Dengue Fever
What is Dengue?
Is an acute fever producing infectious disease
Mostly found in the tropics
Complications can be fatal
It is also known as Dengue fever , breakbone fever or
Dengue hemorrhagic fever
Dengue Virus
• Flavivirus (single-stranded RNA virus)
• Spherical, 40-50 nm (dia.) viral particle
– 3 Structural (E, C, M) proteins
– 7 Nonstructural (NS1, NS2A, NS2B, NS3, NS4A, NS4B, NS5)
• 5 serotypes
– DENV 1 through 5
– Multiple genotypes per serotype
• Common progenitor 1,000 years ago
• Serotypes have further divergence
– 62 to 67% homology based on amino acid sequence
• Varying pathogenicity based on serotype
History of Dengue
•
Clinical descriptions date as far back as 992 AD
in China
•
David Bylon (Batavia) in 1779
– knokkelkoorts --- joint fever
•
Benjamin Rush
– Termed breakbone fever
– Comes from Swahili ka dinga pepo
meaning a sudden cramp like seizure
and plague
Thomas S Advances in Virus Research 2003.
History of Dengue
•
Viral etiology suggested in early 1900
’
s by
Ashburn and Craig
•
DENV-1 and 2 isolated during World War II
•
1956 outbreak in Manila led to identification of
DENV-3 and DENV-4
•
Dengue hemorrhagic fever recognized since
1950
’
s
•
DENV-5 discovered in Sarawak 2013
Thomas S Advances in Virus Research 2003. Kyle J Annu Rev Microbiol 2008. 62:71-92.
Transmission of Dengue
A mosquito is the biological vector
This mosquito is the obligate intermediate
host for some viruses
Aedes albopictus/aegypti
are generally
associated with the spread of dengue fever
Akram, W., (n.d.). Aedes as a vector of Dengue: a possible threat to our lives. Khwarzimig Science Society. University of Agriculture, Faisalabad. Retrieved April 19, 2010 from
Aedes albopictus
Aedes aegypti
life cycle
2-7 days
>4 days 2
days
Classification of Dengue
Old WHO classification New WHO classification
Classical Dengue Fever Probable dengue ( group A - OPD
management) Dengue Fever with hemorrhagic
manifestations
Dengue with warning signs ( Group B - inward observation and management)
( patients are admitted for social reasons and when they are in high risk category)
DHF grade one
DHF grade two
DHF grade three Severe Dengue ( Group C
-resuscitation and management) 1. With compensated shock 2. With hypotensive shock
3. With severe organ impairment DHF grade four
Diagnosis for Dengue
Travel history and symptom profile
Detection of antibodies against the virus: IgM, IgG
Complete blood count
Chemistry panel
Liver function test
Occult blood in stool
DIC panel
Dengue rapid test NS1
PCR
Price, D.D., Wilson, S.R., (2009). Dengue fever: differential diagnoses and workout. Medscape. Retrieved April 19, 2010 from http://emedicine.medscape.com/article/781961-diagnosis
Immune Response & Dengue diagnosis
Acute Acute
Convalescent Convalescent
Day 0 7
NS-1: Effective days 1-5 post onset of symptoms
IgM/IgG: Effective after day 5
A diagnostic capable of detecting both is desirable
Rapid Diagnostic Tests (RDT
’
s)
Important for:
• Quick diagnosis (lab results take time and require labs)
• In resource-limited settings • Alerts a unit to ID threats
• Helpful for triage during outbreaks • Curtail geographic spread of
infectious diseases
• Stability operations and infrastructure building
Worldwide demand for better diagnostics to manage treatment and prevention Current RDT’s
Future RDT’s
Slide courtesy of Dr. Subhamoy Pal
#1: IgG/IgM Dengue Duo Cassette
10μL of serum, plasma, or whole blood
15 minute (time to result)
10 uL of serum
1.5 hours Wu et. al. CDLI 2000, pp 106-109
Product Introduction
#2: NS-1/IgG/IgM Dengue Duo
Cassette
120μL of serum or plasma 15 minute (time to result)
Product Introduction cont'd
Osorio et al. Virology Journal 2010, 7:361
Slide courtesy of Dr. Subhamoy Pal
Standard Diagnostics Dengue Duo (NS-1) RDT
NS1 Ag
3 drops (110 μl) of plasma or serum for early acute phase samples (day 1 ~5)IgG/IgM Ab
10 μl of plasma or serum for early convalescence phase samples (after day 5 ~ 14)
Ag
Treatment for Dengue
No specific therapeutic agents exist for dengue
infections
Bed rest and hydration therapy
Fever control with acetaminophen. Narcotics may be
necessary if headaches are very severe
Aspirin should be avoid because of anticoagulant
properties, children should avoid aspirin when a viral
infection is suspected
Monitoring of signs and symptoms for warning signs of
DHF or DSS
Price, D.D., Wilson, S.R., (2009). Dengue fever: differential diagnoses and workout. Medscape. Retrieved April 19, 2010 from http://emedicine.medscape.com/article/781961-diagnosis
Geographic distribution of Dengue
•
