EMERGENCY MEDICINE
INTRODUCTION
Emergency Medicine has long been established especially in Australasia, Canada, Ireland, the United Kingdom and the United States, in Asia othe emergency medicine officially inauguration of Asian Society of Emergency Medicine in Singapore on the 24th of October 1998 at the first Asian Conference on Emergency Medicine which as Prof.DR.dr. Eddy Rahardjo,SpAnKIC and dr. Tri Wahyu Murni sat as member of Board Director.
It is thus sometimes seen to be synonymous with emergency medical care and within the province and expertise of almost all medical practitioners. However, the Emergency Medicine incorporates the resuscitation and management of all undifferentiated urgent and emergency cases until discharge or transfer to the care of another physician. Emergency Medicine is an inter-disciplinary specialty, one which is interdependent with all other clinical disciplines. It thus complements and does not seek to compete with other medical specialties.
Basic science concepts to help in the understanding of the phatophysiology and treatment of disease.The medical curriculum has become increasingly vertically integrated, with a much greater use of clinical examples and cases to help in the understanding of the relevance of the underlying basic science, The Emergency Medicine block has been written to take account of this trend, and to integrate core aspects of basic science, pathophysiology and treatment into a single, easy to use revision aid.
In accordance the lectures that have been full integrated for studens in 6 Th semester,
period of 2012, one of there is The Emergency Medicine Block. There are many topics will be discuss as below:
Seizure and mental status changes, acute Psychiatric episode, Acute respiratory distress syndrome and failure, Bleeding disorders (epistaxis, dental bleeding, vaginal bleeding) ,Shock, Cardiac critical care (Cardiac arrest and CPR), Emergency toxicology and poisoning, Pregnancy induce Hypertension, Shoulder dystocia, Urologic concern in critical care, Phlegmon, Acute Blistering and Expoliative skin, Trauma which potentially disabling and Life threatening condition and Basic Clinical Skill
Beside those topics, also describes the learning outcome, learning objective, learning task, self assessment and references. The learning process will be carried out for 4 weeks (20 days).
Due to this theme has been prepared for the second time, so many locking mill is available on it. Perhaps it will better in the future
CURRICULUM CONTENTS
Mastery of basic knowledge with its clinical and practical implication.
Establish tentative diagnosis, provide initial management and refer patient with: Seizure and mental status changes
Acute Psychiatric episode
Acute respiratory distress syndrome and failure
Bleeding disorders (epistaxis, dental bleeding, vaginal bleeding)
Shock
Cardiac critical care (Cardiac arrest and CPR) Emergency toxicology and poisoning
Pregnancy induce Hypertension, Shoulder dystocia Urologic concern in critical and non critical care
Phlegmon
Acute Blistering and Expoliative skin
Trauma which potentially disabling and Life threatening condition
SKILLS
To implement a general strategy in the approach to patients with critical ill through history and physical examination and special technique investigations
To manage by assessing, provide initial management and refer patient with critical ill
PERSONAL DEVELOPMENT/ATTITUDE
Awareness to :
Ethic in critical care
Basic principle of critical care
The importance of informed consent to patient and family concerning critical ill situations
Risk of patient with critically ill and its prognosis
COMMUNITY ASPECT :
Communicability of the critical cases Cost effectiveness
PLANNERS
NO. NAME DEPARTMENT
1. Dr.dr. Tjok Gde Agung Senapathi, Sp.An KAR (Coordinator)
Anesthesiology and Intensive Terapy
2. Dr.dr. I Ketut Suyasa, SpB,SpOT(K)Spine Surgery
3. dr. IGN Budiarsa,SpS Neurology
4. dr.Sari Wulan,SpTHT-KL(K), dr.Wayan Sucipta, SpTHT-KL
ENT
5. drg. Putu Lestari Sudirman,M.Biomed Dentistry
6. dr. I Ketut Agus Somia, SpPD(KPTI) Internal Medicine
7. dr. Putu Andrika, SpPDKIC Internist
8. Dr.dr. Dyah Kanyawati, SpA(K) Pediatric
9. Dr.dr. Wayan Megadhana, SpOG(K) Obstetric-Gynecologic
10. dr. Endang Sriwidiyanti, SpOG Obstetric-Gynecologic
11. dr.I Gede Mega Putra, SpOG(K) Obstetric-Gynecologic
12. dr. Gede Wirya Kesuma Duarsa, SpU,MKes; dr.
Kadek Budi Santosa, SpU Surgery
13. Dr.dr.Cokorda Bagus Jayalesmana,SpKJ Psychiatric
14. dr. Nyoman Suryawati, SpKK Dermatology
15 16.
17.
18.
dr. Srie Laksminingsih SpR(K)
dr.IGAG Utara Hartawan,SpAn.MARS
dr. IGN Mahaalit Aribawa,SpAnKAR
dr. IA Sriwijayanti,M.Biomed,SpS
Radiology
Anesthesiology and Intensive Terapy Anesthesiology and Intensive Terapy Neurology
LECTURERS
NO. NAME DEPARTMENT PHONE
1. Dr.dr. Tjok Gde Agung Senapathi, Sp.AnKAR (Coordinator)
Anesthesiology and Intensive Terapy
081337711220
2. Dr. dr. I Ketut Suyasa, SpB, SpOT(K)Spine
Surgery 081558724088
3. dr. IGN Budiarsa,SpS Neurology 0811399673
4. dr.SariWulan,SpTHT-KL(K), dr.Wayan Sucipta,SpTHT-KL
ENT 081237874447(SW
)
08125318941 (WS) 5. drg. Putu Lestari Sudirman,
M.Biomed
Dentistry 081239885740
6. dr. I Ketut Agus Somia, SpPD(KPTI)
Internal Medicine 089617587075
7. dr. Putu Andrika,SpPDKIC Internist 08123989192
8. Dr.dr. Dyah Kanyawati, SpA(K) Pediatric 081285705152
19. Dr.dr. Wayan Megadana, SpOG(K) Obstetric-Gynecologic 08123917002
10. dr. Endang Sriwidiyanti, SpOG Obstetric-Gynecologic 081236745839
11. dr. I Gede Mega Putra, SpOG(K) Obstetric-Gynecologic 08123636172
12. dr.Gede Wirya Kesuma Duarsa, SpU,MKes; dr. Kadek Budi Santosa, SpU
Surgery (Urology) 08155753377
(GWK);
13. Dr. dr. Cokorda Bagus Jayalesmana, SpKJ
Psychiatric 0816295779
14. dr. Nyoman Suryawati, SpKK Dermatology 0817447279
15 16.
17.
18.
