ETV in Hydrocephalus and It`s Problem.
Sri Maliawan , MD, Phd.
Department of Neurosurgery Udayana University, Denpasar Bali, Indonesia.
Introduction
Hydrocephalus are common problem of pediatric neurosurgeon is almost 50%. The incident of
hydrocephalus in western country 2/1000 live birth, in my country 10/1000 live birth, the definitive
treatment is liquoral drainage such as VP shunt and ETV with all it complication and consequences.
Hydrocephalus is an intracranial pressure increase by the cerebrospinal fluid (CSF) accumulation
due to imbalance of the CSF production and absorption in the brain ventricle system.11,12
Hydrocephalus could be categorized into two groups i.e. Obstructive Hydrocephalus (OH) and
Communicants Hydrocephalus (CH).16
Hydrocephalus prevalence is high in the world; in Dutch it was reported about 0,65 per mil
annually and in USA, about 2 per mil annually13.Meanwhile in Indonesia, reached 10 per mil7,8.Etiology
are congenital hydrocephalus present at or soon after birth, many have aquaduct stenosis,
Dandy-Walker malformation, holoprosencephaly, or other more generalized malformation of brain
development. The diagnostic of choice is CT scan, or MRI. The Definitive treatment as a gold standard is
VP shunting. The catheter is added with pressure regulated cleft and the CSF diverses through one way
system which is absorbed by the peritoneum to the blood. Some complications might occur such as.
shunt device disconnection, cut off, skin or gut erosion by the device, over shunting, under shunting, proximal or distal blocked, not properly placed, subdural hemorrhage, and infection.14The complication
within the first month is 25-50 %, then, 4-5 % annually and each time the complication occurs it means
The surgery using ETV technique principally is CSF diversion from the third ventricle bottom to
the interpeduncular cistern in the subarachnoid space posterior to the sella. In ETV there is no device to
be planted, by then the CSF flow is made as almost as physiologic flow to be absorbed at arachnoid villi.
ETV is only for OH. Various studies have shown different successful rate from 40 - 100 %.2,10,18. In OH
cases below 2 years old with ETV have a 70% clinical improvement and 63% radiological improvement,
meanwhile for greater than 2 years old have a 100% clinical improvement and 73% radiological
improvement.3,5,15, 17. In Infantile hydrocephalus successful rate is 46% and 64-74% for the age greater
than 2 years old. In Indonesia, especially in Bali the main problem is the cost of the device which is
relatively expensive moreover there is a replacement on revision surgery that will cost the family a lot.
The advantage of ETV technique is that the procedure is only once, cheaper and simple, very
ideal for Indonesian people. In Sanglah Hospital, Bali the ETV procedure was done for the first time on
7thMarch 2005 and also for the first time in Indonesia. Regarding these techniques, attention should be
given seriously, in order to select the safety method for clinicians to treat OH cases. Based on this
thinking, the author tried to determine the effectivity of the 2 techniques; the most effective one could
be used for OH cases or for the Gold Standard in the management of Obstructive Hydrocephalus.
The second up to the fourth day after ETV, CSF absorption by the arachnoidea villi has been
enough. By the ETV, it is possible to open the drainage system and if the arachnoidea villi are still
functioning, in the period of 2-4 days for the physiologic drainage system for recovery, and on the day
7thoptimal function is reached.9,17.
Material
The incident of hydrocephalus in Bali and Nusa Tenggara (1992-2010) 1020 cases average 4
cases/month, 4/1000 live birth. The main problem is most of them come in late stage with giant head,
malnourish, and of course low social economic parent.
