HIV Prevention through Sexual Transmission Model at the Primary Health Care Level
Pande Putu Januraga; Aang Sutrisna; Vidia Darmawi; Ignatius Praptoraharjo; M. Suharni; Ignatius Hersumpana; Ita Perwira; Swasti Sempulur; Satiti Retno Pudjiati; Eviana Hapsari Dewi
National Library: Catalog under Issuance
HIV Prevention through Sexual Transmission Model at the Primary Health Care Level/ Pande Putu Januraga; Aang Sutrisna; Vidia Darmawi; Ignatius Praptoraharjo; M. Suharni; Ignatius Hersumpana; Ita Perwira; Swasti Sempulur; Satiti Retno Pudjiati; Eviana Hapsari Dewi
Yogyakarta: Center for Health Policy and Management (CHPM) Faculty of Medicine Universitas Gadjah Mada
xiv + 96 pages / 25 x 17 cm First edition, September 2016
1. Sexual Transmission 2.HIV Prevention Model 3. Primary Health Care I. HIV Prevention through Sexual Transmission Model at the Primary Health Care Level
Written with the support of the Australian government through a grant from the Department of Foreign Affairs and Trade (DFAT) to the Center for Policy and Health Management (CHPM), Faculty of Medicine, Universitas Gadjah Mada. This publication does not represent the views of either the Government of Australia or the Government of Indonesia.
All rights reserved.
Any part of the report may be used, reprinted, reproduced, quoted, or cited in any manner through proper citation and for the purpose of community education, not for commercial interests.
For more information please contact the Center for Policy and Health Management (CHPM), Faculty of Medicine, Universitas Gadjah Mada. Suggested citation:
CHPM. 2016. HIV Prevention through Sexual Transmission Model at the Primary Health Care Level. Yogyakarta: CHPM GMU
Copyright © 2016 by
iv
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
Executive Summary
Indonesia is experiencing a shift in epidemic population trends in HIV transmission from injecting drug users (IDUs), followed by direct female sex workers (DFSW), and is now dominated by sexual transmission among indirect female sex workers (IFSW) and men who have sex with men (MSM), including waria. Projections indicate that these key populations will constitute 90% of new infections, that is, 70,000 to 80,000 individuals/per year during the 2014-2019 period. The model-specific intervention to prevent sexual transmission among key populations (PMTS initiative) was developed in 2010 in response to the growing HIV epidemic in Indonesia, unfortunately however, the continuity of the PMTS program has been heavily reliant on financial support from international donors.
This study is a collaboration between the Center for Health Policy and Management (CHPM) Faculty of Medicine, Universitas Gadjah Mada and the Department of Foreign Affairs (DFAT), Australia. Researchers explored the applicability of an integrated services model that would ensure
sustainability of the PMTS program at primary health care level. The study also looked into models of operational policies that would support the implementation of integration. Primary health care level was chosen as the locus of the study considering its function and proven contribution in responding to the HIV epidemic in Indonesia.
The study used a mixed methods approach. A desk review was conducted by compiling references related to HIV prevention through sexual transmission and analyzing
them to subsequently develop a PMTS service delivery model. A questionnaire was developed and was administered by Delphi participants during the meeting. The proposed model shown in this report is the agreement among Delphi participants who are experts and practitioners on HIV in Indonesia.
successfully providing services to high-risk groups, however, this work continues to be informed by global policies and financial support from international donors. The role of public health centres is critical, especially, in the distribution of condoms to high-risk populations, and health promotion targeted to high-risk population groups, as well as the service of antiretroviral therapy (ART) which remains a necessity. Even though this is being carried out, there is still a need for strengthening the capacity of public health centres in the distribution of condoms, in managing STIs, as well as in carrying out voluntary counseling and testing. The two rounds of Delphi survey and post-Delphi discussion conducted with practitioners and experts associated with PMTS concluded that the PMTS model must involve all groups of high-risk populations outside the FSW community and its clients, namely MSM and waria. Further activities should be prepared by considering the differences in epidemic conditions, ability of providers as well as population mapping. In the short term, the role of international donors in funding the activities of PMTS especially the provision of condoms, condom distribution, outreach and education of high-risk groups remains predominant. Integration should be iterated gradually considering the financial capability and commitment of service providers. Furthermore, the results of the survey and post-Delphi discussion also concluded there are 11 specific issues related to the implementation of PMTS activities/ components, especially at the level of current and future service integration which includes
the provision of condoms, distribution of condoms, diagnosis and treatment of STIs at the individual level, screening and periodic presumptive treatment (PPT) with sex workers, circumcision of adult males, HIV testing in public health centre facilities, either through VCT clinics or provider-initiated counseling and testing (PITC) and mobile VCT as an extension of public health efforts targeting high-risk groups, ART services, the promotion of reproductive health and HIV-AIDS to the general population and the continuation of prevailing health promotion activities related to HIV-AIDS high-risk groups.
Consequently, a proposed level of services integration is as follows: (1) a partly
integrated service carried out by others in full coordination with public health centres which provide the bulk of facilities/infrastructure for condom distribution and health promotion services in high-risk groups; (2) integrated services should be coordinated by public health centres along with other parties, with a clear division of tasks and authority particularly in the provision of condoms; (3) integrated services in which financial support and human resources from other parties come from outside the regular funding mechanisms specifically mobile VCT and ART services; and (4) fully integrated services which is routinely carried out by public health centres including the diagnosis and treatment of STIs in individual health efforts, screening and treatment of STIs for FSW, adult male circumcision and finally, health promotion services to the general public.
