VOL.
1 ,NO.
1,zotj
ISSN
No.9772337712005
Joutnal
of
Ageing
and
Development
LIST
OF
CONTENT
1.
"Explorations
of
Challenging
Issues
for
Japan's
Acceptance
of
Indonesian
and
Filipino
Nurses
and Care Workers:
Outcome
of
Quantitative and Qualitative
Surveys
in
Japan and
the
Sending
Countries"
Shun
Ohno...
...
....1
"Gene
Collagen
I
Alphal
Polymorphism
and Osteoporosis
Risk
in
Indonesian Postmenopausal
Women"
Lindawati
S.Kusdhany, Elza
lbrahim, Dwi
Anita
Suryandari,
Tri
Budi Rahardjo, EefHogervorst, Christopher
Talbott.
....
. . . . .. ...17
"Effects
of Isoflavones in Tempeh on Postmenopausal Syndromes"
Diah
M. Utari,
fumbawan, Hadi Riyadi,
Muhilal,
Purwantyastuti...25
2.
3.
"The
Association
of
of
Teeth
Mobility"
Farisza
Gita,
Muslita
Elin
Hediana..
...
..Mandibular
Bone Density
LeYel
with
the Degrec
Indrasari,
Lindawati
S.Kusdhany,
13
"The Clinical
Profile
of Hospitalized Etderly
Patients
with Delirium
in Immanuel
Teaching
Hospital Bandung"
Vera,
Abram
P.Tanuatmadja,
Yuvens
Ricardo
Wibowo...40
"The
Association of
Calcium Intake
and
Nutritional
Status
with
Bone
Density
of Density of
Elderly
Women
in
Primary
Health Center
IV
South Denpasar,
Bali, Indonesia"
K.Tresna
Adhi,
D.Puspitasari, W. Weta,
N
K.Sutiari,
N.W.Rapiasih...
46
The Association ofCalcium Intake... I iADp ,
The Association
of Calcium Intake
and
Nutritional
Status
with
Bone Density of
Elderly
Women
in
Primary
Health Center
IV
South Denpasar,
Bali,
Indonesia
K.Tlesna Adhi, D. Puspitasar i,
N.K.
Sutiari,N.W. Rapiasih
Abstract
Osteoporosis is a metabolic bone disease which is common and highly co(elated with
age, Ieading to disruption or change in bone shape and increases risk
ofbone
fractures, thereby disruptingor linliting
daily activities. which catl ultimately include death. This research aims 10 determine the adequacyofthe
lcvelof
calciurn :ntake and nutritional status on bone density in elderly Balincse uomen. The research was observational,with
a cross-sectional design usirlg simple random sampling.
A
totalof
64 women aged 45years and above were taken as the study sample. Results showed that 95.3 per cent
ol
elderly women indicated
a
calcium intake lessthan
100 per centof
RecommendedDietary
Allowances(RDA). with a total
calcium
intakeof
an
averageoI
107.76 mg/day. The Body Mass Index(BMl) of26
in 40.6 per cent ofrcspondents wasnormal-Qualitative bonc density measuremcnt indicated
that
havinglow
bone dens;ly waslbund in
4l
(64.1 per cent) respondents. Thcre was a significant relationship betweencalcium
intake and nutritional statuswith
bone density (p<0.05). Recommendations includegiving
information about consumptionof
high-calcium food sourccs and also increasing physicalactivity
and exerciscto
help absorptionof
nutrientsfrom
lood consumed to improve bone mineral density.Keywords: Calciunr Intake, NutritionalStatus, Bonc Density, Eldcrly Women
Abstrak
Osteoporosis adalah penyakit metabolik tulang yang umum dan sangat berkorelasi
dengan
usia, yaog
menyebabkan gangguanatau
perubahanbentuk tulang
serta meningkatnyarisiko
patahtulang,
sehingga mengganggu atau membatasi kegiatan sehari-hari, yang pada akhirnya dapat menyebabkan kematian. Penelitianini
bertujuanuntuk
mengetahuiapakah
kecukupantingkat
asupankalsium
dan
status
Bizi berpengaruh pada kepadatantulang
pada perempuan lansiadi
Bali.
