Clinicopathological
Aspects of Breast
Cancer
:
A
joint
study between Indonesia and Japan
Didid
Tiindarbumi',
Muchlis
Ramli'.
Susumu
Watanabeï.
Idral
Darwis-.
Goi
Sakamoto$."
'
iuna*an
Tjahjadi+, Esti Soetrisno+,
Yoihiyuki
Ot"ol,l,'Endang Sri Roosiinit,
Santoso
Cornain+'
.GJoedo Prihartonor,
Sadao Suzu"t<ill, SetyawatiBudiningsihr, Éenji Wakail
IAbstrak
Masalah penatalalcsanaan klinik dari kanker payudara tetap penting d.alam hal diagnosis dan pengobatan. Telah d.isarankan oleh penelitian-penelitian terdahulu bahwa perlu d,ipikirkan dua subset kanker payudara, yaitu penyakit yang agresif dan yang
pertumbuhan-nya tidak nyata secara klinis (indolen). OIeh karena itu, penelitian aspek klinikopatologik kanker payudara berkaitan dengan fenomena sémacam
itu menjadi penting untuk dilakukan pada wanita Indonesia
juga.
Bersamaan dengan penelitian epid,emiologik secara kasus-kontrol 300 kasus kanker payudara telah dianalisa terhadap aspek klinikopatologiknya. Semua kasus dievaluasi secara klinis menggunakan klasifikasi intemasional TNM dan Manchester yanç baku dan secara histopatologik menggunakan modifikasi klasifikasi WHO seperti yang dianjurkan oleh Perhimpunan Kanker PayudaraJepang. Protokol penatalaksanaan kanker
payudara dari Perhimpunan Ahli Bedah Onkologi Indonesia yang d.isesuaikan dengan pedoman yang diterima secara luas diterapkan seperlunya. Hasilnya menunjukkan bahwa kasus-knsus kanker payudara paling sering ditemukan pada golongan umur dibawah 35 tahun dan di anlara 40 dan 44 tahun. Sebagian besar (87 7o) pada stadium lanjut (stadium IIIA, IIIB dan IV) sedangkan hanya1j
Vo pada stadiumdini(stadiumldanll).
Diantara300kasushanyall0
lasusyangoperabel. Prosedurbedahyangditerapkanadalahsebagaiberikut: mastektomi radilul pada 50 kasus (16.6 Vù, mastektomi sederhana pada 40 kasus (13.37 Vù dan bed.ah konsewasi payudara pada 2 kasus (0.67 Vo). Kejangkitan kelenjar getah bening ditemukan pada 20 dari 50 kasus dengan mastektomi radikal, dan jumlah rata-rata kelenjar getah bening yang didiseksi adalah 6.8. Sebagian besar (88.33 Vo) adalah karsinoma duhal invasif dan sisanya jenis khusus (9.67 Vù dan karsinoma non-invasif (1.jj
%). Dua kasus (0.67 %) adalah penyakit Paget payudara. Di antara karsinoma duktal invasif jenis skirus merupakan jenis yang paling sering (49 Vo).Abstracts
Theproblemofclinicalmanagementofbreastcancerremainsimportantinrespecttobothdiagnosisandtreatment. Ithasbeensuggested. from earlier studies that two subsets of breast cancer might be considered, namely the agressive disease and the indolent one. Therefore,
the study of clincicopathological aspects of breast cancer in respect to such phenomena became important to be conducted in Indonesian females as well.
In
parallell
to
the epidemiological case-control study, 300 breasl cancer cases have been analyzedfor
their clinicopathological aspects. All cases were evaluated clinically using standard International TNM and Manchester Classification and hi*opathologically using mod.ified WHO classification as recommended by the Japanese Breast Cancer Society. Breast cancer management protocols of the Indonesian Surgical Oncology Association as adapted from the widely accepted standards were applied accordingly. The results showed that the breast cancer cases were mostly found in the age group und,er 35 years and. between 40 to 44 years. The majority (87 %) were in advanced stage (stage IIIA, IIIB andN)
while only 73 Vo were in early stage (stage I,il)"
Out of 300 cases only 770 cases were operable. The surgical procedures which were applied were as follows: radical mastectomy on 50 cases (16.6 Vo), simple mastectomy on 40 cases (13.37 Vù and breast conserving surgery on 2 cases (0.67 Vo). Lymph node involvement was found in 20 oul 50 cases with radical masteclomy, and the average number of dissected lymph nodes were 6.8. The majority (88.33 Eù was of invasive ductal carcinoma and the resl were special types (9.67 Vù and non-invasive carcinoma (1.33 Vù. Two cases (0.67 Vù were Paget's disease of the breast. Among the invasive ductal carcinoma the scirrhous îype was the most common type (49 %).Keywords
:
b reast ca ncer, clinicopathological aspects, surgical p roceduresDepartntent of Surgery, Ftculty of Medicine, Universily of Indonesia Dr. Cipto Mangunkusmo National Central General Hospital,
Jakar-àonæia-
Clinical
management of breast cancer remains
as ani
x-s.*8try,.cancerlnstitute,Tokvo170,Po':-.
