ardiansyah, M. Fidel Ganis Siregar, Fatin A.
Departemen Obstetri dan Ginekologi Fakultas Kedokteran Universitas Sumatera Utara
Medan, Indonesia, 2013
ABSTRAK
LATAR BELAKANG: Perkembangan teknik biomolekuler saat ini memungkinkan kita untuk melakukan deteksi genotipe DNA HPV sebagai salah satu metode penilaian respon terapi pada penderita kanker serviks pascaradiasi/ kemoradiasi. Tujuan penelitian ini adalah untuk menilai respon terapi berdasarkan tipe DNA HPV pada penderita kanker serviks pasca radiasi/ kemoradiasi di RSUP. H. Adam Malik Medan.
METODE: Subyek penelitian adalahpenderita kanker serviks pascaradiasi/ kemoradiasi yang berobat di poli rawat jalan ataupun rawat inap RSUP H. Adam Malik Medan (n=25) yang diperoleh secara consecutive sampling serta memenuhi kriteria inklusi. Terhadap subyek penelitian dilakukan penilaian respon klinis berdasarkan tipe DNA HPV.
HASIL: Respon terapi parsial lebih sering ditemukan pada tipe DNA HPV 16 yaitu 7 (50%) penderita, respon terapi penyakit menetap ditemukan lebih sering pada tipe DNA HPV 16, 18 dan 31 yaitu 1 (33.3%) penderita, respon terapi penyakit progresif ditemukan sebagian besar pada tipe DNA HPV 16 yaitu 5 (62.5%) penderita. Jenis histopatologi sel skuamos ditemukan lebih banyak pada tipe DNA HPV 16 yaitu 11 (57,9%) penderita, jenis histopatologi adenokarsinoma ditemukan lebih sering pada tipe DNA HPV 18 yaitu 3 (50%) penderita. Jenis histopatologi sel skuamosa ditemukan lebih banyak dengan respon terapi parsial yaitu 10 (52.6%) penderita, jenis histopatologi adenokarsinoma ditemukan sebagian besar dengan respon terapi parsial yaitu 5 (83%) penderita. Terapi kemoradiasi ditemukan lebih banyak pada respon terapi parsial yaitu 12 (57.1%) penderita, terapi radiasi ditemukan lebih sering pada respon terapi parsial dan penyakit progresif yaitu 2 (50%) penderita.
KESIMPULAN: Respon terapi parsial ditemukan lebih banyak pada tipe DNA HPV 16. Respon terapi penyakit menetap ditemukan lebih sering pada tipe DNA HPV 16, 18 dan 31. Respon terapi penyakit progresif sebagian besar ditemukan pada tipe DNA HPV 16.
EVALUATION OF HPV DNA TYPE
IN POST RADIATION/CHEMORADIATION CERVICAL CANCER AT H. ADAM MALIK GENERAL HOSPITAL MEDAN
Deri Edianto, M. Fauzie Sahil, Christoffel L. Tobing, Edy Ardiansyah, M. Fidel Ganis Siregar, Fatin A.
Department of Obstetric and Gynecologic Faculty of Medicine, University of Sumatera Utara
Medan, Indonesia, 2013
ABSTRACT
BACKGROUND: Current development of biomolecular techniques allows us to detect HPV DNA genotype as a method to assess therapy response in post radiation/chemoradiation cervical cancer patients. The objective of the study was to detemine the therapy’s response based on HPV DNA type in post radiation/chemoradiation cervical cancer patients at H. Adam Malik General Hospital Medan.
METHOD: Subjects were postradiation/ chemoradiation cervical cancer patients treated in outpatient or inpatient department of Adam Malik Hospital Medan (n = 25) obtained by consecutive sampling and met the inclusion criteria. Clinical response assessment based on the type of HPV DNA was performed to the subjects.
