CONTENTS
Table of contents ………..………. 2
Introduction ………. 3
Curriculum ……… 4
Block Team ………... 6
Facilitators ……… 7
Time Table ……….……… 8
Meeting of Students representatives ……… 17
Meeting of The Facilitators………. 17
Assessment method ………... 17
Student Project ………...………. 18
Learning Program ……….. 20
Curriculum Mapping ………... 75
INTRODUCTION
Due to the application of integrated curriculum at the Faculty of Medicine Udayana University, the discipline-based subjects of the previous curriculum such as Biology, Anatomy, Physiology, Internal Medicine, etc have been integrated and incorporated into several blocks. One of these blocks is Infections and Infectious Diseases. In this block will be explained in general about pathogenesis, pathophysiology, sign, symptoms, clinical features, diagnosis, and management of certain infectious diseases commonly occur in community.
This book aims to give general information for medical students about infections and infectious diseases and important for facilitators and resource person while facilitating or guiding the students in learning process. This study guide consists of general information on learning time table, block team members, facilitators, and the core curriculum including learning outcomes, learning situations, learning tasks and self-evaluation items.
The block Infection and Infectious Diseases has the equivalent of (six) credits. As a block of six credits, the learning processes will be carried out for 38 days starts from September, 1st 2016 as shown in the Time Table. The examination for Basic Microbiology and Parasitology will be conducted on 30th of September 2016, followed by lecture of infection and infectious disease. Examination for infection and infectious disease will be held on 31st of October 2016. Final mark of this block is combination between result of basic and clinical examination. During the 38 days of learning activities, the students will discuss several topics in varied forms of learning situations such as independent learning, small group discussion, lecture, and skill lab.
More than half of the learning material must be learned independently and in small group discussions. A lecture is given only to emphasize crucial things or objectives of material and to prepare the students before discussion. For small group discussion, the students will be given learning tasks to solve and discuss. After discussion, students also have to evaluate their learning progress independently (self assessment).
From this block, we hope every medical student have knowledge and skill to diagnose and manage infections and certain infectious diseases commonly occur in community, as a frontline in community health.
Since the integrated curriculum of the Faculty of Medicine Udayana University is still in progress, this Study Guide will also, naturally, have some revisions in the future. Therefore, we kindly invite readers to give any comments or suggestions for its improvement and development.
CURRICULUM OF THE BLOCK
AIMS
To comprehend the biology of the infectious diseases
To apply and interpret common laboratory diagnosis of infectious diseases To diagnose and manage common infectious diseases
To carry out basic immunization in children
LEARNING OUTCOMES
Comprehend the practical and clinical implications of the biology of infection Apply the general principles of approach to patients with infectious diseases Apply and interpret common laboratory diagnosis of common infectious diseases Apply the basic principles of immunization in children
Diagnose and manage common bacterial infections (common Gram positive and negative, spirochetal)
Diagnose and manage common parasitic infections (common nematode, trematode, cestode, and protozoal infections)
Diagnose and manage common fungal infections
Clinically diagnose and manage common viral infections (caused by common respiratory virus, herpesvirus, arbovirus)
Clinically diagnose and manage Infection in pregnancy (TORCH)
CURRICULUM CONTENT
1. The biology of infection: bacterial, viral, fungal and parasitic.
a. Principles of bacterial infections such as Staphylococci, Streptococci, Neisseria, Salmonella, Vibrio, anaerobic bacteria¸ Leptospira, Mycobacteria, Gram positive bacilli)
b. Principles of viral infections such as respiratory virus (influenza virus, mumps, measles), retrovirus (HIV), herpesvirus (HSV 1, HSV 2, VZV, arbovirus (dengue virus, Japanese B encephalitis virus).
c. Principles of fungal infections such as Candida, Pneumocytis jiroveci, Histoplasma, Cryptococcus
d. Principles of parasitic infections such as Plasmodium, Toxoplasma gondii, Entamoeba histolytica and soil transmitted helminthes.