Ex
vi
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
Table of Contents
Introduction - 1
Background and Rationale - 10 Objectives - 11Integration Frameworks at
The Primary Health Care
Level - 12
Model Development
Approach - 18
Study Design - 18 Desk Review Strategy - 18Desk Review of PMTS
Integration Models at the
Primary Health Care Level
- 20
HIV transmission through unsafe sexual practices in Indonesia - 20
PMTS Model Integrated into Mainstream Services in other Countries - 23 Literature Review of PMTS Policy - 26 Findings from exploration into the practical application of current PMTS program - 33
Desk review conclusions - 38
Generating Consensus
about a PMTS Model
through a Delphi Study - 40
Practitioner Consensus about PMTS Concepts and Strategies - 41 Consensus on the PMTS concepts and strategies from experts - 55Conclusion on consensus and model development - 61
Proposed PMTS Model for
Indonesia - 63
Final Remarks - 69
Conclusion - 69Recommendations - 70
Appendix - 74
Executive Summary - iv
Figure 1. PMTS Service Integration Framework at the Primary Health Care Level - 17
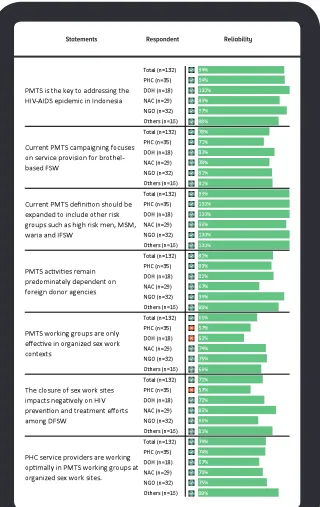
Figure 2. Reliability of the PMTS Definition - 42
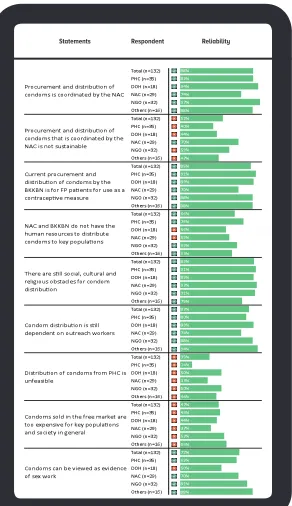
Figure 3. Reliability of condom procurement and distribution strategy - 44
Figure 4. Desirability and feasibility on condom procurement and distribution -
46
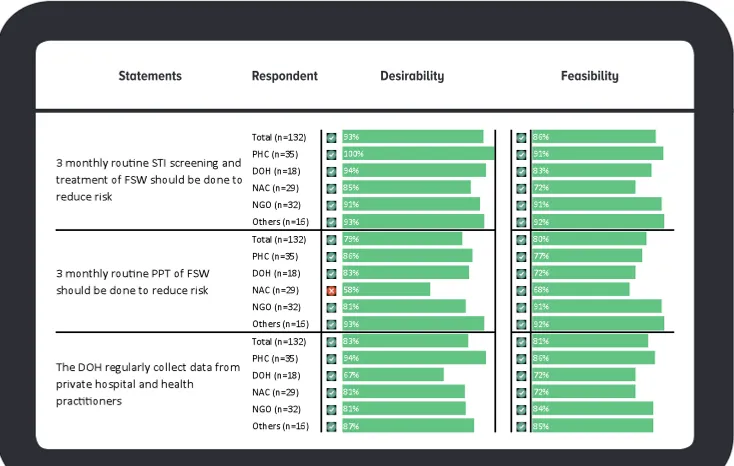
Figure 5. Reliability of STI management - 48
Figure 6. Desirability and feasibility of STI management - 49
Figure 7. Reliability of HIV Testing and Treatment - 50
Figure 8. Desirabilityand feasibilityHIV Testing and Treatment - 51
Figure 9. Reliability on sexual and reproductive health for the community - 52
Figure 10. Desirability and feasibility of STI-HIV prevention education - 53
Figure 11. Desirability and feasibility of the role of implicated stakeholders - 54
Figure 12. Reliability of the PMTS model according to expert cohort - 56
Figure 13. Desirability of the PMTS model according to expert cohort - 59
Figure 14. Feasibility of the PMTS model according to expert cohort - 60
Tabel 1. Sub-System Service Integration Categories According to the Continuum of Integration - 15
Table 2. New HIV Infections in Indonesia - 21
Table 3. Comparative Analysis of PMTS, LKB and WHO Recommendations - 28
Table 4. PMTS LKB Related Services - 29
Table 5. Current and Proposed Sub-System Integration Efforts for PMTS Health Services - 68
List of Figures
/ List of Tables
T
viii
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
ABAT Aku Bangga Aku Tahu/I’m Proud I Know
AIDS Acquired Immunodeficiency Syndrome ANC Ante Natal Care ARV Antiretroviral Drugs ART Antiretrovirals BCC Behaviour Change
Communication BKKBN Badan Kependudukan
dan Keluarga Berencana Nasional/National Population and Family Planning Board CBO Community Based
Organisation
CSO Civil Society Organisations DFAT Department of Foreign
Affairs and Trade DFSW Direct Female Sex Worker DOH Department of Health FP Family Planning FSW Female Sex Worker
GF Global Fund
GFATM Global Fund to fight AIDS, Tuberculosis, Malaria GFNFM Global Fund New Funding
Model
HIV Human Immunodeficiency Virus
IBBS Integrated Biological and Behavioural Surveillance IDP International Development
Partner
IDU Injecting Drug User IEC Information, Education,
Communication
IFSW Indirect Female Sex Worker
KDPA Kader Desa Peduli AIDS/ Village cadres concerned with AIDS
KDS Kelompok Dukungan Sebaya/Peer Support Group
KSPAN Kelompok Siswa Peduli AIDS dan Narkoba/A cadre of students that care about AIDS and drugs
KISS Koordinasi, Integrasi, Sinkronisasi dan Sinergi/ Coordination, Integration, Synchronization, and Synergism
LKB Layanan Komprehensif Berkesinambungan/ HIV Continuum of Care LGBT Lesbian, Gay, Bisexual and
Transgender MOH Ministry of Health MSM Men Who Have Sex with
Men
NAC National AIDS Commission P/DAC Provincial/District AIDS
Commission
NGO Non-government Organisation
NHS National Health System OI Opportunistic Infections OVC Orphans and Vulnerable
Children
PEP Post-exposure prophylaxis PERMENKES Peraturan Menteri
Kesehatan/ Ministry of Health’s Regulation PMK Peraturan Menteri
Kesehatan/ Ministry of Health’s Regulation PHC Primary Health Care or
List of Abbrevations
TB Tuberculosis
UKBM Upaya Kesehatan Berbasis Masyarakat/Community-based Health Effort UKM Upaya Kesehatan
Masyarakat/Public Health Effort
UKP Upaya Kesehatan Perorangan/Individual Health Effort UNAIDS Joint United Nations
Programme on HIV and AIDS
UNAIR Universitas Airlangga/ Airlangga University (East Java)
UNCEN Universitas Cenderawasih/ Cenderawasih University (Papua)
UNDANA Universitas Nusa Cendana/ Nusa Cendana University (East Nusa Tenggara)
UN United Nations
UNUD Universitas Udayana/ Udayana University (Bali) USU Universitas Sumatera
Utara/North Sumatera University
VCT Voluntary Counseling and Testing
WG Working Group
WHO World Health Organisation PICT Provider Initiated
Counseling and Testing PKPP Primary Personal Health
Services
PKMK Pusat Kebijakan dan Manajemen Kesehatan/ Center for Health Policy and Management PLWHA People Living with
HIV-AIDS
PMTCT Prevention of Mother to Child Transmission PMTS Pencegahan Melalui
Transmisi Seksual/ Prevention of HIV through Sexual Transmission PPT Periodic Presumptive
Treatment PR Principal Recipient PrEP Pre-exposure prophylaxis RTI Reproductive Tract
Infections
SIHA Sistem Informasi HIV-AIDS/ HIV-AIDS Information System
SIP/SIMPUS Sistem Informasi Puskesmas/ HIV-AIDS Information System in Public Health Centre SKPD Satuan Kerja Perangkat
Daerah/ Local Government Component Working Unit SPM Standar Pelayanan
Minimal/ Minimum Service Standards
SOP Standard Operating Procedures STI Sexually Transmitted
Infection SUFA Strategic Use for
Antiretrovirals
x
H I V P r e v e n t i o n T h r o u g h S e x u a l Tr a n s m i s s i o n M o d e l a t T h e P r i m a r y H e a l t h C a r e Le v e l
P
r
e
face
I
ntegration of HIV and AIDS response into existing health services has gained significant attention from program administrators, donor organisations and researchers as a feasible concept and strategy to strengthen effectiveness, efficiency, client satisfaction, and sustainability of the response. However, at the implementation level, integration may not be implemented as expected because integration basically demands for negotiation of interests and power owned by various actors. The prevention of HIV through sexual transmission (PMTS) Program is one of programs designed to integrate different actors with different interest and power in a multi sectoral program. Therefore, the implementation of PMTS remains facing obstacles such as establishing a conducive environment, ensuring provision of condoms, encouraging behavioural change, and conducting testing and treatment of STIs and HIV. Due to this dynamics of interaction among the actors in PMTS, assessment and evaluation of the PMTS implementation shall be conducted constantly in order to achieve better result or outcome.The Indonesian National AIDS Commission (NAC) would like to express our appreciation for publication of the PMTS program modelling at primary health service and its networks. Focus in the integration at primary health services is a strategic choice since, historically, the role of primary health services in Indonesia has strong evidence in involving both the community and non-health sectors, and it has also been successful in promoting inter-sectoral collaborations and service integration. It should be aware that the recommended model has considered principles of decentralisation in health sector and regional capacity in providing basic services. Orientation on regional characteristics of the model makes PMTS integration would vary at the sub-national level due to variations of the need of the beneficiaries, capacity of the service providers, epidemic situation, and implementation of main functions of the health system at sub-national level.
