Communication ability in non-right handers
following right hemisphere stroke
Catherine Mackenzie
a,*, Marian Brady
baDepartment of Speech and Language Therapy, University of Strathclyde, Southbrae Drive, Glasgow G13 1PP, UK
bNursing Research Initiative for Scotland, Glasgow Caledonian University, Glasgow G4 0BA, UK
Abstract
Communication ability following right brain damage (RBD) has been frequently investigated, but almost exclusively in the right handed (R) population and where non-right handers (NRs) have been studied their inclusion has been motivated by the presence of aphasia. Communication assessment, covering aspects of spoken discourse and comprehension, which in Rs are sensitive to the effects of RBD, was carried out on five NR adults 3 months after right hemisphere stroke. Performance was compared to matched R stroke participantsðn¼9Þ and non-brain damaged (NBD) participants
ðn¼20Þ:On all communication measures there was remarkable similarity between the scores of the
R and NR RBD groups. Both stroke groups were significantly impaired in comparison with the NBD group in inference comprehension and in non-verbal conversational parameters. The RBDNR group was less efficient than the NBD group in conveying relevant picture description content and a similar trend was present for the RBDR group. The RBDR group scored significantly below the NBD group in tests of discourse and metaphor comprehension. Future research involving NRs should examine communication difficulties within a broad context of functions to inform the relationship between language and other presumed lateralised higher functions.
q2003 Elsevier Ltd. All rights reserved.
Keywords:Communication; Right brain damage; Handedness
The left hemisphere of the brain’s major role in language processing has been recognised since the work of Dax in 1836 and Broca in 1865 when the presence of aphasia began to be
associated with left hemisphere damage in right handed people (Joanette & Goulet, 1994)
Subsequently the belief was widely held that for left handed people language was
lateralised in the right hemisphere (Subirana, 1969). Cases of aphasia in left handers
following left lesions were reported intermittently but it was not until the publication of
0911-6044/$ - see front matterq2003 Elsevier Ltd. All rights reserved. doi:10.1016/S0911-6044(03)00061-7
www.elsevier.com/locate/jneuroling
* Corresponding author. Tel.:þ44-141-950-3454; fax:þ44-141-950-3451.
systematic surveys such as that ofGoodglass and Quadfasel (1954)that it became clear that neurological language control in non-right handers (NRs) was not merely a mirror image of the situation for right handers (Rs). NRs are a heterogeneous group as regards language laterality and it may even be that some have separate hemispheric loci for speech
output and comprehension (Naeser & Borod, 1986).
For the majority of NRs the left hemisphere is dominant for language and functional magnetic resonance imaging (fMRI) data indicate that 8% have right dominance and 14%
show symmetrical activation (Szaflarski et al., 2002). The likelihood of right dominance
appears to increase with the degree of left handedness (Knecht et al., 2000). Incidence of
aphasia following right brain damage (RBD) in NRs is often stated as around 30% though
in most NRs aphasia is associated with left damage (Marien, Paquier, Cassenaer, & De
Deyn, 2002). By contrast, aphasia resulting from RBD is an exceptional occurrence in Rs.
Early studies reported a higher incidence of aphasia in NRs compared with Rs (Conrad,
1949; Gloning, Gloning, Haub, & Quatember, 1969). Also the severity of aphasia was
sometimes noted to be less in NRs than in Rs (Luria, 1970) and prognosis for aphasia
recovery was believed to be better in NRs (Subirana, 1969). Such observations lent
support to the emerging view that in NRs language may be less strongly lateralised and so may be vulnerable with injury to either hemisphere but also less likely to be severely impaired than where left damage occurs in Rs with strong left hemisphere language control. However, in more recent research, differences in aphasia severity and/or recovery
in NR and R patients have not been found (Basso, Farabola, Grassi, Laiacona, & Zanobio,
1990; Kertesz, 1993; Laska, Hellblom, Murray, Kahan, & Von Arbin, 2001; Naeser & Borod, 1986; Pedersen, Jorgensen, Nakayama, Raaschou, & Olsen, 1995) andBasso et al. (1990)concluded that the importance of left handedness had been overemphasised in the past. Handedness related language performance differences were similarly not found in a
recent study of people with Alzheimer’s disease (Doody, Vacca, Massman, & Liao, 1999).
Premorbid handedness is regarded as an important variable to be controlled in
communication research (Brookshire, 1983; Kaplan & Goodglass, 1981; Wertz, 1993). In
most contemporary studies such control has been achieved by exclusion of those not clearly R. There exist few detailed studies of how stroke or other brain injury affects the communication skills of the NR population. Although the majority of the adult population
is R, at 4 – 11% (Ellis, Ellis, Marshall, Windridge, & Jones, 1998) NRs represent an
important section of the population.
In Rs with LBD language impairment is most commonly described using the classical or connectionist system of aphasia classification, though the proportion of cases who conform to definition may range from 30 to 80% depending on the strictness of adherence
to criteria (Goodglass & Kaplan, 1983). Knowledge of how acquired neurological damage
affects communication in NRs is especially limited for RBD. Where such cases have been included in language investigations, some have shown fairly classical aphasia profiles, and
others have had more unusual language patterns (Alexander & Annet, 1996).Gloning et al.