important
problems,
including its biology,
diagnosis
r
of Anatomic Pathologv' Faculry orMedi
rc'universitv
;;â
1;",
tment.
It
has been estimated
that mortality
sll
Medicine, Nagoya University, ,",Totqo170,Ja Schoolan
of
amounted
breaSt
cançer mOrtality has been obServed in
to
40 7o.l
Considerable increase of the
28Medicine,
r
'' l)epartme^
developed
countries
from 1960
to
1980,
with
22
7odrcutz, Untversrty ol lndone tarJal(arla , '2
..I0i30,Indonæia.
change.'
The prognosis
has been considered poor,
" R<ls"orrh Center
for Meilical Science and Technology, Facultyof
with
about 5O
%
S-yearrelative survival
anda
15-20
Vol 4, No 3, July - September 1995
an
andwomen
3.9
per , breastcancer rânked the second
i.e. in the
19g9the relative
It
is
of
interest
to
study the
similarity
and
the dis_
similarity
of
the breast cancer problems between
theIndonesian patients and the
Japanesepatients
in
acollaborative study.
This
study was conducted
to
evaluate the
clinico_
pathological
aspects
of
breast cancer
in
ldonesian
femalesin relation
to theepidemiological
study on riskfactors
in
breast cancer.The findings
will
response
totherapy.
statusbackground w
METHODS
most
instances.In
all cases
histopathological
examination was
doneand
for
clinical
al TNM
Clas_sifications'e
was
and2).
Basedon the extent of
t
metastasis the caseswere
alsoevaluated whether
theywere
operableor non-operable.
Clinicopathologlt of Breast
Cancer
L4gradiotherapy
asadjuvant therapy, according to
Breast Cancer Managementprotocol
of theIndonesian
Surgi_cal Oncology Association
(seeTable 1
).ffitJr".'fr:fJ
was
adaptedfrom widely
acceptedpro-RESULTS
The
agedistribution
of
the
300 female breast
cancer aregiven
in
Table
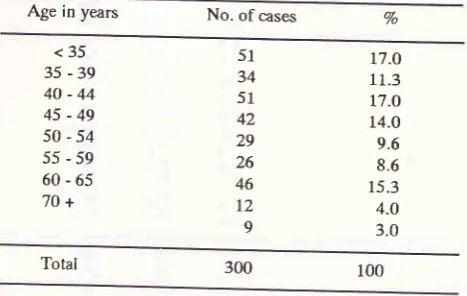
1.The highest
proportion of
breastcancer
caseswere
in
the age group under 35 years andbetween 40_44years.
Lower
peak was seen in the agegroup
of 60_65
years.Table 1. Age distribution of 300 female breast cancer
Age in years No.
ofcases
Vo
<35 35
-39
40-44
45-49
50-54
55-59
60-65
7O+t7.o
11.3
t7.o 14.0 9.6 8.6 15.3 4.O 3.0 51
34 51 42 29 26 46
I2
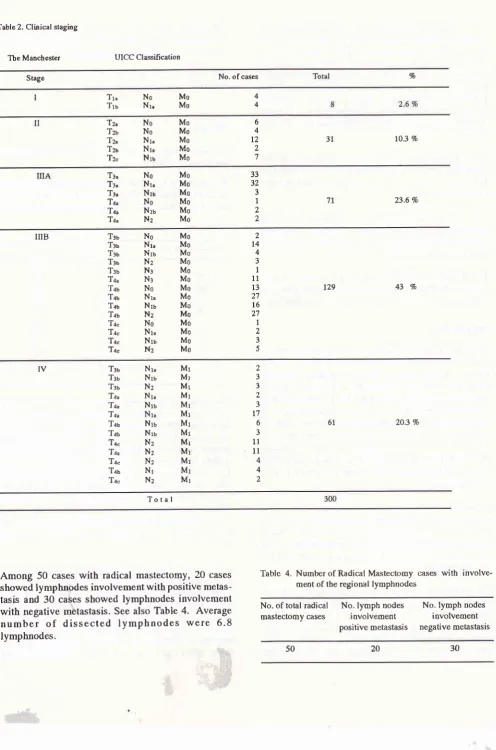
9 [image:2.595.311.545.306.454.2]T able 2. Clinical staging
The Manchester UICC Classification
Stage No. of cases Vo
4
4
No
MoNr"
Mo Tr"Tru
10.3 Vo
3l
6 4 t2 ,)'l
No
MoNo
MoNr"
MoNr"
MoNru
MoTN Tzt Tz. Tza '12"
23.6 Vo
71 33 32 3 1 J
)
No
MoNI"
MONru
MoNo
MoNru
MoN:
MoTt"
Tl.