This model also emphasizes that integration is not the ends of the service, but as the means to provide a service that are accessible, fair, fulfil the basic needs of the population, and sustainable. by defining integration as such, efforts in strengthening PMTS at the primary service level could strategically contribute to achieve better result and outcome in preventing the HIV transmission through sexual transmission in terms of effectiveness, efficiency and continuity. At the sub-national level, recommendations of the study could be utilized as the guidance for policy makers to enhance the implementation of the PMTS program in their areas.
Jakarta, 30th of August, 2016
Dr. Kemal N. Siregar
Secretary of the National AIDS Commission
xii
H I V P r e v e n t i o n T h r o u g h S e x u a l Tr a n s m i s s i o n M o d e l a t T h e P r i m a r y H e a l t h C a r e Le v e l
In
tr
In order to achieve the common
goal of globally ending the HIV
epidemic, the strengthening
of health systems, specifically
in the planning capacities,
implementation abilities, and
evaluation approaches is
imperative (Yu et al., 2008;
WHO, 2007; UNAIDS, 2015).
Large scale reductions in
donor funding have made
this approach even more
relevant, and in order to ensure
sustainability of programs
and services, the successful
integration of specific HIV
interventions into mainstream
health care systems becomes a
necessity (UNAIDS, 2015).
Background and Rationale
The Continuation of PMTS is the key to halting the HIV epidemic in Indonesia
The HIV epidemic that has lasted for more than two decades in Indonesia is indicat-ing a significant shift in epidemic trends, after initially growing quite rapidly among injecting drug users (IDUs), the epidemic exploded among female sex workers (FSW), which was then feared as an epidemic bridge to the general population (Riono and Jazant, 2004; NAC of Indonesia, 2012). The reality of a full shift in the epidemic to be-coming generalised through unsafe sexual practices of FSW and their male clients have come into question owing to a variety
of surveillance data and mathematical modeling which have showed a significant increase in incidence among MSM (MOH of Indonesia, 2008; MOH of Indonesia, 2013). By observing the accumulated number of HIV-AIDS cases and risky behaviours car-ried out by FSW and MSM groups including
waria, it is apparent that continued focus on these populations are key to tackling the HIV epidemic in Indonesia.
HIV prevention efforts among FSW, MSM and waria have predominantly been facilitated through the global initiative in the form of donor funding assistance which has impacted upon the dynamic development of policies and programs among these populations (Yu et al., 2008; CHPM, 2015). In Indonesia, this influence is clearly visible in the national program design which aligned greatly with donor program modeling. In the 90s, prevention programs focused on strengthening the role of civil society and it was characterized by the growth of various NGOs working in HIV-AIDS response. Then, in the 2000s, strengthening of government institutions was promoted so that these bodies would play a greater role in HIV-AIDS prevention activities, especially in the provision of preventive services at primary and secondary levels, such as STI clinics, VCT and ART service providers. Later, the concept of sustainable and comprehensive services, including the test and treat approach, became a major campaign in alignment with the “90-90-90” UNAIDS campaign (CHPM, 2015).
Irrespective of the approach and dynamics of the HIV-AIDS work among the FSW, MSM and waria populations, interventions have largely focused on preventing sexual transmission of HIV through positive behaviour change activities, including condom promotion and early access to diagnosis and treatment of STIs and HIV. Although health interventions specifically focused on key populations
2
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
have proven to be more efficient to implement, especially in countries with limited resources, several weaknesses persist, among others: 1) the development of multiple systems or parallel systems within the broader health system, 2) funding diversity affecting programming approaches, and 3) the lack of incentives and proper adoption of endorsed health systems, which is considered a particular threat to sustainability (Atun et al., 2010; Suharni et al., 2015). Therefore, a focus on the integration of specific HIV prevention initiatives, especially in high-risk populations, in order to ensure the continuity of services at the grassroots level is increasingly being recommended (Suharni et al., 2015; CHPM, 2015; Atun et al., 2010).
The Need for the Development of a National PMTS Service Model and Associated Policies
How to bring about such integration, and determine what models are appropriate to encourage integration are questions that still need to be addressed (Atun et al., 2010; Frenk, 2009). Based on the results of a series of studies on HIV Policies and Programs within the Health System Framework in Indonesia (which is a joint program between the CHPM and DFAT), it is evident that there are variations in levels of integration and levels of effectiveness of health care coverage. In the context of regional differences, this inconsistency is tangible in the ability and capacity of human resources, including disparities in funding, as well as the magnitude of the problem or differences in the level of the epidemic. The results of study I and II also show that the policies to combat HIV-AIDS, including prevention programs for sexual transmission of HIV (PMTS), were comprised of national and local level policies,
however, the execution of said policies was
problematic (CHPM, 2015; Suharni et al., 2015). Systematic effort is needed within the framework of scientific research to create a model for services, policies and programs that correspond to differences in local capacities and epidemic situations of various provinces in Indonesia. This study is the third activity (III) in a series of collaborative research between CHPM and DFAT regarding policies and programs on HIV-AIDS in the Health System Framework in Indonesia.
Objectives
This study aims to explore two lines of query:
1. What kind of integration model would be able to guarantee the continuation of the PMTS program in Indonesia at the primary health care level?
4
H I V P r e v e n t i o n T h r o u g h S e x u a l Tr a n s m i s s i o n M o d e l a t T h e P r i m a r y H e a l t h C a r e Le v e l
In
tegr
a
tion
Fr
am
e
w
orks a
t
Th
e Primary Health
Car
e L
e
v
Integration Frameworks at The Primary Health Care L
evel
T
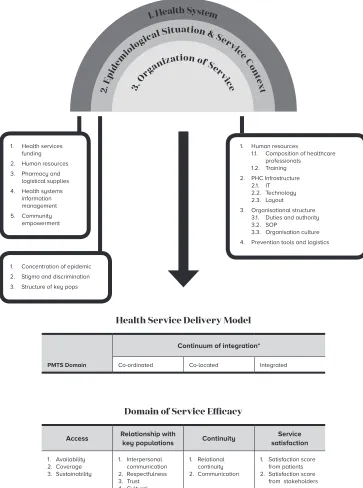
here are two main assumptions in determining the development model of PMTS at the primary care level. The first is the position and important role of primary health care in the national health system, where primary services are placed at the forefront of health care and able to provide comprehensive and essential services, including personal health services and community health promotion, prevention, treatment and rehabilitative activities.1 With such vital position and role,the strengthening of PMTS at the primary health care level will contribute greatly towards efforts to control the HIV epidemic. The second assumption is that owing to the history of the role of public health centres in Indonesia, especially in providing services that involve the community and non-health sectors, and the arguably well executed and managed services provided, they are in an excellent position to lead in the efforts towards integration. Based on the two major assumptions above, the development of the integrated PMTS model at the primary health care level will lead to an increase in the effectiveness of services described within the framework shown in Figure 1, where the integration into the national health system will encourage the implementation of PMTS in order to achieve the desired output of increased access to services, increased coverage and improved quality of service. The output will include positive behaviour change to reduce the risk of STIs and HIV transmissions which will inevitably lead to a decrease in new infections of STIs and HIV.