Penelitian ininrerupakan
penelitian
observasional, dengan desain clossseclional
menggunakansimple random sanzpling. Sebanyak
64
perempuanberusia
45 tahun keatasdipilih
sebagai sampel penelitian. Hasil penelitian menunjukkan bahwa 95,3 persen perempuan
usia
45
tahun keatas menunjukkan asupan kalsium kurangdari
100 pers€n Asupan KecukupanGizi (AKG),
dengan asupan kalsium total rata-rata 107,76 mg/hari. IndeksMassa'lubuh (BMI)
dari
26
di
40,6 persen rcsponden adalah normal. Pengukuran densitastulang kualitatif
menunjukkan respondenmemiliki
kepadatan tulang yang rendalr, ditemukan pada4l
(64,1 persen) responden. Ada hubungan signifikan antara asupan kalsium dengan statusgizi
dengan kepadatan tulang (p<0,05).
Rekomendasi termasuk memberikan infonnasi tentang konsumsi sumber makanantinggi
kalsiumI hc Asoc:,rion olCalcium lnrdke... I lADp
serta mcningkatkan aktivitas
flsik
dan olahraga untuk membantu penyerapan nuirisidari rnakanan yang dikonsumsi untuk menirgkatkan kepadatan mineral tulang.
Kata
Kunci:
Konsumsi Kalsium, Status Gizi, Kepadatan Tulang, Lansia PerempuanIntroducfion
According 10
the
Centml
StatisticsAtcncl
(BP5r, the nlmber
ol
elderll
irrIndonesia
has
increasedsignificantly.
In2007 the total
population included
18.96rnillion
cldrlll
rll.0l
per
(crl
r(siJiJ
inBali)
and this number increased by 7.73 per cent in 2009. lndonesian women's lifeexpectancy
is
longer
than men,
with
a subsequenthigher
frequency
of
elderlywomen coinpared
to
lnen.Life
expectancyofthe
populationolBali
in
2000 was 68.1 years$ith
an increase to approximalely 70.5years
in
2006.12This figure is
rvell
above the national figureof66.2
years.Based
on
data from
DenpasarCity
Health Office, in 2010 the number
ofelderly
in the city
of
Denpasar counted for as much as 8.39 per centofthe
total
population. In2011, there was
a 22.32
perccnt
increase comparedto
the
year 2010. The
PrimaryHealth Center
IV
South Denpasarin
2010 showed that the proportionofelderly
people was 8,39 per cent- The proportionofelderly
increascd
in
the
years2011
to
22.36
per cent,With
an increase irr age. arr increasingnumber
of
elderly
affects many aspectsof
life
due
to
tlle
change
in
the
physical.biological,
psychological,social, and
the emergenceof
degenerative diseases causedby
the
ageing
process.
One
of
thesedegenerative
morbidilie.
is
6.1q6p6,at1,.According
to
rhe lnlernarional Osleoporosi.Foundation
(2007).
osteoporosis
is
aconditioll
characterizedby
a rapid decreasein density and thinning
of
bone tissuc. RiskI-aclors
lor
oseoporo:is
irrchrdc gcnctic..being a woman, the presence
ofchronic
health
problems.
hormone
deficiency,alcohol. smoking
and
lack
ol
exelcise.Calcium
intake
also
contributes
tomaintainine
bone tissue
along
lite, padicularly among the elderly.Several studies in Indonesia fbund that
the
risk
lactors
tbr
osteoporosis included lack ofexelcise. poor nutritional status(BMI
<18.5), cafleine intake, calcium intake <70 per cent Reconnnended Dietary Allowances
(RDA)
anci age2
55 years.6'7 r0rr'r5-r7 on
this
basisit
is
importantto
do
researchto
determine
the eflecl
of
calcium
intake andnutritional status on bonc density ;n Balinese older women.
Methods
This study was an observational study
using
a
cross
sectional
design.
Thepopulation
were 865 clderly
women
\rr'ho cn|ollcd in 2011. Sdmplccrireri.
ue|r
being women aged 45 years and above enrolled inthe
Primary
Healtlr
Center
IV
South Denpasarin
2011,without
abno.malitiesof
the spine or paralysis and beingwilling
to beinterviewed.