(1969)examined 25 matched R/NR pairs with RBD in the first week following hospital admission. On all of a range of language tasks the NR group was significantly more impaired, but the transience of aphasia was noted in this group. No severity difference was observed between R and NR groups who had left hemisphere lesions. The research of
time post-onset, and lesion location. As with their left lesion data, aphasia was very similar in the R and NR subjects. In further contrast to Gloning et al’s findings, for three additional unmatched NRs with RBD, aphasia recovery was unremarkable.
For the R population, while left hemisphere lesions frequently result in obvious and significant deficits in language, much recent research has indicated that RBD may also limit competence in communication, particularly in text level processing and pragmatics (the interaction between language behaviour and context). A cluster of ‘right hemisphere
communication deficits’ are identified in this population (Myers, 1999; Tompkins, 1995)
for which lately the diagnostic labels of ‘pragmatic aphasia’ (Joanette & Anslado, 1999) or
‘apragmatism’ (Myers, 2001) have been suggested. Correspondingly, fMRI and functional
transcranial Doppler ultrasonography (fTCD) studies have objectively demonstrated the right hemisphere’s contribution to language processing in the left hemisphere language
dominant R population (Knecht et al., 2000; Springer et al., 1999). In cases of language
impairment following RBD in NRs reported in the literature, because language assessment has been tailored to the diagnosis of aphasia, only those with frank language impairment would be identified. Information on how NRs with RBD perform in language tasks which are sensitive to the more subtle communication problems associated with right lesions is not readily available.
The present report provides initial data on the communication performance, both verbal comprehension and spoken discourse, of NRs following right hemisphere stroke. Comparison is made with Rs with similar age, education and stroke histories, and Rs without neurological damage. The assessment point for the neurologically impaired groups was 3 months post-stroke.
1. Participants
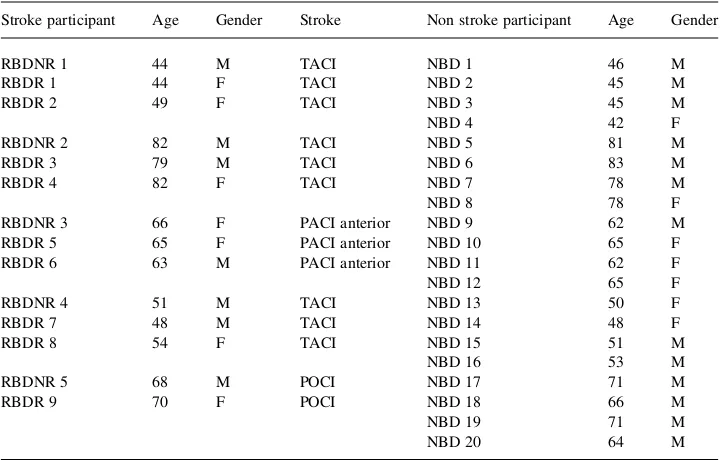
The RBDNR group comprised five non-right handed right hemisphere stroke
participants (mean age 62.2, SD 14.97). Each was matchedþ/2 5 years of age with:
(a) two right brain damaged right handers with similar stroke classification (RBDR),
with the exception of case RBDNR5 for whom only one match was available (n¼9;
mean age 61.56, SD 13.76), and with.
(b) four non-brain damaged right handers (NBD) (n¼20;mean age 61.3, SD 13.14).
Mean ages for the three groups were equivalent (ANOVA, F 0.009, df 2,p¼0:991).
No participant had formal education beyond the minimum UK legal requirement (school leaving age 14 until 1947, thereafter 15 until 1972, with school entry at age 5). Participants
were not gender matched. This is consistent with the findings ofMackenzie (2000a,b)that,
for the communication assessments used, gender was not an influencing variable, unlike age and education.
Repetition Test (Weeks, 1988). No participant was receiving speech and language therapy intervention. NBD participants by self-report were without neurological or psychiatric history. The NBD group was drawn from a database of 189 subjects, aged 40 – 88. Stroke participants had no record or evidence of previous neurological or psychiatric occurrence. The presence of right-sided stroke was diagnosed on the basis of clinical signs and in all but one case verified radiologically by CT or MRI. Stroke was ischaemic in all cases.
Stroke classification was according to the scheme ofBamford, Sandercot, Dennis, Burn
and Warlow (1988). Both RBDR and RBDNR groups were drawn from a database of 70 participants aged 36 – 86 with single right stroke, undergoing communication assessment at 3 months post-stroke. One RBDNR participant (case RBDNR1) was diagnosed by the speech and language therapist researcher as presenting aphasic features in conversation, principally agrammatism and paraphasic errors. None of the RBDR group was diagnosed with aphasia. Age, gender and stroke details for the three participating groups are given in
Table 1.