dr. Srie Laksminingsih SpR (K) dr. IGAG Utara Hartawan, SpAn. MARS
dr.IGN Mahaalit Aribawa, SpAn KAR
dr. IA Sriwijayanti,MBioMed,SpS
Radiology
Anesthesiology and Intensive Terapy Anesthesiology and Intensive Terapy Neurology
08164745561 08123868126
0811396811
081337667939
FACILITATORS
Regular Class (Class A)
No Name Group Departement Phone (2Venuend floor)
1
dr. A.A.Ayu Dwi Adelia Yasmin, M.Biomed, Sp.JP.FIHA
A1
Cardiology 087861402169 2nd floor:
R.2.09
2 dr. I G N Sri Wiryawan,
M.Repro A2
Histology 082341768888 2nd floor:
R.2.10
3 Ni Putu Wardani, Sp.An, M.Biomed A3 DME 08113992784 2nd floor:R.2.11
4 dr. Yukhi Kurniawan, Sp.And A4 Andrology 08123473593 2nd floor:R.2.12
5 dr. Putu Yuliandari, S.Ked A5 Microbiology 089685415625 2nd floor:
R.2.13
6 dr. Yuliana, M.Biomed A6 Anatomy 085792652363 2nd floor:
R.2.14
7 dr. Ida Bagus Putrawan, Sp.PD A7 Interna 081236194672 2nd floor:R.2.15
8 Dr.dr. Ni Putu Sriwidyani , Sp.PA A8 AnatomyClinical 081337115012 2nd floor:R.2.16
9 dr. Ni Luh Putu Ariastuti,
MPH A9
Public Health 0818560008 2nd floor:
R.2.20 10 dr. I Made Suka Adnyana, Sp.BP-RE A10 Surgery 081236288975 2nd floor:R.2.23
11 dr. I Dewa Ayu Inten Dwi Primayanti, M.Biomed A11 Fisiology 081337761299 3nd floor:R.3.20
12 dr. I Made Agus Kresna
Sucandra, Sp.An A12
Anasthesi 081805470888 3nd floor:
R.3.23
English Class (Class B)
No Name Group Departement Phone (2Venue nd floor)
1 Dr.dr. Tjok G A Senapathi, Sp.An. KAR B1 Anasthesi 081337711220 2nd floor:R.2.09
2 dr. Agung Nova Mahendra,
M.Sc B2
Pharmacology 087861030195 2nd floor:
3 Dr.dr. Ni Nyoman Sri
Budayanti, Sp.MK (K) B3
Microbiology 08553711398 2nd floor:
R.2.11 4 Dr.rer.Nat. dr. Ni Nyoman AyuDewi, M.Si B4 Biochemistry 081337141506 2nd floor:R.2.12
5 I Ketut Mariadi, Sp.PD B5 Interna 08123853700 2nd floor:
R.2.13
6 Dr.dr. Ni Made Linawati, M.Si B6 Histology 081337222567 2nd floor:
R.2.14 7 dr. I Wayan Aryabiantara, Sp.An. KIC B7 Anasthesi 08123822009 2nd floor:R.2.15
8 dr. Made Agus Dwianthara Sueta, Sp.B-KBD B8 Surgery 081338648424 2nd floor:R.2.16
9 Dr.dr. Susy Purnawati, M.KK B9 Fisiology 08123989891 2nd floor:
R.2.20
10 dr. Putu Aryani, MPH B10 Public Health 082237285856 2nd floor:
R.2.23
11 dr. I Made Oka Negara, FIAS B11 Andrology 085935054964 3nd floor:R.3.20
12 dr. I G A Sri Darmayani,
Sp.OG B12
DME 081338644411 3nd floor:
TIME TABLE
Regular Class (Class A)DAY/DATE TIME LEARNING ACTIVITY VENUE CONVEYER 1. Thu, 1 Sept 2016 08.00-09.00 Highlight in Emergency Medicine (Coordinator)
Class room Dr.dr. Tjok Gde Agung Senapathi, Sp.AnKAR
09.00-10.30
Individual Learning
- 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room Dr.dr. Tjok Gde Agung
Senapathi, Sp.AnKAR 2. Fri, 2 Sept 2016 08.00-09.00 Lecture 2. Status Epilepticus and Other Seizure
Disorders
Class room dr. IGN Budiarsa,SpS
09.00-10.30
Individual Learning
- 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project
14.00-15.00 Plenary Class room dr. IGN Budiarsa,SpS
3. Mon, 5 Sept 2016 08.00-09.00 Lecture 3. Coma and Decrease of Consciousness
Class room dr. Ida Ayu
Sriwijayanti,MBioMed,SpS 09.00-10.30 Individual Learning 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room dr. Ida Ayu
Sriwijayanti,MBioMed,SpS 4. Fri, 9 Sept 08.00-09.00 Lecture 4. Acute Psychiatric Episodes
2016 09.00-10.30
Individual Learning
10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room Dr.dr. Tjokorda Bagus
Jayalesmana,SpKJ 5. Tue, 13 Sept 2016 08.00-09.00 Lecture 5. Acute Respiratory Distress Syndrome and Failure
Class room dr. Putu Andrika, SpPDKIC, Dr. dr Dyah Kanya Wati,SpA (K), dr. Sucipta, SpTHT KL dr. Srie Laksminingsih, SpR 09.00-10.30 Individual Learning 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room ENT,
Pulmo, Pediatric, Radiology 6. Wed, 14 Sept 2016 08.00-09.00 Lecture 6. Bleeding Disorder(Epistaxis
, Hemorrhage In Pregnancy)
Class room dr Sari Wulan, SpTHT- KL(K),( and ENT Team) Dr.dr Wayan Megadhana, SpOG(K) (and OBGYN Team)
09.00-10.30
Individual Learning
- 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room dr Sari Wulan,
SpTHT-KL(K), ( and ENT Team) Dr.dr Wayan Megadhana, SpOG(K) (and OBGYN Team) 7. Thu, 15 Sept 2016 08.00-09.00 Lecture 7. Shock
Class room dr. IGAG. Utara Hartawan, SpAn MARS
dr.Nyoman
Budihartawan,MSc,SpA
09.00-10.30
Individual Learning
- 10.30-12.00
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room dr. IGAG. Utara Hartawan,
SpAn MARS dr.Nyoman Budihartawan,MSc,SpA 8. Mon, 19 Sept 2016 08.00-09.00 Lecture 8. Cardiac Arrest and
+
Cardiopulmonary Resuscitaton
Class room dr. IGN. Mahaalit Aribawa, SpAn KAR
09.00-10.30
Individual Learning
- 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room dr. IGN. Mahaalit Aribawa,
SpAn KAR 9 Tue, 20 Sept 2016 08.00-09.00 Lecture 9. Emergency Toxicology and Poisoning
Class room dr. IKetut Agus Somia, SpPD KPTI
09.00-10.30 Individual Learning
10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room dr. I Ketut Agus Somia,
SpPD KPTI 10. Wed, 21 Sept 2016 08.00-09.00 Lecture 10 Hypertension In Pregnancy
Class room dr. I Gede Mega Putra, SpOG(K)
09.00-10.30
Individual Learning
- 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room dr. I Gede Mega Putra,
SpOG(K) 11. Thu, 22 Sept 2016 08.00-09.00 Lecture 11. Shoulder Dystocia
Class room dr. Endang
Sriwidiyanti,SpOG
-10.30 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project
14.00-15.00 Plenary Class room dr. Endang Sriwidiyanti,SpOG
12. Fri, 23 Sept 2016 08.00-09.00 Lecture 12. Acute Blistering and Exfoliative Skin
dr. Nyoman Suryawati Sp.KK
09.00-10.30
Individual Learning
-
10.30-12.00 SGD Fasilitator
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary dr. Nyoman Suryawati
Sp.KK 13. Tue, 26 Sept 2015 08.00-09.00 Lecture 13. Trauma Which Potentially Disabling and life
Threatening Conditions
Dr.dr. Ketut Suyasa, SpB SpOT(K) Spine
dr. IGN Wien Aryana, SpOT
09.00-10.30
Individual Learning
- 10.30-12.00
SGD Disc room Fasilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Dr.dr. Ketut Suyasa, SpB
SpOT(K) Spine
dr. IGN Wien Aryana, SpOT 14 Mon, 27 Sept 2016 08.00-09.00 Lecture 14. Phlegmon
Class room drg. Putu Lestari Sudirman
09.00-10.30
Individual Learning -
- 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room drg. Putu Lestari
15 Tue, 28 Sept 2016 08.00-09.00 Lecture 15. Urologic Concern in Critical Care for
NonTrauma Case
Class room dr. Gede Wirya Kusuma
Duarsa, M.Kes, SpU(K)
09.00-10.30
Individual Learning
- 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room dr. Gede Wirya Kusuma
Duarsa, M.Kes, SpU(K)
16 Wed, 29 Sept
2016
08.00-09.00 Urologic ConcernLecture 16. in Critical Care for
Trauma Case
Class room
dr. Budi Santosa, SpU
09.00-10.30
Individual Learning -
- 10.30-12.00
SGD Disc room Facilitators
12.00-12.30 Break 12.30-14.00 Student Project 14.00-15.00
Plenary Class room dr. Budi Santosa, SpU
1 Thu, 30 Sept 2016 08.00-selesai Student Project Presentation and Examination Theater Room FK UNUD Team 2 Fri, 3 Oct 2016 08.00-selesai Student Project Presentation and Examination Theater Room FK UNUD Team 3 Mon, 4 Oct 2016
08.00-Finish Basic clinical skill(1) CPR (English Class and Regular)
Clinical skill
lab Team
4 Tue, 5 Oct 2016 08.00- Finish
Basic clinical skill (2)
Basic Trauma Care (English Class and
Fri, 7 Oct
2016
EXAMINATION
English Class (Class B) DAY/DAT
E
TIME LEARNING ACTIVITY
VENUE CONVEYER
1. Thu, 1 Sept
2016
09.00-10.00 Highlight in
Emergency Medicine (Coordinator)
Class room Dr.dr. Tjok Gde Agung Senapathi, Sp.AnKAR
10.00-11.30 Student Project
-11.30-12.00 Break
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room Dr.dr. Tjok Gde Agung
Senapathi, Sp.AnKAR 2.
