Corresponding author: Azkya Patria Nawawi, Department of Dental Public Health, School of Dentistry, University of Jen-deral Achmad Yani, Email: Azkya [email protected]
P-ISSN 1979-0201, e-ISSN 2549-6212 Available from:http://jurnal.unpad.ac.id/pjd/index DOI:
Submission: Sep 2017 Publishing: Nov 2017
Diferences in the oral health behaviour of the 12-years-old
children in rural and urban area of Cimahi
Azkya Patria Nawawi*, Rina Putri Noer Fadilah*, Andi Supriatna*
*Department of Dental Public Health Dental Education Program Faculty of Medicine University of Jenderal Achmad Yani, Indonesia
ABSTRACT
Introduction: Oral diseases have increased signiicantly in the past decade. The Health Service of Cimahi reports showed an increasing number of oral diseases. Behaviour plays an important role in preventing oral disease. The purpose of this study was to examine the diferences in the oral health behaviour of the 12-years-old children in the rural and urban area of the city of Cimahi. Methods: The research type was analytic with the cross-sectional design. The sample was determined using pathinder survey method from oral health surveys basic methods. Data were collected through a questionnaire containing knowledge and attitudes, observations of actions assessed in the checklist, and assessment of the health status of the teeth using the Patient Hygiene Performance Data Index and analyzed using the Mann-Whitney test. Results: The results showed that children in both rural and urban areas have a good knowledge and positive attitude. Both the rural and urban children have the wrong tooth brushing methods and the children in the rural area had a moderate PHP index whilst the child in the urban area had a bad PHP index. There were signiicant diferences in the knowledge (p = 0,017) and PHP index (p < 0.001), and there was no signiicant diference in the attitude (p = 0,312) and action (p = 1,000) in children of both rural and urban areas. Conclusion: Health education on the proper tooth brushing methods and the calculus removal was needed to be done in order to reduce the value of PHP index, especially in children of the urban areas
Keywords: Behaviour, PHP Index, 12-years-old children
INTRODUCTION
The oral disease is still a big problem in Indonesia. Oral diseases also enter into the largest diseases in Indonesia and are ranked 6th out of 10 major diseases. The results of the Indonesia Basic Health
Research reported in 2013 showed that the 10-14 age group had dental and oral health problems of 25.2%.1
carbohydrate fermentation, saliva, host defence, luoride, and oral and dental hygiene. In addition to factors present in the mouth directly related to caries, there are indirect factors called external risk factors that are predisposing factors and inhibiting factors of caries. External factors include gender, level of education, level of economy, environment and behaviour related to dental health.2,3
According to Bahar in 2000, one of the main factors afecting dental hygiene in the developing world is behaviour. Behavior is an important thing that can afect the dental health status of individuals or communities. Eforts to improve dental and oral health require the participation of the community, especially children through knowledge, attitudes, and actions that are a form of behaviour, especially related to oral health such as dental health education through counselling. Dental and oral health behaviours are closely related and afect the improvement of oral hygiene seen through oral hygiene status.3,4
The period of childhood is a period of growth and development. The period of eruption of the tooth begins at the age of 6 months marked by the appearance of deciduous teeth. The complete period of permanent teeth is at 12 years old so this age is considered ideal because it is easy to reach before the children leave school, this is the foundation by WHO to determine the age of 12 years as global caries monitoring indicator and also as an indicator of the development of dental and oral diseases (monitoring of disease trends).5
Report from Health Service of Cimahi stated that the incidence of high caries incidence reached 6992 teeth in 12-year age group this is due to the behaviour of maintaining bad dental and mouth health and mostly occurs in children in rural areas where health facilities there are fewer than urban area 6). The purpose of this study was to examine the diferences in the oral health behaviour of the 12-years-old children in the rural and urban area of the city of Cimahi.