Handedness was assessed using the Edinburgh Handedness Inventory (Oldfield, 1971).
To be classified as R, subjects reported right handed preference for at least eight of the 10 test activities, including writing. For the NR group for at least six of the activities the left hand was used or either hand was used without preference. No participants recalled a parental history of left handedness.
Table 1 Participant data
Stroke participant Age Gender Stroke Non stroke participant Age Gender
RBDNR 1 44 M TACI NBD 1 46 M
RBDR 1 44 F TACI NBD 2 45 M
RBDR 2 49 F TACI NBD 3 45 M
NBD 4 42 F
RBDNR 2 82 M TACI NBD 5 81 M
RBDR 3 79 M TACI NBD 6 83 M
RBDR 4 82 F TACI NBD 7 78 M
NBD 8 78 F
RBDNR 3 66 F PACI anterior NBD 9 62 M
RBDR 5 65 F PACI anterior NBD 10 65 F
RBDR 6 63 M PACI anterior NBD 11 62 F
NBD 12 65 F
RBDNR 4 51 M TACI NBD 13 50 F
RBDR 7 48 M TACI NBD 14 48 F
RBDR 8 54 F TACI NBD 15 51 M
NBD 16 53 M
RBDNR 5 68 M POCI NBD 17 71 M
RBDR 9 70 F POCI NBD 18 66 M
NBD 19 71 M
NBD 20 64 M
2. Communication assessment
Previous communication research has indicated that measurements of spoken discourse, semantic judgement, and comprehension of metaphor and discourse, including
inference, are sensitive to the effects of RBD (Tompkins, 1995). The measures used in this
study were selected for their routine clinical availability, test – retest reliability for the
neurologically normal population (Mackenzie, 2000a,b) and of special relevance for the
spoken discourse measures, good levels of inter-judge and intra-judge scoring reliability (Mackenzie, 2000; Mackenzie, Begg, Lees, & Brady, 1999).
Auditory Synonym Judgements(ASJ) (Kay, Lesser, & Coltheart, 1992). Sixty pairs of words (divided into parallel sets of 30 pairs each) are presented in spoken form for decision as to whether the two words are similar in meaning or not.
Discourse Comprehension Test(DCT) (Brookshire & Nicholas, 1993). A series of 10 stories (divided into parallel sets of five stories, A and B), each of around 200 words, in which the frequency of content words is representative of adult conversation, is followed by a set of questions to be answered ‘yes’ or ‘no’. The questions cover main ideas and details and stated and implied information.
Metaphor Picture Test(MPT) (Bryan, 1989). Ten sentence metaphors are individually presented in spoken form each accompanied by a set of four pictures, representing the metaphorical meaning, the literal meaning and two control items.
Comprehension of Inferred Meaning Test (CIMT) (Bryan, 1989). Three short paragraphs, one conversational, one narrative and one emotional, each of around 60 words is each followed by four inferential questions. Presentation of both stimuli and questions is in combined written and spoken form with the written stimulus paragraph retained throughout.
Picture description. Description of the ‘cookie theft’ picture from the Boston
Diagnostic Aphasia Examination (Goodglass & Kaplan, 1983) analysed as follows:
number ofinterpretive units(CTIU) (i.e. units which derive meaning within the depicted
situation, e.g. mother, there’s going to be an accident, as distinct from literal units, e.g.
woman, stool), Index of efficiency in conveying content, calculated from word count
(number of words, including repetitions, comments and questions) relative to total content
units (literal plus interpretive) total (CTEFF), Occurences ofextraneous materialsuch as
digression, intrusion of personal material or opinion, relative to total word count (CTEXT). The scoring guidelines for literal and interpretive content units were based on
the work ofMyers (1979) and Yorkston and Beukelman (1980).
Conversation. Approximately 10 min of conversation between the participant and assessor on everyday topics such as weather, employment, holidays, health, day to day activities and family were audio recorded for rating. Perceptual and observational ratings were carried out on eight conversational parameters, five verbal interactive (conversa-tional initiation, turn taking, verbosity, topic maintenance, referencing) and three non-verbal (intonation, facial expression, eye contact) using a five point severity scale, with
five representing ‘normal’ (Burns, Halper, & Mogil, 1985).
Conversational initiation. Conversational responsiveness and participation. Turn taking: co-operation in ‘floor sharing’, with reference to, e.g. interruption, reluctance to
to, e.g. inclusion of unnecessary or peripheral detail and repetition.Topic maintenance: relevance of contribution to topic in hand with reference to, e.g. unsignalled topic change
and introduction of irrelevant material.Referencing: coherence in referring to people and
events, enabling the listener to keep track of who and what is under discussion.Intonation:
variation in intonational contour, without reference to voice quality or habitual pitch. Facial expression: perceived appropriateness of facial expression.Eye contact:perceived appropriateness of pattern of maintenance and interruption. Ratings were summed on the five verbal parameters to provide a conversational interaction (CON) score (maximum 25) and on the three non-verbal parameters to provide a non-verbal (NV) score (maximum 15). Additionally for the RBDNR group, naming ability was assessed using the Graded
Naming Test (GNT) (McKenna & Warrington, 1983).