More specifically, there are 6 main reasons underlying the importance of developing the PMTS program’s integration model at the level of basic services:
1) Peraturan Presiden No.72, 2012, or national legislation endorses an integrated approach.
1. The HIV-AIDS burden is tremendous. It does not only impact on the patient’s health but also on the social and economic welfare of the family. Negative social and economic impacts can be minimized if the transmission of HIV can be addressed, or when transmission has occurred, treatment can be provided as early as possible at the most basic or primary level of service provision or care.
2. The problems of STIs and HIV-AIDS are undoubtedly connected to various other health issues that are often reported in mainstream services, eg. TB and ANC services.
3. Gaps found within the service coverage or within the HIV and STI cascade remain an issue. Surveillance data and results of the study indicated that one of the barriers in the continuity of HIV patient care is access difficulty and convoluted referral systems. The coordinated approach of an integrated PMTS program will help reduce such gaps.
4. Public health centres are found throughout all of Indonesia, therefore, an integrated PMTS approach will help improve access to services.
5. The provision of services at the most basic level would reduce stigma and discrimination. Preliminary evidence suggests that the specialization of services specifically targeting certain populations can actually increase stigma and discrimination towards affected groups.
6. Integration of services at the primary health care level could increase cost-effectiveness.
6
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
there are some major hurdles that must considered to ensure that the proposed model has an adequately strong foundation prior to implementation. The main obstacle in developing an integrated service model is the dominance of donor funding or support from international development partners (IDP), such as the Global Fund (GF), in financing PMTS services and activities. One of the largest components of the funding model from the GF is the financing of human resources. There are two types of health related human resources supported by the grants: firstly, those who work in the government health care system but later received an additional honorarium or salary for conducting HIV-related activities; and secondly, non-civil servant staff recruited by CSOs or NGOs. Therefore, behaviour change efforts at the primary health care level work under separate systems in conjunction with the mainstream health education program (Suharni et al., 2015).
Not only are there differences in the provision of services at the primary health care level, but support services, such as logistical use of medical equipment, and procurement of condoms and lubricants as medical devices for HIV prevention, are also controlled predominantly by the NAC, which functions as a coordinating body outside of official government structures. In other words, the procurement and distribution of condoms is beyond the official procurement system of medical equipment in general (Suharni et al., 2015). Another example is the separation of information/data systems for outreach services and the mainstream national and regional health information
systems. The previous GFATM program was an abundance of health information collated from activities involving outreach programs and the distribution of condoms and lubricants, but this was not reported beyond being used as validation for financial liability and was not used to feed into the planning of health programs. In general, management of the information was not well coordinated and efficient utilization of shared information between the sectors was infrequent (Suharni et al., 2015).
It is vital, therefore, to develop a model capable of addressing these constraints. The approach able to support sustainability of the health system, the epidemic
situation, service providers and the effective implementation of primary care is known as the continuum of integration approach (Blount, 2003; Doherty et al., 1996). The main focus of this framework is to map the integration level of services and activities at the public health centres and among their networks. This approach was appropriated not because it is deemed successful in improving services but rather as a method to provide services that are accessible, equitable and also meet the basic needs of all parties.
Integration Frameworks at The Primary Health Care L
evel
Close collaboration approaching an integrated practice
The level of collaboration and open communication is high . Effectiveness and efficacy of service provision is established, although some aspects of reporting and referral systems remain low.
Full collaboration in a transformed/merged practice
The highest level of integration and a transformed-merged approach applied for the community as a whole. These services are provided to all.
5
6
3
4
Integrated
Services
Co-located
Services
Coordinated
Services
1
2
Minimal collaboration
Services or activities performed in a separate facility using systems different to those of the public health services delivery system. Communication with the public health centre is minimal and dependant on the service needs of individuals and groups.
Basic collaboration at a distance
Services or activities performed in a separate facility from the public health centre and using different systems, but the service providers view each other as mutual sources so as to communicate periodically about the groups or individuals being served.
Basic collaboration onsite
The service is in the same location as mainstream ser-vices, but they either share or do not share the same space. The systems used are still separate but the communication may be frequent. Mutual reconcilia-tion of services or activities are very likely to occur be-cause they are in the same location. Service providers feel as part of a team although its working mechanism is unclear so that decisions regarding the groups or individuals served is still implemented independently by the respective service providers.
Close collaboration with some system integration
8
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
The operational definition of integrated services above can be translated into the definition of a PMTS service model. The results of previous CHPM research on the integration level of HIV-AIDS within sub-system health measures (Financing, Human Resources, Services, Facilities, Management, Regulation, and Information Systems) were categorized into 3 groups: integrated in full (), in part (), and not integrated at all (), subsequently definitions regarding the category of PMTS services integration model with the public health centre was drafted, as shown in the table 1.
The definitions of the practical service integration model can be summarized as follows:
• Level 1: When the service is carried out by others, outside the coordination of public health centres which only receive information sporadically. This level of service, which includes the regulation, management, human resources and financing, functions separately and is not integrated at all within the system at the public health centre, little communication is carried out horizontally on an ad-hoc basis so that it can be categorized as an integrated part.
• Level 2: When the service is carried out in coordination with other parties in public health centres where the regulation and management of public health centres are also actively engaged. This level of service is conducted in a separate area with facilities, human resources and financing not integrated at all with the system at the public health centre. However, the regulation and management of public health centres play a role in the implementation of services, and information is regularly exchanged in writing so that at least the
elements of management, regulation and information are integrated in part.
• Level 3: When the service is carried out in full coordination with public health centres which provide most of the facilities/infrastructure. This level of service is provided simultaneously or in coordination with public health centres although financial and human resources for these services are not at all
integrated with the system at the public health centre. Therefore, there is a need for more intensive communication and information exchange as well as management, facilities, and technical regulations that are partly integrated within the system of public health centres.
• Level 4: When the service is performed by public health centres along with other parties, with clearly defined division of tasks. This level of service is provided jointly by the public health centre in conjunction with other parties both inside and outside the public health centre, though financing is still not integrated with the service financing mechanism of the public health centre. Therefore, at least all the major elements in the sub-system except financing, has been partly integrated with the system at the public health centre.
• Level 5: When the service functions through the help of financial and human resources from other parties outside the regular funding mechanisms. At this level, the technical elements of the service, regulation and management are fully integrated with the system in public health centre excluding elements of human resources and finance.
Integration Frameworks at The Primary Health Care L
evel
Table 1. Sub-System Service Integration Categories
According to the Continuum of Integration
Level of Integration
Financing HR Services Equipment Management Regulation Information
Level 1: Minimal
collaboration
Level 2: Basic
collaboration at a
distance
Level 3: Basic
collaboration onsite
Level 4: Closed
collaboration with some
system integration
Level 5: Closed
collaboration approaching an integrated practice
Level 6: Full
collaboration in a transformed/merged practice
10
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
and is fully integrated with existing mechanisms within the public health centre. At this level, the service has become part of the mandatory services provided by the public health centre and all the main elements in the sub-system level are fully integrated with the system at the public health centre.
