Vitamin D deficiency occur in healthy tropical country women,
not depending on adipocyte status
Dina Keumala Sari1, Harun Al Ra syid2, Nur Indrawaty Lipoeto3, and Zulkifli Lubis4
Author’s affiliation and corresponding information: 1
Dina KS, Department of Nutrition, Medical Faculty of Sumatera Utara, Indonesia, email address: [email protected], postal address: Medical Facultly of Sumatera Utara, Indonesia. Jl. Dr. Mansur, No. 5, Kampus USU , Padang Bulan, Medan. Phone number: +62
61 8212296, cell phone: +62 8174894768 2
Harun AR, Department of Nutrition, Medical Faculty of Sumatera Utara, Indonesia 3
Nur Indrawaty L, Department of Nutrition, Public Health Faculty of Sumatera Barat, Indonesia
4
Zulkifli L, Department of Food Science and Technology, Agriculture Faculty of Sumatera Utara, Indonesia
ABSTRACT
Background: Low circulating of 25-hydroxyvitamin D [25(OH)D] serum may increase risk
of morbidity and mortality, especially in obese women and vitamin D deficiency are considered to be new markers for obesity and diabetes mellitus.
Objective: We investigated whether vitamin D deficiency occur in normoweight and
overweight-obese women who lived in abundant sunlight exposures area such as Indonesia.
Design: This was a cross-sectional study, including healthy normoweight women
(NG/normoweight group, n=41) and overweight-obese women with no other disease subjects (OG/overweight-obese group, n=41), parameters observed were ethnicity, age, sunlight exposure, way of dressed, sunscreen application, whitening application, and nutrient intake. Other parameters such systolic and diastolic pressure, Body Mass Index (BMI), waist circumference, fat distribution, 25-hydroxyvitamin D, and calcium serum were also included.
Results: There were no significant different between the two groups in ethnicity, sunlight
different in systolic (p= 0.001) and diastolic pressure (p=0.019), BMI (p=0.001), waist circumference (p= 0.001), and fat distribution (p= 0.001) between two group. Interestingly, there was found lower 25-hydroxyvitamin D concentration, indicated that vitamin D deficiency happened in healthy tropical country women, but there was no significant different in 25-hydroxyvitamin D (p= 0.140) and calcium serum (p= 0.464) between the two groups.
Conclusions: The results indicated that vitamin D deficiency can be found in tropical country
and there was no significant different between normoweight and overweight-obese healthy women. This study reported that normoweight and overweight-obese healthy women have hypovitaminosis with different possibility caused, in normoweight probably because of lack of vitamin D intake and less UV B exposure, but in overweight-obese probably because of the trap of vitamin D in adipocyte and less UV B exposure.
KEYWORDS: vitamin D, women, tropical country, adipocyte status
INTRODUCTIONS
Overweight and obesity are serious and growing health problems, and could influence human health. Knowadays, the World Health Organization (WHO) estimated 1.1 billion adult people in the world have a problem in overweight and about 312 million people having problem in obesity(1-3). In the United States (US), 2 in 3 adults have a BMI of ≥ 25 (4), but in developing country such as Indonesia, its increasing every year. Women obese found higher prevalence than man (23,8% vs 13,9%), urban found higher prevalence than rural (12,4% vs 10,3%), and the highest found in working women as an employee than other job (13,5% vs 11,7) (5).
studies found that vitamin D deficiency may contribute to an increased cardiovascular disease risk in obese subjects (8,9). Not many tropical countries have reported about this deficiency; studies in Saudi Arabia and Malaysia reported vitamin D deficiency in diabetic subjects, women, and children (10-12), but in Indonesia report elderly could suffer in vitamin D deficiency (13). Nutrient intake in developing countries could influenced the obesity, but the most important is the lifestyle in avoiding sunshine, this could influence the probability to have diabetes mellitus risk higher than other factors.