For stroke participants, communication assessment was carried out within 3 days of the 3 months post-stroke date. Assessors had access to the handedness and neurological status information of participants. Spoken responses were audiorecorded for transcription and analysis. Eye contact and facial expression parameters of conversation were rated at the time of data collection. For the scoring of picture description and all other conversation parameters, following initial practice and discussion, intra-judge and inter-judge reliability was assessed on 20% of the data from the RBD and NBD databases from which the participants for this study were drawn (respectively, 70 and 189 subjects). Agreements for all measures used in this study were at least 90%. Repeat testing of 20% of the group of 189 NBD subjects took place after an interval of 2 months. For all measures
used in this study correlations between T1 and T2 were significant ðp,0:01Þ and
performance differences were non-significant ðp.0:05Þ: Full details are given in
Mackenzie (2000) and Mackenzie et al. (1999).
3. Results
Communication assessment scores of the three participant groups are contained in
Table 2. Given the nature and size of the group compositions and the ordinal level of measurement, non-parametric analysis procedures were used (Kruskal Wallis one way
analyses of variance followed by Mann Whitney U tests for relevant pairwise
comparisons). Two tailed tests were used. In view of the small size of the RBDNR
group the significance level was set at p¼0:05 and exact rather than asymptotic
significance reported for Mann Whitney tests.
Variance amongst the groups was significant in four of the nine measures: two relating to comprehension (DCT, CIMT) and two relating to spoken discourse (CTEFF, NV). In two other measures (MPT, CTIU) non-significant trends were apparent. For these six
measures pairwise comparisons were carried out (Table 3). The R and NR RBD groups
whereas the RBDNR group was not different from NBD. In the picture description efficiency measure the RBDNR group were significantly impaired in relation to normal and for the RBDR group there was a distinct trend in the same direction. Also for RBDNR there was a non-significant trend towards picture description interpretive unit scores being lower than for NBD.
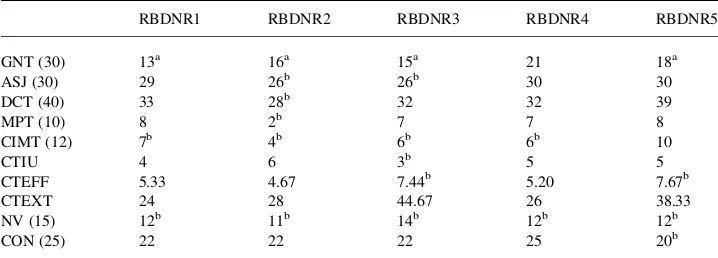
All RBDNR participants were low scorers in some measures.Table 4gives individual
measure scores for each RBDNR participant and indicates those measures on which performance was lower than one SD below the mean for the relevant published NBD age
and education controlled data (Mackenzie, 2000a,b). For GNT, low scores are similarly
identified with reference toMcKenna and Warrington (1983)mean (22.54, SD: 4.3).
NV was the only measure where by this standard the RBDNR group were consistently low performers. For CIMT four of the five participants were likewise impaired. Four participants had low scores on GNT. RBDNR2 and RBDNR3 showed the greatest number of low scores (six of the 10 measures). RBDNR4 was impaired in the lowest number of measures (two) and was the only one of the group to score within 1SD of the GNT mean. RBDNR1 was impaired in three and RBDNR5 was impaired in four measures.
Table 2
Communication assessment scores: means and standard deviations
Measure RBDNRðN¼5Þ RBDRN¼9Þ NBDðN¼20Þ p
ASJ (30) 28.20 (2.05) 27.50 (2.00) 28.15 (1.76) 0.645
DCT (40) 32.80 (3.96) 32.22 (1.64) 34.55 (3.90) 0.043*
MPT (10) 6.40 (2.51) 5.44 (3.54) 7.90 (3.01) 0.064
CIMT (12) 6.60 (2.19) 7.33 (2.06) 9.10 (1.92) 0.029*
CTIU 4.60 (1.14) 4.78 (2.05) 6.90 (3.04) 0.088
CTEFF 6.06 (1.38) 6.21 (2.91) 4.68 (1.74) 0.045*
CTEXT 32.20 (8.89) 30.28 (17.54) 51.34 (36.14) 0.148
NV (15) 12.20 (1.10) 11.22 (2.54) 14.75 (0.44) 0.000*
CON (25) 22.20 (1.79) 23.00 (1.41) 23.55 (2.06) 0.144
*p,0:05; ASJ: Auditory synonym Judgements, DCT: Discourse Comprehension Test, MPT: Metaphor
Picture Test, CIMT: Comprehension of Inferred Meaning Test, CTIU: Cookie theft interpretive units, CTEFF: cookie theft efficiency-higher scores indicate decreased efficiency, CTEXT: cookie theft extraneous information, NV: conversation non-verbal, CON; conversation interaction; RBDNR: right brain damage, non-right handed, RBDR: right brain damage, right handed, NBD: non-brain damage.