Research Methods
Target population are all patients on age of 0 month until 12 years old, who underwent shunting
hospitalized in Sanglah General Hospital. This research is an experimental one with randomized pre-test
post-test control group design. The sample size was counted by Pocock formula. All study activities were
carried out at Central Hospital Denpasar. Then K-S normality test, t-test group and Mann Whitney test
were conducted. All of 1020 cases were treated by VP shunt. A randomized study comparing VP shunt
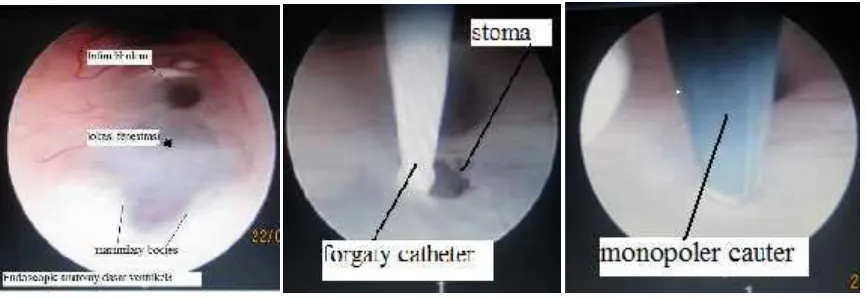
and ETV (Figure. 1) on 180 cases.
Figure 1. Endoscopic Third Ventriculostomy procedure.
Patients already diagnosed with hydrocephalus based on clinical findings and radiologic findings
(CT scan or MRI). There are enlargement of right and left lateral ventricle (Figure. 2). Third ventricle on
sagittal plane, there is clear and enough gap between clivus and basilar artery (below floor of third
ventricle). This gap is important so the endoscope able to move safely without injured the lateral wall of
third ventricle. Age, etiology of hydrocephalus, previous VP shunt surgery, and meningitis are relative
Figure 2. Enlarged Third Ventricle on CT scan and Gap between Clivus and Basillar Artery
It is very important to understand anatomy of Liliquest membrane in order to treat
hydrocephalus, especially when dealing with ETV procedure. Successful ETV will produce direct
connection between third ventricle an subarachnoid space; through interpeduncular cistern and pre
pontine cistern. This shunting will drained CSF to the subarachnoid space (absorb system).
Clinical Outcome
Miele et al. (2004) also found dysfunction and malfunction of VP shunting. Dysfunction can be happened
on distal, proximal, or both. 25% shunt dysfunction is due to distal abdominal complication. Similar
findings also reported that infection can be happened after intracranial ventricle complication; rate of
infection is 1.5-38%. There are report infection is caused not only because of tube, become foreign body
that trigger body response to the implant. There are possibilities about commensal bacteria that stick to
the implant tube, becoming adhesion of bacteria to the environment, colonization of bacteria, and in
the end they will stimulate shunt infection. Generally, VP shunt failure rate is 31.3% in first year and
gradually increase 4.5% every year.
It is suggested that Cytokines pro inflammation level in VP shunting group post-operative is
higher than ETV group, related with a permanent device implant. Cytokines pro inflammation can induce
neuroglia to express NGF; and proved that NGF level in VP shunting group is significantly higher than
ETV group.
In this research, findings have a close relationship with the clinical outcome of 6 months
post-operation, in which the better clinical improvement is significantly in ETV group compared to VP
shunting group. Clinical improvement examined included diplopia (strabismus convergen), sunset phenomena, muscle spasticity, motor respond, and verbal respond with p<0,05. Except in open eye
respond that was not significant (p>0,05).1
ETV successful rate 90% compared to VP shunt 60% after 6 month follow up. This paper will discuss the
detail problem regarding, the diagnostic, treatment, follow up, when do we decide not to treat
hydrocephalus, and last but not least is the possibility to reconstruct the giant head of hydrocephalus.
Conclusions
ETV successful rate, follow up six month better than VP shunt, for giant hydrocephalus reconstruction of
head should be consider for the first choice of treatment, VP shunt only for those who does not
response to ETV.
Acknowledgement
We gratefully acknowledged Antonio Pieri (pediatric neurosurgeon) from Italy, who patiently supervised
me in treating the patient with ETV, and Idanna Pucci who donor all of ETV equipment.
References
1. Andersson, S., Persson, E. K., Aring, E., Hård, A. L., Uvebrant, P., Dutton, G., and Hellström, A. Abnormal Visual Functions in Children with Hydrocephalus. Cerebrospinal Fluid Research. 2004; I (Suppl I): S9.