Obese subjects have a low vitamin D serum, in country which have abundant sunlight exposures, normal 25-hydroxyvitamin D serum should in a range 32-100 ng/mL or 54-90 nmol/L (14). Vitamin D which trapped in adipocyte could not be metabolized effectively in the circulation, resulting in low concentration of 25-hydroxyvitamin D. Hypovitaminosis D have positive correlation with insulin sensitivity and have a negative effect on β cell function
(8).
However, calcium role seem not influenced by vitamin D status even many intervention studies have investigated the effects of vitamin D in combination with calcium showed significant correlation (8). Lifestyle could influence the vitamin D status, women found to tend avoiding sunlight exposure probably due to afraid of being pigmented skin, indeed white skin always become a beautiful model in every advertising cosmetic products. Using sunscreen before going out, using whitening, white skin model, avoiding sunlight could be the reasons for less UV B radiation in tropical countries, so, this is greatest interest to find out whether vitamin D can occur in abundant sunlight exposure. Objective of this study was whether vitamin D deficiency occur in normoweight and overweight-obese women who lived in tropical country such as Indonesia.
MATERIAL AND METHODS Subjects
Study subjects included 82 healthy women (41 normoweight and 41 overweight-obese women), The criteria for eligibility were women with an age of 20-50 years and categorized in two group, normoweight (NG) and overweight-obese group (OG). Age with a mean (±SD) age of 30.85±7.71 y in NG and 35.61±7.67 y in OG. Criteria for normoweight is <22.9 kg/m2 and for overweight-obese is more than 23 kg/m2. We conducted the observational study between May to July 2012, in dry season (April to October is dry season). The location of recruitment was in Sumatera island (Sumatera Utara, Medan) with latitude: 3.57 N and longitude 98.65 E, average temperature: ±32oC (90oF) (20,21).
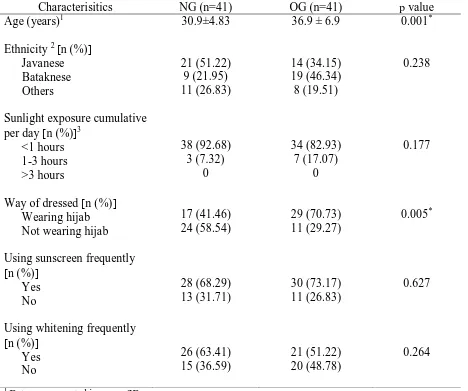
subjects answers the question about the timing they have been exposure by the sunlight all day long. Way of dressed included in examination because of the probability of smaller time directly exposure in women wearing hijab than those not wearing hijab. Wearing a hijab is a women who wearing cloth/dress covering the body except face and hand. Using sunscreen and whitening frequently was devided into two group, based on the answer of subjects which yes or no (Table 1).
All the subjects were measured at their work place with different occupation (teacher, bank employee, and nurse), most of them work indoors, with different ethnicity. The study subjects were recruited after a careful history, physical examination, and normal baseline investigations, which excluded subjects with history of diabetes mellitus, myocardial infarction, renal and liver disfunction. Moreover, subjects with pregnancy, lactation, drugs influenced lipid serum were exclusion criterias, but subjects with regularly with supplementation vitamin D included in this study but was count as vitamin D sources. All participants were given written informed consent to the study procedures, which approved by the Ethics Committee of Medical Faculty of Sumatera Utara University.
Nutrient intake, anthropometry status and body fat
Assessment of nutrient intake was based on food recall for two day (one day for week day and one day for week end), including energy, protein, fat, carbohydrate, calcium, phosphor, cholesterol, vitamin D, and percentage of fulfilment. Calculation using Nutrisurvey 2005, which included Indonesian foods.
BMI=weight (kg)/height (m)/height (m)
Body fat percentage refers to the amount of body fat mass in regards to the total body weight expressed as a percentage, based on Bioelectrical Impedance with simple formula
Body fat percentage (%)={body fat mass (kg)/body weight (kg)}x100
With the following classified: low (5-19.9%), normal (20.0-29.9%), high (30.00-34.9%), and very high (35.0-50.0%).