Table 3
Communication assessment performance: between group comparisons
DCT (40) MPT (10) CIMT (12) CTIU CTEFF NV (15)
NBD vs. RBDR *p¼0:010 *p¼0:049 *p¼0:049 p¼0:127 p¼0:069 *p¼0:000
NBD vs. RBDNR p¼0:303 p¼0:112 *p¼0:035 p¼0:060 *p¼0:035 *p¼0:000
RBDNR vs. RBDR p¼1:00 p¼0:797 p¼0:438 p¼0:699 p¼0:797 p¼0:606
*p,0:05:; DCT: Discourse Comprehension Test, MPT: Metaphor Picture Test, CIMT: Comprehension of
4. Discussion
Performance data on measures sensitive to the subtle communication effects associated with RBD have not previously been reported for NRs sustaining right hemisphere stroke. A group, albeit small, of NRs of similar educational background and with communication assessment carried out at the same point in time after stroke (3 months), permitted the examination of some relevant data. Given the small number of RBDNR participants, the reaching of firm conclusions is not warranted but some preliminary observations may be forwarded along with some suggestions for future research.
On all communication measures there was striking similarity between the scores of the
RBD R and NR groups. This is contrary to the findings ofGloning et al. (1969)whose NR
group was significantly more impaired. It should be noted that this older study involved only global judgements using traditional language measures and participants of unspecified lesion type. There may also have been some differences in handedness patterns, in that all of Gloning et al’s NR group had been required to write with the right hand at an early school stage though some had reverted later to left hand writing. Time of assessment may also contribute to the conflicting results. The Gloning et al data were collected in the first week following stroke and it is possible that recovery after this stage contributes to erosion of group differences. The lack of differentiation of R and NR groups
is in accord with recent language data for left brain damage (Basso et al., 1990; Kertesz,
1993; Laska et al., 2001; Naeser & Borod, 1986; Pedersen et al., 1995).
Unlike previous research involving NRs, participants were not recruited on the basis of a demonstrated communication difficulty. The research was not concerned with diagnosis of aphasia, but to evaluate whether Rs and NRs performed similarly in tests associated with RBD impairment. The presence of communication deficit is clear in that while the scores of both stroke groups were remarkably similar, they were impaired in comparison to
Table 4
Individual RBDNR participant scores
RBDNR1 RBDNR2 RBDNR3 RBDNR4 RBDNR5
GNT (30) 13a 16a 15a 21 18a
ASJ (30) 29 26b 26b 30 30
DCT (40) 33 28b 32 32 39
MPT (10) 8 2b 7 7 8
CIMT (12) 7b 4b 6b 6b 10
CTIU 4 6 3b 5 5
CTEFF 5.33 4.67 7.44b 5.20 7.67b
CTEXT 24 28 44.67 26 38.33
NV (15) 12b 11b 14b 12b 12b
CON (25) 22 22 22 25 20b
GNT: Graded naming Test, ASJ: Auditory synonym Judgements, DCT: Discourse Comprehension Test, MPT: Metaphor Picture Test, CIMT: Comprehension of Inferred Meaning Test, CTIU: Cookie theft interpretive units, CTEFF: cookie theft efficiency, CTEXT: cookie theft extraneous information, NV: conversation non-verbal, CON; conversation interaction.
the non-brain damaged group on several measures, relating to spoken discourse and the comprehension of connected speech. Despite the small group sizes, some clear performance differences between the stroke and neurologically normal groups were demonstrated at 3 months after stroke, a stage where stability of communication
performance is expected (Laska et al., 2001; Pedersen et al., 1995; Holland, Greenhouse,
Fromm, & Swindell, 1989).
Low scores on communication tasks may represent a reduction in cognitive processing
ability as distinct from a communication specific impairment (Cherney & Halper, 1996).
Taxing tests of inferential comprehension, where understanding of the presented material requires the listener to deal with information, which is not given explicitly have frequently
been found to be sensitive to RBD (Harden, Cannito, & Dagenais, 1995). Such tests exact
high demands of cognitive processes, such as sustained attention, memory, and reasoning. Both R and NR groups performed less well than the NBD group on CIMT. Recent brain
imaging data on lateralisation of language (Springer et al., 1999; Szaflarski et al., 2002)
and visual perception and memory (Grady, 1996) have revealed a more symmetric pattern
of activation in older than in younger people. These findings have led to the suggestion that cognitive functions may become less lateralised with advancing age, reflecting
compensation for age-related capacity loss (Szaflarski et al., 2002). While similarity of
performance in Rs and NRs does not signify that the groups have comparable processing impairments or patterns of cerebral language organization, reduced lateralisation may be a relevant contributor to the observed similarities of language performance in R and NR patients. Although RDDR and RDDNR groups were not differentiated on any of the measures of comprehension, there were indications of a more extensive comprehension loss in the RBDR group. In addition to the low scores on CIMT, which both RBD groups showed, in both DCT and MPT, the RBDR group scored significantly below the NBD group. Previous investigators using these assessments have similarly reported impairment
for RBDR subjects (Bryan, 1989; Tompkins, Baumgaertner, Lehman, & Fossett, 1997).