RESULT: Partial response to therapy was found more frequently in type 16 HPV DNA with 7 (50%) patients, resistant to therapy response was found more frequently in types 16, 18 and 31, with 1 (33.3%) patient each, progressive disease response was found mostly in type 16 with 5 (62.5%) patients. Squamous cell histopathology was found more often in type 16 with 11 (57.9%) patients, adenocarcinoma histopathology was found more frequently in type 18 with 3 (50%) patients. Squamous cell histopathology was found mostly in partial response to therapy group with 10 (52.6%) patients, adenocarcinoma histopathology was found mostly in partial response to therapy group with 5 (83%) patients. Chemoradiation was found more often in partial response to therapy group with 12 (57.1%) patients, radiation therapy was found more often in partial and progressive disease response with 2 (50%) patients each. CONCLUSION: Partial response to therapy was found more often in type 16 HPV DNA. Resistant to therapy response was found more frequently in types 16, 18 and 31 HPV DNA. Progressive disease response was found mostly in type 16 HPV DNA.
LATAR BELAKANG
Kanker serviks merupakan salah satu penyakit keganasan ginekologi tersering yang menimbulkan masalah kesehatan pada kaum perempuan di seluruh dunia.Di Indonesia kanker serviks menjadi perhatian penting karena kebanyakan penderita datang sudah dalam keadaan terlambat yaitu pada stadium lanjut sehingga pengobatan yang diberikan adalah radioterapi sebagai terapi utama.Tipe DNA HPV yang terdeteksi pada pemeriksaan genotyping dapat menjadi penanda yang berguna untuk melakukan evaluasi pasien kanker serviks pasca terapi walaupun hanya dengan sisa minimal penyakit dan kekambuhan dini.
METODE PENELITIAN
Rancangan penelitian ini merupakan penelitian observasional deskriptif menggunakan studi potong lintang untuk menentukan tipe DNA HPV berdasarkan respon terapi pada penderita kanker serviks pascaradiasi/ kemoradiasi di RSUP H. Adam Malik Medan. Penelitian dilakukan di Departemen Obstetri dan Ginekologi Fakultas Kedokteran Universitas Sumatera Utara - RSUP.H Adam Malik Medan serta Laboratorium Kalbe Genomic (KALGEN) Jakarta. Penelitian dilakukan pada perode bulan Februari - Juni 2013.
[image:3.595.84.477.526.765.2]HASIL PENELITIAN
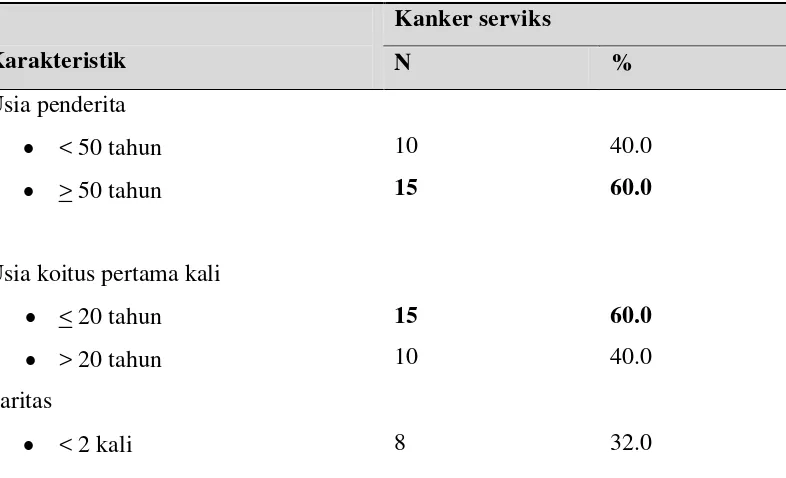
Tabel 1. Karakteristik penderita kanker serviks pascaradiasi/ kemoradiasi di RSUP H. Adam Malik Medan.
