MORTALITY IN SUB-SAHARAN AFRICA?
EVIDENCE FROM MICRO DATA
Masayuki Kudamatsu IIES, Stockholm University
Abstract
Does democracy help babies survive in sub-Saharan Africa? By using retrospective fertility surveys conducted in 28 African countries, I compare the survival of infants born to the same mother before and after democratization to disentangle the effect of democracy from that of changes in population characteristics, which is infeasible with country-level statistics on infant mortality. I find that infant mortality falls by 1.2 percentage points, 12% of the sample mean, after democratization in the post-Cold War period. Relevant aspects of democracy appear to be the combination of multiparty elections and leadership change. (JEL: O15, O55, P16)
1. Introduction
Does democracy promote development? Despite a large number of empirical studies of this question, the evidence remains inconclusive since it is difficult to establish causality running from democracy to development: democracy is likely to be endogenous to socio-economic factors that also affect development (Lipset 1959). As democracy at the national level is clearly not randomly assigned across countries, the empirical challenge is to disentangle the effect of democracy from other confounding factors to the largest possible extent. This paper revisits this question in the context of human development in sub-Saharan Africa. Specifically, I investigate whether the democratization sweeping the region in the 1990s has reduced infant mortality. For
The editor in charge of this paper was Stefano DellaVigna
Acknowledgments: The previous version of this paper was awarded the 9th Moriguchi Prize by the Institute of Social and Economic Research at Osaka University. I thank Maitreesh Ghatak, Tim Besley, Robin Burgess, and Oriana Bandiera for numerous comments and encouragements at various stages of this research project. I am also grateful to the editor, anonymous referees, Wiji Arulampalam, Iwan Barankay, Aimee Chin, Stefan Dercon, Esther Duflo, Ray Fisman, Nicola Gennaioli, Hiro Ishise, Hisaki Kono, Rocco Macchiavello, Ted Miguel, Rohini Pande, Torsten Persson, Steve Pischke, Emilia Simeonova, and seminar and conference participants at Warwick, IDE-JETRO, Pompeu Fabra, SITE at Stockholm School of Economics, IIES at Stockholm University, ISER at Osaka University, University of Hong Kong, the 4th Development Economics PhD Seminar (Namur), CSAE Conference 2007 (Oxford), and Royal Economic Society Conference 2007 (Warwick) for helpful suggestions and discussions. Sylvia Meek kindly guided me through the public health literature. Christina L¨onnblad provided me with editorial assistance. Financial support from the ERC and Handelsbanken’s Research Foundation is gratefully acknowledged.
E-mail: [email protected]
Journal of the European Economic Association December 2012 10(6):1294–1317
c
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1295
this purpose, I use a cross-country micropanel dataset covering 28 countries in the region to remove confounding factors arising from demographic changes.
How to confront underdevelopment in sub-Saharan Africa is one of the most important questions in economics today. Very few people, however, have paid attention to the impact on people’s lives of a wave of democratization experienced by the region since the early 1990s. It might be for this reason that the pessimism as concerns the quality of African government is deeply entrenched in any debate on African underdevelopment. Thus, the long-standing question of whether democracy promotes development gains additional importance in sub-Saharan Africa.
As a measure of development, this paper focuses on infant mortality, defined as death within the first year of life. The survival of infants remains a huge concern in sub-Saharan Africa today, with nearly one in ten babies still dying before his or her first birthday in 2005 (see Web Appendix Figure A1). In addition, focusing on infant mortality has a methodological advantage: unlike other socio-economic outcomes such as personal income, data at theindividuallevel across many countries over a long period of time are available from the retrospective fertility survey component of the Demographic and Health Surveys (DHS). In these surveys, women of childbearing age report when their children were born and whether, and when (if applicable), they died. As surveyed women in Africa on average give birth to four children during their lifetime, I observe a sizable number of mothers having babies both before and after democratization. This characteristic of the data allows me to estimate the effect of democratization by exploiting within-mother variation in the survival of babies, instead of cross-country or within-country variation. As a result, the estimated effect of democratization on infant mortality is robust to the possibility that changes in the composition of the population over time drive both democratization and changes in infant mortality with no direct relationship between the two.
cases, there is no such reduction in infant mortality in countries where the dictator holds multiparty elections and stays in power by winning them or where leadership change takes place in a nondemocratic way.
Due to the lack of appropriate data, I cannot provide conclusive evidence on the mechanism through which democratization has reduced infant mortality. However, suggestive evidence shows that democratization was associated with an increase in the use of some of the health inputs known to be effective in reducing infant mortality, while its association with affluence appears to have been absent. Case studies from two democratized countries suggest that democratically elected new governments indeed changed public health policies to improve maternal and child health care.
This paper contributes to the large empirical literature that tries to identify the effect of democracy on development or other socio-economic outcomes. I am not aware of any studies using micro panel data to estimate the effect of democracy.1 Using country-level statistics, Ross (2006) finds no association between democracy and infant mortality. This finding may be subject to confounding factors at the country level, however.
As an attempt at disaggregating a blunt concept of democracy in the estimation of its effect, this paper is also related to works summarized in Persson and Tabellini (2006). Miller (2008) looks at a particular aspect of democracy—the enfranchisement of women—and finds that this aspect of democracy reduced child mortality in US states in the early twentieth century.
The rest of the paper is organized as follows. The next section presents two country case studies to motivate the present study. It also explains how I measure democracy in sub-Saharan Africa, discusses causes of democratization and their implications for empirical analysis, and then describes the individual-level data on infant mortality. Section 3 describes the empirical method and reports the main results. Section 4 provides suggestive evidence on possible pathways from democratization to the reduction of infant mortality. Section 5 concludes the paper.
2. Background and Data
2.1. Country Case Studies: Zambia and Nigeria
Multiparty election for presidency was reintroduced in 1991 for Zambia, where opposition parties had been banned since 1972, and in 1999 for Nigeria, where military officers had successively ruled the country since 1983. In both cases, the former dictator stepped down and a new president took office. The new government in Zambia embarked upon “possibly the most radical and far-reaching reform of the health sector in sub-Saharan African region” (Lake and Musumali 1999, p. 254). In Nigeria, “the new democratic government has been eager to use the windfall (from
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1297
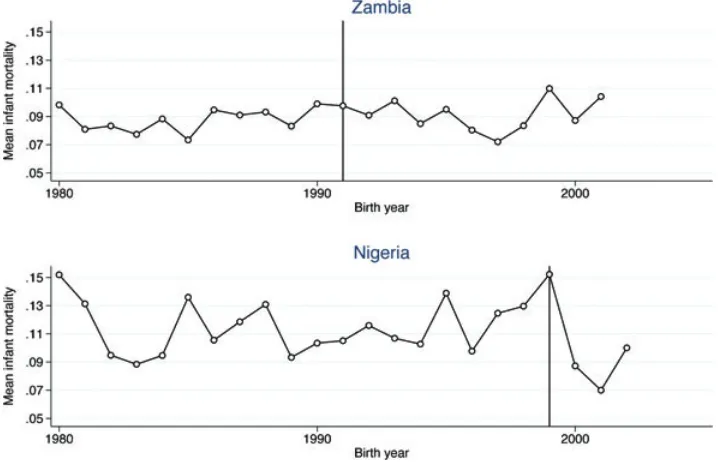
FIGURE1. Annual mean infant mortality rates in Zambia and Nigeria. Plotted are the sample mean infant mortality rates by the year of birth for babies born to those mothers giving birth both before and after the year of democratization (1991 for Zambia and 1999 for Nigeria), indicated by the vertical solid line in the figure. Babies born within a year before the survey are dropped from the sample. Sources: Zambia Demographic and Health Survey in 2001 and Nigeria Demographic and Health Survey in 2003.
oil exports) to deliver so-called ‘democracy dividends’ to the people. In particular, spending on primary health care has increased substantially” (Das Gupta, Gauri, and Khemani 2004, p. 7).2Figure 1 shows the average annual infant mortality rates for babies born to those mothers giving birth both before and after democratization in these two countries. Nigeria sees a clear drop in infant mortality. For Zambia, the pattern is less clear-cut, but the long-run increasing trend appears to be reversed shortly after the year of democratization.3
These two episodes might be exceptions. Figure 1 may be contaminated by confounding factors. In the analysis that follows, I argue that the decline in infant mortality after democratization is not limited to these two countries and that many, if not all, possible confounding factors do not explain this decline.