Waist circumference was measured with non-plastic tape: i.e. normal (<80 cm) and risk of metabolic (> 90 cm) for Asia (1). Height measured with staturemeter to calculate BMI. Systolic and diastolic pressure were measured with Automatic Blood Pressure Monitor-Omron.
Laboratory analysis
We measured 25(OH)D by chemiluminescent immunoassay (CLIA) technology (Diasorin, Stillwater, MN). Measures between 4.0 and 150 ng/mL. The lowest value is 4.0 ng/mL which is based on an inter-assay precision 3.90% CV. Reference range are <20 ng/mL categorized deficiency, 20-32 ng/mL (insufficiency), 32-100 ng/mL (sufficiency), 54-90 ng/mL (normal in sunny countries), >100 ng/mL (excess), >150 ng/mL (intoxication). To convert ng/mL to nmol/L is multiply with 2.496 (14).
Statistical analysis
Categorical variables were expressed as percentage proportions and using chi-square to expressed significancy difference between two groups, p= <0.05. Continuous variables were expressed as continuous variables as means±SDs. Because age and systolic pressure in NG and calcium serum in OG were nonnormally distributed, as tested by the Kolmogorov-Smirnov test, data were then normalized by logarithmic (Log10) transformation. If the data cannot be normalized, data ere we presented as median (minimum-maximum), such as nutrient intake data. The unpaired t test was used to compare continuous values of the study groups if the data normally distributed and Mann Whitney test was used for non-normally distributed data. The p values <0.05 were considered statistically significant. We used SPSS program (version 11.5; SPSS Inc, Chicago, IL) to perform the analysis.
RESULTS
Descriptive characteristic for 82 women is presented in Table 1, devided into two groups. A majority of women in NG were 30.9±4.83 years, significantly different with OG, which was significantly older than NG (36.9±6.9 y). Vitamin D deficiency occurred in normoweight and overweight-obese women who lived in abundant sunlight exposures area such Indonesia. Ethnicity were not differ between the two groups, the highest ethnic is Javanese (51.22%) found in NG, but in the OG Bataknese was the highest ethnic (46.34%). Bataknese consisted of three small groups i.e.: Bataknese, Mandailingnese, and Karonese. The other ethnics consisted of Acehnese, Minangkabau, Malay, Chinese, and Nias.
higher in the two group with no significantly difference, 73.13% in OG and 68.29% in NG. Whitening application was found no different between the two groups, most of the subject used whitening, in NG 63.41% using whitening vs 36.59% not using. In OG 51.22% using whitening vs 48.78 not using (Table 1).
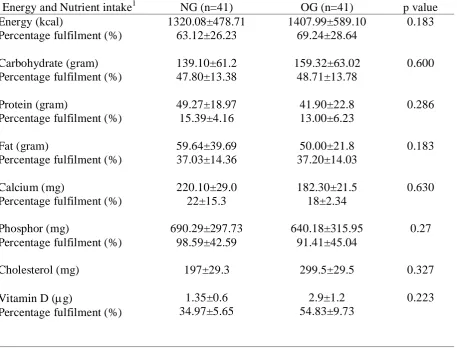
For nutrient intake, no energy intake different was found between the two groups (p=0.183), subjects in OG fulfill the energy for 69.24±28.64%. Carbohydrate, protein, fat, calcium, phosphor, vitamin D, and cholesterol seem less than the requirement, but not significanlty differ between the two groups. Carbohydrate requirement was 50-60%, but it was 47.80±13.38 in NG and 48.71±13.78 in OG, with p= 0.6. Protein was 15.39±4.16% in NG and 13±6% in OG, with p= 0.286. Fat intake gave 37.03±14.36% fulfillment in NG and 37.20±14.03% in OG, with p= 0.183. Calcium had a low intake instead of phosphor, and varied in NG. In NG reported for calcium intake 220.10±29.0 mg and 182.30±21.5 mg, but no significant differ between two groups. Phosphor intake was almost reach the requirement, in NG 98.59±42.59% and in OG 91.41±45.04, with p= 0.27. Data reported for cholesterol intake, 197±29.3 mg in NG and 299.5±29.5 mg in OG. Vitamin D intake showed no different between two groups, 1.35±0.6 g in NG and 2.9±1.2 in OG (Table 2).