More diffuse organization of sentence and paragraph comprehension skills in the NR group may have provided some protection against the effects of RBD, whereas the high cognitive demands of CIMT resulted in impaired performance in both R and NR RBD groups.
Four of the five RBDNR participants experienced difficulty with GNT, the word finding test administered to this group only, when only RBDNR1 was frankly aphasic in the view of the assessing speech and language therapist. The presence of aphasia did not affect participation in the assessments. Low confrontation naming scores are not specifically associated with RBD, although problems with divergent word finding tasks have been
noted (Hough, Pabst, & DeMarco, 1994; Varley, 1995). The low education level of the
description task. Also this task and GNT use visual material and performance may be affected by impairments in visual perception which may be associated with RBD.
In Rs the right hemisphere is regarded as having a specialized role in a variety of higher functions and impairments related to for example attention, praxis, affect, and visuospatial
skills are thought to be typically associated with non-dominant hemisphere lesions (Myers,
1999; Coppens & Hungerford, 2001). It is unknown whether the same applies to NRs with left language lateralisation, whether the left hemisphere fulfils this function if language is lateralised in the right hemisphere or whether both hemispheres contribute should
language be bilaterally represented. Coppens and Hungerford (2001) hypothesise an
independence in the lateralisation of language and visuospatial skills. Alexander and
Annet (1996)report a left handed patient with a left lesion in whom language, praxis, affect, and visuospatial skills appeared to all be lateralised in the right hemisphere. Future research in NRs with RBD should examine communication difficulties in the context of other lateralised functions to inform the relationship between language and other higher functions.
The desirability of viewing communication behaviours within a broader context is also clear when the non-verbal scores of the RBD participants are considered. The NV score, which were based on eye contact, facial expression and intonation during conversation, was the communication measure, which most distinguished the stroke participants, both R and NR, from the NBD group. However, it should be noted that the ratings for eye contact and facial expression were made at the time of assessment so were not subject to the rigorous inter and intra judge reliability monitoring which was applied to the other spoken language measures. Future research might make use of video rather than audio recording or have a second judge in attendance during a representative proportion of data collection. The reason for the presence of the suggested limitations in these non-verbal behaviours cannot be determined from the current study. Although these are pragmatic dimensions which are associated with RBD, motor speech impairment, depression and affective disorder may all have some bearing on the low scores of R and NR RBD stroke patients. Only RBDNR1 was perceived to exhibit some aphasia, which suggests that the right hemisphere played a significant role in language processing in this participant. Although RBDNR1 was the lowest scorer on GNT and despite the aphasia, overall on the communication battery he was certainly not the weakest of the group and in the majority of measures scored around the NBD mean for his age and education grouping This may be because for this participant the left hemisphere subserved the communication role which in right handers is associated with the right hemisphere. The other four NR participants were not regarded as aphasic and it is likely that for them the right hemisphere was less involved in language processing. Further speculation about patterns of language lateralisation in the RBDNR group in this investigation would be inappropriate. Until recently, knowledge about the lateralisation of language processing and the heterogeneity of the NR population was based on brain damaged groups and the results of experimental procedures, such as Wada’s intracarotid sodium amytal test and unilateral electro-convulsive shock. The information becoming available from investigations which employ modern neuroimaging techniques enhances and challenges our knowledge base,
confirming right hemisphere language activity in Rs (Knecht et al., 2000; Springer et al.,
but complete right hemisphere lateralisation is very uncommon. (Pujol, Deus, Losilla, & Capdevila, 1999) The majority of relevant imaging studies have used single word recognition and generation tasks. Future research using imaging techniques will hopefully include a variety of language measures, sampling comprehension and production and also higher level communication tasks which are sensitive to RBD.
In research where handedness may be relevant there is a need for clearly defined groups. Various methods for assessing handedness have been used, including self-report, preference inventories, and task performance. The categorization of people into right and non-right-handed groups masks the continuum of laterality patterns which are present in the population and which have an association with language dominance. Handedness should be defined using multiple measures that assess different aspects of
preference and performance (Corey, Hurley, & Founda, 2001). Familial handedness
may be relevant to language organization (Knecht et al., 2000). None of the NRs in
the current study recalled left handedness in parents. It may be relevant to question regarding other relatives also. However, it must be recognized that the exploration of familial handedndess patterns is problematical especially in cultures such as in the UK where in previous generations many people with left handed tendencies were pressurised to use the right hand and even punished for not doing so at school.