2. See Web Appendix Section A.1 for more details on these new health policies implemented by new democratic governments in Zambia and Nigeria.
2.2. Measuring Democracy in Africa
The definition of democracy in this paper follows the one by Przeworski et al. (2000) with minor modifications to fit it into the context of African politics. Democracy is defined as a political system where (1) the chief executive of the national government has been elected in multiparty elections with universal suffrage, without subsequently banning opposition parties; and (2) anewchief executive has assumed office by winning multiparty elections.4As none of the existing democracy datasets allow me to measure democracy in that way, I consulted Nohlen, Krennerich, and Thibaut (1999), Europa Publications (various years), and some other sources to collect relevant information for 28 sub-Saharan African countries for which micro data on infant survival are available.5
This coding procedure reveals the following pattern of the evolution of democracy in the 28 countries (see Table 1). Among 24 countries that had become independent by the 1960s, 12 were democratic at the time of independence. However, all these countries experienced a collapse of democracy either by a military coup or by the banning of opposition parties by the early 1970s. Around 1980, three countries (Ghana, Nigeria, and Uganda) became democratic, but all of them saw military coups toppling democratic governments by the mid-1980s. Since 1990, eleven countries have been democratized within the period for which micro data on infant mortality are available.6
Web Appendix Figure A2 shows the geographic distribution of these eleven countries that were democratized after 1990. These countries are not concentrated in a particular area of Africa, thus ensuring that the estimated impact of democracy will not pick up an unobservable trend in infant mortality in a specific part of the continent.
2.3. Difference of Democracy in Africa Before and Since the 1990s
One might expect that the impact of democracy in Africa would differ before and after the end of the Cold War. During the Cold War period, attempts to subvert democracy in Africa were tolerated by the West so that African countries would not seek the support of the Soviet Union. After the end of the Cold War, however,
4. Web Appendix Section A.2 provides theoretical motivations behind the definition of democracy in the present paper and discusses alternative definitions of democracy such as Polity IV. In their analysis of the causes of democratization in Africa, Bratton and van de Walle (1997, pp. 10–13) adopt a similar definition of democracy to the one in the present paper.
5. See Web Appendix Section B for more details.
K
TABLE1. Periods of democracy and multiparty politics between 1950 and 2004.
Year of Periods of Periods of Sample Sample mean infant
Country independence democracy multiparty politics period mortality before 1990
Benin 1960 1960–61,1991- - 1964–2000 0.118∗
Burkina Faso 1960 - 1978–80, 1998- 1966–2002 0.105∗
Cameroon 1960 1960–65 1992- 1968–2003 0.086
Chad 1960 1960–62 1996- 1962,65,67-2003 0.112∗
Comoros 1975 1975,1990–99, 2002- - 1975–1995 0.111∗
Cote d’Ivoire 1960 2000- 1990–99 1962–1998 0.100∗
Ethiopia - - 1995- 1963–1999 0.131∗
Gabon 1960 1960–61 1993- 1962–1999 0.067
Ghana 1957 1969–72, 1979–81,2000- 1960–64, 1992–2000 1967–2002 0.082
Guinea 1958 - 1993- 1961–1998 0.142∗
Kenya 1963 1963–69, 2002- 1992–2002 1965–2002 0.074
Lesotho 1966 1966–70,1993- - 1967,69–2004 0.072
Madagascar 1960 1960–65,1993- - 1962–1996 0.105∗
Malawi 1964 1994- - 1964–1999 0.133∗
Mali 1960 1992- - 1964–2000 0.152∗
Mauritania 1960 - 1992- 1962–2000 0.078
Mozambique 1975 - 1994- 1975–2002 0.155∗
Namibia 1990 1990- - 1990–1999 0.050
Niger 1960 1993- - 1960–1997 0.140∗
Nigeria 1960 1979–83,1999- - 1965–2002 0.115∗
Rwanda 1962 1962–65 2003- 1963–1999 0.089
Senegal 1960 1960–63, 2000- 1978-2000 1961–1996 0.092
South Africa 1910 1994- - 1961–1997 0.065
Tanzania 1964 - 1995- 1968–2004 0.096
Togo 1960 1960–61 1993- 1960–1997 0.112∗
Uganda 1962 1962–69, 1980-85 1996- 1964–2000 0.091
Zambia 1964 1964–72,1991- - 1965–2001 0.087
Zimbabwe 1980 1980- - 1980–1998 0.048
Western donor countries became less willing to accept the collapse of democracy.7As a result, African policymakers may no longer expect to receive foreign aid if democracy collapses.8
To stay in power, policymakers in a democracy either need to improve the welfare of citizens to win multiparty elections or ignore citizens’ welfare and, whenever they would otherwise be voted out, terminate democracy by buying off a few politically powerful people. It can plausibly be assumed (1) that the cost of choosing the latter option is smaller than that of choosing the former and (2) that the benefit from staying in power, in the African context, depends on the amount of foreign aid from which policymakers can extract rent. These two assumptions, together with the above-mentioned change in how foreign donors respond to the collapse of democracy after the end of the Cold War, imply that there should have been a significant drop in the payoff from ignoring citizens’ welfare and, if necessary, terminating democracy to remain in power after the end of the Cold War. Therefore, in Africa, democratic institutions have been more likely to shape the incentive of policymakers since the 1990s than before. Consequently, I estimate the impact of democracy separately between the eleven cases since 1990 and the other cases during the Cold War.9
2.4. Causes of Post-Cold War Democratization in Africa
As democratization is hardly exogenous, it is essential to understand the causes of democratization in Africa after the end of the Cold War, in order to understand what may bias the estimation of the impact of democratization. In a widely cited study from the political science literature on the causes of democratization in Africa in the early 1990s, Bratton and van de Walle (1997) find that democratization is cross-sectionally correlated with military intervention in politics in favor of democracy, more official development assistance (ODA), more frequent political protests, and the presence of cohesive opposition to the incumbent dictator.10While military intervention in politics is unlikely to affect infant survival, ODA is potentially a confounding factor for
7. Indeed, military coups against democratic governments in the 1990s were quickly suppressed by foreign intervention (the Comoros in 1995, Lesotho in 1994 and 1998) or immediately followed by fresh multiparty elections due to donor pressure (Niger in 1996).
8. Consistent with this possibility, Dunning (2004) finds that it is only after 1986 (when the Soviet Union withdrew its financial support to African countries) that the amount of ODA is positively correlated with the degree of democracy in Africa.
9. An anonymous referee points out that there might have been a dramatic increase in global investments in child health since 1990, which may have interacted with democracy in Africa. According to Rosenfield and Min’s (2009) account of the history of international cooperation in maternal and child health, it was in 1982 that the “child survival revolution” took place, after which immunization and oral rehydration therapy (used to treat dehydration caused by diarrhea) were heavily promoted in developing countries. Due to the lack of democratization episodes in Africa after 1982 and before 1990, we cannot rule out the possibility that democratic governments in Africa before 1982 could not improve child survival because of the lack of international assistance even if they wanted to.
