Abstrak
Tuknk stres adalah suatu kelainan akut mukosa saluran cerna akibat berfugai kondisi patologis, nkalnya tumor otak, trduma kepalç operasi otalç lulabaknr, pasiendengangagalorgan ganda, strokdanlnin-lain.Tulukstespadapenderitastrokbelum banyakdiselidiki. Makalah ini melaporlran hasil penelitian prevalensi tukak stres pada penderita strok Dilakukan penelitian pada 77 penderita strok pada korteks dan subkortel<s. Strokbanng otak dikeluarkan dari penelitian. Diagnosis strok ditegakkan berdasarkan pemeriksaan CT scan, sedangkan diagnosis tul<ak stres ditegakkan berdasarkan pemeriksaan endoskapi dengan nrengikuti prosedur standar. Prevalensi tula.k
stres pada penderita sffok henoragik 47,7%, pada penderita strok iskenik 18,4%, dan secara keseluruhan 33,6%. Perbedaan antara prevalensi tukak stres pada penderita strok he,noragik dan penderita strok iskemik secara statistik berbeda bennakna 1x2
:
7,02,p
:
0,0085), risika terjadinya tukak stres pada penderita strok hetnoragik lebih tinggi secara bernakna dibanding penderita
stok isketnik
dengan OR -- 3,88 (1,25 < OR < 12,44).Abstract
Stress ulcer is definedas anacute uwcosallesion ofthe upper gastrointestinaltractcaused by anindirect influence ofseveralpathological situations such as brain tumor, severe burn, patients with utultiorganfailure and stroke. Many investigators have reported the prevalence of stress ulcer anong patienrc with stroke. This article
will
report the result of endoscopic exarnination among patients with strolce. Seventy-seven patients with cortical and subcortical stroke have been exanined by nteans ofendoscopy. Diagnosis ofstroke was made b), CT scan exantination and stress ulcer was diagnosed by endoscopic exanination according to a standardprocedure. The overall prevalence of stress ulcer anong patients with stroke was 33.6%, i.e. 47.7% anong patients with henorrhagic stroke and 18.4% auong patients with ischaenic stroke. The dffirence in prevalence of stress ulcer benveen these nio groups was statistically significant(x
:
7-02, p
:
0.0085). The risk of stress ulcer anong patients with haenorrhagic stroke was higher than patients with ischaetnic stroke (OR:
3.88, 1.25 < OR < 12.44).Keywords.' stres.s
ulcer, stroke
I7O
DaWiyono et al.Prevalence
of
Stresss
Ulcer Among Patients
with
Stroke
Daldiyono*,
Dadang
Makmun *, Yusuf Misbach**,
S.M. Lumban
Tobing**
Stress
ulcer
isdefined as
an acute mucosal lesion of theupper gastrointestinal
tract,
predominantly
in
the
stomach
and
duodenum,
as
a
result of
several
pathological conditions such
as
brain tumor,
severeburn, patients
with multiorgan failure, and stroke.l'2,3
Eventhough
the lesionsof
this
acute mucosal damageare
not
always ulcerated,
these
conditions are still
included into
theterm
of stress
ulcer.4Stress
ulcer must be differentiated from
acute
uppergastrointestinal
lesions causedby
somedirect noxious
agents such as_salicylate andnonsteroidal
anti-inflam-matory
drugs.5MedJ Indones
e
beenreported
from
3
Doig
und Shufur,6
ngsby Kitamuras
andWe
will
report
theresults
of the
endoscopic
examina-tions on stroke
cases from theDepartment
of
Neurol-ogy,
Dr. Cipto
Mangunkusumo
Hospital
Jakarta.METHODS
Seventy-seven
stroke
cases have beenendoscopically
examined.
Only stroke
of
the cortex and
subcortex
were
included in this study.
Stroke
of
the
brain stem
wasexcluded
becauseof
the clinicalconditions
which
wererelatively
contraindicated
for an endoscopic
pro-cedure.
The diagnosis
of
stroke
was confirmed
by
computed tomography
(CT) scan
examination.
*
Divisiotr of Gastoenterology, Departnentof
Medicine,Faculty of Medicine University of Indonesia,/Dr. Cipto Man-gunkuswno Hospital, Jakarta, Indonesia
**
Departnent of Neurology, Faculty of Medicine lJniversityof
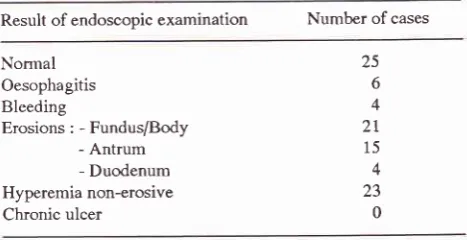
Normal Oesophagitis Bleeding
Erosions : - Fundus/Body - Antrum - Duodenum Hyperemia non-erosive Chronic ulcer
Vol.S, No.3, July - Septenber 1996
Endoscopic examinations were
performed
according
to
a
standard
procedure as usual, after obtaining
awritten informed
consentfrom
thefamily.
Ethical
clearance
for
the
investigation
was
issuedby
the
Research
Ethical Committee
of
the Faculty
of
Medicine University of
Indonesia
Jakarta.RESULTS
The
result
of
theendoscopic examinations is reported
in Table
1.Table
l.
Result of endoscopic examination on 77 stroke casesResult of endoscopic examination Number of cases
Stress
IJIcer I'll
statistically different
thanin
ischaemic stroke (47.7
%vs
18.4%,xz ='7.O2,p
=0.0035).