Karakteristik
Kanker serviks
N %
Usia penderita • < 50 tahun • > 50 tahun
10 15
40.0 60.0
Usia koitus pertama kali • < 20 tahun • > 20 tahun
15 10
60.0 40.0
Paritas
• ≥ 2 kali 17 68.0 Ukuran massa tumor
• ≤ 4 cm • > 4 cm
11 14
44.0 56.0 Jenis Histopatologi
• Sel skuamous • Adenokarsinoma • Adenoskuamosa
19 6 0
76.0 24.0 0
Stadium Klinis
• I
• II
• III
• IV
3 8 12 2
12.0 32.0 48.0 8.0
Jenis Terapi
• Kemoradiasi • Radiasi
21 4
84.0 16.0
Respon terapi
• Respon Parsial (RP) • Penyakit Menetap (PM) • Penyakit Progresif (PP)
14 3 8
56.0 12.0 32.0
Tipe DNA HPV • Tipe 16 • Tipe 18 • Tipe 31 • Tipe 33 • Ti[pe 52 • Tipe 58
13 6 1 2 1 2
Dari hasil penelitian didapatkan bahwa sebagian besar penderita berusia > 50 tahun yaitu 15 (60%) penderita, sedangkan yang berusia < 50 tahun yaitu 10 (40%) penderita. Dari hasil penelitian didapatkan bahwa sebagian besar penderita menikah pertama kali pada usia <20 tahun yaitu 15 (60%) penderita, sedangkan yang menikah pertama kali pada usia > 20 tahun yaitu 10 (40%) penderita. Dari hasil penelitian didapatkan bahwa sebagian besar penderita memiliki paritas > 2 kali yaitu 17 (68%) penderita, sedangkan penderita yang memilki paritas < 2 kali yaitu 8 (32%) penderita. Dari hasil penelitian didapatkan bahwa penderita dengan ukuran massa tumor > 4 cm ditemukan lebih banyak yaitu 14 (56%) penderita dibandingkan dengan penderita yang memiliki ukuran massa tumor ≤ 4 cm yaitu 11 (44%) penderita.Dari hasil penelitian didapatkan
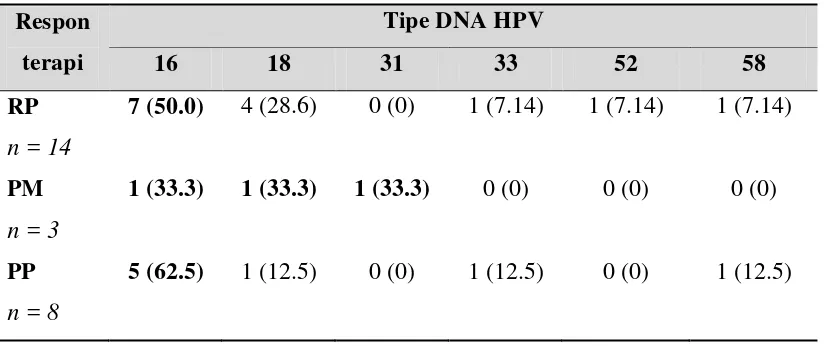
[image:5.595.74.486.546.719.2]bahwa penderita kanker serviks dengan stadium III ditemukan paling banyak yaitu 12 (48%) penderita, diikuti oleh stadium klinis II pada 8 (32%) penderita, stadium I 3 (12%) penderita, sedangkan penderita kanker serviks dengan stadium IIA, IIIA, IVA dan stadium IV 2 (8%) penderita.Dari hasil penelitian didapatkan bahwa umumnya penderita mendapatkan terapi kemoradiasi yaitu 21 (84%) penderita, sedangkan penderita yang hanya mendapatkan terapi radiasi saja yaitu 4 (16%) penderita.Dari hasil penelitian didapatkan bahwa pascaradiasi / kemoradiasi penderita dengan respon terapi parsial ditemukan lebih banyak yaitu pada 14 (56%) penderita, diikuti dengan penderita yang mengalami respon penyakit progresif yaitu 8 (32%) penderita dan yang mengalami respon penyakit menetap yaitu 3 (12%) penderita. Tabel 2. Distribusi respon terapi berdasarkan tipe DNA HPV pada penderita kanker
serviks pascaradiasi/ kemoradiasi di RSUP. H. Adam Malik Medan. Respon
terapi
Tipe DNA HPV
16 18 31 33 52 58
RP
n = 14
7 (50.0) 4 (28.6) 0 (0) 1 (7.14) 1 (7.14) 1 (7.14)
PM
n = 3
1 (33.3) 1 (33.3) 1 (33.3) 0 (0) 0 (0) 0 (0)
PP
n = 8