2. Bergsneider, M., Egnor, M.R., Johnston, M., Kranz, D., Madsen, J. R., McAllister II, J.P., Stewart, C., Walker, M.L., and Williams, M. A. What We Don t (but Should) Know about Hydrocephalus. J. Neurosurg. 2006; (3 Suppl Pediatrics) 104:157 159.
3. Decq, P., Le Guerinel, C., Palfi, S., Djindjian, M., Keravel, Y., and Nyuyen, J. P. A New Device for Endoscopic Third Ventriculostomy. Technical Note, J. Neurosurg. 2000; 93:509 512.
4. Gaab, M. R., and Schroeder, H. W. S. Neuroendoscopic Approach to Intraventricular Lesions. J. Neurosurg. 1998; 88:496 505.
5. Ishimaru, H., Takahashi, A., Ikarashi, Y., and Maruyama,Y. NGF Delays Rather than Prevents the Cholinergic Terminal Damage and Delayed Neuronal Death in the Hippocampus after Ischemia. Brain. Res. 1998; 789:194-200.
6. Kossmann, T., Stahel, P. F., Lenzlinger, P. M., Heinz, R., Rolf, W. D., Otmar, T., Guenter, S., and Morganti-Kossmann, M. C. Interleukin-8 Released into the Cerebrospinal Fluid After Brain Injury is Associated with Blood-Brain Barrier Dysfunction and Nerve Growth Factor Production. Journal of Cerebral Blood Flow and Metabolism.1997; 17: p. 280 289.
Conjunction with The World Federation of Neurological Societies (WFNS). Nusa Dua, Bali Indonesia. 2006; 42.
8. Maliawan, S., Asadul.A.I., Mahadewa. T. The Clinical Improvement between Ventriculoperitoneal Shunt and Endoscopic third Ventriculostomy. World Federation of Neurosurgical Societies, 13th Interim Meeting/The 12th Asian- Australian Congress of Neurological Surgeons. November, 2007; 18-22. EP18-6-1.
9. Nishiyama, K., Mori, H., and Tanaka, R. Changes in Cerebrospinal Fluid Hydrodynamics Following Endoscopic Third Ventriculostomy for Shunt-Dependent Noncommmunicating Hydrocephalus. J. Neurosurg. 2003; 98:1027-1031.
10. O Brien, D.F., Hayhurst, C., Pizer, B., and Mallucci, C.L.2006. Outcomes in Patients Undergoing Single-Trajectory Endoscopic Third Ventriculostomy and Endoscopic Biopsy for Midline Tumors Presenting with Obstructive Hydrocephalus. J. Neurosurg. 2006; (3 Suppl Pediatrics) 105:219 226.
11. Piatt, J. H. Jr., and Carlson, C. V. A Search for Determinants of Cerebrospinal Fluid Shunt Survival: Retrospective Analysis of a 14 Year Institutional Experience. Pediatr. Neurosurg. 1993; 19:233 242.
12. Piatt, J. H. Jr. About Hydrocephalus: For Parents and Patients. Drexel University College of Medicine.2003.
13. Platenkamp., M., Hanlo, P. W., Fischer, K., and Gooskens, R. H. J. M. Outcome in pediatric hydrocephalus: a comparison between previously used outcome measures and the Hydrocephalus Outcome Questionnaire. J Neurosurg. 2007; (1 Suppl Pediatrics). 107:26 - 31. 14. Sherman, C.S., Wensheng, Guo. A Mathematical Model of Survival in a Newly Inserted
Venticular Shunt. J. Neurosug. 2007; (6 Suppl. Pediatics) 107: 448 454.
15. Singh, D., Gupta, V., Goyal, A., Singh, H., Sinha, S., Singh, A., and Kumar, S. 2. Endoscopic Third Ventriculostomy in Obstructed Hydrocephalus. Neurol. India. 2003; 51:39-42.
16. Suny, Suny Upstete Medical University, Last Modified: 2003;March 26.
17. Van-Aalst, J., Beuls, E. A. M., Van Nie, F. A., Vles, J.S.H., and Cornips, E. M. J. Acute Distortion of the Anatomy of the Third Ventricle during Third Ventriculostomy Report of Four Cases. J Neurosurg, 2002; 96: 597 599.