EFFECT OF SPRING GRIP ACTIVE ASSISTIVE ROM EXERCISE ON UPPER EXTREMITIES MUSCLE STRENGHTH IN ISCHEMIC STROKE PATIENTS
Prapti, N.K.G., Armini, N.K.S., Azis, A.
ABSTRACT.
Stroke is the second leading cause of death in the world after heart disease, it also the number one cause of disability in both the developed and developing countries. Approximately 85% of stroke patients admitted to hospital with problems at their upper limb. The physical impairments of stroke such as a muscle weakness, pain, and spasticity was leading to a declinement of the ability to use the stroke-affected upper limb in daily activities. Therefore upper extremity needs to be trained, One form of its training by using the spring grip device. Gripping exercises using spring grip device are performed actively and assisted. This study aims to find out the effect of ROM active assisted spring grip exercise toward the strength of upper extremity muscle in ischemic stroke patients at IRNA D Sanglah Hospital. This is a pre test - post test design study with a control group. This study held for 6 days with treatment twice daily. The 30 respondents were taken as a subjects in this study that consists of 15 patients of the treatment group and 15 patients as a control group . The results of an statistical paired t-test obtained p value = 0.000 (< 0.05). So it can be concluded that there is an effect of ROM active assisted spring grip exercise to the changes of muscle strength between pre and post ROM active assisted spring grip exercise at IRNA D Sanglah Hospital . Based on the above results suggested to the hospital to consider apply ROM active assisted spring grip exercise in ischemic stroke patients.
Background and Significant of the Problem
Stroke is the number two cause of death in the world after heart disease, and is the
number one cause of disability in both developed countries and in developing countries (America
Heart Association [AHA], 2010). According to Health Research (2008), the stroke becomes first
cause of death rank in Indonesia in 2011. Based on the profile of Bali provincial health
department in 2010, patients with cerebral infarction were hospitalized in Bali amounted to 968
people. While data from Center General Hospital (RSUP) Sanglah the period January to June
2013 states that in a month, stroke patients who are hospitalized have an average number of 37
people. Based on preliminary studies that have been conducted on July 1, 2013, the number of
stroke patients who are hospitalized in Inpatient D (IRNA D) Sanglah approximately in a month
period from April to June 2013 a number of 32 people with the average amount of suffering an
ischemic stroke as much as 24 people per month, in the age range 30 to 80 years.
Stroke becomes a major problem of movement disorders and body function in adults
(Irfan, 2010:69). About 85% of stroke patients who are hospitalized have muscle weakness, pain,
and spasticity so that impact on decrease in the ability to indulge. Decrease in ability impacts on
the loss of muscle strength, decrease in range of motion and fine motor skills (Eng & Harris,
2009).
Recovery of upper extremity muscle strength and returns of joint flexibility require
rehabilitation as soon as possible after the patient's condition is considered stable (Waluyo,
2009:106). Rehabilitation can be given to patients is the exercises of motion range or
Range of
Motion
(ROM). Allotment of training is preferred on specific skills that are meaningful to
patients with stroke (Smeltzer & Bare, 2002:399, Susilawathi, 2013:56), such as; grasping,
holding, and lifting objects (Irfan, 2010:203, Mehrholz, 2012: 75). Irfan (2010) and Mehrholz
(2012) state that one of the forms of specific exercise that can improve upper extremity muscle
strength and can restore hand function is to use the tool of spring grip by way of gripped.
Based on the results of preliminary studies that were conducted in Sanglah Hospital,
ROM passive rehabilitation has been done by the therapist once a day in the morning, but not
optimal due to limitation of personnel therapist. Nurse who is in charge in the area of stroke has
a major role to train the patient due to 24 hours near the patient. Based on the above presentation,
researcher is interested in knowing the effect of spring grip exercise active assistive to the upper
RESEARCH METHODS
This study is quasy-exsperimental research with pretest-posttest design with control group.