Models designed need to consider how these levels of integration can be implemented in public health centres. The first issue is how to integrate both national and regional health systems in support of service delivery, such as in sub health financing system and how financing policy differs at the national and regional levels to ensure financial capability when providing
Integration Frameworks at The Primary Health Care L
evel
Health Service Delivery Model
PMTS Domain
Continuum of integration*
Co-ordinated Co-located Integrated
Domain of Service Efficacy
Access Relationship with
key populations Continuity
Service satisfaction 1. Availability
2. Coverage 3. Sustainability
1. Interpersonal communication 2. Respectfulness 3. Trust 4. Cultural
competence
1. Relational continuity 2. Communication
1. Satisfaction score from patients 2. Satisfaction score
from stakeholders
Figure 1. PMTS Service Integration Framework at the
Primary Health Care Level
1. Health services
funding 2. Human resources 3. Pharmacy and
logistical supplies 4. Health systems
information management 5. Community empowerment
1. Human resources
1.1. Composition of healthcare
professionals 1.2. Training
2. PHC Infrastructure 2.1. IT 2.2. Technology 2.3. Layout
3. Organisational structure 3.1. Duties and authority 3.2. SOP
3.3. Organisation culture 4. Prevention tools and logistics 1. Health System
2. E
pid
em iolo
gical Situation & Serv ic
e C on
tex t
3. O
rganization of Servic e
1. Concentration of epidemic
2. Stigma and discrimination
12
H I V P r e v e n t i o n T h r o u g h S e x u a l Tr a n s m i s s i o n M o d e l a t T h e P r i m a r y H e a l t h C a r e Le v e l
Model De
v
elopm
en
t
Appr
oa
Model Development Approach
Study Design
T
his study used a mixed-methods approach (Johnson and Onwuegbuzie, 2004; Creswell, 2008) in order to collect in-depth and varied information from a variety of sources. A desk review of the issues and strategies of sexual transmission prevention services within the context of the problem, policy, structure and organization of health services in Indonesia was conducted. The desk review results were then compiled into a working paper supported by information gathered from a Delphi study which was conducted to explore the support or consensus of practitioners and experts on the proposed PMTS models. The approach to data collection was a sequential design (Creswell, 2008) wherein the desk review was a major part of the data collection method.Desk Review Strategy
A literature review of the PMTS integration model was conducted to obtain information on three major points: the first is related to the role of sexual transmission in the development of the HIV-AIDS epidemic in Indonesia as well as the various attempts that have been made to mitigate the impact of the HIV-AIDS epidemic. The second literature review was intended to obtain an overview of the various models of prevention of sexual transmission that have been carried out in various countries around the world and to examine how the integration model was instrumental in the success of their implementation. Thirdly, on PMTS policy developments in Indonesia, and on policy that may support and obstruct the implementation of the PMTS integration model.
To provide understanding on the four main topics of review above, the search and analysis was directed to literature on the application and impact of PMTS in Indonesia, PMTS models used in other countries and the factors that influenced the outcomes, as seen from the service organizations, including the role of
integration in the system of health provision, as well as the research strategies implicit in the policy document on PMTS in Indonesia.
Literature research strategy
In order to assess the extent and distribu-tion of the implementadistribu-tion of prevendistribu-tion programs in Indonesia, a review on peer re-viewed publications in international journals was conducted.
14
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
• The epidemic level reported in key populations;
• The magnitude of the problem and an illustration of the risk of transmission through sexual activity;
• The social, political, economic, and policy conditions affecting the issue and descriptions of the risk of HIV transmission through sexual activity;
• If there are intervention settings to reduce or prevent the risk of HIV transmission through sexual activity including specific interventions undertaken, description, duration, comparison, and the presence of co-interventions;
• Characteristics of the study, such as design and duration;
• Participatory study including unit of analysis, number of participants in the intervention group and comparison;
• The impact or outcomes of the studies and interventions;
To complement the results of the study of peer reviewed literature, reports on case studies of activities in several cities in Indonesia were used to add the latest information on the application and outcomes of the impact of PMTS activities in Indonesia. PMTS case studies were conducted in Medan, Surabaya, Bali, East Nusa Tenggara and Papua. These case studies were conducted in different key population groups, including MSM and FSW.
Literature research strategy
and analysis of PMTS in other
countries
In order to obtain information on the delivery of care, a literature review was
conducted on peer reviewed articles from the PubMed database with the key words: ((vertical[Title/Abstract]) OR (horizontal[Title/ Abstract]) OR (integrat*[Title/Abstract]) OR (coordinat*[Title/Abstract]) OR (co-ordinat*[Title/Abstract]) OR (link*[Title/ Abstract])) AND ((program*[Title/Abstract]) OR (care[Title/Abstract]) OR (service*[Title/ Abstract]) OR (delivery of health care, integrated[MeSH Terms])) AND ((HIV[MeSH Terms]) OR (STDs[MeSH Terms])). The search resulted in 3524 articles which were refined and resulted in 861 identified abstracts. Ultimately, 28 full text articles were downloaded and 22 were reviewed.
Scope of the literature covers three main topics, namely:
• Regional settings or areas of intervention, care delivery system settings and population or target groups;
• Specific interventions into the health system, description, duration, comparison, and the presence of co-interventions;
• The impact or outcomes of studies and interventions;
• The level and quality of integration including leadership and governance, financing, planning, service delivery, monitoring and evaluation;
• The policy setting or contextual factors: continuity or sustainability, prospect or opportunities, and the willingness for integration or desirability.
Indonesian PMTS policy
research strategy
Model Development Approach
were unstructured with more emphasis on knowledge of documents available to the public.
16
H I V P r e v e n t i o n T h r o u g h S e x u a l Tr a n s m i s s i o n M o d e l a t T h e P r i m a r y H e a l t h C a r e Le v e l
Desk R
e
vie
w of PMTS
In
tegr
a
tion Models a
t
th
e Primary Health
Car
e L
e
v
Desk R
eview of PMTS Integration Models at the Primary Health Care L
evel
HIV Transmission Through
Unsafe Sexual Practices in
Indonesia
H
IV-AIDS through sexual transmission in Indonesia was to begin with widely reported to have developed among FSW, particularly from the 90s until the 2000s and this is detailed in a report on Surabaya (Joesoef et al., 1997). The rate was reported as an approximate of merely 0.2% (Ford et al. 2000a), but was reported to be much higher in the study by Januraga et al. (2013) with a prevalence of over 15% among direct FSW and 6% among indirect FSW in Bali in 2010.Although in the early development of the epidemic HIV prevalence among female sex workers was reported to be very low, several studies reported a potential epidemic outbreak among this group, due mainly to the high incidence of STIs such as syphilis and gonorrhoea (Joesoef et al., 1997; Joesoef et al., 1998; Ford et al., 2000a). In addition to the high incidence of STIs, studies in the 90s and early 2000s also reported risky behaviours especially in the DFSW population, such as the high number of clients per day and low use of condoms (Wirawan et al., 1993; Fajans et al., 1995; Ford et al., 1995; Ford et al., 1998; Sedyaningsih-Mamahit, 1999; Ford et al., 2000a; Basuki et al., 2002). Surprisingly enough, more recent publications reported a high incidence of STIs in nine provinces in Indonesia as well as 70% inconsistent use of condom (Tanudyaya et al. 2010). In the same year, Majid et al. (2010) reported an increase in the incidence of syphilis in DFSW in nine cities in Indonesia from 2005 to 2007 (8% -14%).