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1301
democracy if more aid-dependent countries tend to be democratized due to donor pressure. In the analysis that follows, I will check if the main result is robust to controlling for the amount of ODA. Frequent political protests and opposition cohesiveness may have resulted from an increased ability for African citizens to solve collective action problems, which may also have helped the survival of babies (by, for example, improving the accountability of local health care staff as in Bj¨orkman and Svensson 2009). Due to the lack of time-variant data on collective action, we cannot exclude the possibility that the estimated impact of democratization in this paper picks up this effect.
While Bratton and van de Walle (1997) downplay the role of economic factors, Br¨uckner and Ciccone (2011) find that negative rainfall shocks in the previous year increase the probability of democratization in Africa during the period 1980–2004. As income mostly depends on rain-fed agriculture in Africa, they interpret this result as the effect of a temporally low opportunity cost of revolution, the key determinant of democratization according to Acemoglu and Robinson (2000). Since unusually low precipitation is found to increase infant mortality in arid climate zones of Africa (Kudamatsu, Persson, and Str¨omberg 2010), I will check the robustness of the main result to controlling for annual rainfall and its one-year lag.
2.5. Micro Data on Infant Mortality
The micro data on infant mortality (and all other characteristics of babies used in this paper) are obtained from the Demographic and Health Surveys (DHS). The DHS questionnaire is standardized so that researchers can compile cross-country micro datasets. In each DHS survey, a nationally representative sample of women of child-bearing age (15 to 49) are interviewed about the date of birth, and the date of death if applicable, of up to 20 children to whom they gave birth in the past. From this recall data, a panel dataset of mothers can be constructed where the time dimension is the year of child birth given by each mother. Therefore, as long as at least one round of survey was conducted in a country, a panel dataset of mothers is available for that country.
After dropping babies born either before the year of independence of their country or within twelve months before their mother’s interview from the sample (to avoid measurement error in infant mortality), the 28 DHS surveys provide a sample of 643,846 children born to 161,876 mothers with the year of birth of the children spanning from 1960 to 2004. To measure individual-level infant mortality, a dummy is constructed for whether a child dies before the age of one year. Since the literature suggests that determinants of infant death within the first month of life (known as neonatal mortality) differ from those for the rest of the first year of life (e.g. Razzaque et al. 1990), a dummy for whether a child dies before the age of onemonth is also constructed.
Web Appendix Section A.4 discusses in detail data issues such as recall bias, mortality selection bias, and fertility selection bias. It shows that for those 21 countries where the previous round of the DHS survey is available, the difference across surveys in the reported annual infant mortality rates for a particular birth cohort of women is not significantly associated with democratization. It also provides evidence that neither changes in fertility of the interviewed women nor changes in the mortality of sisters of the interviewed women after democratization differ across different observable characteristics such as education, affluence, and the area of residence (urban or rural).
The sample average infant mortality rate is 10% of live births. The sample mean neonatal mortality rate is 4.7%, indicating that nearly half of the infant deaths occur within the first month after birth.11
With mother fixed effects being controlled for, it is those mothers giving birthboth before and after the year of democratization that contribute to the identification of the democracy effect. There are more than 27,000 such mothers in the sample (about 17% of the total number of mothers in the sample).12Compared to the other mothers of the same age in the same country, these mothers are more likely to be uneducated, poor (in terms of consumer durable ownership), and living in rural areas (see Web Appendix Section A.6). Column (1) of Table 2 shows that for these mothers, the sample mean infant and neonatal mortality rates fall after democratization. Column (2), on the other hand, shows that the sample mean mortality rates are higher for babies born to those mothers giving birth only after democratization than for babies born to those giving birth only before democratization. Column (3), where we exclude mothers giving only one birth from those in column (2) so that the fertility rate is more comparable to column (1), strengthens this observation, suggesting that the composition of mothers in the eleven democratized countries appears to have changed after the democratization. These observations suggest the importance of controlling for the mother fixed effects to estimate the impact of democracy on infant survival.
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1303
TABLE2. Mean infant and neonatal mortality rates in democratized countries.
(1) (2) (3)
Both before Only before Only before or only after and after or only after with 2+ births
Infant death
before democratization 0.120 0.101 0.103
after democratization 0.094 0.109 0.123
Neonatal death
before democratization 0.056 0.047 0.048
after democratization 0.042 0.054 0.061
Number of live birth observations
before democratization 98,330 77,717 73,757
after democratization 47,929 25,893 16,855
Notes: Live birth observations for the eleven democratized countries are included in the sample of this table. Each column represents a subsample by the type of mothers: column (1) for those giving birth both before and after democratization; column (2) for those giving birth either only before or only after democratization; column (3) for those giving birth more than once but either only before or only after democratization.Infant deathis the indicator for death at the age of less than twelve months;Neonatal deathis the indicator for death at the age of less than one month.
3. Empirical Analysis
3.1. Method
To investigate whether democratization has reduced infant mortality, I estimate the following linear probability model:13
yimact =αm+βat+γ1Dct∗1(t ≥1990)+γ2Dct ∗1(t <1990) +δcTRENDct+x$
imactθ+εimact. (1)
The dependent variableyimactis a dummy that equals one if babyiwho was born to
mothermof birth cohortain countrycin yeartdies before reaching the age of one year (or one month if the outcome of concern is neonatal mortality). Mother fixed effects αmand mother’s birth cohort by child’s birth year fixed effectsβatare controlled for so
that we estimate the impact of democracy by first taking a difference in infant mortality for the same mother over time and then taking a difference in these differences between mothers of the same birth cohort across countries. By allowing child birth year fixed effects to differ across different birth cohorts of mothers, I nonparametrically control for the effect of a mother’s age at birth that is allowed to change over time due to the continent-wide improvements in the survival of babies (see Web Appendix Figure A.1).
Dct is a dummy variable equal to one if country c is a democracy throughout
yeart. Therefore, this dummy is turned on a year after the year of democratization.
1(·) is an indicator function that equals one if the argument holds true. The term δcTRENDct represents a linear time trend specific to country c.14 The vector of
exogenous covariates,ximact, includes a dummy for girls, a dummy for multiple births
(i.e. twins, triplets, or quadruplets),15and dummies for each birth order from the second to the ninth as well as the tenth or higher (with the first birth as the omitted category).16 Standard errors are clustered at the country level to take into account any arbitrary correlations of the error term,εimact, over space and time within each country. As the
number of countries is only 28 in the sample, I also report thep-value obtained from Cameron, Gelbach, and Miller’s (2008) wild cluster bootstrap-tprocedure for the main result.
The parameters of interest, γ1 and γ2 in equation (1), measure the impact of democracy since 1990 and before 1990, respectively. For a consistent estimation ofγ1 andγ2, the error termεimactmust be strictly exogenous; that is, it must be uncorrelated
with the democracy dummies not only contemporaneously but also in the past and the future when the same mother gives birth. It must also be uncorrelated with the democracy dummies for other countries where mothers of the same birth cohort give birth in the same year. After the main estimation results have been presented in what follows, I check the validity of this identifying assumption.
3.2. Main Results
Table 3 reports estimated coefficients on the two democracy dummies. To see how controlling for mother fixed effects affects the estimation results, column (1) controls for country fixed effects instead of mother fixed effects in addition to cohort-year fixed effects and exogenous covariates. The coefficient on democracy since 1990 is negative and statistically insignificant. Column (2) controls for mother fixed effects instead of country fixed effects. The post-Cold War democracy coefficient becomes larger in absolute terms and is now significantly different from zero at the 5% level.
Why does the post-Cold War democracy coefficient become larger in absolute terms once mother fixed effects are controlled for? Column (3) replaces mother fixed effects with country fixed effects that are allowed to differ across different birth cohorts of mothers. The post-Cold War democracy coefficient is now estimated to be of similar
14. As there are plenty of observations before the years of post-Cold War democratization, linear trends are unlikely to pick up the post-treatment trends (Wolfers 2006).