2. General approach to the patients with infection such as: a. Clinical manifestations (local and systemic infections)
b. Laboratory examination to support diagnosis of infections i.e. Microbiological examination, Parasites examination, Clinical pathology examination, Pathology examination and Imaging examination
3. Management patients with infection such as:
a. Common bacterial infections such as bacterial meningitis, typhoid fever,diarrhea, endocarditis, diphtheria, tetanus, food poisoning, genital gonorrhoeae, non gonococcal urethritis, etc.
b. Common parasitic infections such as malaria, amoebiasis, toxoplasmosis.
d. Common viral infections such as mumps, measles, influenza (especially H5N1), SARS, varicella, herpes labialis, herpes genitalis, dengue fever, Japanese B encephalitis, and HIV.
PLANNERS TEAM
No Name Departement Phone
1 dr. Made Susila Utama, Sp.PD-KPTI Internal Medicine 08123815025 2 dr. Putu Yuliandari, S.Ked Microbiology 089685415625 3 dr NN Dwi Fatmawati, Sp.MK, Ph.D Microbiology 087862200814 4 Dr. dr. Made Sudarmaja, M.Kes Parasitology 08123953945
5 dr. Putu Gede Sudira, Sp.S DME 081805633997
LECTURERS
NO NAME DEPT PHONE
1. Prof. Dr. dr. Tuti Parwati Merati, SpPD, KPTI-FINASIM
Internal Medicine (Tropical Disease)
08123806626
2. Prof.Dr. dr. Raka Sudewi, Sp.S (K) Neurology 0816710244 3.
dr. Made Susila Utama, Sp.PD Internal Medicine (Tropical Disease) 08123815025 4.
dr. Agus Somia, SpPD Internal Medicine (Tropical Disease) 08123989353 5. dr. AA Yuli Gayatri, Sp.PD Internal Medicine
(Tropical Disease)
08123803985
6. dr. Ni Made Dewi Dian Sukmawati,
Sp.PD Internal Medicine (Tropical Disease) 081805656501 7. dr W. Gustawan,M.Sc., Sp.A Pediatri 08123848241 8. dr. Made Bagiada, Sp.PD-KP Pulmonology 08123607874 9. Dr. dr. Wayan Sudhana, SpPD-KGH Internal Medicine
(Nefrology)
08123914095
10.
dr. Ratih Karna, Sp.KK Dermatology &Venerology 081337808844 11.
Dr. dr. IB Fajar Manuaba, SpOG GynecologyObstetric & 081558101719
12. dr. Luh Ariwati Parasitology 08123662311
13. dr. Kadek Swastika, M.Kes Parasitology 08124649002 14. Dr. dr. Made Sudarmaja, M.Kes Parasitology 08123953945 15. dr NN Dwi Fatmawati, Sp.MK, Ph.D Microbiology 087862200814 16. Dr. dr. Sri Budayanti, Sp.MK Microbiology 08583711398 17. Dr. dr. I Dewa Made Sukrama, M.Si,
Sp.MK (K) Microbiology 081338291965
18. dr. Made Agus Hendrayana, M.Ked Microbiology 08123921590 19. I.B. Nyoman Putra Dwija, S.Si,
FACILITATORS
(REGULAR CLASS)
NO NAME GROUP DEPT PHONE VENUE
1 dr. Ni Made Susilawathi, Sp.S 1 Neurology 08124690137 3nd floor: R.3.09 2 dr. Ketut Agus Somia,
Sp.PD-KPTI
2 Internal
Medicine
089617587075 3nd floor: R.3.10 3 dr. Tjok Istri Anom Saturti,
Sp.PD
3 Internal
Medicine
082145854167 3nd floor: R.3.11
4 dr. Putu Sudira, Sp.S 4 DME 081805633997 3nd floor:
R.3.12 5 dr. Agus Roy Rusly HH,
Sp.BE-RE
5 Surgery 081239990399 3nd floor: R.3.13 6 dr. IA Dewi Wiryanthini,
M.Biomed
6 Biochemistry 081239990399 3nd floor: R.3.14 7 dr. IN Gede Wardana, M.
Biomed
7 Anatomy 087860405625 3nd floor: R.3.15 8 Prof. Dr. dr. I Putu Adiatmika,
M.Ked
8 Physiology 08123811019 3nd floor: R.3.16 9 dr. I Wayan Juli Sumadi, Sp.PA 9 Patology
Anatomy
082237407778 3nd floor: R.3.17 10 dr. IA Kusuma Wardani, Sp.KJ,
MARS
10 Psychiatry 08123813831 3nd floor: R.3.19
FACILITATORS
(ENGLISH CLASS)
NO NAME GROU
P
DEPT PHONE VENUE
1 dr. Komang Andi Dwi Saputra, Sp.THT-KL
1 ENT 081338701878 3nd floor:
R.3.09 2 dr. Henky, Sp.F, M.Beth 2 Forensik 08123988486 3nd floor:
R.3.10 3 dr. I Wayan Niryana, Sp.BS,
M.Kes
3 Surgery 08179201958 3nd floor: R.3.11 4 dr. Ni Nyoman Metriani Nesa,
Sp.A, M.Sc
4 Pediatry 081337072141 3nd floor: R.3.12 5 Dr. dr. BK Satriyasa, M.Repro 5 Pharmacology 087777790064 3nd floor:
R.3.13 6 Dr. dr. GN Indraguna P 6 IKK IKP 08123816424 3nd floor:
R.3.14 7 dr. Made Satria Yudha
Dewangga, SpJP
7 Cardiology 081805057315/ 082163500096
3nd floor: R.3.15 8 dr. I Wayan Sugiritama, M.Kes 8 Histology 08164732743 3nd floor:
R.3.16 9 dr. Tjahya Aryasa EM, Sp.An 9 Anesthesiology 081339713553 3nd floor:
R.3.17 10 Desak Ernawati, S.Si
PGPharm, M.Pharm,Ph.D
TIME-TABLE
(Block Basic Microbiology, Parasitology, Infection and infectious
Diseases)
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class English Class 1 Thursday Sept 1st 2016
08.00-08.30 09.00-09.30 Lecture 1
Introduction of block Basic Infection and Infectious Diseases
Introduction of
the Block Class room Prof. Dr. dr. TutiParwati Merati, SpPD, KPTI
08.30-09.00 09.30-10.00 Lecture 2
General Parasitology Dr. dr. Made Sudarmaja, M.Kes
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-14.30 15.00-15.30 Plenary
Session Class room Prof. Dr. dr. Tuti Parwati Merati, SpPD, KPTI
14.30-15.00 15.30-16.00 Plenary
Session Class room Dr. dr. Made Sudarmaja, M.Kes
2 Friday, Sept 2nd
2016
08.00-08.30 09.00-09.30 Lecture 3 Introduction of Microbiology
Lecture Class room Dr. dr. I Dewa Made Sukrama, M.Si, Sp.MK
08.30-09.00 09.30-10.00 Lecture 4 Patogenesis of bacterial infection
Lecture Class room dr. Made Agus Hendrayana, M.Ked
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small Group
Discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-14.30 15.00-15.30 Plenary Class Room Dr. dr. I Dewa Made Sukrama, M.Si, Sp.MK 14.30-15.00 15.30-16.00 Plenary Class Room dr. Agus
Hendrayana, M.Ked
3 Monday, Sept 5th 2016
08.00-08.30 09.00-09.30 Lecture 5
Diagnosis of Malaria Lecture Class Room Dr. dr. Made Sudarmaja, M.Kes
08.30-09.00 09.30-10.00 Lecture 6
Diagnosis of Filariasis Lecture Class room Dr. dr. Made Sudarmaja, M.Kes
09.00-10.30 12.00-13.30 Individual Learning 10.30-12.00 13.30-15.00 Small group
discussion
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class
English Class
12.30-14.00 10.00-11.30 Individual learning
14.00-15.00 15.00-16.00 Plenary Class room Dr. dr. Made Sudarmaja, M.Kes
4 Friday Sept 9th 2016
08.00-09.00 09.00-10.00 Lecture 7,8,9 Toxoplasmosis, amoebiasis, and systemic fungal infection
Lecture Class Room dr. Luh Ariwati
09.00-10.30 12.00-13.30 Individual Learning 10.30-12.00 13.30-15.00 Small group
discussion