Dengue disease occurs in tropical and subtropical
areas
•
Endemic in over 100 countries in the Caribbean,
South, Central and North America, Africa, the
Pacific Islands, Hawaii, Asia, Eastern
Mediterranean and Australia
•
Before 1970 only nine countries had experience
dengue hemorrhagic fever epidemics, a number
that had increased more than four-fold by 1995
Geography distribution of Dengue
Blue dot: Geographic extension of dengue 2000-2007 Blue shaded areas: Risk of dengue transmission
Lines: Lines demarcate the area where the vector for dengue exists
Suitability for Dengue Transmission
High suitability
Low suitability
Unsuitable or nonendemic
Estimated Burden of Dengue by
continent (2010)
Estimated annual economic burden in
SE Asia (in million USD 2010)
Economic burden of dengue
• Significant Economic Burden
– Direct and Indirect costs
– SE Asia: 1,300 disability-adjusted life years
• DHF in Thailand: $19 to $51 (US) Million/year
– Similar to TB, other childhood and tropical diseases – 1981 Cuban DF/DHF/DSS epidemic
• $103 Million (US), including control measures ($43 Million) and medical services ($41 Million)
– Puerto Rico DF/DHF/DSS annual
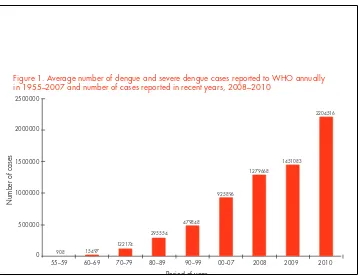
Figure 1. Average number of dengue and severe dengue cases reported to WHO annually in 1955–2007 and number of cases reported in recent years, 2008–2010
2500000
Number of cases
55–59 60–69 70–79 80–89 90–99 00–07 2008 2009 2010
Period of year
908 15497
Natural history of Dengue
Natural history of Dengue
Susceptible host
Time
Incubation period
Exposure Onset
Latent Infectious Non-infectious Infected
Non infected
Clinical horizon Death
Cure
Global Strategy
GOAL:
TO REDUCE THE BURDEN OF DENGUE
OBJECTIVES:
UÊ /ÊÀi`ÕViÊ`i}ÕiÊÀÌ>ÌÞÊLÞÊ>ÌÊi>ÃÌÊxä¯ÊLÞÊÓäÓäI UÊ /ÊÀi`ÕViÊ`i}ÕiÊÀL`ÌÞÊLÞÊ>ÌÊi>ÃÌÊÓx¯ÊLÞÊÓäÓäI UÊ /ÊiÃÌ>ÌiÊÌ iÊÌÀÕiÊLÕÀ`iÊvÊÌ iÊ`Ãi>ÃiÊLÞÊÓä£x IÊ/ iÊÞi>ÀÊÓä£äÊÃÊÕÃi`Ê>ÃÊÌ iÊL>Ãii°
Technical element 1:
Diagnosis and case management
Technical element 2:
Integrated surveillance and outbreak preparedness
Technical element 3:
Sustainable vector control
Technical element 4:
Future vaccine implementation
Technical element 5:
Basic operational and implementation
research
ENABLING FACTORS FOR EFFECTIVE IMPLEMENTATION OF THE GLOBAL STRATEGY:
UÊ >`ÛV>VÞÊ>`ÊÀiÃÕÀViÊLâ>ÌÊ
GLOBAL STRATEGY
Case management
• Improve case management and diagnosis to prevent deaths
from dengue
– Improve early clinical case detection for dengue with
warning signs and severe dengue;
– Improve management of severe cases.
• Improve capacities to facilitate a reduction in the burden of
the disease
– Improve access health care services;
– Reorganization of health service for better managing
outbreak situations;
– Establish QA in both the private and the public sector;
Surveillance and outbreak preparedness
•
Improve surveillance to enhance reporting,
prevention and control of dengue
– Surveillance indicators – for clinical reasons, a minimum
set of indicators should be reported;
– Risk indicators:
• Mosquito breeding sites (i.e. household water storage containers, poor urban water drainage)
• Environmental control measures (i.e. tightly fitting water storage lids, presence of fish or other biological control measures, and regular cleaning containers)
– sentinel sites for age- stratified seroprevalence and burden
of disease (including economic costs).
Surveillance and outbreak preparedness
•
Outbreak preparedness (10 priority area)
1. Establish a multisectoral dengue action committee
2. Formalize an emergency action plan 3. Enhance disease surveillance
4. Perform diagnostic laboratory testing 5. Enhance vector surveillance and control
6. Protect special populations and reduce the impact 7. Ensure appropriate patient care
8. Engage the community in dengue control and ensure participation in dengue prevention and control 9. Investigate the epidemic
10. Manage the mass media.
Sustainable vector control
•
Combination of:
–
Environmental management
–
Biological control
New vaccine
DENGVAXIA®
(Sanofi Pasteur)
Phase&3&Trials&of&CYD.TDV&
Adapted!from!Guy%(2015)%
DENGVAXIA®
(Sanofi Pasteur)
DENGVAXIA®
(Sanofi Pasteur)
VE&against&DENV1.4&by&age&(ITT&–&M0.M25)&
Study&PopulaXon& CYD14& (2.14&years)&
CYD15& (9.16&years)&
All&ages& 54.8%
&
(46.8F61.7)!
64.7%
&
(58.7F69.8)!
2.5&years& 33.7%
&
(11.7F50.0)!
NA!
6.11&years& 59.5%
&
(48.9F68.0)!
61.7%
&
(52.3F69.3)!
12.16&years& 74.4%
&
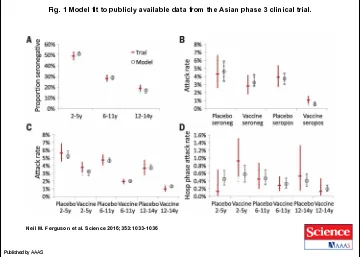
Fig. 1 Model fit to publicly available data from the Asian phase 3 clinical trial.
Neil M. Ferguson et al. Science 2016;353:1033-1036
Published by AAAS