Te" Tq" Tq. Ta^43 Vo
t29)
t4 4 J 1 11 t3 2'7l6
27 1)
3 5Ttu
No
MoTl
Nt"
MoT*
Nt
MoT:r
Nz
MoT:u
Nr
MoTau Nt
MoT.lr
No
MoTlu
Nr"
MoTlu
Nru
MoTau Nz
MoT+
No
MoTu
Nt"
MoTl"
Ntt
MoTn.
Nz
MoIIIB 61
)
3 3 a J t7 6 3 1r 11 4 4 2 IVTtt
Trr Tru Tu Tu Tu Tlu Tat Ta. Ta' Ta. Tru Ta. Nr, Nru Nz Nt" Nru Nt" Nru Nru Nz Nu Nz Nr Nz Mr Mr Mr Mr Mt Mt Mr Mr Mr Mr Mr Mr Mr203 Vo
Total
Among 50
caseswith
radical
mastectomy,
20
cases showedlymphnodes involvement
with
positive
metas-tasis and 30
cases showed lymphnodes involvementwith
negative
metastasis. Seealso Table
4.
Average
number
of
dissected
lymphnodes
were
6.8
lymphnodes.
Table 4. Numberof Radical Mastectomy cases
with
involve-ment of tbe regional lympbnodesNo. of total
radical
No. lymphnodes
No. lymph nodes mastectomycâses involvement
involvementpositivemetastasis negativemetâstasis
[image:3.595.71.568.61.812.2]Vol 4, No 3, July - September 1995
The
operable caseswere evaluated for their tumor
siteand
the
results can be
seenin
Table
5. patients
with
radical mastectomy was higher than the one with
simple
mastectomy
(16.6 %
and
13.37%
of
thetotal
300 breast cancer
casesrespectively. BCT
was
only
performed on
2 cases.Table 3. Number of patients o[ respective surgical method
Surgical method No. of operable cases Peroentage
(from all 300)
Clinicopathologt of Breast
Cancer
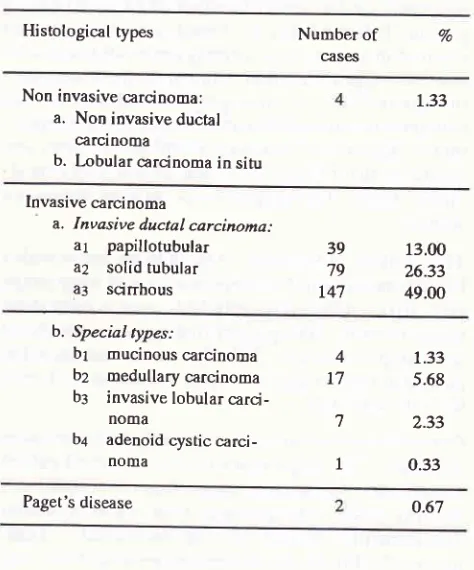
151Table 6. Distribution of 300 breast canær qrses according to
histological types
Histological types Number
of
Vocasqs
Non invasive carcinoma: a. Non invasive ductal
carcinoma
b. Lobular carcinoma in situ
1.33
Invasive carcinoma
a. Invasive ducîal carcinoma:
a7
papillotubulara2
solid tubulara3
scinbous39 79 r47 13.00 26.33 49.00 Radical mastectomy
Simple mastectomy
Lumpectomy / BCT
50 40 2 L6.6 13.37 0.67
b. Special types:
bt
mucinous carcinomabz
medullary carcinomabr
invasive lobularcarci-noma
b+
adenoidcysticcarci-noma
Total
Most of
breast cancerswere
found in
theupper outer
quadrant
(73.9
Vo),followed by
upper inner
quadrant(I0.8
%o),lowerinner
quadrant (8.6%),subareolar
(4.3 7o) andlower
outer quadrant
(Z.l
Eo).Table
5.