Although the focus of reporting or publications were initially concerned with the potential of an HIV epidemic outbreak among DFSW, the role of male customers of
sex workers started to emerge in the early 90s as presented by Fajans et al. (1994, 1995) and Setyaningsih-Mamahit (1997). Another study reported a lack of customers’ knowledge on STIs and HIV, a high number of sexual partners, low rates of condom use and a high number of respondents reporting symptoms and signs of STIs. Interestingly, not much was found on the client’s role in sexual transmission of HIV affecting the development of the HIV epidemic in Indonesia after the 90s. Searches related to this only found one study by Davies et al. (2007) that reported fairly high positive antibody findings of HSV-2 in men who visited STI clinics in Indonesia.
In early 2000, publications began reporting on the progress of the epidemic among MSM and waria. For example, that of Joesoef et al. (2003), which showed a high incidence of sexually transmitted infections among waria in Jakarta, which was subsequently supported by the Pisani et al. study (2004). Recent studies have reported a high incidence of HIV among waria and the emergence of an HIV epidemic among MSM in Indonesia, especially Jakarta. The study by Prabawanti et al. (2011) reported a high prevalence of HIV (24%), syphilis (27%) and rectal gonorrhoea or chlamydia (47%) in Java. More recent studies related to the increased incidence of HIV associated with the development of sexual transmission in MSM and waria in Bali have been published by Januraga et al. (2013), and subsequently in Jakarta by Safika et al. (2014). In Bali, the research reported an increase in HIV prevalence among MSM and waria, while the research in Jakarta which reported on patterns of risk behaviours of MSM and
waria showed that condom use among MSM
18
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
the density of sexual networks is of serious concern.
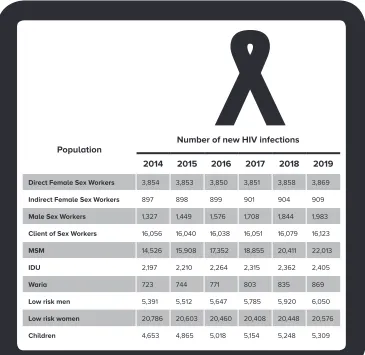
Sexual transmission continues to dominate the pattern of HIV transmission in Indonesia with an indication of increase in HIV prevalence in MSM populations and sero-discordant couples. Transmission of HIV through sexual activity is the main cause of HIV in Indonesia. Estimates and projections of the HIV epidemic shows that 90% of 70,000 to 80,000 new HIV infections per year in 2014 -2019 occur through sex,
whereas transmission through the exchange of non-sterile injecting equipment is only 3%, and 7% through transmission from mother to baby.2 This estimate is consistent
with the percentage of the risk factors of reported AIDS cases at the end of 2015, namely 80% heterosexual, 8% homosexual (MSM), 4% of HIV-positive mother to child, and 3% IDU.3 Therefore, the current PMTS
2) Kemenkes RI (2016). Laporan Perkembangan HIV-AIDS Triwulan IV Tahun 2015.
[image:31.482.60.425.99.454.2]3) KPAN (2014). The Case for Increased and More
Table 2. New HIV Infections in Indonesia
Population
Number of new HIV infections
2014 2015 2016 2017 2018 2019
Direct Female Sex Workers 3,854 3,853 3,850 3,851 3,858 3,869
Indirect Female Sex Workers 897 898 899 901 904 909
Male Sex Workers 1,327 1,449 1,576 1,708 1,844 1,983
Client of Sex Workers 16,056 16,040 16,038 16,051 16,079 16,123
MSM 14,526 15,908 17,352 18,855 20,411 22,013
IDU 2,197 2,210 2,264 2,315 2,362 2,405
Waria 723 744 771 803 835 869
Low risk men 5,391 5,512 5,647 5,785 5,920 6,050
Low risk women 20,786 20,603 20,460 20,408 20,448 20,576
Desk R
eview of PMTS Integration Models at the Primary Health Care L
evel
program model has been developed for high-risk and vulnerable groups (PMTs guidelines NAC, Permenkes No. 21 of 2013, as well as LKB guidelines for 2014).
The focus of literature in peer reviewed publications originating from Indonesia is on interventions that have been developed to control the epidemic among FSW, MSM and waria. The development stage of the PMTS program in Indonesia concentrated on behavioural interventions and general treatment of STIs followed by a more specified treatment of the STIs discovered.
The development of behaviour change interventions using a direct outreach approach to the population of female sex workers and their clients is based predominantly on studies conducted in Bali, especially by Yayasan Kerti Praja, a local pioneering NGO which still bring about impact upon policies at both local and national levels. Outreach activities employing field staff on duty to educate and distribute condoms at FSW sites for clients and pimps were first reported by Ford et al. (1996). Follow up studies were conducted (Ford et al. 2000a) by collecting additional data associated with the incidence of STIs and HIV post behaviour change intervention following the diagnosis and treatment of STIs including syphilis, chlamydia, gonorrhoea, herpes and HPV. The study reported an increased knowledge and behaviour change regarding condom use, although the numbers remained quite low at under 60%. STIs were also reported to be high among FSWs in Bali owing to the high number of male clients and high level of mobility.
In relation to behaviour change strategies, several models employ the use of peer educator programs, as reported in a study undertaken in Denpasar, Bali (Ford et al., 2000b). Intervention involving peer educators recruited from FSW who
Strategic Investment in HIV in Indonesia.
were supervised to educate and distribute condoms resulted in increased knowledge and consistent condom use in locations where peer educators stayed for over 6 months of intervention. The main obstacle of this intervention strategy is the high proportion (50%) of peer educators who are no longer in the same sex work site after six months of intervention. There was also a lack of information on the reporting processes of peer educator performance and its monitoring and evaluation method.
Challenges and obstacles in the devel-opment of behaviour change interventions and management of STIs among DFSW was also reported in two publications by the same author in Jakarta (Setyaningsih-Mamahit, 1997; Sedyaningsih-(Setyaningsih-Mamahit, 1999). Both articles explain in detail the social environment as well as the locus and structure of power relations that affect deci-sions made by FSW in accessing prevention services and having a preventive attitude. They also elaborate on the role of agency, such as personal motivation, in the decision to enter the sex industry as well as various personal problems including relationship issues as influential in decisions related to prevention. The role of social structure and other factors in influencing STI and HIV pre-vention behaviours were reported in a more recent research conducted by Januraga et al. (2014) in Bali. The location and mobil-ity of the FSWs plays a role in increasing susceptibility towards the transmission of STIs and HIV. The role of social structure found in various working environment and how it relates to differences in condom use by FSW in Mataram, Lombok, was also reported by Safika et al. (2013).
20
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
(gonorrhoea and chlamydia) was lower in FSWs who had received at least one dose of periodic presumptive treatment. In addition to implementing PPT, studies in two areas in Central Java and Bintan discussed the implementation of STI syndromic management. Another biological survey of ten cities in Indonesia reported a significant relationship between low prevalence of syphilis and PPT (Majid et al., 2010).
Search results on peer reviewed articles published internationally did not find studies on PMTS interventions or ways to integrate activities into primary health care level. This was because the search was limited to the English-speaking international database. Indeed, although there are many research reports and evaluation studies undertaken, these were not entirely suitable for this literature review.