Collecting data in this study is conducted on patients with stroke ischemic who experience weakness in
the upper extremities. Measurements of muscle strength in patients with stroke ischemic are conducted
before and after given intervention by using Handgrip dynamometer. The sample in this study consisted
of 15 people who are given ROM exercises according to the procedure in the hospital and added to the
Spring grip active assistive exercise that is conducted twice a day and 15 others as a control group get
only ROM exercises according to the procedure in Sanglah Hospital. The analysis that is used in this
study is a parametric test.
RESEARCH RESULT
Characteristics of Respondents
In this research, the characteristics of respondents are categorized by sex, age, and history of
stroke that can be described as follows:
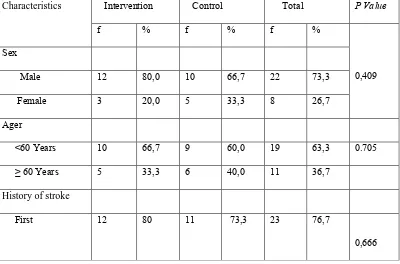
Tabel 1 the characteristics of respondents
Characteristics Intervention Control Total P Value
f % f % f %
0,409 Sex
Male 12 80,0 10 66,7 22 73,3
Female 3 20,0 5 33,3 8 26,7
Ager
<60 Years 10 66,7 9 60,0 19 63,3 0.705
≥ 60 Years 5 33,3 6 40,0 11 36,7
History of stroke
First 12 80 11 73,3 23 76,7
Repeated 3 20 4 26,7 7 23,3
The sex of respondents are either the treatment group or the control group are mostly male with age <60
years and most of them suffered first stroke. The p value of each characteristic of respondents is more
than 0.05, so it can be concluded that the sample is homogeneous.
Upper Extremity Muscle Strength in the Treatment Group and Control Group Before Given Intervention
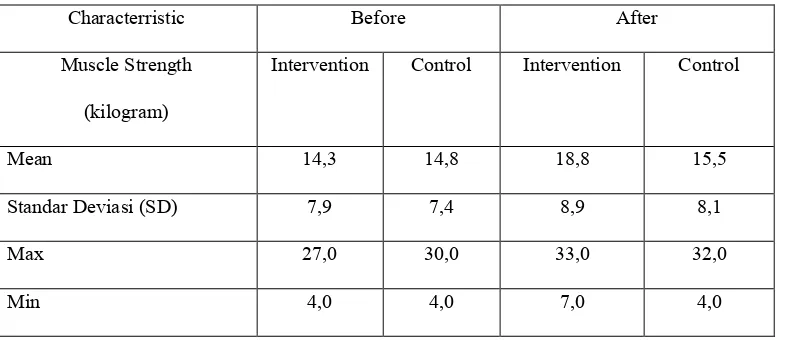
Tabel 2 Upper extremity muscle strength in stroke ischemic patients
Characterristic Before After
Muscle Strength
(kilogram)
Intervention Control Intervention Control
Mean 14,3 14,8 18,8 15,5
Standar Deviasi (SD) 7,9 7,4 8,9 8,1
Max 27,0 30,0 33,0 32,0
Min 4,0 4,0 7,0 4,0
Before the intervention, respondents in the treatment group had an average of upper extremity
muscle strength of 14.3 kg (SD ± 7,9), while the control group had an average of upper extremity muscle
strength of 14.8 kg (SD ± 7,4). After given the intervention (post test), the treatment group on average
muscle strength reached 18.88 kg (SD ± 8,9), while the control group with an average of 15.5 kg (SD ±
8,1).
Upper Extremity Muscle Strength in the Treatment Group and Control Group After Given Intervention
Tabel 3 Muscle strength of upper extremitas in stroke iscemic patients
Induicator muscle strength
(Kilogram)
Group z P Value
Mean 4,5 0,7 -4,763 0,000
Standar Deviasi 1,4 0,9
Max 7,0 2,0
Min 3,0 0,0
Changes in muscle strength before and after given the intervention in the treatment group had an
average of 4.5 kg (SD ± 1,4), while the control group had an average change of 0.7 kg (SD ± 0,9). Results
of statistical test by using Mann Whitney test (data not normally distributed) showed a p-value of 0.000 (p
<0,05), which means that Ho is rejected or, in other words there is a significant difference between the
allotment of spring grip active assistive ROM exercise to the upper extremity muscle strength.