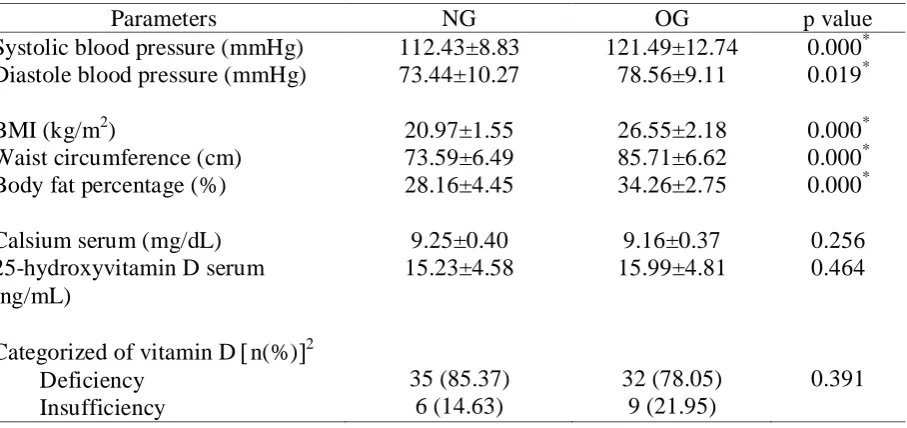
Subjects clinical characteristic subjects showed significant difference between the two groups (Table 3), mean systolic blood pressure in NG was 112.43±8.83 mmHg and in OG results gave twice rising than the NG (121.49±12.74 mmHg, p= 0.001). Diastolic pressure gave significant difference in both groups, 73.44±10.27 mmHG in NG and 78.56±9.11 mmHg in OG (p= 0.019).
73.59±6.49 cm in NG and 85.71±6.62 cm in OG (p= 0.001). Criteria for waist circumference in Asia, >80 cm have a metabolic risk, OG showed higher risk than NG. Fat distribution mean 28.16±4.45% in NG and 35.6±2.75% in OG (p= 0.001). Table 3 showed that was NG categorized normal in fat distribution but higher in OG.
Calcium and 25-hydroxyvitamin D serum did not significantly differed between the two groups. In NG, mean calcium serum was 9.25±0.40 mg/dL and in OG 9.16±0.37 mg/dL with p= 0.256. Mean calcium serum in NG was categorized normal in both groups. Both groups showed no significant different in 25-hydroxyvitamin D, 15.23±4.58 ng/mL in NG and 15.99±4.81 ng/mL in OG with p=0.464. Vitamin D deficiency was found 85.37% in NG and 78.05% in OG (Table 3).
DISCUSSION
The aim of this study was to investigate whether vitamin D deficiency occur in normoweight and overweight-obese women who lived in abundant sunlight (UV) exposures area such Indonesia. Many study found vitamin D deficiency only found in the country with four seasons, some of the study showed vitamin D deficiency was found in obese subject (11, 13, 22, 23). This study showed that even in abundant sunlight exposure such tropical country with two season (Indonesia), deficiency can be found in normoweight and overweight -obese subjects.
25-hydroxyvitamin D concentration are largely determined by vitamin D intake and UV exposure (22). Alvarez et al (9), reported that 25(OH)D may contribute to the ethnic difference, especially in African American which have lower insulin sensitivity than European Americans. This study with three different ethnic group (Javanese, Bataknese, and other ethnics) showed that no significant different among them, all subjects showed lowered concentration of 25(OH)D.