Fri, 2 Sept
2016
09.00-10.00 Lecture 2.
Status Epilepticus and
Other Seizure Disorders
Class room dr. IGN Budiarsa,SpS
10.00-11.30 Student Project
-11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. IGN Budiarsa,SpS
3. Mon, 5 Sept
2016
09.00-10.00 Lecture 3.
Coma and Decrease of Consciousness
Class room dr. Ida Ayu
Sriwijayanti,MBioMed,SpS
10.00-11.30 Student Project
11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. Ida Ayu
Sriwijayanti,MBioMed,SpS 4.
Fri, 9 Sept
2016
09.00-10.00 Lecture 4.
Acute Psychiatric Episodes
Class room Dr.dr. Tjokorda Bagus Jayalesmana,SpKJ
10.00-11.30 Student Project
11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room Dr.dr. Tjokorda Bagus
5. Tue, 13 Sept
2016
09.00-10.00 Lecture 5.
Acute Respiratory Distress Syndrome and
Failure
Class room dr. Putu Andrika, SpPDKIC, Dr. dr Dyah Kanya
Wati,SpA (K), dr. Sucipta, SpTHT KL
dr. Srie Laksminingsih, SpR
10.00-11.30 Student Project
11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room ENT
Pulmo, Pediatric, Radiology 6. Wed, 14 Sept 2016
09.00-10.00 Lecture 6.
Bleeding Disorder(Epistaxi s, Hemorrhage In
Pregnancy)
Class room dr Sari Wulan, SpTHT- KL(K),( and ENT Team) Dr.dr Wayan Megadhana, SpOG(K) (and OBGYN Team)
10.00-11.30 Student Project
-11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room dr Sari Wulan, SpTHT-
KL(K),( and ENT Team) Dr.dr Wayan Megadhana, SpOG(K) (and OBGYN Team)
7. Thu, 15 Sept
2016
09.00-10.00 Lecture 7.
Shock
Class room dr. IGAG. Utara Hartawan, SpAn MARS
10.00-11.30 Student Project
-11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. IGAG. Utara Hartawan,
SpAn MARS 8.
Mon, 19 Sept
2016
09.00-10.00 Lecture 8.
Cardiac Arrest and + Cardiopulmonary
Resuscitaton
Class room dr. IGN. Mahaalit Aribawa, SpAn KAR
10.00-11.30 Student Project
-11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. IGN. Mahaalit Aribawa,
SpAn KAR 9
Tue, 20 Sept
2016
09.00-10.00 Lecture 9.
Emergency Toxicology and
Poisoning
Class room dr. Agus Somya, SpPD
KPTI
11.30-12.00 Break Disc room Facilitators 12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. Agus Somya, SpPD
KPTI 10.
Wed, 21 Sept
2016
09.00-10.00 Lecture 10.
Pregnancy Induce Hypertension
Class room dr. Gede Megaputra, SpOG(K)
10.00-11.30 Student Project
-11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. Gede Megaputra,
SpOG(K) 11.
Thue, 22 Sept
2016
09.00-10.00 Lecture 11.
Shoulder Dystocia
Class room dr. Endang
Sriwidiyanti,SpOG
10.00-11.30 Student Project
-11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. Endang
Sriwidiyanti,SpOG 12.
Fri, 23 Sept
2016
09.00-10.00 Lecture 12.
Acute Blistering and Exfoliative
Skin
dr. Nyoman Suryawati Sp.KK
10.00-11.30 Student Project
-11.30-12.00 Break Fasilitator
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary dr. Nyoman Suryawati
Sp.KK 13.
Tue, 26 Sept
2016
09.00-10.00 Lecture 13.
Trauma Which Potentially Disabling and life
Threatening Conditions
Dr.dr. Ketut Suyasa, SpB SpOT(K) Spine
dr. IGN Wien Aryana, SpOT
10.00-11.30 Student Project
-11.30-12.00 Break Disc room Fasilitators
12.00-13.30 Individual Learning
13.30-15.00 SGD
15.00-16.00 Plenary Dr.dr. Ketut Suyasa, SpB
SpOT(K) Spine
dr. IGN Wien Aryana, SpOT 14
Mon, 27 Sept
2016
09.00-10.00 Lecture 14.
Phlegmon
Class room drg. Putu Lestari Sudirman
10.00-11.30 Student Project -
-11.30-12.00 Break Disc room Facilitators
13.30-15.00 SGD
15.00-16.00 Plenary Class room drg. Putu Lestari Sudirman
15 Tue, 28 Sept
2016
09.00-10.00 Lecture 15.
Urologic Concern in Critical Care for NonTrauma
Case
Class room dr. Gede Wirya Kusuma
Duarsa, M.Kes, SpU(K)
10.00-11.30 Student Project
-11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning 13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. Gede Wirya Kusuma
Duarsa, M.Kes, SpU(K)
16 Wed, 29 Sept
2016
09.00-10.00 Lecture 16.
Urologic Concern in Critical Care for Trauma Case
Class room
dr. Budi Santosa, SpU
10.00-11.30 Student Project -
-11.30-12.00 Break Disc room Facilitators
12.00-13.30 Individual Learning 13.30-15.00 SGD
15.00-16.00 Plenary Class room dr. Budi Santosa, SpU
1 Thu, 30 Sept 2016 08.00-selesai Student Project Presentation and Examination Clinical skill lab Team 2 Fri, 3 Oct 2016 08.00-selesai Student Project Presentation and Examination Clinical skill lab Team 3 Mon, 4 Oct 2016 08.00-Finish
Clinical skill (1) CPR (English Class and Regular Class) Clinical skill lab Team 4 Tue, 5 Oct 2016 08.00-
Finish Clinical skill (2)Basic Trauma Care (English
Class and Regular Class)
Clinical skill
lab Team
7 Oct 2016
EXAMINATION
ASSESSMENT METHOD
Assessment will be carried out onthe day written according to class calendar. There will be 100 questions consisting mostly of Multiple Choice Questions (MCQ) and some other types of questions. The minimal passing score for the assessment is 70. Other than the examinations score, your performance and attitude during group discussions will be consider in the calculation of your average final score. Final score will be sum up of student performance in small group discussion (5% of total score) and score in final assessment (95% of total score). Clinical skill will be assessed in form of Objective structured clinical examination (OSCE) at the end of semester as part of Basic Clinical Skill Block’s examination.
STUDENT PROJECT
Students have to write a paperwork with topic given by the lecturer. The topic will be chosen randomly on the first day. Each small group discussion must work on one paperwork with different tittle. The paperwork will be written based on the direction of respective lecturer. The paperwork is assigned as student project and will be presented in class. The paper and the presentation will be evaluated by respective facilitator and lecturer.