Disc. Room Facilitator
12.30-14.00 10.00-11.30 Individual learning
14.00-15.00 15.00-16.00 Plenary Class room dr. Luh Ariwati
5 Tuesday, Sept 13th
2016
08.00-09.00 09.00-10.00 Lecture 10, 11 Ascariasis, Trichuriasis
Lecture Class room dr. Luh Ariwati
09.00-10.30 12.00-13.30 Individual
learning
-10.30-12.00 13.30-15.00 Small group discussion
Disc. Room Facilitator
12.30-14.00 10.00-11.30 Individual learning
14.00-15.00 15.00-16.00 Plenary
Session Class room dr. Luh Ariwati
6 Wednesday,
Sept 14th
2016
08.00-09.00 09.00-10.00 Lecture 12,13,14 Hookworm infection, Strongyloidiasis, Enterobiasis
Lecture Class room Dr. dr. Made Sudarmaja, M.Kes
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-15.00 15.00-16.00 Plenary
Session
Class room Dr. dr. Made Sudarmaja, M.Kes
7 Thursday
Sept 15th
2016
08.00-09.00 09.00-10.00 Lecture 15,16 Larva migrans, Pediculosis
Individual
learning dr. Kadek Swastika, M.Kes
09.00-10.30 13.30-15.00 Small group
discussion Disc. Room Facilitator 10.30-12.00 10.00-11.30 Individual
learning
12.30-14.00 15.00-16.00 Plenary
Session
Class room dr. Kadek Swastika, M.Kes
8 Monday, Sept 19th
2016
08.00-09.00 09.00-10.00 Lecture 17,18,19 Schistosomiasi, Taeniasis, Sistisercosis
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class
English Class
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion
Disc. Room Facilitator
12.30-14.00 10.00-11.30 Individual learning
14.00-15.00 15.00-16.00 Plenary
Session Class room dr. Kadek Swastika, M.Kes
9 Tuesday Sept 20th
2016
08.00-16.00 08.00-16.00 STUDENT PROJECT (REGULER CLASS) Teather Room Evaluator & Fasilitator 10 Tuesday Sept 21st
2016
08.00-08.30 09.00-09.30 Lecture 20, 21 Gram positive and negative bacteria
Lecture Class room dr. Made Agus Hendrayana, M.Ked
08.30-09.00 09.30-10.00 Lecture 22: Mycobacterium
Lecture Class room IB Nyoman Putra Dwija, S.Si, M.Biotech
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-14.30 15.00-15.30 Plenary
Session Class room dr. Made Agus Hendrayana, M.Ked
14.30-15.00 15.30-16.00 Plenary
Session Class room IB Nyoman Putra Dwija, S.Si, M.Biotech
11 Thursday,
Sept 22nd
2016
08.00-09.00 09.00-10.00 Lecture 23, 24
Pathogenesis of viral infection,
DNA virus
Lecture Class room Dr. dr. Ni Nyoman Sri Budayanti, Sp.MK
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-15.00 15.00-16.00 Plenary Class room Dr. dr. Ni Nyoman Sri Budayanti, Sp.MK
12 Friday, Sept 23rd
2016
08.00-09.00 09.00-10.00 Lecture 25, 26 RNA virus, Zoonosis
Lecture Class room Dr. dr. Ni Nyoman Sri Budayanti, Sp.MK
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class
English Class
14.00-15.00 15.00-16.00 Plenary Class room Dr. dr. Ni Nyoman Sri Budayanti, Sp.MK
13 Monday, Sept 26th
2016
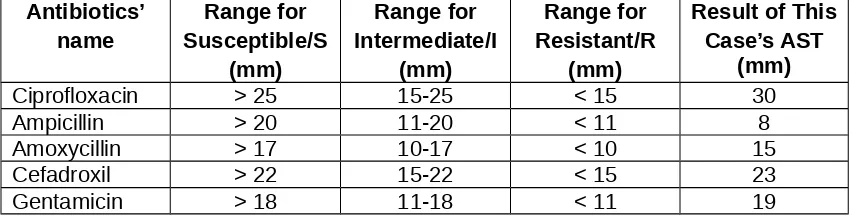
08.00-09.00 09.00-10.00 Lecture 27, 28 Specimen collection Microbial
identification & Antimicrobial
Sensitivity Test (AST)
Lecture Class room dr. Ni Nengah Dwi Fatmawati, Sp.MK, Ph.D
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 MIDDLE BLOCK MEETING
14.00-15.00 15.00-16.00 Plenary dr. Ni Nengah Dwi
Fatmawati, Sp.MK, Ph.D
14 Tuesday, Sept 27th
2016
08.00-08.30 09.00-09.30 Lecture 29
Mechanism of action and resistance of antibiotic
Lecture Class room dr. Ni Nengah Dwi Fatmawati, Sp.MK, Ph.D
08.30-09.00 09.30-10.00 Lecture 30 Biosafety & Biosecurity