Distribution ofoperable breast cancer casesaccord-ing tumor site
Site
No. of cases PercentageThe
histological typing
was evaluatedon
110 operable cases, as can be seen in Table 7.Similarly,
theinvasive
ductal carcinoma
weredominant, consisting of
mostly
(64.54
7o) thescirrhous type,
followedby
12.72 Toof
papillo{ubular type
and7.27
%of solid-tubular
type.
The
restwere the special
type
(mucinous, medullary,
lobular
andadenoid cystic).
Paget's dlsease o.67
Table
7.
Distribution of 110 operable cases ofbreast canceraccording to histological types
Histological types Number of
cases 92 4
I7
7 1 1.33 5.68 2.33 0.33Upper outer quadrant
Lower outer quadrant
Upper inner quadrant
Lower i nner quadrant
Subareolar % 68 2 10 8 4 72 2 6 5 1 2 73.9 2.r 10.5 8.6 4.3
Invasive ducfal papillo-tubular carcinoma
Invasive ductal solid tubular carcinoma
Invasive ductal scinhous carcinoma
Mucinous carcinoma Medullary carcinoma Invasive lobular carcinoma Adenoid cystic carcinoma
Paget's disease
I4 14.72 7.27 64.54 1.81 5.45 4.54 0.90 1.81
Total 92 100
The results
of histological typing oil all
300 cases aregiven in
Table 6. The
majority
tù/erethe invasive
car-cinoma, consisting mostly (88.33
Vo)of
theinvasive
ductal
carcinoma
and9.66 7o
of
thespecial type, and
the rest (1.33 7o)werenon-invasive
anrcinoma.paget's
[image:4.595.322.559.107.392.2] [image:4.595.58.296.332.646.2] [image:4.595.319.555.390.735.2]DISCUSSION
The
study on
the
agedistribution
of all
breast cancerpatients indicated that the
breast cancer has
alreadyoccured
in
younger
age,namely under
40
years,with
relatively
high
proportion. Similar
findings
were seenin
Jakartars and
in
other
geographicat
area
of
our
country
w it h ra the_r- different
demo graphicaI
co mpo si-tion
i.e. EastJava.ro
Such agedistribution
pattern wassimilar
to
that
of
Japanesewomen but
differs
corsid-erably
from
other
populations such as American
women.4
The
analysis
of
the
stageof
the
disease has revealed that themajority
(87
Vo)were in
advanced stage (stageIIIA,
IIIB
andIV)
while only
13 7o werein early
stage(stage
I
andII).
The
presentfindings
were
consistentwith
ourprevious
data.^'''' This
wasin
contrast to thepattern
of
breast ca4cerin
Japan, themajority
of
caseswere
in
early
stage.)Out
of
300 breast cancerpatients
only
110 cases wereoperable. The proportion
of
casesthat
need radical
rnastectomy was
slightly
higher than
thesimple
mas-tectomy
cases. Our previous study
showed
similar
dataeven
after
1O-yearsurvival observation.lT
Lu--pectomy or
breastconserving tumorectomy
wereonly
performed
in
2 cases(0.67
7o).The evaluation on tumor site
showed that
the tumor
occurred
mostly
(73.9
Eo)in
the upper outer quadrant.Histological typing
on
all
300 breast cancer cases hasrevealed that the
majority
were the invasive carcinoma,with
predominance
of
invasive ductal type
andsmall
proportion
of
special type, while
only
1.33
7owere
non-invasive carcinoma.
Evaluation
on
110 operable casesresulted
in
similar findings, i.e. mostly the
in-vasive ductal carcinoma,
two-third of which
were
thescirrhous
type.
The
latter
has been observedto show
lower
10-year
survival
rate
ascompared
to
the other
types i.e. papillo-tubular
and
medullary tubular
car-cinoma.)
Paget's
diseasewere
only
found
in
2 cases.Our
datashowed
both sirnilarity
anddissimilarity
be-tween
the breastcancer
in
Indonesian women
and theJapanese
*o-"o.18
Our prelirninary study
of
hor-monal receptor expression
in
50
lndonesian
breast cancer casesindicated
thatT2o/o were estrogenreceptor
(ER)
rich
breast cancers.