Format of the paper :
1. Cover Title (TNR 16)
Name Green coloured cover Student Registration Number
Faculty of Medicine, Udayana University 2012
2. Introduction
3. Journal critism/literature review 4. Conclusion
5. References
Example :
Journal
Porrini M, Risso PL. 2005. Lymphocyte Lycopene Concentration and DNA Protection from Oxidative Damage is Increased in Woman. Am J Clin Nutr 11(1):79-84.
Textbook
Abbas AK, Lichtman AH, Pober JS. 2004. Cellular and Molecular Immunology. 4th ed.
Pennysylvania: WB Saunders Co. Pp 1636-1642.
Note.
Student Project (SP) Emergency Medicine
September-October 2016
Berikut dibawah ini adalah judul SP yang sudah dibagi pergrup SGD. Masing-masing Grup SGD mendapat satu judul dan Nama Penguji Sudah tercantum. Pembimbing SP sudah disepakati adalah masing-masing fasilitator tiap Group
SGD yang bersangkutan.
Pada akhir SP sudah dijadwalkan Ujian-Presentasi SP sesuai Jadwal yang sudah dibuat di Time Table.
No Student Project Group Penguji (2Venuend floor)
1
Perdarahan Pervaginam Kasus Ginekologi Keganasan
A1
Dr.dr Wayan Megadhana, SpOG(K)
2nd floor: R.2.09
2 Toxic Metabolic Coma A2 dr. Ida Ayu Sriwijayanti,
MBioMed, SpS
2nd floor: R.2.10 3 Kehamilan Dengan Hipertensi Kronis A3 dr. I Gede Mega Putra,SpOG(K) 2nd floor:R.2.11 4 Trauma Abdomen A4 Dr.dr. Ketut Suyasa, SpB SpOT(K) Spine 2nd floor:R.2.12
5 Skizofrenia Hebefrenik A5 Dr. dr. Cokorda Bagus
Jayalesmana, SpKJ
2nd floor: R.2.13 6 Septic Shock Pada Pediatrik A6 dr.Nyoman Budihartawan,MSc, SpA 2nd floor:R.2.14
7
Dengue Shock Syndrome
Pada Pediatik A7 Dr. dr Dyah Kanya Wati,SpA
(K),
2nd floor: R.2.15
8
Urogenital Trauma Pada
Anak-anak A8
dr. Gede Wirya Kusuma Duarsa, M.Kes, SpU(K)
2nd floor: R.2.16
9 Laringotrakeobronkitis A9 dr. Wayan Sucipta, SpTHT KL 2nd floor:R.2.20
10 Pneumonia A10 dr. Putu Andrika, SpPDKIC 2nd floor:
R.2.23 11 Perdarahan Pascaekstraksi
Gigi A11
drg. Putu Lestari Sudirman 3nd floor: R.3.20
12 Petit Mal Seizure A12 dr. IGN Budiarsa,SpS 3nd floor:R.3.23
English Class (Class B)
No Student Project Group Penguji Venue
(2nd floor)
1 Emergency Medicine Roles
in Natural Disaster B1
Dr.dr. Tjok Gde Agung Senapathi, Sp.AnKAR
2 Radiology Roles in ARDS B2 dr. Srie Laksminingsih, SpR 2nd floor: R.2.10
3 Angiofibroma B3 dr Sari Wulan, SpTHT- KL(K) 2nd floor:R.2.11
4 Shock In Adult B4 dr. IGAG. Utara Hartawan,
SpAn MARS
2nd floor: R.2.12
5
Sudden Cardiac Death
Rescue B5
dr. IGN. Mahaalit Aribawa, SpAn KAR
2nd floor: R.2.13
6 Alcohol Intoxication B6 dr. I Ketut Agus Somia, SpPDKPTI 2nd floor:R.2.14 7 Abdominal and Pelvic PainIn The Nonpregnant Female B7 dr. Endang Sriwidiyanti,SpOG 2nd floor:R.2.15
8 Toxic Shock Syndrome B8 dr. Nyoman Suryawati Sp.KK 2nd floor:
R.2.16
9 Acute Kidney Injury B9 dr. Kadek Budi Santosa, SpU 2nd floor:R.2.20
10 Thoraxic Trauma B10 dr. IGN Wien Aryana, SpOT 2nd floor:R.2.23
11 Acid Base Disorders B11 dr. I Made Agus Kresna
Sucandra, Sp.An
3nd floor: R.3.20
12 Fluid and Electolites B12 dr. I Wayan Aryabiantara,
Sp.An. KIC
LEARNING PROGRAMS
Abstracts of Lectures
Tjokorda Gde Agung Senapathi
Objective
To describe
1. Highlight Emergency Medicine
2. Basic principal of Emergency Medicine 3. Triad Emergency Medicine
4. Ethics in critical care
Physicians have been called on to provide emergency care for patients. However, in the house of medicine, the formal specialty of emergency medicine is still relatively young— measured in decades. Emergency medicine developed differently from perhaps many of the other more traditional medical and surgical specialties. In the case of emergency medicine, public demand more than scientifi c inquiry fueled the formation and growth of the specialty. In the 1950s and 1960s, with more physicians seeking specialty training, the number of general practitioners began to decline. At that time, hospitals were becoming more modernized and technologically advanced. Ultimately, these factors, along with the changing demographic and social conditions of the post–World War II era, led to an increased public reliance on hospital emergency departments for the provision of unanticipated medical care. Unfortunately, a uniform system for providing high-quality emergency care did not exist. At that time, junior medical and surgical house offi cers staffed many hospital emergency departments with little or no attending supervision. Most of these physicians did not have the necessary clinical skills to properly care for the increasing complexity of cases seeking medical attention. It was also becoming evident that the physician staffing patterns were inadequate to keep up with the ever increasing patient volume.
Basic principal and triad emergency medicine please read in the lecture power point. Medical ethics is the art of resolving conflicts that arise around treatment and treatment decisions. The conflict may involve the patient, family, caregivers, or society. An approach to these conflicts is as necessary as, say, an approach to hypotension or oliguria. Without an approach we would be ignoring the mechanism that led the conflict or problem in the first place. A little preparation will allow one to be more comfortable when confronting these situations, making responses more likely to be useful (and less likely to make things worse).
There are four basic principles or medical ethics that give us the tools to begin to resolve some of these conflicts : autonomy, beneficence, and justice. The weight we give each of these four different principles is often determined by our individual and societal morals.
Lecture 2
SEIZURE
STATUS EPILEPTICUS
IGN Budiarsa
Status epilepticus is defined as a condition in which epileptic activity persists for 30 minutes more.
The seizures can take the form of prolonged seizures or repetitive attacks without recovery in between. There are various types of status epilepticus and a classification :
(Table below)
Status epilepticus confined to early childhood 1. Neonatal status epilepticus
2. Status epilepticus in specific neonatal epilepsy syndrome 3. Infantil spasms
Status epilepticus confined to later childhood 1. Febrile status epilepticus
2. Status in childhood partial epilepsy syndrome 3. Status epilepticus in myoclonic – static epilepsy 4. Electrical status epilepticus during slow wave sleep 5. Landau – Kleffer syndrome
Status epilepticus occurring in childhood and adult life 1. Tonic – clonic status epilepticus
2. Absence status epilepticus 3. Epilepsia partialis continua 4. Status epilepticus in coma
5. Specific form of status epilepticus in mental retardation 6. Syndrome of myoclonic status epilepticus
7. Simple partial status epilepticus 8. Complex partial status epilepticus
In clinical practice status epilepticus classified : A. Convulsive status epilepticus
B. Non convulsive status epilepticus
Principle of management of status epilepticus 1. Lifesaving (ABC)
Lecture 3
COMA AND DECREASE OF CONCIOUSNESS
IA Sri Wijayanti
AIM:
Describe condition of coma and altered states of consciousness, know the current definition of coma and altered states of consciousness, etiology, mechanism based of altered states of consciousness, clinical presentation, diagnostic work-up including history, clinical examination and early management of altered states of consciousness.