Lecture Class room IB Nyoman Putra Dwija, S.Si, M.Biotech
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-14.30 15.00-15.30 Plenary Class room dr. Ni Nengah Dwi Fatmawati, Sp.MK, Ph.D
14.30-15.00 15.30-16.00 Plenary Class room IB Nyoman Putra Dwija, S.Si, M.Biotech
15 Wednesday,
Sept 28th
2016
08.00-09.00 09.30-10.00 Lecture 31, 32 Health
care-associated infection Anaerob bacteria & Spirochaeta
Lecture Class room Dr. dr. I Dewa Made Sukrama, M.Si, Sp.MK
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class
English Class
14.00-15.00 15.00-16.00 Plenary Class room Dr. dr. I Dewa Made Sukrama, M.Si, Sp.MK
Thursday, Sept 29th
2016
SILENT DAY
Friday, Sept 30th
2016
BASIC MICROBIOLOGY & PARASITOLOGY EXAMINATION
16 Monday, Oct 3rd 2016
08.00-09.00 09.00-10.00 Lecture 33
Host response to infection
(viral, bacterial, fungal, parasite)
Lecture Class room Prof. Dr. dr. Tuti Parwati Merati, SpPD, KPTI
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion
Disc. Room Facilitator
12.30-14.00 10.00-11.30 Individual learning
14.00-15.00 15.00-16.00 Plenary Class room Prof. Dr. dr. Tuti Parwati Merati, SpPD, KPTI
17 Tuesday, Oct 4th 2016
08.00-09.00 09.00-10.00 Lecture 34, 35, 36 Hematology &
Immunology infection (dengue fever, dengue hemorrhagic fever, dengue shock syndrome)
Lecture Class room dr Dewi Dian Sukmawati, SpPD
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-15.00 15.00-16.00 Plenary Class room dr Dewi Dian Sukmawati, SpPD
18 Wednesday,
Oct 5th 2016
08.00-16.00 08.00-16.00 STUDENT PROJECT (ENGLISH CLASS)
Teather room Evaluator & Fasilitator
19 Thursday, Oct 6th 2016
08.00-09.00 09.30-10.00 Lecture 37 Infection in
pregnancy (TORCH in pregnancy)
Lecture Class room DR Dr IB Fajar Manuaba, SpOG
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class
English Class
12.30-14.00 10.00-11.30 Individual learning
14.00-15.00 15.00-16.00 Plenary Class room DR Dr IB Fajar Manuaba, SpOG
20 Friday, Oct 7th 2016
08.00-08.30 09.00-09.30 Lecture 38 Malaria
Lecture Class room dr Susila Utama, SpPD-KPTI 08.30-09.00 09.30-10.00 Lecture 39
Leptospirosis Lecture Class room dr Agus Somia, SpPD-KPTI 09.00-10.30 12.00-13.30 Individual
learning 10.30-12.00 13.30-15.00 Small group
discussion
Disc. Room Facilitator
12.30-14.00 10.00-11.30 Individual learning
14.00-14.30 15.00-15.30 Plenary Class room dr Susila Utama, SpPD-KPTI 14.30-15.00 15.30-16.00 Plenary Class room dr Agus Somia,
SpPD-KPTI
21 Monday, Oct 10th 2016
08.00-09.00 09.00-10,00 Lecture 40
Skin infection Lecture Class room dr Ratih Karna, SpKK 09.00-10.30 12.00-13.30 Individual
learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-15.00 15.00-16.00 Plenary Class room dr Ratih Karna, SpKK
22 Tuesday,
Oct 11st 2016
08.00-09.00 09.30-10.00 Lecture 41 Central nervous system infection (meningitis, encephalitis)
Lecture Class room Prof DR Dr Raka Sudewi, SpS(K)
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-15.00 15.00-16.00 Plenary Class room Prof DR Dr Raka Sudewi, SpS(K)
23 Wednesday,
Oct 12nd
2016
08.00-09.00 09.00-10.00 Lecture 42
Child Immunization Lecture Class room dr W. Gustawan,SpA 09.00-10.30 12.00-13.30 Individual
learning
Class room
10.30-12.00 13.30-15.00 Small group
discussion Facilitator 12.30-14.00 10.00-11.30 Individual