METHODS
The research method used was analytic with cross-sectional study design. The sample in this research is 6th-grade students of SDN 12 years old. The study sample refers to WHO Oral Health Surveys
Basic Methods based on Pathinder surveys. This is a stratiied cluster sampling technique based on a subgroup with diferent levels, examination of a number of standard subjects and includes only speciic age indexes. Groups taken from geographical units (villages, sub-districts, urban-village, districts, etc.)7 Thus, the sample used
is the age group of 12 years with each region in select 1 Region representing Urban and 1 Region representing Rural. From each region selected 2 districts that represent rural and urban areas. From each rural and urban areas selected 1 school In each school selected each of at least 50 children from the urban area and obtained 25 boys and 25 girls Grade 6 Cipageran Cimahi North Primary and 50 children in the rural area with the amount of distribution the same in SDN Utama Cimahi Selatan so the total sample is 100 children.
The inclusion criteria in the study were as follows: (1) Primary school children aged 12 years, (2) Primary school children who have a full eruption of all permanent teeth until the irst molar. The criteria for exclusion in the study were as follows: (1) sick children in the mouth are unable to open their mouths, (2) children who have been given topical luoric applications, (3) 12-years-old primary school children using an orthodontic plate or ixed orthodontics. The behaviours examined include PHP knowledge, attitudes, actions, and indexes. Measurement of knowledge using questionnaire type closed-ended multiple choice questionnaire contains 15 questions where the correct answer is given score 1 and wrong one given score 0. The assessment results are summed and divided by the number of questions and multiplied 100%. Then the inal result is put into good category
(100-76%), enough (56-75%) and less (<55%) (8) Measurement of attitudes using questionnaires with Likert scale, where each answer is given a value for positive statements of value 4 (strongly agree), 3 (agree), 2 (less agree), 1 (disagree) and for negative statements of value 1 (strongly agree) 2 (agree), 3 (less agree), 4 (disagree). The result is added and then calculated the average score. The results of individual values are entered into 2 categories. Positive when the value is greater than the average value. Negative when the value is smaller than the average value.
Measurement of action using the checklist of tooth brushing steps contains 6 steps to brush your teeth. The results are entered into two categories if all actions are correctly entered into the appropriate category, and if any of the actions are not done correctly entered into the category is not appropriate. PHP index measurement is a valuation to examine the indication of oral hygiene. The measurement procedure using a disclosing solution was applied to all teeth and then indexed the irst molar teeth on the right and left, the irst incisor on the right, the right lower left mandible and the left irst left incisive. Inspection using glass where each part of the tooth is divided into 5 divisions ie mesial, middle, distal, cervical, and occlusal parts. Each area is given a score of 1 so that the total score of each section is 5. Results Scores categorized Very good = 0, Good = 0.1-1.7, medium = 1.8-3.4 and bad = 3.5-5.0 9)
All instruments used are irst tested for validity and reliability. The collected data was
then processed and analyzed using the Mann-Whitney test (comparative test of 2 unpaired samples) with a degree of signiicance of p≤ 0.05 to see diferences in the two diferent groups.
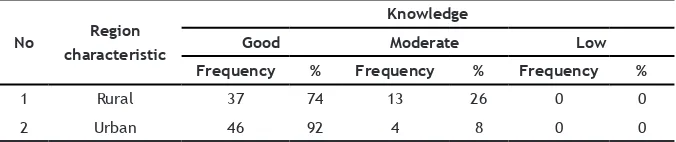
All analysis using SPSS v22.0. This study has obtained ethical approval from Medical Ethics Board of Padjadjaran University with No. Registration: 0815100804. Subjects of previous research have been given informed consent before the research and examination. region selected 2 sub-districts representing rural and urban areas and then selected 2 schools of knowledge in each group are described in Table 1. Based on the results of the study showed that both children in rural and urban areas have a good and adequate category of knowledge. In rural areas, as many as 37 children have good knowledge (74%), while there are 46 children in urban areas with good knowledge (92%). It can be concluded that children in urban areas had better knowledge category than in rural areas. Description of
Table 1. Knowledge of oral health care in both rural and urban groups
No Region
characteristic
Knowledge
Good Moderate Low
Frequency % Frequency % Frequency %
1 Rural 37 74 13 26 0 0
2 Urban 46 92 4 8 0 0
Table 2. Behaviour related to oral health care in both rural and urban groups
behaviour related to the oral health of children in both areas was presented in Table 2 below
The results showed that oral hygiene behaviour in 12-year-old children in rural and urban areas was positive, whereas in rural areas there were 32 children (64%) and urban area there were 27 children (54%). A description of measures in maintaining oral health can be seen in Table 3.