21
22
H I V P r e v e n t i o n T h r o u g h S e x u a l Tr a n s m i s s i o n M o d e l a t T h e P r i m a r y H e a l t h C a r e Le v e l
PMTS Model
In
tegr
a
ted In
to
Mainstr
eam Servic
es
in Oth
er C
oun
PMTS Model Integrated Into Mainstream Services in Other Countries
T
he literature search indicates that there are not many international publications that directly present the results of activities, strategies or models for integrating prevention services into mainstream primary health care services. Available publications discussing the integration of services generally focus on two or more service-specific interventions, such as integrating STI, HIV and Hepatitis into one integrated service, as reported by (Flanigan et al., 2010; Chow et al., 2009; Fenton et al., 2014). Other publications discuss two or more health interventions, for instance, the integration of sexual health services or reproductive health with HIV testing services and or treatment of HIV (Phakathi, 2009; Lusti-Narasimhan et al., 2014; Delvaux et al., 2011) and Syphilis screening services with HIV services in a large-scale program funded by donors (Avahan) in India (Parthasarathy et al., 2013). There are also publications that report on the integration efforts of family planning services with HIV prevention with indicators of improved contraceptive use and a decrease in unwanted pregnancies (Kosgei et al., 2011).Filtering and analysis only revealed three articles that specifically reported on the integration of STI or HIV into mainstream primary health care services (Banwat et al., 2009; Pfeiffer et al., 2010; Price et al., 2009). The three publications were entirely derived from information on generalized epidemics in Africa. Of the three articles, only one reported on the integration of specific health interventions such as STI treatment based on symptoms (syndromic case management) with primary health care services (Banwat et al., 2009).
Integration activities at the public health centre level is done primarily through staff training on STI and HIV management, clini-cal management and laboratory
strength-ening and referral systems and integration with ANC services. One concern highlighted in the implementation of integrated ser-vices was the increasing burden on primary services which may bring about a decline in quality and reduced access to existing ser-vices. This, however, is unproven because a strengthening of the internal capacity, would bring about an increase in access to services. In addition, integration can bring about an increase in the responsiveness of health workers and an improvement in referral systems facilitating the transfer of patients between services (Pfeiffer et al. 2010; Price et al., 2009).
In order to support the successful integration of HIV prevention programs into primary health care services, it is necessary to increase the performance of health system components, such as financing (Price et al., 2009), human resources, pharmaceutical supplies and medical devices (Pfeiffer et al., 2010). The results of the study did not describe the role of effective leadership and governance, planning, and monitoring and evaluation in successful integration. Publications analysed also under-reported the influence of policy environment and sustainability issues.
24
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
Biomedical Prevention Services within PMTS
1. The provision, promotion and distribution of condoms. Consistent condom use is a highly effective way to prevent sexually transmitted infections including HIV at the individual level. Some important things to note regarding this service are:
• The need to increase availability and accessibility;
• The need to improve knowledge, acceptance and demand;
• Increased access to ART services could increase the need and opportunity to accelerate the promotion of condoms.
2. Voluntary circumcision for adult men. This service can reduce the risk of HIV transmission in men up to 50-60%. Some important things to note in the implementation of this service are:
• It must be part of a comprehensive range of services (including HIV VCT, STI management, promotion of safe sex and condom provision);
• It must be performed in particular regions - WHO recommends areas where HIV prevalence in the general population is more than 15%;
• It is a short-term intervention to accelerate prevention efforts.
3. Testing and counselling for HIV. This is an entry point for ART medication, treatment, care and support for people living with HIV that can reduce the possibility of transmission in discordant couples.
4. Diagnosis and treatment of STIs. Although it is a biological marker of risky sexual behaviour and a factor in increasing the risk of HIV transmission, many clinical studies have not found a decrease in new HIV infections as a result of STI diagnosis and treatment services. Some important things to note in the implementation of this service are:
• In areas with concentrated HIV epidemics focusing on high risk populations, the focus is the population most at risk, people who come with complaints of STI, people with HIV still engaging in risky behaviours, and other at risk populations (teenagers, migrant and sedentary workers who actively engage in sexual intercourse). Meanwhile, the focus of the type of services includes:
• diagnosis and treatment of STI infection in the genitals and anus for women and men with risky behaviour.
• presumptive treatment or STI screening for women and men with risky behaviours.
• In areas of concentrated HIV epidemic, the focus of the population also includes people who have undergone HIV testing and counselling as well as sexually active adolescents. While the focus of services is coupled with interventions on sexual partners of people with STI symptoms such as abnormal fluids found in the genitals, urethra, or anus. 5. Antiretroviral treatment (ARV) based prevention, which includes:
• Post-exposure prophylaxis (PEP) through the provision of zidovudine within 72 hours after exposure. This effectively decreases the possibility of transmission to people exposed to the HIV virus.
• ART medication given (Treatment as Prevention) as early as possible to reduce the possibility of HIV transmission through sexual intercourse by more than 90% in discordant couples, and
PMTS Model Integrated Into Mainstream Services in Other Countries
Behaviour Change Services within PMTS
6. Behaviour Change Interventions/Communications (BCC) stand-alone to reduce the risk of sexual transmission of HIV through multiple communication channels such as:
• The media – the results of several studies generally show the positive impact of BCC
through mass media, with an increase in knowledge and risk perception as indicators.
• BCC at the community level, such as campaigns and mobilization, has proven to
increase the coverage of HIV testing and condom use.
• Good interpersonal communication with peers, health workers and outreach workers. A
recent meta-analysis found that interpersonal communication coverage had a significant association with increased knowledge and use of condoms.
• Information can be designed for those who engage in sex with multiple partners,
commercial sex workers, teenagers, and about a range of other issues.
26
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
Structural Support within PMTS
8. Reformation of rules and policies to reduce stigma and discrimination against people living with HIV and marginalized populations who are most at risk.
9. Programs focusing on gender mainstreaming and gender-based violence. 10. Economic empowerment and other multi-sectoral approaches.
27
28
H I V P r e v e n t i o n T h r o u g h S e x u a l Tr a n s m i s s i o n M o d e l a t T h e P r i m a r y H e a l t h C a r e Le v e l
Lit
er
a
tur
e R
e
vie
w of
PMTS P
olic
Literature R
eview of PMTS P
olicy
T
he prerequisites for effective control of HIV and AIDS are a sense of direction and political commitment. This is often reflected in constitutional and statutory regulations, as well as in executive policy and sectoral elements. Without clear policy, there is no standardization or means for determining objectives, no definition of means of achieving those objectives, and no politic-bureaucratic motivation to achieve them. The government’s commitment to control HIV and AIDS can be gauged from the codification and articulation of policies related to HIV.In Indonesia there is no basic policy in the form of legislation that is a coherent strategy for HIV and AIDS prevention. The existing policies are sectoral, vertical and strongly influenced by foreign grants. Most of the existing legislations are still determined by the executive authority of government. HIV and AIDS are often viewed as merely a health problem. Therefore, an analysis was conducted to review existing policies and technical guidelines as well as other references regarding effective service models in PMTS.
Assessment and analysis of rules and guidelines on the administration of health services enables us to gain an overview of general and specific policies in the health sector and organisation of various health services administration of the PMTS program at the primary health care level. A literature review was conducted by analysing the following policy documents in order from the highest level to those relevant to the objectives of this study.