Dari 14 penderita kanker serviks pascaradiasi/ kemoradiasi dengan respon terapi parsial didapatkan bahwa tipe DNA HPV 16 ditemukan lebih banyak yaitu pada 7 (50%) penderita. Diikuti dengan tipe DNA HPV 18 yaitu pada 4 (28.6%) penderita. Sedangkan untuk tipe DNA HPV 33, 52 dan 58 masing masing ditemukan hanya pada 1 (7.14%)
penderita.Dari 8 penderita kanker serviks pascaradiasi/ kemoradiasi dengan respon terapi penyakit progresif terlihat bahwa sebagian besar penderita memiliki tipe DNA HPV 16 yaitu 5 (62.5%) penderita. Sedangkan penderita dengan tipe DNA HPV 18, 33 dan 58 masing-masing hanya pada 1 (12.5%) penderita.
KESIMPULAN
Berdasarkan karakteristik, umumnya penderita kanker serviks menjalani terapi kemoradiasi yaitu 21 (84%) penderita. Sebagian besar penderita kanker serviks adalah berusia > 50 tahun yaitu 15 (60%) penderita, usia koitus pertama kali < 20 tahun yaitu 15 (60%) penderita, paritas > 2 kali yaitu 17 (68%) penderita, jenis histopatologi sel skuamosa yaitu 19 (76%) penderita. Lebih banyak penderita kanker serviks dengan ukuran massa tumor > 4 cm yaitu 14 (56%) penderita, mengalami respon terapi parsial yaitu 14 (56%) penderita, terdeteksi memiliki tipe DNA HPV16 yaitu 13 (52%) penderita, dan lebih sering ditemukan pada stadium III yaitu 12 (48%) penderita. Distribusi berbagai respon terapi berdasarkan tipe DNA HPV didapatkan bahwa, respon terapi parsial lebih banyak ditemukan pada tipe DNA HPV 16 yaitu pada 7 (50%) penderita. Respon terapi penyakit menetap lebih sering ditemukan
terapi radiasi lebih sering ditemukan dengan respon terapi parsial dan respon terapi penyakit progresif yaitu 2 (50%) penderita.
SARAN
Pemeriksaan tipe DNA HPV hendaknya dapat dijadikan protokol
pemeriksaan pada penderita kanker serviks yang berobat di RSUP. H. Adam Malik Medan, sebagai salah satu metode evaluasi pra dan pascaterapi untuk tujuan perencanaan terapi dan menentukan prognosa penyakit.
DAFTAR PUSTAKA
1. Schellekens MC, et al. Prevalence of single and multiple HPV types in cervical carcinomas in Jakarta, Indon esia. Gynecologic Oncology 2004;93:49-53.
2. De Boer MA, et al. Human papillomavirus type 16 E6, E7, and L1 variants in cervical cancer in Indonesia, Suriname, and The Netherlands. Gynecologic Oncology 2004;94;488-94.
3. Tjokroprawiro BA, dkk. Eliminasi Human Papillomavirus (HPV) dan
Respon Terapi pada Adenokarsinoma Serviks dan Karsinoma Sel Skuamos Serviks yang mendapat pengobatan Kemoradiasi. Majalah Obstetri Ginekologi Indonesia. Vol 32, No 2. April 2008: 105-15.
4. Datta NR, et al. Does preteratment human papillomavirus (HPV) titers predict radiation respons and survival outcomes in cancer cervix?-A pilot study. Gynecologic Oncology 103 (2006). 100-05.
5. Morris M, et al. Pelvic radiation with
Con-current Chemotherapy Compared with Pelvic and
Para-Aortic Radiation for High-risk Cervical Cancer. The New England of med J. 1999; 340:1137-43.