The lifestyle in avoiding sunlight, using sunscreen, and/or whitening probably become factors reducing 25(OH)D concentration in all subjects. Indonesia is a tropical country, with two season (dry and wet season), this study done in dry season so UV exposure was much more than other season. Wearing hijab does not influenced since they have a very little time to exposure by sunlight and shade can reduce UV radiation by 50% (25). Using sunscreen can reduce vitamin D3 synthesis, 92.5-99% (SPF 8 and 15, respectively) (15). This study showed that image to avoid sunlight exposure because of many reason, such as white skin more attractive than pigmented skin making subjects protect their skin from the sunlight through sunscreen and whitening. Skin pigment and aging process can reduce vitamin D3 synthesis by 99%.
place at lower latitude so it should be enough UV B radiation, but the results showed that lower vitamin D, so less 25(OH)D could be due to lifestyle.
Holick (28) estimated that exposure of the whole body in a bathing suit to 1 (individual) minimal erythemal dose (MED) is equivalent to ingesting 10,000 IU of vitamin D. Thus exposure of 6-10% of the bodysurface to 1 MED is equivalent to ingesting 600-1000 IU. The current recommended daily intake of vitamin D for children is 400 IU and for adults is 200 IU (1 IU=0.025g vitamin D), although recent research suggests that this should be increased to 600 IU (with some suggesting daily intake of up to 4000IU) in the absence of sunlight exposure. Based on these data, daily exposure of 6-10% of the body surface (one arm, one lower leg, or face and hands) to 1 MED should be sufficient to maintain vitamin D sufficiency (>50nmo/l). It should be noted however that recent research suggested that the lower level of vitamin D sufficiency should be raised to at least 80nmo/l=32.05ng/mL.
Nutrient energy showed there were no significant different between the two groups, NG or OG showed very less energy. Each group showed variation data that tend to less energy, carbohydrate, and protein. Daily requirement is 50-60% for carbohydrate, 12-15% for protein, and 20-25% for fat. Fat percentage fulfilment showed a higher rate. Calcium and phosphor intake showed no significant different between the two groups, but results of the study showed percentage of phosphor have higher rate than calcium intake. This study results showed that milk is less consumption by all subjects, it because of there is a thought that drinking milk could rising body weight. Even there is no significantly different between two groups, but in NG reported higher calcium intake than in OG, proba bly because of the subjects in NG keep drinking milk to support higher energy intake. It should be noted that to reduced calcium level in blood can increased osteomalacia and osteoporosis incidence.
salmon, sarden, mackerel, tuna, and cod fish oil, but less found in milk, eggyolk, butter, margarine. Some of these food sources already fortified with vitamin D, some supplement already contain ergocalciferol (D2) that extracted from mushroom or D3 from lanolin. UV B exposure may be one of suggestion to rise serum 25(OH)D level, but many studies also mention about. It is neither necessary nor advised that people receive excessive UV irradiance to obtain adequate vitamin D production. While it is now evident that ordinary
dietary sources of vitamin D3 do not supply enough for adequate health (around 250–300 IU/day in the USA; very little fortification with vitamin D3 in Europe), supplements are a
safe and reliable source of vitamin D3. However, supplements are not consumed by enough
subjects in this study, nor food sources of vitamin D (27, 28). This study found that in NG,
dietary vitamin D consumed 1.35±0.6 g per day in NG and 2.9±1.2 g per day in OG. Food
sources found in egg yolk, fish, and meat, less eat mushroom is the caused of less dietary
vitamin D. All nutrient recall data showed a bias (responden bias), for example in OG, the subjects tried not to report nutrient intake per day and in NG, seems over intake, but we minimized it with food models and trained nutritionist.