Understanding of the HIV situation is the first prerequisite in developing HIV strategies and control programs. In addition to understanding the epidemic context, reflection must be undertaken on what has been done, and the costs required to achieve certain targets. Regulation of the
Minister of Health (PMK) No. 21 of 2013 Article 7 and 8 state that one of the duties and responsibilities of the local government is to determine the status of the HIV epidemic in the region. At the state level, in line with the criteria of the UNAIDS-WHO documents issued by the Ministry of Health and the National AIDS Commission, it is reported that the HIV epidemic in parts of Indonesia has been concentrated in several key populations since 2002,45 and has
entered into a generalized epidemic in two provinces of Papua since 2006.6
Various efforts to control and prevent HIV-AIDS have been carried out by the Indonesian government, ranging from the innovative program of Harm Reduction in 2006;7 prevention of transmission through
sexual activity (PMTS) starting in 2010;8
strengthening the Prevention of Mother to Child Transmission (PMTCT) in 2011;9
Sustainable development Comprehensive Service (LKB) at the public health centre in 2012;10 to the most recent breakthrough,
the Strategic use of ARV (SUFA), which began mid-2013.11 Some guidelines for the
integration of STI and HIV services with other health services have also been issued by the Ministry of Health as Technical Guidelines for Clinical Governance Co-infection of TB-HIV in 2012, along with the National Action Plan for TB-HIV 2011-2014 and 2015-2019; Reproductive Health
4) Kemenkes RI (2003). Laporan Estimasi Nasional Infeksi HIV pada Orang Dewasa Indonesia Tahun 2002. 5) KPA (2005). Country Report UNGASS 2003-2004 6) KPAN (2007). Rencana Aksi Nasional Penanggulangan HIV dan AIDS di Indonesia 2007-2010
7) Keputusan Menteri Kesehatan Nomor: 567/Menkes/ SK/VIII/2006
8) KPAN (2010). Pedoman Program Pencegahan HIV Melalui Transmisi Seksual (PMTS)
9) Peraturan Menteri Kesehatan Nomor 51 Tahun 2013 10) Kemenkes (2012). Pedoman Layanan Komprehensif HIV-IMS Berkesinambungan (LKB)
11) Surat Edaran Menteri Kesehatan Nomor 129 Tahun
30
HIV Prevention Through Sexual T
ransmission Model at The Primary Health Care L
evel
Programs in Integrative Services and Primary Service Level in 2001; and Service Guidelines for the Integration of RTI / STI services, and the Early Detection of Cervical Cancer and Breast Cancer in 2014.
The Ministry of Health Strategic Plan 2015-2019 placed HIV and AIDS as one of the priorities for infectious disease control with related performance indicators and targets as follows:12
1. Impact indicators in the form of: a. increasing efforts to improve health promotion and community development, as well as the financing of promotion and prevention activities; and b. increasing efforts to improve hygiene and general health.
2. Outcome indicators such as HIV prevalence of 0.46% (2014) to <0.50 (2019).
3. Performance indicators such as an increase in the percentage of HIV cases treated (number of PLWHA undergoing ARV treatment) / (number of PLWHA eligible to start ARV therapy) x 100%) from 42% (2014) to 55% (2019).
Regulation of the Minister of Health (PMK) Number 21 of 2013 on HIV and AIDS in Chapter IV states that HIV and AIDS prevention activities include:
1. Health Promotion to improve knowledge, to prevent transmission of diseases and to eliminate stigma/ discrimination through public campaigns for the use of condoms, promotion of health in adolescents, and other integrated health promotion activities in adolescent health care, reproductive health services and family planning, antenatal care testing, STI service promotion, drug rehabilitation, and tuberculosis testing and treatment.
12) Keputusan Menteri Kesehatan Nomor: HK 02.02/ MENKES/52/2015 tentang Rencana Strategis Kementerian Kesehatan tahun 2015-2019
2. Prevention
a. PMTS with 4 integrated activities: i). increased stakeholder involvement; ii). behaviour change intervention to reduce vulnerability; iii). improvement in procurement and distribution of prevention tools to ensure availability; and iv). STI prevention activities (diagnosis, treatment and behaviour change counselling)
b. Prevention of HIV transmission through non-sexual modes c. Prevention of transmission from
mother to child
3. HIV testing
4. Treatment and Care 5. Rehabilitation
The PMK No. 21 of 2013 in the NAC PMTS Program Guidelines 2010 is still limited to services and activities for FSW. Components / main pillars within the guidelines, its purpose, and its main indicators include:
1. Enhancing the role of stakeholders to create a conducive environment, with the main indicator of establishing “functioning working groups” that can coordinate with the Department of Health and BKKBN in the provision of condoms / lubricants.
2. Behaviour Change Communication so that HIV vulnerability is reduced through qualified “peer educators” .
3. Condom supply management to ensure that condoms and lubricants are always available and that there is “ease of access and availability of condoms and lubricants”
Literature R
eview of PMTS P
olicy
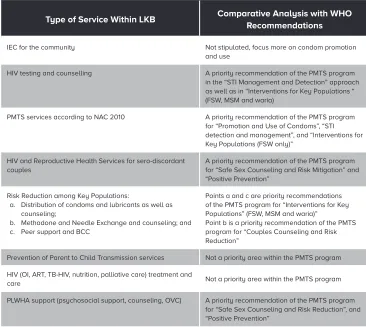
The impact of the PMTS program for FSW is estimated to only affect a third of the projected new infections of 2014-2019. The results from projections of the HIV epidemic in 2012 and IBBS in 2011 and 2013 indicate that the spread of HIV through sexual transmission will be more common in MSM.
[image:44.482.56.422.312.639.2]All components / pillars of the NAC 2010 PMTS guidelines are accommodated in the comprehensive services outlined in the STI-HIV MoH 2012 LKB Guidelines. LKB Guidelines also include all health services and activities recommended by WHO as
Table 3. Comparative Analysis of PMTS, LKB and WHO
Recommendations
Type of Service Within LKB Comparative Analysis with WHO
Recommendations
IEC for the community Not stipulated, focus more on condom promotion
and use
HIV testing and counselling A priority recommendation of the PMTS program in the “STI Management and Detection” approach as well as in “Interventions for Key Populations “ (FSW, MSM and waria)
PMTS services according to NAC 2010 A priority recommendation of the PMTS program for “Promotion and Use of Condoms”, “STI detection and management”, and “Interventions for Key Populations (FSW only)”
HIV and Reproductive Health Services for sero-discordant couples
A priority recommendation of the PMTS program for “Safe Sex Counseling and Risk Mitigation” and “Positive Prevention”
Risk Reduction among Key Populations:
a. Distribution of condoms and lubricants as well as counseling;
b. Methadone and Needle Exchange and counseling; and c. Peer support and BCC
Points a and c are priority recommendations of the PMTS program for “Interventions for Key Populations” (FSW, MSM and waria)”
Point b is a priority recommendation of the PMTS program for “Couples Counseling and Risk Reduction”
Prevention of Parent to Child Transmission services Not a priority area within the PMTS program HIV (OI, ART, TB-HIV, nutrition, palliative care) treatment and
care Not a priority area within the PMTS program
PLWHA support (psychosocial support, counseling, OVC) A priority recommendation of the PMTS program for “Safe Sex Counseling and Risk Reduction”, and “Positive Prevention”
health sector priority interventions. The list of types of services in LKB and their status according to WHO recommendations can be seen in the table 3.