6. Novel SS, et.al. Perbandingan Beberapa Metode Molekuler dalam uji DNA HPV (Human
Papillomavirus). Cermin Dunia Kedokteran 186. Vol 38 no 5. Juli-Agustus 2011.:356-58.
7. Iskandar MT, dkk. Uji klinik kemoradiasi dibanding radiasi terhadap respon infeksi HPV dan respon klinik pada karsinoma sel skuamosa serviks uteri. Majalah Obstetri Ginekologi Indonesia. Vol 32, No 4. Oktober 2008: 212-22. 8. Nagai Y, Toma T, Moromizato H.
Persistence of human papillomavirus infection as a predictor for recurrence in carcinoma of the cervix after radiotherapy. Am J Obstet Gynecol 2004; 191: 1907-13.
9. Noviana H. Human Papillomavirus dan Kanker Serviks. Cermin Dunia Kedokteran-189. 2012. Vol 39 no.1: 65-66.
10. Lee MF, et al. Detection of human papillomavirus types in cervical adenocarcinoma by the polymerase chain reactin. International Journal of Gynecology and Obstetrics 63 (1998): 265-70.
11. Tseng CJ, Tseng LH, Lai CH. Identification of human papillomavirus types 16 and 18 deoxyribonucleic acid sequences in bulky cervical cancer after chemotherapy 1997;176: 865-9.
sequencing. Oncol Rep 2002; 10: 175-9.
13. Ferdousi J, et al. Impact of human papillomavirus genotype and response to treatment and survival in patient receiving radiotherapy for squamous cell carcinoma of the cervix. Experimental and therapeutic medicine 1. 2010: 525-30.
14. Song YJ, et al. Persistent human papillomavirus DNA is associated with local recurrence after radiotherapy of uterine cervical cancer.
15. Hecker NF, Friedlander ML. Berek and Hacker’s Gynecology Oncology: Cervical Cancer. Edisi 5. Lippincott williams & wilkins. 2010. 342-88 16. Monk BJ, et al. Clinical Ginecologic
oncologic: invasive cervical cancer. Edisi VII. Mosby Elsevier. 2007. 55-65.
17. Kreshnamurti I, dkk. Radioterapi pada kanker serviks. Departemen Obgin FK UNSRI. 2010.
18. Burger RA, et al. Human papillomavirus type 18: association with poor prognosis in early stage
cervical cancer. http://www.ncbi.nlm.nih.gov/entrez/
query.fcgi. J natl Cancer Inst. 1996; 2,88 (19): 1361-8.
19. Fingert HJ, Pardee BA, Campisi J. Molecular biology and biochemistry of cancer. In: Knapp J, Berkowitz RS, editors. Gynecology oncology. 2nd ed. Boston: McGraw-Hill. 1993: 3-35.
20. Chaterjee R, et al. Detection of HPV DNA in cervical carcinoma after treatment in India. Int J Hum Gen 2005; 5: 27-31.
21. Kulmala SM, et al. Human papillomavirus testing with hybrid capture 2 assay and PCR as screening tools. J Clin Microbiol 2004; 42: 2470-5.
22. Sounderland-strand A, et al. Comparison betweenthe Hybrid Capture II test and a PCR-Based
Human Papillomavirus Detection Method for Diagnosis and PosttreatmentFollow-up of Cervical Intraepithelial Neoplasia. J ofClin Micobiology. 2005; 43: 3260-6. 23. Dusenbery KE, Gerbi BJ. Technical
basic of radiation therapy: radiation therapy for cervical cancer. Springer Heidelberg. Edisi 4. Germany 2006: 579-90.
24. Giuntoli RL. Bristow RE. Danforth’s obstetric and gynecology: cervical cancer. Lippincott williams & wilkins. 2008: 973-87.
25. Beyzadeoglu M, et al. Basic of Radiation oncology: Gynecological cancers. Springer Heidelberg. New York. 2010: 411-43.