More
than
two-third of
patients
with
moderate differentiation showed
ER-positivity.
Furthermore,
it
contributed
to the evidenceof subsets
of
breast
callcer relative
to its
biological
behavior,
i.e. agressive,
indolent or in between.
Fur-ther study
needselucidating
related factors
in
respect1o such
difference
in biological
behavior.
Thus,
we
anticipated
that clinicopathological
study
would
take the
benefit of
related studies such
ashor-monal receptors
(estrogen andprogesteron
receptors)and oncogenes
(c-erbB-2
and
p53).
It
has
been reportedrecently
that the expressionof
suchmolecular
markers
might
influence
therisk of
tumor
growt-h, thedisease
prognosis
and the responseto
lherapy.19-22Acknowledgments
The authors are
grateful
to the nursesMs.Emi
andMs.
Ros
and
for public health
nurses,
Ms. July
and Ms.
Erlaini
for
excellent care and
collection
of
data of
breast cancer cases andcontrols.
We
are alsoindebted
to
thelaboratory
lechnician for
excellent
work
on thesurgicopathological
specimens.This work
was supportedby
theMinistry
of Education
and
Culture,
Japan,
Grants
No.
01042007
and
04042013; and was
partly
supportedby
theIndonesian
Cancer
Foundation. This collaborative study was
apart
of
Special
Cancer ResearchProject
in
Monbusho
International
Scientific
Research
Program,
with
theapproval of
the Dean,Faculty of
Medicine, University
of
Indonesia, No. 4383
lPT02.H4.RK /
E
/
88.REFERENCES
1. Waterhouse
JAH.
Measurement and monitoring of the im-pactoFcancer. In: KhogaliM,
OmarYT,GjorgovA, IsmailAS, editors. Cancer Prevention
in
Developing Countries. Oxford: Pergamon Press, 1986:211-7.2. Stanley K, Stjemsward J, Koroltchouk
V.
Women andcan-cer. Wld hlth statistquart 1987;40:267-78.
3. Mueller CB, Jelfries
W. Cancer of tbe breast: Its outcome
as measured by the rate
of
dying and causes of death. Ann Surg 1975; I 82:334-41 .4. Sakamoto
G,
SuganoH,
HartmanWH.
Comparative pathological studyof
breast carcinoma among Americanand Japanese women. In: McGuire WL, editors. Breast
Can-cer. Nasbville USA:
PlenumPublishing
Corporation,L98I:2II-31.
5. Sakamoto G, Sugano H. Pathology of breast cancer: Present
and prospect
in
Japan. Breast Cancer Res and Treatment 1991;18:S81-3.6. Cornain S, Mangunkusumo R, Nasar IM, Prihartono J. Ten Most Frequent Cancers in Indonesia: Pathology based
Can-cer Registry Data
of
1988-1989.In:
Czncer Registry inIndonesia. National Cancer Registry Center, Jakarta Coor-dinating Board, 1990.
7.
Sarjadi.
Cancer Incidence 1985-1989in
Semarang,In-donesia. Indonesian Cancer Society 1990.
8. Baum M. Breast Cancer: The facts. Oxford: Oxford Univer-sity Press, 1981.
9.
TNM
Atlas: Illustrated Guide to tbe TNMÆTNM
Vol 4, No
j,
July - September 199510. Breast Cancer Management protocol ofthe Indonesian Sur_
gical
Oncology Association.(In
Indonesian). Ropanasuri1989;18, 89-93
11.
Heelman S, RosenbergSA.
Cancer principlesf
Oncology. Philadelphia: J.B. Lippincorr Co.,12. Vadya MOP, Shukla S. A textbook of Breast Cancer. New Delhi: Vikas publisher, Home pVT Ltd, 19g3:54-67. 13. Haagensen CD. Diseases
ol the Breast. philadelphia: W.B.
Saunders, 2Dd ed l97l:.348-54.
14. Donegan WL, Spratt JS. Cancer of the Breast, philadelphia:
W.B. Saunders, 1979:15-43.
15. Tjindarbumi
D.
Early detectionof
breast cancer(ln
In-donesian). Annual Scientific Meeting of Indonesian Surgeon
Associations, Jakarta, 1982.
16. Sukardja I.D.G. Early detection o[breast cancer in EastJava,
impact of public education on cancer:
A
longitudinal study. PhD Thesis. Surabaya: Facultyof
Medicine, Airlangga University, 12Jlly,
1984.Clinicopathologt of Breast
Cancer
153I7.
D.