15. See Klasen (1996) and references therein for available evidence on gender bias in infant mortality in Africa. Pison (1992) reports that in sub-Saharan Africa, twins are three to four times as likely to die within the first year of life as singletons. Although there is no a-priori association with democratization, controlling for these exogenous characteristics of babies reduces the error variance and thus increases the precision of the democracy coefficient estimates.
K
udamatsu
D
emocratization
and
Inf
ant
Mortality
in
Sub-Saharan
A
frica
1305
TABLE3. Infant mortality drops after democratization since 1990.
(1) (2) (3) (4) (5) (6) (7) (8)
Dependent Infant Infant Infant Infant Neonatal Infant Infant Infant
variable death death death death death death death death
Democracy since 1990 −0.009 −0.013∗∗ −0.013∗ −0.012∗∗ −0.006∗∗∗ −0.012∗∗ −0.012∗∗ −0.010∗
(0.006) (0.005) (0.006) (0.005) (0.002) (0.005) (0.006) (0.006)
[0.076]∗
Democracy before 1990 −0.001 −0.001 −0.000 0.006 −0.001 0.007 0.006 0.007∗
(0.005) (0.005) (0.005) (0.004) (0.002) (0.004) (0.004) (0.004)
F-test 0.83 1.86 2.44 7.57∗∗ 3.91∗ 7.92∗∗∗ 8.27∗∗∗ 6.03∗∗
[0.371] [0.184] [0.130] [0.010] [0.058] [0.009] [0.008] [0.021]
Exogenous covariates YES YES YES YES YES See notes See notes YES
Cohort-year fixed effects YES YES YES YES YES YES YES See notes
Country fixed effects YES NO See notes NO NO NO NO NO
Mother fixed effects NO YES NO YES YES YES YES YES
Country-specific linear trends NO NO NO YES YES YES YES YES
Number of countries 28 28 28 28 28 28 28 28
Number of mothers 161,876 161,876 161,876 161,876 161,876 161,876 161,876 161,876
Observations 643,846 643,846 643,846 643,846 643,846 643,846 643,846 643,846
Notes: Standard errors clustered at the country level are reported in parentheses.Infant deathis the indicator for death at the age of less than twelve months;Neonatal deathis the indicator for death at the age of less than one month. For column (4), reported in brackets is thep-value obtained from Cameron, Gelbach, and Miller’s (2008) wild cluster bootstrap-tprocedure for the null that the coefficient onDemocracy since 1990is zero. TheF-test row reportsF-statistics (and its associatedp-value in brackets) for the null that coefficients onDemocracy since 1990andDemocracy before 1990are the same. TheExogenous covariatesrow indicates whether birth order dummies and dummies for girls and multiple births are controlled for. Column (3) controls for country fixed effects that differ across mother cohorts. Column (6) controls for country-specific birth order dummies as well as girl and twin dummies. Column (7) controls for country-specific mother age quadratic trends as well as birth order, girl and twin dummies. Column (8) controls for cohort-year fixed effects that differ between countries with high and low pre-1990 mortality rates.
magnitude to the mother fixed effects estimate in column (2). This result suggests that the cohorts of women who give birth only after democratization may be unhealthier and thus face a higher chance of their infant’s death. Their health status during adulthood might be negatively affected by the early childhood exposure to the lack of nutrition (e.g. Maccini and Yang 2009).17The result in column (3) also suggests that the mother fixed-effect estimate of the democracy effect may be applicable to a broader category of mothers, namely, the cohorts of women that have their fertile period around the year of democratization.
Column (4) estimates equation (1) by controlling for country-specific linear trends in addition to the set of controls in column (2). The post-Cold War democracy coefficient remains almost the same and statistically significant at the 5% level. The p-value from Cameron, Gelbach, and Miller’s (2008) wild cluster bootstrap-t procedure is 0.076. This result shows that the coefficient estimate in column (2) does not reflect a steeper declining trend in infant mortality in democratized countries than in nondemocratized countries. Democratization since 1990 is followed by a reduction in the infant mortality rate by 1.2 percentage points, which is as much as 12% of the sample mean.
Column (5) reports the result for neonatal death in the same specification as in column (4). The probability that a mother sees her baby die within the first month of life falls by 0.6 percentage points after democratization (statistically significant at the 1% level), about 13% of the sample mean. A sizable portion of the fall in mortality within the first year of life after post-Cold War democratization is therefore due to the fall in mortality within the first month of life.
The coefficient on the dummy for democracy during the Cold War is, on the other hand, closer to zero and statistically insignificant in columns (4) and (5). The difference between the coefficients on democracy before 1990 and from 1990 and onwards is significant at the 5% level for infant mortality (column 4) and at the 10% level for neonatal mortality (column 5). Although this result is not conclusive due to the limited number of observations exposed to democracy during the Cold War, democracy in Africa appears to have an impact only after the end of the Cold War.18
3.3. Validity and Robustness Checks
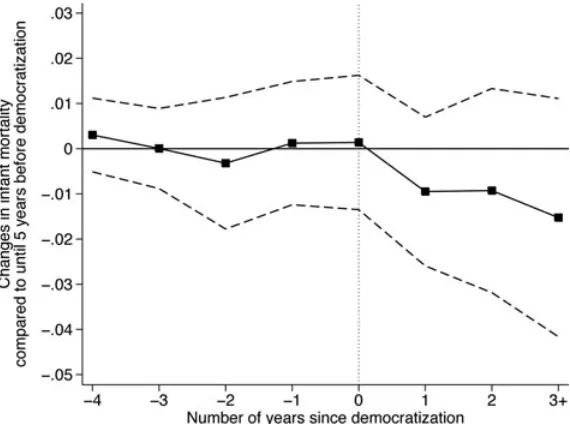
To validate the identifying assumption, I estimate year-wise changes in infant mortality before and after democratization. Specifically, I replace Dct ∗ 1(t ≥ 1990) in
equation (1) with the set of year-wise dummy variables which equal one if nyears have passed since the year of post-Cold War democratization, where −4 ≤ n ≤ 2, and another dummy variable equal to 1 if three years or more have passed.19
17. See Web Appendix Section A.7 for some suggestive evidence for this possibility.
18. The number of mothers exposed to democracy during the Cold War for at least one child birth is 3,096 (1.9% of the total number of mothers in the sample).
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1307
FIGURE 2. Dynamics of infant mortality before and after democratization. The horizontal axis measures the number of years since democratization. The plots connected by the solid line indicate changes in infant mortality compared to the period until five years before democratization conditional on mother fixed effects, cohort-year fixed effects, dummies for girls, multiple births, and birth orders, the Cold War democracy dummy, and country-specific linear trends. See Web Appendix Table A.9 for the exact numbers of these point estimates. The dotted lines indicate the 95% confidence intervals where standard errors are clustered at the country level. The comparison between two years since democratization and three years or more should be interpreted with caution because the composition of democratized countries is different (only two years after democratization are observed for Ghana).
Figure 2 plots the estimated coefficients on these dummies and shows the 95% level confidence intervals.20These are interpreted as changes in infant mortality, relative to nondemocratized countries, as compared to the period until five years before post-Cold War democratization. The point estimates show that there was no hike or dip in infant mortality before post-Cold War democratization and that the decline in infant mortality started only after democratization. Although the decline after democratization is not statistically significant at the conventional level, these point estimates encourage the interpretation that democracy has reduced infant mortality.21
Columns (6) to (8) in Table 3 deal with three further concerns on the identifying assumption. Columns (6) and (7) control for country-specific birth order dummies and country-specific mother’s age quadratic trends, respectively, to see if the main result is
after post-Cold War democratization. Therefore, I lump together three years or more after democratization in order to prevent changes in the composition of democratized countries from affecting the result. 20. The regression table for this result can be found in Web Appendix Table A.9.
driven by steeper declining trends of birth order or the mother’s age in infant mortality for democratized countries.22 In column (8), I interact βat in equation (1) with an
indicator variable for the 14 countries whose sample mean infant mortality before 1990 is higher than the rest (see the last column in Table 1) so that changes in the outcome could be dependent on a country’s initial level in the absence of democratization.23In all cases, there is little change in the size of the estimated democracy coefficient.