The selected samples werc 64 women aged 45 years and above, using thc sampling technique
of
simple random sampling. Thedata
coilection
was
done
by
tracing
theprimary data
collectedthrough
interviewsabout
the
respondents'
characteristicsincluding nanre, age and educational level. Meanwhile,
to
determine the calcium intake,qualitative and quantitative interviews were
conducted
usi0g
semi-quantitative
Food Frequency Questionnaire (SQ-FFQ).Nutaitional status
of
respondents was assessedby
usingBody
Mass Index(BMI)
defined as the
weight in
kilograms dividedThe Association oi Calcium tntate-..
i
t,qn,,I
by
the
squareof
the
height
in
meters (kg/m'?).Weighl
was assessed using digitalscales
accurateto
0.1
kg.
Height
was measuredwith
microtoice stature meter thathad
0.1 cnr accuracy-
Bone dcnsity wasnreasured
using
the
Bone
DensitomettyAchilles
Express.
Statistical analysis was done using computer soltware and analyzed usingChi
Square Tests, $'ith a p-valueol5
per cent to establish significance.Results
The
researchwas
conductedon
64wonen
aged 45 yearc and above who were enrolled in the pd$/d77.1r, or who visited thePrimary
llealth
CenterIV
South Denpasar.Table
I
provides
thc
distribution
of
respondents
based
on
their age
andedLrcation Ievel.
Table 1. Distributiod of Respondent Characterisdc
Bas€d on Age and Education L€vel
Recommended
Dielao
Allo\^ances (RDA) ot 800mg/i6y
'Tabl€ 2. Th€ Distribulion ofCalcium lnlake. Nutritional Statui, and Bone Denlity
alnong Respondents
Calcium Intake Inw (< R-DA)
Normal
(:
RDA)6l
3
(e5.3) (4.8)
6 (e.4)
5t 179.7) 7 (10.9)
Bone Density
Low(<-r
)Noflnal
(:
-l
)23 (35.9)
4l (64.1)
Table
2
sho$s
that
most
oI
the respondents havea
normal nulritional status(79.7 per cent), reflected
by
a
noflnal BMI.lheir
bonc density was assessed qualitatively using the Bone Densitonetry and showed that most respondents had low bone density (64.1pl]r cent.). Age
45-59 yr
60-69 ],r
r70)n
Education Level
No schooling
Primary
lunior and senior high school Bachelor Degree
Distribution of
r rJ (2rJ.l) l5 (s4.7)
1t (17.2)
j9 (60.9)
12 (18.8)
7(n
0) 6 (e.4)g*
550
540
From the results
of
the dcscriptive analysrs presentedin
Table
I,
it
is
clearthat
most respondents were in in the age groupof
60-69 years (54.7 per cent) with the majorityof
them
not
havingany
schooling (60-9 percent).
Measurementof
dietary
calciumintake
ol
respondenrs\\3,
mecJured usingSemi
Quantitative
Food
FrcquencyQuestionnaire
(SQFFQ).
For
complete results we reler to Table 2.The respondents' level ofcalcium intake was mostly
low
(95.3 per cent consumedit
below the RDA) with an average totalcalcrum intake
of
107.76 mdday, whichis
belowof
Asecteso es (yed)
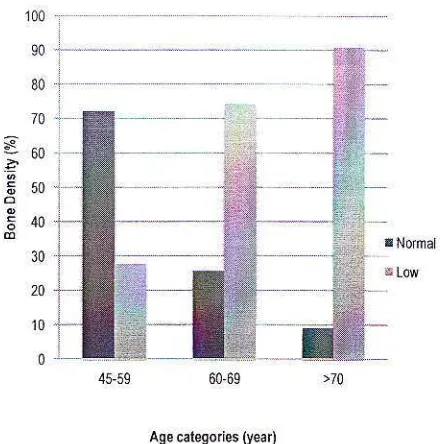
Figure
l
Dis.ribution ofBone Densi$ Based on AgeBody Mrss Ind€x (BMl)
UndeNeigh(<18.5 ks/N-)
Normal (18.5-25 kg/m:) Overweishl (>25 ks/ntr)
The Association of Calc;um
Intake.-Figurc
I
shows
the
distribution
of
bone density bascd on respondent's age. 11 showsthat an
increasing ageof
the
respondents increasesthe
risk
oi
a
decline
in
boneden.ir1.