26. Viswanathan AN, Petereit DG. Brachiterapy, Aplication and
Technique: Gynecologic Brachiterapy. Edisi 1. Lippincott
williams & wilkins. AS.2007: 224-50.
27. Burger RA, et al. Human papillomavirus type 18: association with poor prognosis in early stage cervical cancer. http://www.ncbi.nlm.nih.gov/entrez/ query.fcgi. J natl Cancer Inst. 1996; 2,88 (19): 1361-8.
28. Young RC, et al. General Principles of cancer therapy. In: Berek JS, Adaashi EY, Hilard PA. Novaks Gynecology.12nd
29. Belia JA. The radiobiologic basic for radiation therapy. Gynecologic Oncology. 2
ed. Baltimore: Williams & Wilkins, 1996: 1015-20.
nd
30. Malloy C, Sherris J and Herdman C. HPV DNA Testing: Technical and Programmatic Issues for Cervical Cancer Prevention in Low-Resource Settings. Path, 2000.
ed. McGraw Hill Inc. Singapore 1993: 109-18.
32. Sulistyo B. Evaluasi Respon Radiasi Klinik pada Penderita Karsinoma Epidermoid Dibandingkan dengan Adenokarsinoma Serviks Uteri Stadium III 4 Bulan Pasca Radiasi Lengkap. Laporan penelitian. Kedokteran Universitas Diponegoro. Semarang. 2004. 11-15
33. Qinghua F, et al. Evaluation of Transported Dry and Wet Cervical Exfoliated Samples for Detection of human Papillomavirus Infection. Journal of Clinical Microbiology, 2010, 48; 3068-72.
34. Gravitt Pe, et al. Human Papillomavirus (HPV) Genotyping using Paired Exfoliated Cervicovaginal Cells and
Paraffin-Embedded Tissues to Highlight Difficulties in Attributing HPV Types to Specific Lesions. Journal of Clinical Microbiology, 2007, 45; 3245-50.
35. Carvalho NO, et al. Comparison of HPV Genotyping by Type Specific PCR and Sequencing. Mem Inst Oswaldo Cruz, 2010, 105; 73-8. 36. Lai CH, et al. Clinical implication of
human papillomavirus genotype in cervical adeno-adenosquamous carsinoma. European Journal of Cancer (2013) 49. 633-41.
37. Andrijono. Kanker Serviks. Divisi onkologi Departemen Obstetri dan Ginekologi Fakultas Kedokteran Universitas Indonesia. Jakarta 2012. Edisi ke 4: 113-17.
38. Faradina D. Histerektomi Radikal pada Kanker Serviks di RSUP. H. Adam Malik Medan. Departemen Obstetri dan Ginekologi Fakultas
Kedokteran Sumatera Utara.Tesis 2009.
39. Mamarzadeh S, Natarajan S, Dandade DP, Ostrzega N, Saber PA, Berek JS. Lymphvascular and perineural invasion in the parametria: a prognostic factor for early stage cervical cancer. Obstet Gynecol 2003; 102: 612-19.
40. Sahil MF, Edianto D. Penatalaksanaan Kanker Serviks di RSUP H Adam Malik dan RSUD Dr Pirngadi Medan Selama 5 Tahun (1 Januari 1996 sampai dengan 31 Desember 2000). Departemen Obstetri dan Ginekologi FK USU/RSUP H Adma Malik Medan. Majalah Kedokteran Nusantara. Vol 39 No 1. Maret 2006: 16-20.
41. Chen RJ, et al. Influence of histologic type and age on survival rates for invasive cervical carcinoma in Taiwan. Gynecol Oncol 1999; 73: 184-90.
42. Loizzi V, et al. Chemoradiation:A new approach for the treatment of cervical cancer. Int J Gynecol Cancer. 2003: 13: 580-6.
43. Hong JH, et al. Comparison of clinical behaviours and responses to radiation between squamous cell carcinoma and adenocarcinoma/ adenosquamous carcinomas of the cervix. Chang Gung Med J 2000; 7: 396-404.