Table 4 reports estimation results when possibly confounding variables for democracy are controlled for in equation (1). The first two columns control for some of the causes of democratization in Africa found in the literature (see Section 2.4). Column (1) controls for total yearly rainfall at the country level and its one-year lag, obtained from the Africa Rainfall Dataset by Miguel, Satyanath, and Sergenti (2004). Column (2) controls for total ODA as a percentage of GDP (World Bank 2008).24In both cases, the estimated coefficient on democracy since 1990 is of similar size as in column (4) of Table 3 and remains statistically significant (now at least at the 5% level). Column (2) also reports a significantly positivecoefficient on ODA, suggesting that there was an increase in ODA when infant mortality went up. An interesting issue is whether the impact of democratization is larger with more ODA. Column (3) answers this question by including the interaction term of democracy since 1990 and ODA. The coefficient on the interaction term is not statistically significant from zero, thus suggesting that ODA does not appear to be a major channel of the estimated impact of democratization.
Columns (4) to (8) in Table 4 control for other variables that may be correlated with both democracy and infant mortality. Columns (4) and (5) add as a regressor the logarithm of real GDP per capita taken from Heston, Summers, and Aten (2006) and the average years of female education taken from Barro and Lee (2000), respectively.25 Columns (6) and (7) control for a dummy for being the location of armed conflicts with more than 1,000 battle-related deaths, taken from the Armed Conflict Database version 3-2005b (Gleditsch et al. 2002), and the fertility rate at the country level, respectively.26Column (8) controls for a dummy for less than 24 month birth intervals (this dummy is set to be zero for the first birth of each mother), created from the DHS data.27In all cases, there is little change in the size of the point estimate for the democracy coefficient, and its statistical significance remains intact. Finally, column
22. Controlling for country-specific mother’s age dummies or higher-order trends is computationally too demanding to implement.
23. The result does not change if we instead use the sample mean infant mortality in the 1980s. 24. The result is similar if we use the amount of ODA committed by the donor countries to health or water supply and sanitation, obtained from the OECD-CRS database (OECD 2008).
25. Barro and Lee’s (2000) data on the average years of education among women aged 15 or above is only available for 18 out of the 28 sample countries. If we estimate equation (1) for the same sample as in column (5), the point estimate for the coefficient on democracy since 1990 is –0.013 with a standard error of 0.006, significant at the 5% level.
26. The fertility rate is obtained from World Bank (2008) and linearly interpolated to fill out missing values because the data are available every two to three years.
K
TABLE4. Robustness to controlling for possible confounders to democracy.
(1) (2) (3) (4) (5) (6) (7) (8) (9)
Democracy −0.011∗∗ −0.015∗∗∗ −0.021∗∗∗ −0.012∗∗ −0.012∗ −0.012∗∗ −0.011∗∗ −0.011∗∗ −0.011∗∗
since 1990 (0.005) (0.005) (0.005) (0.005) (0.006) (0.005) (0.005) (0.005) (0.005)
Democracy 0.009 0.007 0.007 0.004 0.007 0.006 0.006 0.007 0.008
before 1990 (0.006) (0.004) (0.004) (0.004) (0.007) (0.004) (0.004) (0.004) (0.010)
Log rainfall 0.000 0.006
(0.005) (0.006)
Lagged −0.007 −0.007
log rainfall (0.006) (0.009)
Total ODA 0.0003∗∗∗ 0.0003∗∗ 0.0002∗∗
as % of GDP (0.0001) (0.0001) (0.0001)
Democracy 0.0003
[0.023] [0.002] [0.001] [0.017] [0.096] [0.011] [0.011] [0.010] [0.132]
# of countries 27 28 28 28 18 28 28 28 18
# of mothers 154,903 157,019 157,019 161,862 104,193 161,876 161,869 161,876 98,772
Observations 550,534 605,370 605,370 643,641 405,312 643,846 643,515 643,846 341,436
Notes: Standard errors clustered at the country level are reported in parentheses. The dependent variable is the indicator for death at the age of less than twelve months. TheF-test row reports F-statistics (and its associatedp-values in brackets) for the null that coefficients onDemocracy since 1990andDemocracy before 1990are the same. All columns control for birth order dummies, dummies for girls and multiple births, mother’s cohort by child birth year fixed effects, mother fixed effects, and country-specific linear trends. See Section 3.3 for the definition of other control variables. In column (1), the Comoros is dropped from the sample due to the lack of rainfall data.
(9) shows that the main result is robust to controlling for all the covariates at the same time.28
3.4. What type of political change matters?
The definition of democracy in this paper involves two concepts: multiparty elections and leadership change. Columns (1)–(4) of Table 5 investigate whether only one of the two is sufficient to drive infant mortality down.
I first create a dummy that equals one if the whole year falls into the period in which the chief executive is elected by multiparty elections and the former dictator or the single ruling party continuously stays in power (see Table 1). This dummy for multiparty politics is then interacted with the dummies for before 1990 and since 1990. In column (1), these two interaction terms are additionally included as regressors in equation (1). In column (2), the interaction term of multiparty politics with the period since 1990 is further interacted with the dummy for Ethiopia, where the yearly mean infant mortality drops a great deal in the year of the first multiparty election, and this triple interaction term is added as an additional regressor. The coefficient on multiparty politics since 1990 is always smaller than the one on democracy since 1990, and once the outlier of Ethiopia has been taken into account, the two coefficients are significantly different at the 5% level.
To see if it is only leadership change that drives the results, I identify seven episodes of nondemocratic leadership change in the late 1980s and the early 1990s after which the same dictator stays in office until the end of the sample period.29I create a dummy variable that equals one if the whole year falls in the period after one of these seven nondemocratic changes in the chief executive, and this dummy is added as a regressor to equation (1) in column (3). Column (4) adds two interaction terms of this variable with the dummies for Ethiopia and Rwanda, respectively. As mentioned previously, there was a huge drop in infant mortality in Ethiopia in 1995, four years after the nondemocratic leadership change. In Rwanda, civil wars broke out in 1990, which culminated in the well-known massacre in 1994, the year of nondemocratic leadership change. Infant mortality kept rising during this period of civil wars in Rwanda. The coefficient on the period after nondemocratic leadership change is always smaller than the one on democracy since 1990, and once the two outliers are taken into account, the difference is statistically significant at the 5% level.
One potentially important element of democracy that is missing in the present paper’s definition is press freedom. Media freedom allows citizens to learn about government performances beyond their own experiences. Therefore, combined with
28. Web Appendix Table A.11 shows that the result is robust to dropping one country from the sample at a time, which suggests that the results in Table 3 are not driven by one outlier. Web Appendix Figure A.7 shows the distribution of the democracy coefficient estimates when two countries are dropped from the sample at a time. The point estimate ranges from−0.007 to−0.019.
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1311
TABLE5. What type of political change matters?