LEARNING OUTCOMES:
1. Know current definition of coma and altered states of consciousness
2. Understand and be able explain etiology and mechanism based of coma and altered states of consciousness
3. Be able to explain a comprehensive history, clinical examination and assessment of comatose patients and altered states of consciousness.
4. Understand early management of altered states of consciousness
ABSTRACT
Impaired consciousness is among the most difficult and dramatic of clinical problems. The ancient Greeks knew that normal consciousness depends on an intact brain, and that impaired consciousness signifies brain failure. The brain tolerates only limited physical or metabolic injury, so that impaired consciousness is often a sign of impending irreparable damage to the brain.
Altered states of consciousness may have an organic or functional cause. This condition represents a spectrum of disease presentations from profoundly depressed arousal requiring emergent intubation to severe agitation and confusion requiring restraint and sedation. Initial stabilizing measures are often needed before complete history and physical examination can be performed (Lee, 2014).
All unconscious patients should have neurological examinations to help determine the site and nature of the lesion, to monitor progress, and to determine prognosis. Neurological examination is most useful in the well-oxygenated, normotensive, normoglycemic patient with no sedation, since hypoxia, hypotension, hypoglycemia and sedating drugs profoundly affect the signs elicited. Therefore, immediate therapeutic intervention is a must to correct aberrations of hypoxia, hypercarbia and hypoglycemia. Medications recently taken that cause unconsciousness or delirium must be identified quickly followed by rapid clinical assessment to detect the form of coma either with or without lateralizing signs, with or without signs of meningeal irritation, the pattern of breathing, the size and reactivity of pupils and ocular movements, the motor response, the airway clearance, the pattern of breathing and circulation integrity, etc.
Looking for the pathogenesis of coma, two important neurological components must function perfectly that maintain consciousness. The first is the gray matter covering the outer layer of the brain and the other is a structure located in the brainstem called the reticular activating system (RAS or ARAS), a more primitive structure that is in close connection with the reticular formation (RF), a critical anatomical structure needed for maintenance of arousal. It is necessary to investigate the integrity of the bilateral cerebral cortices and the reticular activating system (RAS), as a rule. Unilateral hemispheric lesions do not produce stupor and coma unless they are of a mass sufficient to compress either the contralateral hemisphere or the brain stem (Bateman 2001). Metabolic disorders impair consciousness by diffuse effects on both the reticular formation and the cerebral cortex. Coma is rarely a permanent state although less than 10% of patients survive coma without significant disability (Bateman 2001); for ICU patients with persistent coma, the outcome is grim. Maneuvers to be established with an unconscious patient include cardiopulmonary resuscitation, laboratory investigations, a radiological examination to recognize brain edema, as well as any skull, cervical, spinal, chest, and multiple traumas. Intracranial pressure and neurophysiological monitoring are important new areas for investigation in the unconscious patient.
Learning resources
Kitchener, Hashem, Wahba, Khalaf, Shafir, Mansoor. How to Approach Unconsciousness Patients. In Critical Care in Neurology. Flying Publisher and Kamp; 2012:Chapter 2.
Posner, Saper, Schiff, Plum. Diagnosis of Stupor and Coma. 4th ed. Oxford University Press;
Lecture 4
ACUTE PSYCHIATRIC EPISODE
Cokorda Bagus Jayalesmana
Objective:1. To describe etio-pathogenesis and pathophysiology of acute psychiatric episodes 2. To implement a general strategy in the approach to patients with acute psychiatric
episodes through history and special technique investigations
3. To manage by assessing, provide initial management and refer patient with acute psychiatric episodes
4. To describe prognosis patient with acute psychiatric episodes
Emergency occur in psychiatric just as we do in every field of medicine. However, psychiatric emergencies are often particularly disturbing because we do not just involve the body’s reactions to an acute disease state, as must as actions directed against the self or others. These emergencies, such as suicidal acts, homicidal delusions, or a serve in ability to care for oneself, are more likely than medical ones to be sensationalized when they are particularly dramatic or bizarre. Frequently identified medical causes of abnormal behavior include hypoglycemia, hypoxia, seizures, head trauma, and thyroid abnormalities. Patients should also be assessed for the presence of delirium or dementia, as both have potentially treatable causes.
Psychosis is difficult term to define and is frequently misused, not only in the newspaper, movies, and on television, but unfortunately among mental health professionals as well. Stigma and fear surround the concept of psychosis and the average citizens’ worries about long-standing myths of mental illness, including psychotic killers, psychotic rage, and equivalence of psychotic with the pejorative term crazy. Aggressive and hostile symptoms can overlap with positive symptoms but specifically emphasize problems in impulse control
History and physical examination, including a neurologic and mental status examination, may be sufficient to determine whether the patient has an acute psychiatric illness. However, any abnormality noted from the history and physical exam warrants further evaluation and treatment looking for a medical etiology. Once medical issues have been addressed, patients with presentation of psychosis, depression, anxiety, suicidal, or homicidal ideation need an appropriate psychiatric evaluation and disposition. Clinical judgment is often necessary to determine the need for admission in patients with chronic suicidal or homicidal ideation, and patients with other psychiatric illnesses and the potential inability to care for oneself.
LEARNING RESOURCES
1. Kaplan & Saddock’s Synopsis of Psychiatry, 10th ed
Lecture 5
ACUTE RESPIRATORY DISTRESS SYNDROME AND FAILURE
Putu Andrika
Respiratory distress is a term combining the patient’s subjective sensation of dyspnea with signs indicating difficulty breathing. The acute respiratory distress syndrome (ARDS) is a form of hypoxemic respiratory failure that is characterized by severe impairment of gas exchange and lung mechanics, with a high case fatality rate. In the USA, 150.000 cases were found per year and 50% of them died due to respiratory failure.
ARDS can be triggered by a number of different pulmonary and extrapulmonary insults. The characteristic pathological changes of ARDS include an exudative phase, with the accumulation of fluid within the lung, the release of proinflammatory cytokines and infiltration of inflammatory cells, especially neutrophils, into the lung parenchyma. Damage to the alveolar epithelium and pulmonary capillary endothelium occur and patients develop the characteristic histological appearance of diffuse alveolar damage. This manifests clinically as non-cardiogenic pulmonary edema, which reduces lung compliance and impairs gas exchange.
Diagnosed based on : complaint, sudden breathing difficulties, coughing, tiredness and decrease in consciousness and usually preceded by basic illness and triggering factors. On the thorax photo it was found infiltrate diffuse in the two lungs region, while in ARF depend on basic illness. The important thing is examination of blood gas analyses where there is a decrease on PaO2 until below 50 and PaO2 above 50 or refer to as rule of fifty.
Principle of procedure is to give the Oxygen, CO2 removal either with or without ventilator, liquid restriction, clearing of breathing pathway, overcoming obstruction using bronchodilator, etc.
Learning Objective
ACUTE UPPER AIRWAY OBSTRUCTION
Wayan Sucipta
Abstract
Acute upper airway obstruction is a life-threatening emergency that requires immediate intervention. Airway obstruction can be the result of a variety of disorders, including trauma, neoplasm, infection, inflammatory process, neurologic dysfunction, presence of a foreign body, hemorrhage, and anatomic condition. Affected sites can include the oral cavity, oropharynx, hypopharynx, larynx, and trachea. Presentation of the symptom: dyspnea, stridor, chest retractions, tachypnea and tachycardia, hoarseness. Physical examination: mirror or fiberoptic laryngoscopy should be performed. The chest should be examined visually and by auscultation. Vital sign should be determined. Pulse oximetry is also useful for measures arterial oxygen saturation. Laboratory: Arterial blood gases should be obtained. Imaging studies: chest or soft tissue neck radiographs, sometime need CT Scan.
Management: Acute upper airway obstruction can cause respiratory distress. The dicision to use a particular approach depends upon numerous factors, including the degree, cause, location, and evolution of the obstruction. See the figure:
Fever?
Susp foreign body? Status asthmaticus?