lhi.
change in bone (onrposilion ithus
a
result
of
the
ageing
process!ol-alternatively,
depcnds
on thc
particularlable
J
shor\s
lhdl
lo$
c.rl.iurnintake cortributes to low bone density where
nonnal level
decreasesthe
risk by 68
per cent. For anal),tical purposes, the ntltritionalsrctu\
i(
calegorzed
inlo
l*o.
calegorrcsnormal
{BMl:
18.5-
'5
kg/rn't and
notnormal
(underweight/overweight (BMI:
<18.5 kg/m'?and
>25
kg/m'?,respeclively)-Chi
square
test
results
showed
that respondentswilh
low weight were 9.1 limesmore
li(cl)
lo
hir\e
lou
bone
densitl conpared \\,ith respondcnts who had normal nuLntioncl\lJru\.
lhis
nrean5 Ihal lhcrei'
asignificant
association between nutritionalstatus and bone density.
Tabel
3.
Bivarintc
Analysis of Bone Density Based on Calciumlntakc
andNutritional
Status
Bone Density CI
Variable Nornral
'Total
X)
n
(rer
cent
n(per
cenl)
n (Per cent)Low
UpCalcium Intake
I-ow
4l(
100.0)
20(87.0)
6i(95.3)
0(0.0) 3(13.0)
3(4.7)
5.611 0.018
0.328
0.229
0.470Normal
4r(r00.0)
23(100.0Nutritional
StatDsNot
nornrl
Nornul
2e170.1)
22(9s.7)
5l(79.7)
s.653
0.017 9.103
1.099
75.382Total 4 r(
r00.0)
23(100.0)
64(100.0)Discussion
According
to
experts,
to
avoid osteoporosis, one must go through a process that startsfiom
early prevention.A
diet thatcan lead to
osteoporosis
involves consumption ofless calcium and unbalancednulritional
intake.talcium
d<ficienc1is
asituation where
the
concentrationof
totalcalcium in scrunr ofless than 8.5
mg/dl
(2-2mmol/L) or when calcium ion levcls are less
than
1.0
rnmoVL.ra
Calciurn
deficiency occurs during periodsof
rapid bone growth {modelingrunlil peal
bone mass andi(
veryinfluentialon a person's bone
fragility.")
Consuming enough calcium every day
is very impoftant
to
assjst the establishment and maintenance ofstrong bones. Asideliom
beirrga
precursorof
bone, calcium tsalso
important
for
some
other
bodylinctions. lfyou
donot
consume enough calcium every day as a result, the bodywill
take calcium
from the
bones.This
is
what causes osteoporosis-In
additionto
adequate cak iurn intake. rhebodl
also needs vilaminD3, which needs to be sufficienl
for
optimal calcium absorption to take place. This is best synthesized during sun exposure rather thantte taken in sunlight.
According to a study
that
1|
minutes adc1 of srrn exposure uas qufficienl lo sustain
bone
mass.6
Sports activities such
aswalking. jogging,
aerobics
and
physical exercisewith
weighls
canalso be
usedto
prevent
osteoporosis.
In
people
with
The Association of Calcium tntake... I Jrule
osteoporosis,
this
can slowdown bone loss, but exercise can also provide the mechanicalstimulation
of
n]uscle contractionon
the spine and other padstlut will
stimulate boneLess mobility
can
accelerate
andexacerbate ostcoporosis-
However.
for
patients with osteoporosis
it
is recommendednot
to
exercise exoessivelyto
avoid
thcoccurrencc
of
fractures.
Another
factoraffe.ting
lheIe\cl. ot
calcium in plastnair
lhc
rario
aal
in
lood. ldcall).
calcium intake should be in the same rangewith
theconsumption
of
phosphorus(P),
and
theratio
ol'P:
Ca:
I.5:
I
may be acceptable. Butiftlle
ratio is more than 2:1, especiallyil
calcilrm intake
is
low. this
will
hav.-negalive influences
which
can cause bone demineralization.eIt
is
estimaledthal
this
may
be oneimportant
factor
in
the
developmentof
ostcoporosis,a
phenomenonthat
decreasesbonc
denrit) and
min<ralization.
lhii
iscommon
with
an increasing age, especiallyin
postmenopausalwomen.e
To
preventosteoporosis,
smoking,
dlinking
coflee.alcohol and
soft
drinks should be reduccd. Insterd.elderl)
shorrld locus L,n consuminBa
high
calcium-conlainingfoods
such asanchovies, shrhnp rebon, beans, tempeh or
dri:rking milk.615
Poor
nutritional
statusil]
the
elderlv can be due to:l.