Managementandresultsofoperablebreasteral hospitals in Jakarta: A lO_year survival rate
Indon J Oncol 1991;2: t47 _160.
18. Cornain S, Ohno Y. progress Report. Japan-Indonesia Joint
Study on Etiology and Clinioopathology o[Breast Cancer.
Jakarta: School of Medicine University of Indonesia
,
lgg2,
Muy.19. Mcleman A, Thomas DB, Johnson LIÇ Rossman
D.
Risk factors for estrogen receptor-rich and estrogen_poor breast câncers. JNCI 1986;77 :849-54.20. Cavalli F. Clinical research in advanced breast canoer: Back
to the future. Ann Oncology l99L;2:621-2.
2l.Iwaya K,
Tsuda H, HiraideH, Tamaki
IÇ Tamakuma
S,Fukutomi T, et al. Nuclear p53 immunoreaction associated wi th poor prognosis of breast cancer. Jpn J Cancer Res 1991;
82:83540.
22. Taktkawa
Y,
NoguchiM, Kitagawa
H, Thomas
M.
Im_munohistochemical detection
of
p53 and c-erbB_2 proteins: Prognostic significance in operable breast canær. Breast154
Tjhdarbumi
a
aLAppendix-1
Breast canær management protocol - Indonesian Surgical Oncology Association, December 1989
MedJ
IndonesStage
I
Tt"
Tru
No-t" No-ta
Mo Mo
Radical mastectony or modified radical mastectomy
If
lymph node negative: observation onlyIf
lymph node positive: regional imadiation + adjuvant chemotherapyStage
II
ToT1" Tru
Tzt
Tu
Tzu
Nru Nru
Nrr
No-1.
Nr
Nru
Mo Mo Mo Mo Mo Mo
Radical mastectomy or modified radical mastectomy with irradiation on
tumor bed and regional lymph node
Stage
III
Any Tr with any N MoAny Ta with any N Ms
Any T with N2 Mo
Any
Twith
Ng MoStage
III
is divided into StageIIII
and StageIII3
Stage
IIIA
T3"-4"
No-z
MoTu-zt Nz
MoSimple mastectomy with irradiation of tumor bed + regional lymph-node
+ chemotherapy as adjuvant therapy
Stage
IIIB
f36a5-a. any N Mo Considered as non-operable primary treatment is irradiation ontumor bed + lymphnode region + chemotherapy + hormonal therapy
Stage
IV
Any T any N witbMl
Primary treatment is hormonal tberapy. This is divided into 3 groups.l.Premenopausal women
-
castration / anti estrogen therapy2.Women with 1-5 yr post menopausal status were evaluated for the estrogen activity on vaginal smear:
If positive
.-
castration/or anti estrogen tberapyIf
negative-
considered as post menopausal case+
anti estrogen therapy3 Women after5 yrs post menopausal status
-
estrogen therapyEstrogen and Progesteron receptor assessmeDt in respect to the therapy is not yet done routinely in our Hospital
Notes:
Adjuvant chemotherapy is given with the regimen of CMF (6 cycles).
C
=Cyclophosphamide orally 60-80 mgm2lday,day 1 until day 14.M =Methotrexate 4O mglm2 i.v., day 1 and day 8.
F
=5 Fluorouracil 600/m2 i.v., day 1 and 8.I
Vol 4, No
j,
July - Septenber 1995Appendix-2
Breast Cancer Classification:
TNM
system (UICC) Tumor size (T)Clinicopatlnloglt of Breast
Cancer
155Not palpable
=2m
>2-5 cm>5cm
No deep fixation To Tr
Tu
T:.
With
[ixation
Tru
TzaAny size + direct chest extension Any size + skin infiltration or oedema
or peau d'orange or satelite nodule confided to same breast
Tau
T+
T+t
T++Tnu+=T4c
Nodal Status (N)
No
Nr
Nrr
NzHomolateral axillary nodes Not palpable Palpable Palpable Palpable
Clinical non-malignant
Clinical
malignant Malignantfixed
Homolateral clavicular node(s) clinically malignant or oedema of arm
Nr
Metastases (M)
Mo
No clinically apparent distant metastasesMr
Distant metastases apparentThe Manchester / UICC Classification
Stage I
Tt"
Tz.
NoNo MoStage
Il
ToTt"
Tz^
Nr
Nr Nr
Mo
Stage
III
TgTo,t,z
Ttu, Tzu Tq
Nqr,z Nz
Nqlz
Nqr,z
Mo