Thedifference of
theprevalence
of
stress
ulcer
between haemorrhagic
stroke and ischaemic stroke cases
being
sosignificant,
indicated
that
haemorrhagic stroke
could
be
con-sidered
asa risk factor
in
the
development
of
stressulcer
(OR
=3.88;
1.25 <OR
<
12.4).The prevalence
of
stressulcer
in
this report differed
from
those reported
by other investigators,
Segawagreported the prevalence
of
92%
stressulcer in
stroke
cases, where as 45%of
them proved- to bewith
mucosalbleeding of
the stomach.Kitamurat in t975
reported
aprevalence
of
52%
for all
of
the stroke
cases.The
difference
might
be dueto
theallocation of inclusion
criteria. This investigation was only done on
stroke
cases at thecortical
andsubcortical levels,
whereasin
the investigations
of
Kitamura
and
Segawaall
stroke
cases,
including
stroke
of
the
brain
stem, were taken
into
consideration.
The difference
of
the
prevalence
of
stress
ulcer
be-tweenhaemorrhagic
stroke cases andischaemic stroke
cases
could be explained
as
follows. Bleeding is
al-ways accompanied
by catecholamine release,'* which
Dromote
vasoconstriction
of
the microcirculation
of
ihe gastric
-.r"osa,ls
and theblood
in
theintracranial
space
lead
to
an increaseof
the
intracranial
pressure'The
increaseof
the
intracranial
pressureactivate
thehypothalamus-pituitary-qdrenal
axis
and
the
autonomic nervous
system. l6Acknowledgment
The
authors
would
like to
thank
Prof.Dr.
Sumarmo
Markam
for
his
permission and guidance
during
this
investigation,
and also
to the
nurses
for
their kindly
help
in
preparing
theendoscopic examinations.
REFERENCES
1. Robert
A,
Szabo S. Stress ulcer. In : Selye H, ed. Selye's, Guide to stress research. New York Scientific and Academic Editions, 1983:'22-46.2. Schiessel R, Feil W, Wenzl E. Mechanism of stress ulcera-tion and implication for treatment. Gastroenterol Clin North Am 1990;
l9:l0l-20.
3. Dalgaard JB. Cerebral vascular lesions and peptic ulceration. Arch Pathol 1959; 69: 359-70.
4. Levine BA. Stress ulcer. [n: Cheli
&
ed. Gastric protection. NewYork:
Raven Press, 1988: 1344.5. Robert
A,
KauffmanGL.
Stress ulcer.In
: Slaisenger,
Fordtran eds. Gastrointestinal disease:
pathophysiology, diagnosis, management,3rd
ed. Philadelphia: Saunders, 1975:42-8.6. Doig J, Shafar A. Gastric haemorrhage in acute intracranial vascular accident. Quart
I
Med 1956; 25:l-19.
25 6 4
2t
15 4 23 0Note : More than one type of lesion may be encountered in the same
The
description
of thefindings
concerning stressulcer,
specified
in
haemorrhagic
andischaemic stroke
casesrespectively, is shown
in
Table
2.Tab\e2.
Stress ulcer in 77 cases olstroke, specified in haemor-rhagic and ischaemic strokeType of stroke Stress
ulcer
PrevalenceHaemorrhagic Ischaemic 44 37 19 7
4'7.7 % 18.4Vo
Total 33.6
x2 ='7.02 p = 0.0085 OR = 3.88 (1.25 < OR < 12.44) Yatcs' correction x2 = 5.80 p = 0.016
DISCUSSION
As
shown
in
table
I
the majority
of
lesions
were
located
in
thefundus
andbody
(21 cases), andinvolv-ing
the
antrum (15
cases). Thesefigures
representedthe
characteristics
of
stress
ulcer which have
been reportedin
ot
asbrain operation
andhead
trauma
o'll
and also
in
burn
cases
(Curlin
The
overall
prevalenceof
stressulcer in this
investiga-tion
was 33.6%, whereas in haemorrhagic strokeit
was [image:2.595.35.269.256.376.2]172
Daldiyono et al.7. Jura E. Gastrointestinal disturbances in stroke. Acta Neurol Scand 1987; 76:168-71.
8. Kitamura
I
ItoKL.
Acute gastric changes in patient with stroke I. With reference to gastroendoscopic finding. Stroke 1976;7:460-3.9. Segawa K, Nakazawa S, Chujo H. The upper gastrointestinal lesions associated
with
the
cerebrovascular accident. Proceeding trI APCDE, Taipei, 1980: 33-6.10. Cushing
H.
Peptic ulcers and interbrain. Surg Gynecol Obstet 1932; 551-34.11. Brown TH, Davidson PF, Larson MG. Acute gastritis
occur-ring within
24 hoursof
severe headinjury.
Gastrointest Endosc 1989; 35: 37-40.12. Friesen SR. The genesis of gastroduodenal ulcers following bums: An experimental study. Surgery 1950;28: 123-58.
Med J Indones
13. Pruitt BA, Folley FD, Moncrief JA. Curling ulcers: A clini-cal- pathology study
of
323 cases.Ann
Surg L97O; I72: 523-36.14. Gann DS. General body response to trauma. In: Schwart GR,
Safar
P,
StoneIH,
et
al
eds. Principles and practice ofemergency medicine 2nd ed. Philadelphia: Saunders, 1980:
t64-69.
15. Omadani
H,
KamisakiY,
Itoh
T.
Stress-induced gastric mucosal lesions and changes in amino acid metabolism dueto the activation of the sympathetic nervous system in rats.
Yanago Acta Medica
I99l;34(l):37
-52.16. Feibel
I,
KellyM,
LeeI,
Woolf P. Loss of adrenocorticalsuppression after brain injury: Role of increased intracranial pressure and brainstem function. J Clin Endocrinol Metab