Several studies have shown 25-hydroxyvitamin D related to insulin sensitivity, hypovitaminosis D are at a higher risk of insulin resistance and the metabolic syndrome. Several pathways reported, which vitamin D could promotes the secretion of insulin (30). Vitamin D promotes uptake of calcium by β cells via non-selective voltage-dependent
Our data showed that there was no reduction in blood pressure by vitamin D or influenced by calcium in both group. This could be because of blood pressure shows markedly cicardian variations, we cannot rule out that the method we used was inappropriate to detect small but significant changes in systolic or diastolic blood pressure.
In this study, we observed that deficiency was not only happened in overweight-obese subjects but also in normoweight, so it did not depend on adipocyte status. We noticed that there were three factors that influenced, firstly, in obese subjects, vitamin D deficiency could be because of adipocyte trap, so that the vitamin D was hard to release. Secondly, in normoweight subjects, the less intake of fat and vitamin D sources could caused deficiency people with less sunlight exposure is probably have higher incidence to have a lower serum 25(OH)D concentration.
Setiati et al (13) showed that UV B exposure from sunlight for 25 minutes, 3 times a week for 6 weeks could improves the vitamin D status in elderly women in Indonesia. Zitterman et al (6) also reported that vitamin D supplement of 83 g/d does not adversely affect weight loss and is able to significantly improve several cardiovascular disease risk markers in overweight subjects with inadequate vitamin D status. Hypovitaminosis D researchers clearly mentioned that one of the cause is vitamin D receptor (VDR) gene
polymorphism. However, every population give different prevalence of single nucleotide
polymorphism for each VDR gene such as Taq1, Bsm1, Fok1 or Apa1 (10). Need more
research for every population that correlated to hypovitaminosis D especially in Indonesia.
Furthermore, we need to reassess the requirement for vitamin D in tropical country.
different location and larger sample size to present variation among ethnics in tropical country. Summary of this result were there are factors that clearly different between normoweight and overweight-obese women, whether in age, adipocyte status, systolic or diastolic pressure, but in lifestyle that avoiding sunlight exposure, serum 25(OH)D and calcium concentration showed no significant different. Serum 25(OH)D level categorized deficiency was found in both groups.
CONCLUSIONS
This study reported that in normoweight and overweight-obese healthy women found vitamin D deficiency with different possibility has been found, in normoweight probably because of lack of vitamin D intake and less UV B exposure, but in overweight-obese probably because trap of vitamin D in adipocyte and less UV B exposure. With this result we can generalized that in the population especially in indoor working women and further analysis of the caused effect study, can prevent the vitamin D deficiency in tropical country.
REFERENCES
1. WHO-WPRO. The Asia-Pacific perspective: Redefining obesity and its intervention, pp. 22. Health Communications Australia Pte. Limited. 2000. Available from http://www diabetes.com.au/pdf/obesity_report.pdf cited 25 Januari 2011.
2. WHO. The World Health Report: Working together for health, Geneva. A growing challenge. N Engl J Med. 2006; 356:3, 213-215.
3. Hossain P, Kawar B, and Nahas ME. Obesity and diabetes in developing world. N Eng J Med. 2007; 356: 213-215.
4. Bray GA and Bellanger T. Epidemiology, trends, and morbidities of obesity and the metabolic syndrome. Endocrine 2006; 29: 109-17.
5. Riset Kesehatan Dasar/Riskesdas. Badan Penelitian dan Pengembangan Kesehatan, Departemen Kesehatan, Republik Indonesia, 2010.
6. Zittermann A, Frisch S, Berthold HK, Gotting C, Kuhn J, Kleesiek K, Stehle P, Koertke H, and Koerfer R. Vitamin D supplementation enhances the beneficial effects of weight loss on cardiovascular disease risk markers. Am J Clin Nutr. 2009; 89: 1321-1327.
7. Haslam DW and James WP. Obesity. Lancet. 2005; 366:1, 197-209.
8. Chiu KC, Chu A, Go VLW, and Saad MF. Hypovitaminosis D is associated with insulin resistance and β-cell disfunction. Am J Clin Nutr.2004; 79: 820-825.