Trauma & unilateral absent breath sounds
Complit obstruction: Back or chest or abdominal blows, laryngoscopy & removal, needle cricothyrotomy
Avoid IV & other potentially agitating or painfull intervention. Evaluate for definitive airway byphysician most skilled in difficull airway
Epinephrine IM, Nebulized albuterol, steroids IV, Terbutaline Prepare for assisted ventilation
Needle thoracotomy followed by tube thoracotomy
Partial obstruction?
NO Allow patient to assume position of comfort. Obtain brief history and begin treatment based on suspected disease process. Order labs and imaging as indicated. Continue to reassess patient and obtain additional history Respiratory distress Respiratory arrest Yes Yes Assess ABC s, ˈ
Place IV, give IVfluid bolus, give oxygen, place on monitor
Immediate resuscitation, Clear airway, Assist ventilations, chest compression, IV,O2, IVF No
Sign of impending respiratory failure?
Airway: Stridor at rest, irregular respirations, apnea.
Breathing: severe retraction, grunting, nasal flaring, poor aeration, progressive fatigue. Circulation: poor color (cyanotic, ashen, Mottled), sluggish capiary refi
Mental status: Decreased level of consciousness, agitation, decreased response to pain
ACUTE RESPIRATORY DISTRESS SYNDROME in Pediatric
Diah Kanyawati
Abstract
ARDS is Acute catastrophic event, develops following either “direct” or “indirect” lung injury. Pneumonia and pulmonary aspiration are among the most common conditions with the potential to inflict direct lung injury and ARDS, but traumatic pulmonary contusion, fat embolism, submersion injury, and inhalational injury are relatively common causes as well. The most common forms of indirect lung injury include systemic conditions, such as sepsis, shock, exposure to cardipulmonary bypass, and transfussion-related lung injury.
Diffuse alveolar disease that meets criteria for ARDS prodeces a predictable sequence of clinical changes. When fluid accumulation in the interstitial space exceeds the absorptive capacity of the pulmonary lymphatics, lung compliance decline and tachypnea ensues as the patient attempts to generate adequate minute ventilation in the face of lower tidal volumes. The eventual leakage of proteinaceous fluid into the alveoral spaces interferes with native surfactant function, creating conditions that favor regional atelectasis and small-airways closure, as well as a decrease in EELV to a point near or bellow closing capacity, as specially in small infants and those with highly compliant chest walls (e.g., patients with neuromuschular dissease). At this point, hypoxia rapidly worsens, and breathing becomes more labored in an effort to generate transpulmonary pressures sufficient first manifests tachypnea. However, as the work of breathing escalates, the PaCO2 will further rise as
respiratory muscle fatigue ensues. At this stage, positive-pressure ventilation is required to open sufficient number of atlectatic lung units for adequate gas exchange. On auscutation, the patient will typically demonstrate rales over areas of atelectasis or aveolar congestion and dicreased air entry over areas that are largely consolidated. Occasionally, it is possible to appreciate wheezes over areas in which intermittent small-airways closure is occurring.
RADIOLOGY
Srie Laksminingsih
Learning ObjectiveAt the end of meeting, the student will be able to :
1. Describe the radiology imaging of thorax photo for IRDS (Idiopathic Respiratory Distress Syndrome) case, Bronchopneumonia, CHD, Pericardial Effusion, Lung Edema, Pneumothorax, Pleural Effusion, Vena Cava Superior Syndrome.
Lecture 6
BLEEDING DISORDER
Vaginal Bleeding
Wayan Megadhana
OBJECTIVES
1. To recognize life-threatening cause of vaginal bleeding. 2. To develop an approach to the causes of vaginal bleeding.
3. To diagnose and manage vaginal bleeding in pregnant patients (Ectopic pregnancy, Ante partum hemorrhage and Post partum hemorrhage).
Ectopic Pregnancy
Approximately 1% of diagnosed pregnancies are ectopic. Risks factors include PID, IUD, infertility treatment, pelvic surgeries, tubal ligations and endometritis. Mortality is 1 in 850 women if treated, but nearly 100% if untreated. Median time for rupture of a tubal pregnancy is 8 weeks; however interstitial (cornual) ectopic pregnancies can rupture later in pregnancy 12-16 weeks with catastrophic result. The diagnose of ectopic pregnancy is vaginal bleeding, acute abdominal pain. Many of the bleeding ectopic pregnancies are treated surgically and medicamentosa with MTX (Methotrexate).
Ante partum hemorrhage
Diagnostic possibilities for vaginal bleeding in late pregnancy range from trivial to life threatening and include placenta previa, abruption placentae and uterine rupture.
Abruptio placenta is a premature separation of the normally implanted placenta from the uterus. It is associated with various hypertensive, cardiovascular and connective tissue autoimmune disorders. Often, it is associated with various degree of trauma. Abruptio placentae classically presents with a tender contracted uterus, signs of hemorrhage (concealed abruption, there may not be any external bleeding) and fetal distress. Abruptio placentae is often misdiagnosed as preterm labor. Abruptio placentae management based on degree of abruption and labor phase, so it can be expectant vaginal delivery or abdominal delivery.
Placenta previa is the result of implantation and placenta development over the internal cervical os. Risks include multiparity, abnormal uterus, fibroids and prior surgeries. Classically, placenta previa presents with painless bleeding, often preceded by trauma or intercourse. Do not attempt a pelvic examination because it may worsen the hemorrhage in placenta previa. Any patient presenting with vaginal bleeding after the first trimester should have an ultrasound prior to any pelvic exam. Management of placenta previa based on gestational age and it can be conservative management or by surgery.
Uterine rupture occurs in 0.05% of pregnancies. Maternal mortality is 8% while fetal mortality is 50%. It usually seen during labor, so may encounter it in the emergency department when a patient presents following an attempted home delivery. Management of uterine rupture can be conservative management by conservative surgery or by hysterectomy.
Non life threatening causes of third trimester bleeding include: bloody show, cervical traumatic bleeding and marginal sinus rupture.
Postpartum Hemorrhage
passage is necessary. If atony is present, Oxytocin 30 units in 1 litre of normal saline at 200 cc/hr can be helpful. Ultrasound will assist in ruling out retained products. Make sure that patient is afebrile. Postpartum endometritis may either complicate bleeding or in fact be the contributing factor.
Epistaxis
SARI WULAN
ENT TEAM
ObjectiveAble to
1. Identify the pathophisiology of the epistaxis, 2. Do proper treatment to protect complication
3. Do ongoing care of epistaxis in order to prevent rebleeding
Preface
Epistaxis is acute bleeding from the nose or nasopharyng. It is not a diseases but the sign of other diseases which is 90% can be stopped spontaneously. Principle of managements are stop bleeding, prevent complication and rebleeding.
Patophisiology
There is a thin and weak area within the bleeding spot area in the younger age that probably caused by mild trauma and ischemia. In the middle age and older can be found changing and thikening of tunica media from capillary endotel that caused the blood vessel loosing their elasticity, so the bleeding usually profuse.
Classification
1. Anterior Epistaxis, usually from pleksus kiesselbach (little’s area) there is anastomosis of capilary in the anterosuperior nasal septum and also from anteroinferior of inferior turbinate
2. Posterior Epistaxis, from a. sfenopalatina and a. posterior ethmoidalis.
Diagnosis
Good and complete question should be done as soon as possible about habits and the past history of the systemic diseases if any to recover the caused of the bleeding and also to prevent from rebleeding. Identify the bleeding spot is require in order to give optimal treatment to protect complication.
Anterior epistaxis is usually caused by mild trauma, such as scratching the nose, infection (rhinitis), climate changing. Posterior epistaxis is usually caused by systemic diseases such as hypertension, cardiovascular diseases, fraktur and tumor.