Recent research on language performance of right and NRs have not revealed
differences in neurologically intact adults (Szaflarski et al., 2002) nor in children
(Natsopoulos, Koutselini, Kiosseoglou, & Koundouris, 2002), thus justifying the absence of a non-brain damaged non-right handed group in this study. Nevertheless until knowledge in this area is more complete, future larger scale research involving NRs should consider the inclusion of a NR control group reflecting the distribution in the adult population. It is hoped that this initial report will stimulate interest in communication skills associated with non-dominant hemisphere language processing in the non-right-handed population. The research contributes to the growing body of evidence as to the similarity of presentation of Rs and NRs on communication assessment. Nevertheless, the literature confirms wide variation in performance in language tasks in neurologically normal and in brain damaged people and small groups may not be truly representative of their populations. Only further research will demonstrate whether performance differences which were not apparent in the right brain damaged right handers and NRs in this small investigation are evident when larger groups are studied.
Acknowledgements
References
Alexander, M. P., & Annet, M. (1996). Crossed aphasia and related anomalies of cerebral organization: case reports and a genetic hypothesis.Brain and Language,55, 213– 239.
Bamford, J., Sandercot, P., Dennis, M., Burn, J., & Warlow, C. (1988). A prospective study of acute cerebrovascular disease in the community: the Oxfordshire Community Stroke Project, 1981 – 1986. 1. Methodology, demography and incident cases of first-ever stroke.Journal of Neurology, Neurosurgery and Psychiatry,51, 1373 – 1380.
Basso, A., Farabola, M., Grassi, M. P., Laiacona, M., & Zanobio, M. E. (1990). Comparison of aphasia profiles and language recovery in non-right-handed and matched right-handed patients.Brain and Language,38, 233– 252.
Brookshire, R. H. (1983). Subject description and generality of results in experiments with aphasic adults.
Journal of Speech and Hearing Disorders,48, 342– 346.
Brookshire, R. H., & Nicholas, L. E. (1993).Discourse comprehension test. Tucson: Communication Skill Builders.
Bryan, K. L. (1989).The right hemisphere language battery. Kibworth: Far Communications.
Burns, M. S., Halper, A. S., & Mogil, S. I. (1985).Clinical management of right hemisphere dysfunction. Maryland: Aspen.
Cherney, L. R., & Halper, A. S. (1996). A conceptual framework for the evaluation and treatment of communication problems associated with right hemisphere damage. In A. S. Halper, L. R. Cherney, & M. S. Burns (Eds.),Clinical management of right hemisphere dysfunction(pp. 21 – 30). Maryland: Aspen. Conrad, K. (1949). Uber aphasische sprachstorungen bei hirmverletzten linkshnander.Nervenarzt,20, 148– 154. Coppens, P., & Hungerford, S. (2001). Crossed aphasia: two new cases.Aphasiology,15, 827– 854.
Corey, D. M., Hurley, M. M., & Foundas, A. L. (2001). Right and left handedness defined: a multivariate approach using hand preference and hand performance measures.Neuropsychiatry, Neuropsychology and Behavioral Neurology,14, 144 – 152.
Doody, R. S., Vacca, J. L., Massman, P. J., & Liao, T. Y. (1999). The influence of handedness on the clinical presentation and neuropsychology of Alzheimer disease.Archives of Neurology,56, 1133– 1137. Ellis, S. J., Ellis, P. J., Marshall, E., Windridge, C., & Jones, S. (1998). Is forced dextrality an explanation for the
fall in the prevalence of sinistrality with age? A study in northern England.Journal of Epidemiological Community Health,52, 41 – 44.
Gloning, I., Gloning, K., Haub, G., & Quatember, R. (1969). Comparison of verbal behaviour in right-handed and non right-handed patients with anatomically verified lesion of one hemisphere.Cortex,5, 43 – 52. Goodglass, H., & Kaplan, E. (1983).The Boston diagnostic aphasia examination. Philadelphia: Lea and Febiger. Goodglass, H., & Quadfasel, F. (1954). Language laterality in left-handed aphasics.Brain,77, 521– 548. Grady, C. L. (1996). Age-related changes in cortical blood flow activation during perception and memory.Annals
of New York Academy of Sciences,777, 14 – 21.
Harden, W. D., Cannito, M. P., & Dagenais, P. A. (1995). Inferential abilities of normal and right hemisphere damaged adults.Journal of Communication Disorders,28, 247 – 259.
Holland, A. L., Greenhouse, J. B., Fromm, D., & Swindell, C. S. (1989). Predictors of language restitution following stroke: a multivariate analysis.Journal of Speech and Hearing Research,32, 232 – 238. Hough, M. S., Pabst, M. J., & DeMarco, S. (1994). In M. E. Lemme (Ed.),Categorization skills in right
hemisphere brain damage for common and goal-derived categories(pp. 35 – 51).Clinical aphasiology, Vol. 22, Austin: Pro-Ed.
Joanette, Y., & Anslado, A. I. (1999). Clinical note: acquired pragmatic impairments and aphasia.Brain and Language,68, 529 – 534.