(1) (2) (3) (4) (5)
Democracy −0.014∗∗ −0.014∗∗ −0.012∗∗ −0.013∗∗ −0.011
since 1990 (0.005) (0.005) (0.005) (0.005) (0.011)
Multiparty politics −0.005∗∗ −0.003
since 1990 (0.002) (0.003)
Multiparty politics −0.025∗∗∗
since 1990 (0.003)
∗Ethiopia
After nondemocratic −0.006 0.001
leadership change (0.004) (0.003)
After nondemocratic −0.017∗∗∗
leadership change (0.003)
∗Ethiopia
After nondemocratic −0.027∗∗∗
leadership change (0.004)
Number of countries 28 28 28 28 28
Number of mothers 161,876 161,876 161,876 161,876 157,709
Observations 643,846 643,846 643,846 643,846 552,397
Notes: Standard errors clustered at the country level are reported in parentheses. The dependent variable is the indicator for death at the age of less than twelve months. TheF-test 1 row reportsF-statistics (and its associated
p-value in brackets) for the null that coefficients onDemocracy since 1990andMultiparty politics since 1990
are the same;F-test 2 for the null that coefficients onDemocracy since 1990andAfter nondemocratic leadership changeare the same. See Section 3.4 for the definitions ofMultiparty politics,After nondemocratic leadership change, andPress freedom. All columns control for birth order dummies, dummies for girls and multiple births, mother’s cohort by child birth year fixed effects, mother fixed effects, and country-specific linear trends. ∗∗Significant at 5%;∗∗∗significant at 1%.
contested elections, free media may create a greater incentive for politicians to improve citizens’ welfare.30 In order to see if press freedom increases the impact of democratization, column (5) adds to equation (1) the degree of press freedom (0 for not free, 1 for partially free, and 2 for free), taken from Freedom House (2008),
and its interaction term with democracy since 1990. The coefficient on the interaction term is zero, suggesting that the lack of press freedom does not weaken the impact of democratization on child survival.
In summary, Table 5 shows that the combination of multiparty elections and leadership change is likely to be the driving force for the decline in infant mortality while press freedom is not complementary to this effect. This finding is an advance in our understanding of what aspects of democracy are crucial in improving people’s welfare, which would not be possible if we used the standard measures of democracy such as the Polity dataset.
4. Pathways
The DHS’s retrospective fertility survey component asks women only about the survival of their child, preventing us from analyzing the pathways through which democratization has reduced infant mortality with mother fixed effects being controlled for. The availability of government health policy variables is very sketchy for African countries.31
However, the DHS surveys do provide information on several health inputs and other household-level variables at the time of the survey. For 21 out of the 28 African countries in the sample for the infant mortality analysis, DHS surveys were conducted more than once. Therefore, I can construct a repeated cross-sectional sample of infants at the time of each survey. This sample allows us to see whether more health inputs for infant survival are used after democratization.
Jones et al. (2003) identify 21 health interventions that are known to reduce child mortality from major causes of death. Among these interventions, the following six interventions can be tracked over time by different rounds of the DHS surveys: tetanus toxoid vaccination for pregnant women (prevention of neonatal tetanus), skilled delivery assistance (prevention of neonatal tetanus and sepsis), access to piped water (prevention of diarrhea), access to toilets32 (prevention of diarrhea), exclusive
31. Reliable cross-country data on government health expenditures are, for example, not widely available for Africa: the World Health Organization started reporting such data only after 1995; and the IMF’s Government Finance Statistics reports government health expenditures for only eleven countries out of the 28 sample countries, of which only three countries (Ghana, Madagascar, and Zambia) were democratized. With this available data, I do not find any evidence that there was an increase in health expenditures after democratization. Even if this result represents all the 28 countries, it does not necessarily imply that the democratically elected governments did not change health policy. Statistical correlations between government health expenditures and health outcomes are known to be very weak (Filmer and Pritchett 1999). The democratized governments may have changed the allocation of health expenditures which can bring a huge improvement in child survival (see de Savigny et al. 2004 for an example from two districts in Tanzania). Finally, government funds in developing countries are often seized by corrupt bureaucrats (see Reinikka and Svensson (2004) for an example of education funds in Uganda). Democratized governments may have mitigated such thefts for public health services without increasing the expenditures.
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1313
breastfeeding33in the first six months of life (prevention of diarrhea and pneumonia), and the oral rehydration solution (treatment of diarrhea).34For each of these six health inputs, I create an indicator variable,yiracs, which takes the value of 1 if infantiborn
to the mother of groupr35 and of birth cohortareceives the health input in country cin five-year periods.36 I also create dummies for infanti’s household owning each of the six consumer durable goods (radio, television, refrigerator, bicycle, motorcycle, and car), owning none of these assets, and having access to electricity, in order to see whether the affluence of an infant’s household improved after democratization. I then estimate the following equation:
yiracs =αr +βas +γDcs+x$iracsθ+εiracs, (2) where αr is a mother-group fixed effect, βas is a mother’s birth cohort by five-year
period fixed effect, and xiracs includes the birth order dummies, dummies for girls
and for multiple births. The democracy dummy,Dcs, is set to be one if countrycis
democratizedbeforethe DHS survey was conducted in periods. Since no survey is available for the period of democracy before 1990, we cannot estimate its coefficient in this sample. The standard errors are clustered at the country level. As there are only 21 countries in the sample, we also report thep-values obtained from Cameron, Gelbach, and Miller’s (2008) wild cluster bootstrap-tprocedure.
The estimatedγ in equation (2) is reported for each of the six health inputs in Table 6 and for each of the asset variables in Table 7. Almost none of the democracy coefficients are statistically significant. However, the point estimates for some of the health inputs are very large relative to the sample mean. A crude calculation (see Web Appendix Section A.8 for details) shows that the increased incidence of skilled delivery assistance, exclusive breastfeeding, and the oral rehydration solution could each explain 13% to 42% of the fall in neonatal or infant mortality after democratization. The latter two health interventions could be improved soon after democratization, consistent with the quick decline in infant mortality found in Figure 2.37On the other hand, changes in
dumped from a bucket or a plumbing system or whether the disposal system is a pit, septic tank or public sewer system.”
33. Exclusive breastfeeding is defined as breastfeeding without giving any food or other liquid. 34. For some other interventions identified by Jones et al. (2003), the DHS surveys either stop collecting data in the early 1990s (antibiotics for pneumonia, antimalarials) or only start collecting data recently (insecticide-treated bed nets for malaria prevention, vitamin A for preventing diarrhea and treating measles). Data on measles vaccination is available in all the DHS surveys, but I exclude it from the analysis because it mainly prevents deaths during the second year of life and later (the WHO recommends the measles vaccination at the age of nine months).
35. A mother group is defined by where mothers live (which administrative regions and whether urban or rural areas), their level of education (whether they attended at least primary school or did not go to school at all), and their birth cohort (year of birth). Thus, I make this analysis as comparable as possible to the infant mortality analysis where mother fixed effects are controlled for. See Web Appendix Section C for how administrative regions are matched across different rounds of surveys.
36. Five-year spellsrefers to 1985–1989, 1990–1994, 1995–1999, or 2000–2004 when the DHS survey was conducted. The DHS survey is usually conducted every fifth year with the exact year of survey being different between countries.
TABLE6. Do health inputs become more accessible after democratization?
(1) (2) (3) (4) (5) (6)
Dependent Tetanus Skilled Access to Access to Exclusive Oral
variable toxoid delivery piped toilets breastfeeding rehydration
vaccination assistance water solution
Sample mean 0.670 0.452 0.267 0.055 0.355 0.288
Democracy 0.081 0.050 0.002 0.018∗ 0.147 0.062∗
since 1990 (0.067) (0.041) (0.040) (0.009) (0.101) (0.036)
[0.370] [0.328] [0.994] [0.108] [0.212] [0.170]
Countries 21 21 21 21 21 21
Mother groups 19,055 19,244 19,127 19,125 13,975 8,234
Observations 69,807 71,567 70,427 70,413 34,853 14,426
Notes: Standard errors clustered at the country level are reported in parentheses; reported in brackets are the
p-values obtained from Cameron, Gelbach, and Miller’s (2008) wild cluster bootstrap-tprocedure for the null that the coefficient onDemocracy since 1990is zero. The sample includes all babies (both living and dead at the survey date) born within twelve months before the survey date in columns (1) to (4), all living babies aged less than six months at the survey time in column (5), and all living babies aged less than twelve months who had diarrhea within two weeks before the survey date in column (6). All regressions control for birth order dummies, dummies for girls and for multiple births, mother group fixed effects and mother’s birth cohort by five-year period fixed effects. See Section 4 for the definitions of mother groups and cohort-period fixed effects.