Treatment
Anterior Epistaxis
1. Cauterisation by AgNO3 20-30% or trichloroasetic acid 10% 2. Anterior packing with vaseline
Posterior Epistaxis
1. Posterior packing with vaseline 2. Balloon packing
Re ferrence
1. Watkinson JC. Epistaxis. Dalam: Mackay IS, Bull TR. Scott – Brown’s Otolaryngology. Volume 4 (Rhinonology). Ed. 6 th. Oxford: Butterwort - Heinemann, 1997: 1–19. 2. Thornton MA, Mahest BN, Lang J. Posterior epistaxix: Identification of common
bleeding sites. Laryngodcope, 2005. Vol. 115 (4): 588 – 90.
Lecture 7
SHOCK
IGAG Utara Hartawan
Objective
1. To describe the term, etio-pathogenesis and pathophysiology of shock
2. To implement a general strategy in the approach to patients with shock through history, physical examination and special tehnique investigations.
3. To manage by assesing, differential diagnosis, provide initial management and refer patient with shock
4. To describe prognosis patient with shock
Shock is a state in which the oxygen (O2) and metabolic demands of the body are not met by the cardiac output. When this process occurs in a single organ, rather than throughout the body, organ ischemia and infarction ensue. When shock occurs on a more global level, multiorgan dysfunction and failure are the consequence, ultimately leading to death if not corrected. Shock is most often accompanied by hypotension, termed decompensated shock. However, shock may also occur with normal or elevated blood pressure. Examples include hypertensive emergency with compromised cardiac output, or carbon monoxide intoxication with the inability to deliver O2 despite normal hemodynamics. The approach to the patient in shock must proceed with the same urgency as the patient suffering from an acute myocardial infarction or cerebral vascular accident.
Shock states are classified according to the underlying physiologic derangement. Hypovolemic shock is defined by decreased circulating blood volume, either due to blood or fluid loss, such that cardiac output is compromised. Impaired cardiac performance characterizes cardiogenic shock. Loss of vasomotor tone with hypotension is the hallmark of distributive shock, as in sepsis, anaphylaxis, or certain intoxications. Anatomic interruption of sympathetic output, usually secondary to spinal cord injury with disruption of the cervical sympathetic chain, leads to bradycardia and hypotension in neurogenic shock. Obstruction of blood flow through the cardiopulmonary circuit is the etiology of obstructive shock, as in tension pneumothorax, cardiac tamponade, or massive pulmonary embolus. Finally, a few patients present with a mixed syndrome, such as a patient with sepsis who develops gastrointestinal (GI) hemorrhage, or who suffers a concomitant myocardial infarction.
If shock is defined by impaired global organ perfusion, then it follows that signs of shock are derived from impaired organ function. Hypotension is an obvious sign of decompensated hemodynamics associated with shock. Alteration in mental status, chest pain, signs of cardiac failure, difficulty breathing, abdominal pain from intestinal ischemia, low urinary output, and mottled skin all suggest shock.
In a proportion of patients, the etiology of the shock state remains in question after initial evaluation. Often, therapeutic intervention must be initiated without a firm diagnosis. The core principle in treatment of such patients is that O2 delivery to the vital organs must be optimized.
General treatment principles are : oxygenation, cardiac intervention, blood product transfusion, volume intervention, and vasoactive agents intervention.
Goal treatments are :
CVP 8-12 mmHg
PAOP 8–12 cmH2O
CO 3.8–7.5 L /min (approximate for normal size adult)
CI 2.4–4.0 L /min/m2
SVR 800–1400 dyne/s/cm5 (approximate for normal size adult)
SVRI 1600–2400 dyne/s/m2/cm5
CVP: central venous pressurePAOP: pulmonary artery occlusion pressure CO: cardiac outputCI: cardiac indexSVR: systemic vascular resistanceSVRI: systemic vascular resistance index
Prognosis depends on early recognition, intervention, source control, and smooth transitions of care help, ensure the most ideal outcomes. Some clinical variables are associated with poor outcome, such as severity of shock, temporal duration, underlying cause, preexisting vital organ dysfunction and reversibility. While associated morbidity and mortality remain high for patients with shock, integration of protocol-based care pathways, with ongoing refinement in response to new information, may lead to continued reductions over time.
Copied from : Sigillito RJ and DeBlieux PMC. Shock. In An Introduction Clinical Emergency Medicine Guide for Practioner in the Emergency Department. Cambridge University Press. 2005. p.85-92
References :
1. Butterworth, J.F., 2013. Fluid Management & Blood Component Therapy. In Morgan & Mikail’s Clinical Anesthesiology. New York: Mc Graw Hill Education, pp. 1161–1181. 2. Nicks, B.A., 2016. Aprroach to Shock. In J. E. Tintinalli, ed. Tintinalli’s Emergency
Medicine. New York: Mc Graw Hill Education, pp. 63–69.
3. Smith, L.M., 2014. Shock. In S. C. ; Joseph M. W. Sherman, ed. Clinical Emergency Medicine. New York: Lange, Mc Graw Hill Education, pp. 42–45.
SHOCK IN PEDIATRIC
I Nyoman Budihartawan
Abstracts
Lecture 8
CARDIAC ARREST AND CARDIOPULMONAR RESCUSTATION
IGN Mahaalit Aribawa
Objective :
1. To describe etio-pathogenesis and pathophysiology of cardiac arrest 2. To know how to identify patients with cardiorespiratory arrest
3. To understand the chain of survival
4. To Understand the principles of treating cardiac arrest incorporate basic life support and advance life support
5. To describe the need for continued resuscitation after return of spontaneous circulation (ROSC )
6. To describe the role of the resuscitation team
Abstract
Cardiac arrest is the cessation of clinically detectable cardiac output. It is unpredictable and rarely occurs with doctors in attendance, can occur anywhere, anytime and to anybody. Cardiac arrest can be because of a disease or due to drowning, poisoning and others that are capable of causing respiratory and cardiac arrest.
The initial rhythm found may be ventricular fibrillation ( VF ), ventricular tachycardia ( VT ), asystole, and pulseless electrical activity ( PEA ). Bystanders need to commence cardiopulmonary resuscitation ( CPR ) immediately if the victim is to survive.
Permanent brain damage can occur if blood circulation has stopped for more than a few minutes (now it has been agreed more than 4-6 minutes) or after a trauma with severe hypoxia or loss of lots of blood which are not corrected. If resuscitation / CPR is given immediately and correctly brain death can be avoided and the patient recovers completely.
Resuscitation can be done anywhere, anytime, with or without equipment by trained whether public or health personnel. CPR (cardiopulmonary resuscitation) is an effort of medical emergency to cure respiratory function and circulation which has failed drastically on a patient that has the chances of living. CPR incorporates basic life support ( BLS ), that is, making use of basic equipment or without equipment and advanced life support (ALS), that is, using advanced equipment including drugs, defibrillators and advanced airway management.
Lecture 9
EMERGENCY TOXICOLOGY AND POISONING
I Ketut Agus Somia
BASIC MANAGEMENT OF INTOXICATION
OBJECTIVE: Intoxication or poisoning should be think in patient suddenly onset of disease, with previously healthy condition, and difficult to explain or unclear of the causes. It is complex situation included possibility crime and law, even that the emergency and life threatening. To Underetand of Toxic syndrome is once of method for identification of the toxicant, by specific odor, colour of urine, heart rate, pulse rate, reapiratory rate, body Qransaction and consiousness. Laboratory test is important for to known serum level of the agent,and target organ effect. Osmolar gap and ion gap is also important in toxicology Qransact to support the diagnosis. The time of the first contact with tocicant is very I for determine of prognosis and treatment. The antidote is Qransact therapy for management of patient intoxication, but not always available and should be used carefully because can induced intoxication. The basic treatment of emergency cases is base on ability to control of airways, breathing and circulation( or ABC Qransacti). The specific presedure in intoxication cases beside ABC also DE (Decontamination and Elemination). The heathcare of patient intoxication should be comprehendsive by Team care depend on targen organ damage.