The results showed that oral hygiene behaviour in 12-year-old children in rural and urban areas was positive, whereas in rural areas there were 32 children (64%) and urban area there were 27 children (54%). A description of measures in maintaining oral health can be seen in Table 3
In Table 4 can be seen PHP index of each group. In the rural group, the result of PHP index is in the middle category (56%) while for an urban
area is in a bad category (58%). The results of the
examination conducted in the ield found that in children who live in urban areas have more tartar than in children who live in rural areas. Comparison of dental health behaviours in children in urban and rural groups can be seen in Table 5.
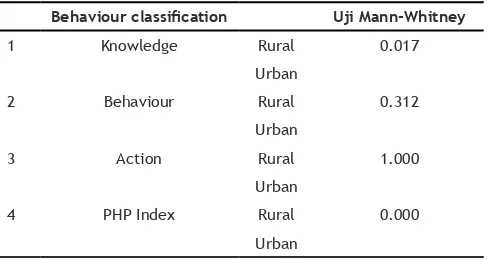
Mann-Whitney test results indicate that there is a signiicant diference between knowledge (p = 0.017) and PHP index (p < 0.001) in children in rural and urban areas. Test results on attitudes (p = 0.312) and action (p = 1,000) showed no signiicant diferences in children in rural and urban areas
Table 4. The PHP Index of oral health care in both rural and urban groups
No Region
Characteristic
PHP Index
Very Good Good Moderate Bad
Frequency % Frequency % Frequency % Frequency %
1 Rural 0 0 14 28 28 56 8 16
2 Urban 0 0 1 2 20 40 29 58
Table 5. The Mann-Whitney test results in both rural and urban groups
Behaviour classiication Uji Mann-Whitney
1 Knowledge Rural 0.017
Urban
2 Behaviour Rural 0.312
Urban
3 Action Rural 1.000
Urban
4 PHP Index Rural 0.000 Urban
DISCUSSION
Health behaviour is the response of an individual related to health problems, the use of health facilities, lifestyle, and the surrounding environment.10 Bloom’s theory shares behaviours
in three domains: knowledge, attitude, and action.4 The results of this study indicate that
there are signiicant diferences in knowledge in rural and urban areas, although both groups are in the good category in rural areas, the percentage is
less than urban (rural 74%, and urban 94%). Sociological studies have shown a high distinction between knowledge, attitude, and action between urban and rural groups.11 Research
in Burnika Faso, Africa shows that children in urban areas have a high level of knowledge about dental health. Higher parental education, more active school teachers, and easy access to information in urban areas that can explain this phenomenon.12
Children in rural and urban areas do not difer signiicantly from the attitude of maintaining healthy teeth in the good category. In urban areas, the percentage is smaller than the rural area (64% rural and urban 54%), which when viewed from the perspective of knowledge is much higher in the urban areas than rural areas.
Attitudes can be changed after the cognitive change.4 The existence of this new
for the formation of maintaining oral health on respondents. The information received carries a suggestive message so that it can be a powerful foundation for judging a thing and forming a certain attitude.
A behaviour is formed by a certain attitude
First the behaviour is not much determined by the general attitude, but by a speciic attitude toward something. Second, the behaviour is inluenced not only by attitudes but also subjective norms that are beliefs about what others want to do.