Joanette, Y., & Goulet, P. (1994). In M. L. Lemme (Ed.),Right hemisphere and verbal communication: Conceptual, methodological and clinical issues(pp. 1 – 23).Clinical aphasiology, Vol. 22, Austin: Pro-Ed. Kaplan, E., & Goodglass, H. (1981). Aphasia-related disorders. In M. T. Sarno (Ed.),Sarno Acquired aphasia
(pp. 303– 326). New York: Academic Press.
Kertesz, A. (1993). In M. Paradis (Ed.),Neurophysiological foundations of aphasia rehabilitation(pp. 365– 378).
Foundations of aphasia rehabilitation, Oxford: Pergamon Press.
Knecht, S., Drager, B., Deppe, M., Bobe, L., Lohmann, H., Floel, A., Ringelstein, E. B., & Henningsen, H. (2000). Handedness and hemispheric language dominance in healthy humans.Brain,123, 2512– 2518. Laska, A. C., Hellblom, A., Murray, V., Kahan, T., & Von Arbin, M. (2001). Aphasia in acute stroke and relation
to outcome.Journal of Internal Medicine,249, 413– 422.
Luria, A. R. (1970).Traumatic aphasia: Its syndromes, psychology and treatment. The Hague: Mouton. Mackenzie, C. (2000a). Adult spoken discourse: the influences of age and education.International Journal of
Language and Communication Disorders,35, 269– 285.
Mackenzie, C. (2000b). The relevance of education and age in the assessment of discourse comprehension.
Clinical Linguistics and Phonetics,14, 151– 161.
Mackenzie, C., Begg, T., Lees, K. R., & Brady, M. (1999). The communication effects of right brain damage on the very old and the not so old.Journal of Neurolinguistics,12, 79 – 93.
Marien, P., Paquier, P., Cassenaer, S., & De Deyn, P. P. (2002). The history of crossed aphasia: early development of concepts and hypotheses.Journal of Neurolinguistics,15, 129– 142.
McKenna, P., & Warrington, E. K. (1983).Graded naming test. Windsor: NFER-Nelson. Myers, P. M. (2001). Towards a definition of RD syndrome.Aphasiology,15, 913– 918.
Myers, P. S. (1999).Right hemisphere damage: Disorders of communication and cognition. London: Singular. Myers, P. S. (1979). Profiles of communication deficits in patients with right cerebral hemisphere damage: implications for diagnosis and treatment. In R. H. Brookshire (Ed.), Clinical Aphasiology Conference Proceedings(pp. 38 – 45). Minneapolis: BRK Publishers.
Naeser, M. A., & Borod, J. C. (1986). Aphasia in left-handers: lesions site, lesion side, and hemispheric asymmetries on CT.Neurology,36, 471– 488.
Natsopoulos, D., Koutselini, M., Kiosseoglou, G., & Koundouris, F. (2002). Differences in language performance in variations of lateralization.Brain and Language,82, 223– 240.
Oldfield, R. C. (1971). The assessment and analysis of handedness: the Edinburgh Inventory.Neuropsychologia,
9, 97 – 113.
Pedersen, P. M., Jorgensen, H. S., Nakayama, H., Raaschou, H. O., & Olsen, T. S. (1995). Aphasia in acute stroke: incidence, determinants and recovery.Annals of Neurology,38, 659 – 666.
Pujol, J., Deus, J., Losilla, J. M., & Capdevila, A. (1999). Cerebral lateralization of language in normal left-handed people studied by functional MRI.Neurology,52, 1038– 1043.
Springer, J. A., Binder, J. R., Hammeke, T. A., Swanson, S. J., Frost, J. A., Bellgowan, P. S., Brewer, C. C., Perry, H. M., Morris, G. L., & Mueller, W. M. (1999). Language dominance in neurologically normal and epilepsy subjects: a functional MRI study.Brain,122, 2033 – 2046.
Subirana, A. (1969). Handedness and cerebral dominance. In P. J. Vinken, & G. W. Bruyn (Eds.),Handbook of clinical neurology, disorders of speech, perception and symbolic behavior(pp. 248– 272). Amsterdam: North Holland Publishing Company.
Szaflarski, J. P., Binder, J. R., Possing, E. T., McKiernan, K. A., Ward, B. D., & Hammeke, T. A. (2002). Language lateralisation in left-handed and ambidextrous people: fMRI data.Neurology,59, 238– 244. Tompkins, C. A. (1995).Right hemisphere communication disorders: Theory and management. San Diego:
Singular.
Tompkins, C. A., Baumgaertner, A., Lehman, M. T., & Fossett, T. R. D. (1997). Suppression and discourse comprehension in right brain-damaged adults: a preliminary report.Aphasiology,11, 505 – 519.
Varley, R. (1995). Lexical-semantic deficits following right hemisphere damage: evidence from verbal fluency tasks.European Journal of Disorders of Communication,30, 362– 371.
Weeks, D. J. (1988).The anomalous sentences repetition test. Windsor: NFER-Nelson.
Wertz, R. T. (1993). Efficacy of various methods of therapy. In M. Paradis (Ed.),Foundations of aphasia rehabilitation(pp. 61 – 76). Oxford: Pergamon Press.