ORGANOPHOSPHAT INTOXICATION
CAUSTIC INTOXICATION
Lecture 10
HYPERTENSION IN PREGNANCY
I Gede Mega Putra
OBGYN Team
Objective :
1. Define hypertension in pregnancy
2. Review appropriate fetal/maternal assessment
3. Discuss appropriate management of hypertension in pregnancy
4. Recognize when and how to transport patient with hypertension in pregnancy
Hypertension in pregnancy occurs in approximately 10% of pregnancies and can be associated with significant maternal and fetal morbidity and mortality. The spectrum of disease is divided into 3 main categories: gestational hypertension, preeclampsia, and eclampsia. Preeclampsia affects 2-6% of pregnancies in the United States, with a higher incidence globally. Eclampsia occurs in < 1 % of patients with preeclampsia.
Gestational hypertension is defined as a blood pressure >140/90 mmHg in a pregnant patient without preexisting hypertension. The hypertension will resolve within12 weeks postpartum. When proteinuria is also present, it is defined as preeclampsia. Preeclampsia typically occurs after 20 weeks' gestation. A subset of patients will develop severe preeclampsia, which is associated with one of more of the following: severe hypertension (>160/110 mmHg on 2 separate occasions >6 hours apart), large proteinuria, neurologic symptoms, epigastric/right upper quadrant (RUQ) pain, pulmonary edema, or thrombocytopenia. Eclampsia is preeclampsia with seizures. HELLP syndrome affects some patients with preeclampsia and eclampsia and is associated with hemolysis, elevated liver enzymes, and low platelets.
Although the exact etiology of preeclampsia is unknown, there are several factors that are thought to contribute.These include maternal immunologic intolerance, abnormal placental implantation, endothelial dysfunction, and genetic factors.
Hypertensive disorders in pregnancies are the leading causes of maternal death in emerging countries. All caregivers must be able to promptly recognized the signs, symptoms and laboratory findings of gestational hypertension with or without proteinuria and with other adverse manifestation. Caregivers must appreciate fully the seriousness of gestational hypertension, its potential for multi – organ involment and the risk for perinatal and maternal morbidity and mortality. The appropriate management of gestational hypertension may vary based on the availability of resources. In this lecture student will discuss such as : the classification and definition of hypertensive disorders in pregnancy; management and treatment of gestational hypertension.
Lecture 11
SHOULDER DYSTOCIA
Endang Sriwidiyanti
OBGYN Team
Objective
1. Define shoulder dystocia
2. Review appropriate fetal/maternal assessment 3. Discuss the risk factors of shoulder dystocia 4. Discuss the complications of shoulder dystocia
5. Discuss appropriate management of shoulder dystocia
Shoulder dystocia is one of emergency problems during delivery. Following the delivery of the head, there is impaction of the anterior shoulder on the symphysis pubis in the AP diameter, in such a way that the remainder of the body cannot be delivered in the usual manner. More than 50% of cases shoulder dystocia occur in the absence of any identified risk factor. The student will discuss the assessment of shoulder dystocia, the complication for fetus and mother, identification of risk factor, diagnosis and management
Definition
After the birth of the head, external rotation will take place which causes axis of the head to be on the normal axis to the spine. Generally shoulder will be on the oblique axis under the pubic ramus. Pushing of the mother will cause the anterior shoulder become under the pubis. If the shoulder fails to hold a rotation of adjusting to the axis of tilted pelvis and remain in the anteroposterior position, the baby will most collision front shoulder to the symphysis.
Shoulder dystocia is mainly caused by deformities of the pelvis, the failure of the shoulder to "folded" into the pelvis (eg on macrosomia) caused by active phase and short second stage of labor in multiparas so the descence of the head is too quickly, causing the shoulder does not fold through the birth canal or head has through the middle pelvis after a prolong of the second stage of labor before the shoulder successfully folded into the pelvis.
Incidence
• 1 - 2 in 1000 Birth
• 16 in 1000 baby weight > 4000 g
Complication : • Baby
- Death
- Asphysxia and its complications - Fracture of Clavicula, humerus - Brachial Plexus Injury
- Postpartum haemorrhage - Uterine Rupture
Risk Factors :
• Post date pregnancy • Maternal Obesity • Macrosomia baby
• History of prior shoulder dystocia • Operative vaginal delivery
• Prolong second stage of labour • Uncontrolled Maternal Diabetes
Diagnosis
• Turtle’ sign
• Prolonged second stage of labour
• Fail to deliver the baby with maximal effort and proper management
Management
Requirement :
Maternal vital condition is sufficient to work together to completing deliveries
The mother has the ability to pushing
The passage and the pelvic outlet are adequate for the baby's body accommodation
The baby is still alive or are expected to survive
Not monstrum or congenital abnormality that prevents the delivery of baby
The management : "ALARMER"
1. Principles : Do not 4 “P” :
Panic
Pulling (the head of the baby)
Pushing (the fundal of uterine)
Pivoting (the head of the baby with coccygeus as fulcrums
2. Ask For Help :
The mother of patient
Husband
Midwife
Physician in charge or other paramedic
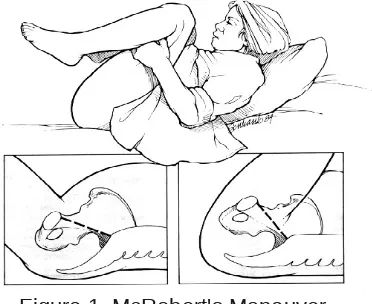
[image:37.595.238.424.597.749.2]3. Lift the buttock- McRobert’s Maneuver
4. Anterior Disimpaction -
4.1. Suprapubic Pressure (Manuver Massanti )
[image:38.595.244.400.140.285.2]• Suprapubic pressure on the baby's anterior shoulder toward the chest of the baby.
Figure 2. Suprapubic Pressure
4.2. Rubin Manouver
• vaginal approach
• adduction anterior shoulder by pressing the posterior shoulder towards the chest
• Consider episiotomy
Figure 3. Rubin Manouver
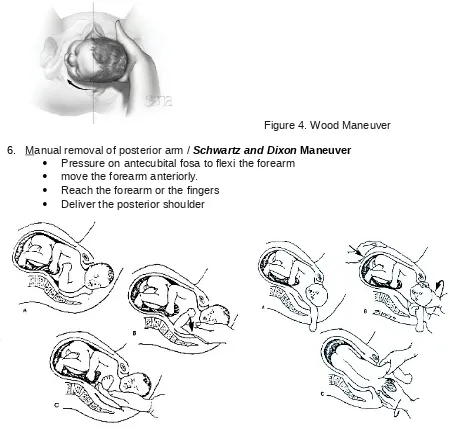
[image:38.595.142.513.398.563.2]Figure 4. Wood Maneuver
6. Manual removal of posterior arm / Schwartz and Dixon Maneuver
Pressure on antecubital fosa to flexi the forearm
move the forearm anteriorly.
Reach the forearm or the fingers
Deliver the posterior shoulder
Figure 5. Schwart and Dixon Maneuver
7. Episiotomy-consider
Help Wood Manouver or giving more space to deliver the posterior arm, rotate the chest and ease reaching the posterior shoulder
8. Roll over
9. Last Efforts :
Break the clavicle
Cephalic replacement (Zavenelli Manouver)
Symphisiotomy
10. After procedure :
• Post partum haemorrhage anticipation • Exploration of lasceration and tear • Examination of the baby
• Record the procedure
Reference
1. Cunningham FG, Leveno KJ, Bloom SL, Spong, CY, Dashe JS, Hoffman BL, Casey BM, Sheffield JS. 2014. William Obstetrics, 24 edition. Mc Graw Hill.
2. Buku Acuan Modul PONEK. 2008. JNPK-KR. 3. ALARM International Course
Lecture 12
DERMATO - EMERGEMENCIES
ACUTE BLISTERING AND EXFOLIATIVE SKIN
Nyoman Suryawati
Objective
To understand the basic principle of acute blistering and exfoliative skin Able to identify a case with acute blistering and exfoliative skin
Able to manage and referral a case with acute and exfoliative skin
Abstract
Steven