∗Significant at 10%.
TABLE7. Do households with infants become more affluent after democratization?
(1) (2) (3) (4) (5) (6) (7) (8)
Dependent Radio Television Refrigerator Bicycle Motorcycle Car None Electricity variable
Sample mean 0.552 0.101 0.055 0.340 0.086 0.036 0.310 0.149
Democracy 0.001 −0.013 0.006 −0.003 −0.001 0.002 −0.014 0.015 since 1990 (0.032) (0.019) (0.008) (0.035) (0.008) (0.005) (0.044) (0.016)
[0.994] [0.578] [0.502] [0.928] [0.968] [0.716] [0.766] [0.380]
Countries 21 21 20 21 21 21 21 21
Mother groups 19,099 19,099 17,706 19,090 19,066 18,727 18,687 18,857 Observations 70,219 70,219 66,550 70,187 68,960 67,849 67,916 68,920
Notes: Standard errors clustered at the country level are reported in parentheses; reported in brackets are the
p-values obtained from Cameron, Gelbach, and Miller’s (2008) wild cluster bootstrap-tprocedure for the null that the coefficient onDemocracy since 1990is zero. The sample includes all the babies (both living and dead at the survey date) born within twelve months before the survey date. All regressions control for birth order dummies, dummies for girls and for multiple births, mother group fixed effects and mother’s birth cohort by five-year period fixed effects. See Section 4 for the definitions of mother groups and cohort-period fixed effects. In column (3), Malawi is dropped from the sample as its surveys do not collect information on the ownership of refrigerators.
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1315
5. Conclusions
By comparing the survival of babies born to the same mother in sub-Saharan Africa over time, I find that infant mortality has dropped since the introduction of multiparty elections resulted in the inauguration of a new chief executive of the national government during the post-Cold War period. Such changes in infant survival did not occur when dictators stayed in power by winning multiparty elections or when a new chief executive took office nondemocratically.
As democracy is never randomly assigned across countries, we cannot claim that these pieces of evidence establish the causal impact of democracy on development. Unlike the previous studies using country-level statistics, however, the use of micro data in this paper makes the above findings immune to confounding changes in the demographic composition of the population, encouraging us to believe that democratization may be an important means of promoting development in some of the poorest countries in the world.
Supporting Information
Additional Supporting Information may be found in the online version of this article:
Appendix S1a. Material that cannot be included in the main article due to space constraints (including tables and figures) (pdf file)
Appendix S1b.Description of construction of dataset, and raw data (pdf file)
Appendix S1c.Description of matching of subnational administrative regions across different rounds of the DHS surveys in the analysis for Section 4 (pdf file)
Appendix S2.Data files (zip file)
Please note: Blackwell Publishing are not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article.
References
Acemoglu, Daron and James A. Robinson (2000). “Why Did the West Extend the Franchise? Democracy, Inequality, and Growth in Historical Perspective.”Quarterly Journal of Economics, 115, 1167–1199.
Aghion, Philippe, Alberto Alesina, and Francesco Trebbi (2008). “Democracy, Technology, and Growth.” In Institutions and Economic Performance, edited by Elhanan Helpman. Harvard University Press.
Barro, Robert J. and Jong-Wha Lee (2000). “International Data on Educational Attainment: Updates and Implications.” Harvard University Center for International Development Working Paper No. 42.
Besley, Timothy and Robin Burgess (2002). “The Political Economy of Government Responsiveness: Theory and Evidence from India.”Quarterly Journal of Economics, 117, 1415–1451.
Bj¨orkman, Martina and Jakob Svensson (2009). “Power to the People: Evidence from a Randomized Field Experiment on Community-Based Monitoring in Uganda.”Quarterly Journal of Economics, 124, 735–769.
Bratton, Michael and Nicolas van de Walle (1997). Democratic Experiments in Africa: Regime Transitions in Comparative Perspective. Cambridge University Press.
Br¨uckner, Markus and Antonio Ciccone (2011). “Rain and the Democratic Window of Opportunity.” Econometrica, 79, 923–947.
Cameron, A. Colin, Jonah B. Gelbach, and Douglas L. Miller (2008). “Bootstrap-based Improvements for Inference with Clustered Errors.”Review of Economics and Statistics, 90, 414–427. Das Gupta, Monica, Varun Gauri, and Stuti Khemani (2004). “Decentralized Delivery of Primary
Health Services in Nigeria: Survey Evidence from the States of Lagos and Kogi.” World Bank Africa Region Human Development Working Paper 70.
de Savigny, Don, Harun Kasale, Conrad Mbuya, and Graham Reid (2004).Fixing Health Systems. Ottawa: International Development Research Centre.
Dunning, Thad (2004). “Conditioning the Effects of Aid: Cold War Politics, Donor Credibility, and Democracy in Africa.”International Organization, 58, 409–423.
Europa Publications. (various years).Africa South of the Sahara. Europa Publications.
Ferraz, Claudio and Frederico Finan (2008). “Exposing Corrupt Politicians: The Effect of Brazil’s Publicly Released Audits on Electoral Outcomes.” Quarterly Journal of Economics, 123, 703–745.
Filmer, Deon and Lant Pritchett (1999). “The Impact of Public Spending on Health: Does Money Matter?”Social Science and Medicine, 49, 1309–1323.
Freedom House (2008).Freedom of the Press. http://www.freedomhouse.org/report-types/freedom-press/.
Garenne, M. and A. Gakusi (2006). “Vulnerability and Resilience: Determinants of Under Five Mortality Changes in Zambia.”World Development, 34, 1765–1787.
Gleditsch, Nils Petter, Peter Wallensteen, Mikael Eriksson, Margareta Sollenberg, and Havard Strand (2002). “Armed Conflict 1946–2001: A New Dataset.”Journal of Peace Research, 39, 615– 637.
Heston, Alan, Robert Summers and Bettina Aten (2006). “Penn World Table Version 6.2.” Center for International Comparisons of Production, Income and Prices at the University of Pennsylvania. http://pwt.econ.upenn.edu/
Hobcraft, J. N., J. W. McDonald, and S. O. Rutstein (1985). “Demographic Determinants of Infant and Early Child Mortality: A Comparative Analysis.”Population Studies, 39, 363–385. Institute for Resource Development and Macro International (1990). “Demographic and Health
Surveys Phase II: Model “B” Questionnaire with Commentary for Low Contraceptive Prevalence Countries.” DHS II Basic Documentation Number 2. http://www.measuredhs.com/pubs/ Jones, Gareth, Richard W. Steketee, Robert E. Black, Zulfiqar A. Bhutta, Saul S. Morris, and the
Bellagio Child Survival Study Group (2003). “How Many Child Deaths Can We Prevent This Year?”The Lancet, 362, 65–71.
Klasen, Stephan (1996). “Nutrition, Health and Mortality in Sub-Saharan Africa: Is There a Gender Bias?”Journal of Development Studies, 32, 913–932.