Decreased
basal
melabolisrn.where
caloric
needs
decrease resulting in overweight/obesity;2.
Reduced physical activity resulting in overweight/obesity;3.
Economic prosperity,
food
con-sumption becomes excessive, the
result tends
to
be
overweight/ obesitYl4. Taste
loss,
eating
becomesuncomlortable
and
decreasesappetite, resulting
in
elderlybecoming malnourished (consum-ing less protein energy);
5.
Periodontal disease (teeth),result-ing
in
difliculty
eating
fiber (vegetables, meat) anda
tendencyto
eat soft
foods
(high
caloric), resulting in overweight/obesity;6.
Dccrca'ein ga'tric
acid secrerionof
digestive enzymesand
food,interferes
with the
absorption {r1' r itamins arrd rnirrrlals. rcsuhing indeficiency of micro nutdents;
7-
Decreased
bowel
nobility,
resulting in constipation, so elderly
olien
sufler
liom
hemorrhoidswhich can cause bleeding and lead
to anemia:
8.
Frequent useof
drugsor
alcohol.this
can
decreaseappetite
tlmtcauses malnutrition and hepatitis or liver canccr;
q.
Di.orders ol-mororslills.
rc.ukingin
dilficulties
lbr
thc
eldcrll
irrpreparing
their
own
food
andbecoming malnourished;
10.
Less socializing
and
lonelinessr p.1cho
lngical chJnge\i
resuhtngin
decreased
appetite
andmalnutrition:
I1.
Decreased revenues(retire),
foodcon\unr|lron
i.
louered
result inSin nralnutrition;
12. Dementia,
rcslrlting
in
i|frequent mealsor
even forgelling
to
eat,which
can
cause obesity
ormalnutrition.o
t
hcsc problcms ineldcrl)
alTect lheirnutritional
status.
that
can
be
obseNedthrough body mass index measurement.
In
this
research
there
was
a
significant associalion be.ween nutritional status andbone density-
Thesedata
suggested thatclinicians and health service providers need
to
provide intensive information about theright diet lbod sources, especially foods high in calcium such as anchovies, beans, tempeh
and
milk.
They
should
also
support increased physicalactivity
to
prevent ihe decreasein
bone density
that
will
help sustain a healthy elderly population.The weakness
ofthis
study is the useof
dietary
assessment, since noneof
thedietary
assessment
methods
ploduces accurate nutrient requirements in the elderlyThe Associatior of Calcium lntake...
because
of
memory deficits that can lead tobias
in
research
resulls.
lrr
addition, measurementsof
nutritional
statusin
thisstudy have
not
been using height predictorelde.ly
(fathoms
long/high
knees/seatheight)
lor
the
people aged60
years and above sothat it
canresull
in
a
biasin
theinterpretation
of
nlrtritional
assessmentof
elderly.6
However,our
data suggestlhat
afocus on maintenance
of
the correct weightby exercising and the correct diet could aid
eldcrll
uomcn
in preventitrg o.teoporosi. in Bali.Acknowledgernent
Thanks 1o Primary
Heallh
CenterIV
South Denpasar stalfand the ANLENE teani
lor
help and cooperationin
data collection and inlormation in this study.PostDenoDausal Osteoporolic Women in North
Wcst
of
lran
Asid Pac.t
Clin N
r'.2009:18(l):4843.
9. r-inder
MC.