9. Alvarez JA and Ashraf AP. Role of vitamin D in insulin secretion and insulin sensitivity for glucose homeostasis. J Endocrinol. 2010; 351-385.
11.Rahman SA, Chee WS, Yassin Z, and Chan SP. Vitamin D status among postmenopausal Malaysian women. Asia Pac J Clin Nutr. 2004; 13: 255-260.
12.Khor GL, Chee WSS, Shariff ZM, Poh BK, Arumugam M, Rahman JA, and Theobald HE. High prevalence of vitamin D insufficiency and its association with BMI-for-age among primary school children in Kuala Lumpur, Malaysia. BMC Public Health. 2011; 11: 95-103.
13.Setiati S, Oemardi M, Sutrisna B, and Supartondo. The role of ultraviolet-B from sun exposure on vitamin D3 and parathyroid hormone level in elderly women in Indonesia. Asian J Gerontol Geriatr . 2007; 2: 126-132.
14.Grant WB and Holick MF. Benefit and requirement of vitamin D for optimal health: a review. Altern Med Rev. 2005; 10: 94-111.
15.Holick MF. The vitamin D epidemic and its health consequences. J. Nutr . 2005 135: 2739S-2748S
16.Holick MF. Vitamin D deficiency. N Engl J Med. 2007; 357: 266-281.
17.Vieth R, Biscohff-Ferrari H, Boucher B et al. The urgent need to recommend an intake of vitamin D that is effective. Am J. Clin Nutr. 2007; 85: 649-50
18.Aloia JF, Patel M, Dimaano R, et al. Vitamin D intake to attain a desired serum 25 -hydroxyvitamin D concentration. Am J Clin Nutr. 2008; 87: 1952-8
19.AKG. Angka Kecukupan Gizi yang Dianjurkan bagi Bangsa Indonesia. Keputusan Mentri Kesehatan Republik Indonesia. No. 1593/MENKES/SK/XI/2005.
20.www.indonesia.com/whether_of_Indonesia.html
21.www.worldatlas.com/aatlas/htmfindlatlong.htm
23.Norman AW. Sunlight, season, skin pigmentation, vitamin D, and 25 -hydroxyvitamin D: integral components of the vitamin D endocrine system. Am J Clin Nutr. 1998; 67: 1108-10.
24.Jain R,von Hurst PR, Stonehouse W et al. Association of vitamin D receptor gene polymorphisms with insulin resistance and response to vitamin D Metab Clin and Exp 61. 2012; 293-301.
25.Lucas R, McMichael T, Smith W Amstrong B. Environmental Burden of Disease Series, No. 13 Solar Ultraviolet Radiation Global burden of disease from solar ultraviolet radiation. 2006. World Health Organization Public Health and the Environment Geneva.
26.Holick, M.F. Sunlight "Dilemma: risk of skin cancer or bone disease and muscle weakness. Lancet. 2001; 357 (9249): 4-6.
27.Hollis, B.W. Circulating 25-hydroxyvitamin D levels indicative of vitamin D sufficiency: implications for establishing a new effective dietary intake recommendation for vitamin D. Journal of Nutrition.2005; 135 (2): 317-322.
28.http://www.epa.gov/sunwise/doc/uvradiation.html
29.Palomer X, Gonzalez-Clemente JM, Blanco-Vaca F, and Mouricio D. Role of vitamin D in the pathogenesis of type 2 diabetes mellitus. Diabet, Ob and Metab, 2008; 10, 185-197.
TABLE 1. Descriptive characteristics of subjects by age, ethnicity, and lifestyle
Ethnicity: Bataknese: Batak, Mandailing, and Karo; Others: Aceh, Minangkabau, Malay, Chinese, Nias
3
TABLE 2. Distribution of subjects according to nutrient intake
TABLE 3. Clinical characteristics of subjects
Data was presented in mean±SD
2