Third, attitude towards an intention to behave certainly. From the opinion above the possibility of respondents still, have a general attitude and has not created a speciic attitude so that the results of good attitude do not necessarily produce good behaviour.13
Dental hygiene measures did not difer signiicantly in rural children with urban areas. In fact, both are in the category of inappropriate so that it can be concluded both children rural and urban areas are not true in the way of brushing his teeth. Good tooth brushing ability is an important factor for the maintenance of oral health. This is inluenced by the correct frequency and time of brushing, as well as the use factor of dental brushing devices and methods.14
In a study conducted by Nurhidayat, Tunggul, and Wahyono in 2012 showed that the behaviour of people who have not realized the importance of maintaining oral health is still high. This is evident from 22.8% of Indonesians not brushing and from 72.2% brushing only 8.1% who brushing their teeth on time (Eliza Herijulianti et al., 2001)15
The PHP Index (Patient Hygiene Performance Index) is an index used to assess the extent of dental plaque and debris that would indicate oral hygiene. Debris on the PHP index is deined as a soft foreign material consisting of bacterial plaque, alba material and food debris safely attached to the tooth surface softly.9
The PHP index in rural and urban children difers signiicantly, whereas in rural children fall into the moderate category and in urban children fall into the bad category. When viewed in its intra-oral state, in urban children have more tartar than rural children so that debris can be easily attached. The high PHP index score can also be inluenced by the motivation of urban children to visit existing health facilities.16
Food factors also afect oral hygiene, wherein children in urban areas usually eat sweet and sticky food than rural children who can still eat sweet foods from fresh fruit that is high ibrous so indirectly clean the teeth.
CONCLUSION
Health education on the proper tooth brushing methods and the calculus removal was needed to be done in order to reduce the value of PHP index, especially in children of the urban areas.
ACKNOWLEDGEMENT
This research was fully supported by the Center for Research and Community Services of Universitas Jenderal Achmad Yani.
REFERENCES
1. National Institute of Health Research and Development (NIHRD). Indonesia Basic Health Research (RISKESDAS) 2013. Jakarta: Ministry of Health Republic of Indonesia; 2013.
2. Meyer-Lueckel H, Paris S, Ekstrand KR. Caries Management-Science and clinical practice. 1st
ed. Stuttgart: Thieme; 2013.
3. Warni L. Hubungan Perilaku Murid SD Kelas V dan VI Pada Kesehatan Gigi dan Mulut Terhadap Status Karies Gigi di Wilayah Kecamatan Delitua Kabupaten Deli Serdang [thesis]. Medan: USU; 2009.
4. Notoatmodjo S. Pendidikan dan perilaku kesehatan. 1st ed. Jakarta: Rineka Cipta; 2010.
5. Hobdell M, Petersen PE, Clarkson J, Johnson N. Global Goals for Oral Health 2020. Int Dent J. 2003;53(5):285-8.
6. Dinas Kesehatan Pemerintah Kota Cimahi. Laporan Tahunan Program Kesehatan Gigi dan Mulut. Cimahi: Dinkes Pemkot Cimahi; 2016. 7. World Health Organization. Oral Health Survey
- Basic Methods. 5th ed. Geneva: WHO Library
Cataloguing-in-Publication Data; 2013.
8. Arikunto S. Prosedur Penelitian: Suatu Pendekatan Praktik. 6th ed. Jakarta: Rineka
Cipta; 2013.
9. Marya CM. A Textbook of Public Health Dentistry. 3rd ed. New Delhi: Jaypee Brothers
10. Notoadmodjo S. Pendidikan dan Perilaku Kesehatan. Jakarta: Rineka Cipta; 2003.
(already cited in citation number 4).
11. Pine CM, Harris R. Community Oral Health. 2nd
ed. Copenhagen: Quintessence; 2005.
12. Varenne B, Petersen PE, Ouattara S. Oral health behaviour of children and adults in urban an rural areas of Burkina Faso, Africa. Int Dent J. Apr 2006;56(2):61-70.
13. Rahmawati I, Hendrartini J, Priyanto A. Perilaku Kesehatan Gigi dan Mulut pada Anak sekolah dasar. J Comm Med Publ Health. 2011;27(4):180-6.
14. Azwar A. Pengantar Ilmu Kesehatan Lingkungan. 4th ed. Jakarta: Mutiara Sumber
Widya; 1995.
15. Nurhidayat O, Tunggul E, Wahyono B. Perbandingan media power point dengan lip chart dalam meningkatkan pengetahuan kesehatan gigi dan mulut. Unnes Journal Of Public Health. Jul 2012;1(1):31-5. DOI: 10.15294/ujph.v1i1.179.