Nutt-itioidl Biochentistr an.ltlerarolB,r lakafi!: UI-Prcss. 1992.
r0
.^ltuatsier S. PrksipDasu
n
Cizi (BosicPrnkiple of Ntutitia"). Jakdna:
l'l
CdtudidPustaka t,tamr 2009
11. Litir SC. M4ro clrlic Fdnlil! Hedlth Book Al Fantilt Htolth (nrile J.kn1a:
l''l'
Scholdsli. Jakatu. 2007.Prina4, Healrh Cenler
Moulh
Denpase. Lislof
IHC Hcalth CenlerlV
Elderl)in
Soull'Dcrpsar Yea. 201L
i2.
Prihatini S. MahituwatiVK Jah!fi AB, Sudiman H. Deterninants of Osteoporosis Risk lactou inThB
I'rovinces in
lndonesia hLlp:,' r\Nrllizi
hthans.depkesso il./index.plp. (Accessed: 201l, .,ar6y 20) 2009.
li
Rosenberg AE. Bones, JoinLr .nd Sot l issueTumos. In: Kumar V. Abbas AK. Fausto N, (editots)- Robbnts Pahologi. on.l Contran qali.
,/
Daeara
81h ed. Philadclphia: Satr'idc6 Elsciver. 2005r 1273'03.I4. RLrjiarro
.^.
Pcryakil Nlctabolisne Klki'nn(Hiperkdhenia dar Hipokalsni!) dala'n Ku6us
D6a Metabolislrc Kalsiunr daD Penylkil fulanr
PERKIINI (L\) (Calciunr Melabolisn Disease
(lllpedlcaemia and IlypocdlcaeDia) Ilasic Cou6c in Calciun Melabolism aM Bonc Discdc PIRKENI. (lX)): 2001:l-23.
li
siriburianl'.
h
addilion to Calcnnn. lc'nalel\4enorark i{cquircs Antioxidaxs and Alen 2006.
16. Sudarla$rn S. Pathoecncsis and ClinicalAspcds
or'
Osreopo'osis.Prbli.
Hed|hh
a elia17. Sqono. Khomen A. Setia\rn B. Martianlo D. Sukandar
D
Erect of Milk Againsr thc BodyMass Index And Spinc Dcnsity
of
YourgWonen .to ndl of Nttition und Faad. 2407:2
{ l): I -7.
18. Seojono CH. Bonc Mehbolism
h
Uderl). Dde.l) lnlegraled and Plcnatl'. Ccntcr tbrlnfomution ard Publishine Section of Intcaral
Midicine Faculty
of
Medicirc. Indoncsia. Jakana.2002.I 9. WidiakarF Nalioral Food ard NuLriLion. hdonesiaD R€commended Dielary llos ances
(RDA).2004.
References
L CcntLal Burcau ofstatistics. Residents of Bali. tlc PopulatioD Cens[r 2007. Jatana. 2008.
2 CenrFl Bureau of S1alis1i.s. Residcnts ofEali. tle Populatior Census 2009. Jal,ada. 2010.
:
ll.rll'
Drld,Irfl
.l
Denodsa. lordl PoDuldl ur'.dccordiq 10 the Clasification of Tarsels Dldcrly and Sex per villaee Ycar 2010
iI
the Cil' ol' Derpdar.2010.4
lr"lrl' D(p",1,,r!
,'i Oe p.'d
To 'l Pop lar'on, acco.dnrg b the Clasification ol Tarsels ljlde.ll ,nd Sex per Vilhge Year20ll
iD tlE City ofDenp6ar.2011.
5.Indonesia llealth Deparhcnl. Guidelines for Fllderly lleallh Corchire For Heallh
Off6r
II.Dired$
Ceneratof
Comnrnily Heallh Developnent Jakart4 I 999.6.latmah. Gizi Da.ld Usia Ldnilt (N
htio
in thet/./e/t
. Jakana: lrldDggd. 2010.T lldnono.
M
P,evenanean'{
O\,',LaiaeOr/.opolortr. Jakana: PL$pa Swm- 2004.
5 Hcaz J, Mo\kd.rE J. I'olJh S .nd fbEl,imi-Mamaghdi
M.
Nutilion
Status anrongK.Tresna
Adhi,
D.Puspitasari, W.Weta, andN.K.Sutiari:
SchoolofPublic
Health, FacultyolMedicine,
Udayana UniversityN.W Rapiasih: Sanglah Hospital, Denpasar,
Bali
Corespondence to:
kadek
[email protected]