Kramer, M. S., B. Chalmers, E. D. Hodnett, Z. Sevkovskaya, I. Dzikovich, S. Shapiro, J. P. Collet, I. Vanilovich, I. Mezen, T. Ducruet, G. Shishko, V. Zubovich, D. Mknuik, E. Gluchanina, V. Dombrovskiy, A. Ustinovitch, T. Kot, N. Bogdanovich, L. Ovchinikova, E. Helsing, and PROBIT Study Group (2001). “Promotion of Breastfeeding Intervention Trial (PROBIT): a randomized trial in the Republic of Belarus.”Journal of the American Medical Association, 285, 413–420. Kudamatsu, Masayuki, Torsten Persson, and David Str¨omberg (2010). “Weather and Infant Mortality
in Africa.” Working paper, Stockholm University.
Kudamatsu Democratization and Infant Mortality in Sub-Saharan Africa 1317
Lipset, Seymour Martin (1959). “Some Social Prerequisites of Democracy: Economic Development and Political Legitimacy.”American Political Science Review, 53, 69–105.
Maccini, Sharon and Dean Yang (2009). “Under the Weather: Health, Schooling, and Socioeconomic Consequences of Early-life Rainfall.”American Economic Review, 99(3), 1006–1026.
Miguel, Edward, Shanker Satyanath, and Ernest Sergenti (2004). “Economic Shocks and Civil Conflict: An Instrumental Variables Approach.”Journal of Political Economy, 112, 725–753. Miller, Grant (2008). “Women’s Suffrage, Political Responsiveness, and Child Survival in American
History.”Quarterly Journal of Economics, 123, 1287–1327.
Nohlen, Dieter, Michael Krennerich, and Bernhard Thibaut. (eds.) (1999).Elections in Africa: A Data Handbook.Oxford University Press.
OECD (2008).International Development Statistics (IDS) Online Databases on Aid and Other Resource Flows.http://www.oecd.org/dac/stats/idsonline
Persson, Torsten and Guido Tabellini (2006). “Democracy and Development: The Devil in the Details.”American Economic Review, 97(2): 319–324.
Pison, Gilles (1992). “Twins in Sub-Saharan Africa: Frequency, Social Status, and Mortality.” In Mortality and Society in Sub-Saharan Africa, edited by Etienne van de Walle, Gilles Pison, and Mpembele Sala Diakanda. Clarendon Press.
Przeworski, Adam, Michael E. Alvarez, Jose Antonio Cheibub and Fernando Limongi (2000). Democracy and Development: Political Institutions and Well-Being in the World, 1950–1990. Cambridge University Press.
Razzaque, Abdur, Nurul Alam, Lokky Wai, and Andrew Foster (1990). “Sustained Effects of the 1974-5 Famine on Infant and Child Mortality in a Rural Bangladesh.”Population Studies, 44, 145–154.
Reinikka, Ritva, and Jakob Svensson (2004). “Local Capture: Evidence from a Central Government Transfer Program in Uganda.”Quarterly Journal of Economics, 119, 679–705.
Rosenfield, Allan and Caroline J. Min (2009). “A History of International Cooperation in Maternal and Child Health.” InMaternal and Child Health, edited by John Ehiri. Springer.
Ross, Michael (2006). “Is Democracy Good for the Poor?”American Journal of Political Science, 50, 860–874.
Sen, Amartya (1989). “Food and Freedom.”World Development, 17, 769–781.
Wolfers, Justin (2006). “Did Unilateral Divorce Laws Raise Divorce Rates? A Reconciliation and New Results.”American Economic Review, 96(5), 1802–1820.
World Bank (2008).World Development Indicators Online. http://data.worldbank.org/data-catalog. Zenger, Elizabeth (1993). “Siblings’ Neonatal Mortality Risks and Birth Spacing in Bangladesh.”
REDUCED INFANT MORTALITY IN
SUB-SAHARAN AFRICA? EVIDENCE FROM
MICRO DATA”
Masayuki Kudamatsu IIES, Stockholm University
Section A contains supplementary materials that cannot be included in the main text due to the space constraints (including Appendix Figures and Tables). Section B describes how I constructed the democracy data and presents its raw data. Section C describes how I matched subnational administrative regions across different rounds of the DHS surveys in the analysis for Section 4. All the papers cited in this appendix (including those cited in the main text) can be found in the bibliography at the end of this appendix.
Appendix A: Supplementary materials
A.1. Country Case Studies in Detail
Zambia. Until multiparty elections, the �rst in about 20 years, brought a new government in power in 1991, public health facilities were not well-maintained; drugs were scarce, staff demoralized (Mpuku 1997). Expenditure on health declined by almost 30% in real terms between 1981 and 1991 (Government of Zambia 1992, p. 7).
The new democratically elected government implemented several health sector reforms (World Bank, Undated; Lake and Musumali 1999): decentralizing health management authority to districts along with increased district grants (which was facilitated by the funding from the DANIDA, the Danish bilateral aid agency, in 1993) and with district health staff capacity-building; changing the focus from curative and hospital-based services to preventive and health center-based ones; introducing user fees with the exemption for children under�ve years where the revenue is retained by clinics for�nancing service quality improvements; and pooling donor funds to�nance district-level health services for improving aid coordination. In 1995, the Ministry of Health conducted a cost-effectiveness analysis to set priorities among various
E-mail: [email protected]
Kudamatsu Web Appendix to "Democratization and Infant Mortality in Sub-Saharan Africa"2
health interventions. The resulting prioritized interventions for child survival were immunization, perinatal care, and the treatment of malaria, diarrhea, and respiratory diseases.1
From 1993 to 1994, the proportion of the national budget allocated to health care increased from 8% to 13%, vaccination coverage rose from 75% to 95%, malnutrition cases dropped from 126,351 to 82,193, and the annual cholera epidemic was greatly muted in 1994 (World Bank, Undated).2Blas and Limbambala (2001) �nd that the rates of measles vaccination and child delivery at health centers (both of which are supposed to be exempt from fees) were on the rise in the years from 1993 to 1997.
Lake and Musumali (1999) argue that a more effective management of external resources from donor countries was achieved partly due to political support for the health sector reforms at the highest level of the Zambian government. Gilson et al. (2003) note that the health sector was the�rst sector in which the way of allocating budgetary resources was changed, and argue that such a quick health policy change was feasible because of the political momentum created by democratization.
Nigeria. In 1999, the year of democratization, “a new drive to substantially re-vitalize the immunization system commenced” in Nigeria (WHO 2008). The funding for the National Programme of Immunization has gone up from 9 million naira in 1998 to nearly 7.5 billion naira in 2001 (Das Gupta et al. 2004, p. 7). In 2000, the Nigerian government hosted an assembly of representatives of 44 African countries to approve a plan of action for controlling malaria (the Abuja Declaration). The use of insecticide-treated bed nets (ITNs), one of the most effective ways for preventing children and pregnant women against malaria infections (see Lengeler 2004 for a review on randomized trials), is recommended in this declaration. In the following year, the Nigerian government removed tariffs and taxes on insecticides for public health use, which had been 42%, and reduced tariffs and taxes on netting materials from 40% to 5%, in order to promote the use of ITNs (Simon et al. 2002, p. 896). According to Baume and Marin (2008, Table 2), in selected areas of Nigeria, the percentage of households with children under�ve years old owning ITNs went up from zero in 2000 to 8.9 in 2004; the shares of children less than�ve years old and pregnant women sleeping under an ITN were both zero in 2000 but went up to 3.3% and 4.4% in 2004, respectively.
A.2. Definitions of Democracy
Theoretical Motivations for this Paper’s Definition. Three political economy models justify the �rst condition for a country to be democratic in this paper: the chief
1. Other prioritized interventions were reproductive health, HIV/AIDS prevention, the treatment of tuberculosis and sexually transmitted diseases.
2. World Bank (Undated) also notes that “the malaria case fatality per 1000 admissions rose from 38.7 in 1993 to 63.7 in 1995” (page 9). However, this rise may re�ect an increased usage of health care centers by seriously ill malaria patients.