The Effect of Spring grip active assistive Exercise to the Upper Extremity Muscle Strength in Ischemic Stroke Patients
These results indicate that allotment of Spring grip active assistive exercise to the muscle
strength had increased by an average of 4,5 kg, while in the allotment of ROM exercises had increased
only give muscle strength an average of 0,73 kg. Which in this study, the allotment of Spring grip active
assistive ROM exercise has an influence on the increase of muscle strength which is greater than the
ROM exercise.
This research is in line with research that is conducted by Santoso (2013), which indicates that
there are differences in the effectiveness of active ROM with ROM assistive active (spherical grip) (p
value 0,046). Exercise is physical activity to make the condition of the body, improve health, and
maintain physical health. Exercise is also used as a treatment for overcoming deformities, or restoring the
entire body to maximum health status. If a person exercises, there will be a physiological change in the
body system. According to Kozier, et al. (2008) exercise has several objectives, including for repair,
maintenance and increase muscle strength, maintain and improve the flexibility of joints. ROM exercises
and spring grip are part of the exercise that are focused on improving muscular strength, especially in
patients who have a weakness in the upper extremities.
A similar study is done by Anggraini (2013) who get the result that the handling precision
assistive active exercise can increase fingers muscle strength of non-hemorrhagic stroke patients (p =
hospitalized to improve the outcome. Selection of the type of therapy is adapted to the conditions of
experienced stroke and the patient needs to be independent. The greater intensity of therapy can speed up
the recovery process and produce in better functional ability. Exercises are given precedence on the
specific skills that are important and meaningful for patients with stroke (Susilawathi, 2013:56).
Rehabilitation for upper extremity that can be given to people is the range of motion exercises or Range
of Motion (Smeltzer & Bare, 2002:399), but it can be given a specific rehabilitation that can increase
muscle strength and to restore a hand functional. Exercise by grasping, holding, lifting objects, one form
of exercise can use the grip spring tool. (Irfan, 2010:203, Mehrholz, 2012:75).
Conclusion
Allotment of Spring grip active assistive ROM exercises has a greater increase than the ROM exercise
only (0,73 kg and 4,5 kg). It can be concluded that the Spring grip active assistive exercise has a better
effectiveness than the ROM exercise only.
Suggestion
It is expected to health workers on the use of spring grip as an additional tool in conducting the
rehabilitation of the upper extremity in order to accelerate the muscle strength recovery of patients with
ischemic stroke.
REFERENCES
Agustini. (2012). Effect of Exercise Ball Against Grip strength Upper Extremity Muscles In Ischemic Stroke Patients in Sanglah Hospital in Denpasar, research has not been published.
Anggraini. (2013). Effect of Exercise Active assistive Precision Handling Of Muscle Strength Radius Hands On Non Haemorrhagic Stroke Patients at Dr Sanglah, research has not been published.
Indrawati, (2007). Differences Influence of Motion Against Muscle Strength Exercise in Patients with Non-Haemorrhagic Stroke Hemiparese Right Compared with Hemiparese left in the Hospital Dr. Moewardi Surakarta, (Online), http://eprints.undip.ac.id/14217/, diakses 15 Agustus 2013.
Irfan, M. (2010). Fisioterapi for Insan Stroke. Yogyakarta: Graha Ilmu.
Mehrholz. (2012). Physical Therapy for the Stroke Patient. New York: Thieme.
Nurbaeni, dkk. (2010). ROM exercises on Arm Improves muscle strength in Post-Stroke Patients in RSU Dr. Kusuma Wijaya Soedono Madiun, (online), http://alumni.unair.ac.id, access on 15Agustus 2013.
Santoso, (2013). Differences ROM Active and ROM Active assistive (Spherical Grip) of the Upper Extremity Muscle Strength Non Haemorrhagic Stroke Patients In Sub Karanganyar Pekalongan, (online), http://www.digilib.stikesmuh-pkj.ac.id, access on 21 Februari 2014.
Sugiyono, (2012). Education Research Methods Quantitative and Qualitative Approaches. Bandung: Alfabeta.