learning
14.00-15.00 15.00-16.00 Plenary
Session
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class English Class 24 Thursday, Oct 13rd 2016
08.00-08.30 09.00-10.00 Lecture 43
Thypoid fever Lecture Class room dr Agus Somia, SpPD-KPTI 08.30-09.00 09.30-10.00 Lecture 44
Acute gastroenteritis Lecture Class room dr Yuli Gayatri, SpPD 09.00-10.30 12.00-13.30 Individual
learning 10.30-12.00 13.30-15.00 Small group
discussion
Disc. Room Facilitator
12.30-14.00 10.00-11.30 Individual learning
14.00-14.30 15.00-15.30 Plenary
Session
Class room dr Agus Somia, SpPD-KPTI
14.30-15.00 15.30-16.00 Plenary
Session Class room dr Yuli Gayatri, SpPD
25 Friday, Oct 14th 2016
08.00-08.30 09.00-09.30 Lecture 45
Urinary Tract Infection (acute pyelonephritis, lower urinary tract infection)
Lecture Class room DR Dr Wayan Sudhana, SPPD-KGH
08.30-09.00 09.30-10.00 Lecture 46
Lower respiratory tract infection (pneumonia, acute bronchitis)
Lecture Class room dr. Made Bagiada, SpPD-KP
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion
Disc. Room Facilitaor
12.30-14.00 10.00-11.30 Individual learning
14.00-14.30 15.00-15.30 Plenary
Session Class room DR Dr Wayan Sudhana, SPPD-KGH
14.00-14.30 15.00-15.30 Plenary
Session
Class room dr. Made Bagiada, SpPD-KP
26 Monday, Oct 17th 2016
08.00-08.30 09.00-09.30 Lecture 47 Toxoplasmosis
Lecture Class room dr Yuli Gayatri, SpPD
08.30-09.00 09.30-10.00 Lecture 48
Filariasis Lecture Class room dr Dewi Dian Sukmawati, SpPD
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitaor 12.30-14.00 10.00-11.30 Individual
learning
14.00-14.30 15.00-15.30 Plenary
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class
English Class
14.30-15.00 15.30-16.00 Plenary
Session Class room dr Dewi Dian Sukmawati, SpPD
27 Tuesday, Oct 18th 2016
08.00-09.00 09.00-10.00 Lecture 49 HIV infection (pathogenesis & opportunistic infection)
Lecture Class room Prof DR Dr Tuti Parwati, SpPD-KPTI
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitaor 12.30-14.00 10.00-11.30 Individual
learning
14.00-15.00 15.00-16.00 Plenary
Session Class room Prof DR Dr Tuti Parwati, SpPD-KPTI
28 Wednesday Oct 19th 2016
08.00-09.00 09.00-10.00 Lecture 50, 51
Avian influenza, SARS
Lecture Class room dr Agus Somia, SpPD-KPTI
09.00-10.30 12.00-13.30 Individual learning 10.30-12.00 13.30-15.00 Small group
discussion
Disc. Room Facilitaor
12.30-14.00 10.00-11.30 Individual learning
14.00-15.00 15.00-16.00 Plenary
Session
Class room dr Agus Somia, SpPD-KPTI
29 Thursday, Oct 20th 2016
08.00-08.30 09.00-09.30 Lecture 52
Parotitis Lecture Class room dr Dewi Dian Sukmawati, SpPD
08.30-09.00 09.30-10.00 Lecture 53
Bacteremia, Sepsis Lecture Class room dr Susila Utama,SpPD-KPTI
09.00-10.30 12.00-13.30 Individual learning
10.30-12.00 13.30-15.00 Small group
discussion Disc. Room Facilitaor
12.30-14.00 10.00-11.30 Individual learning
14.00-14.30 15.00-15.30 Plenary
Session
Class room dr Dewi Dian Sukmawati, SpPD
14.30-15.00 15.30-16.00 Plenary
Session Class room dr Susila Utama,SpPD-KPTI
30 Friday,
08.00-08.30 09.00-09.30 Lecture 54 Rabies
DAY/ DATE Time Topic Learning
situation Place PIC
Regular Class
English Class
Oct 21st 2016 08.00-09.00 09.30-10.00 Lecture 55
Tetanus Lecture Class room dr Yuli Gayatri, SpPD
09.00-10.30 12.00-13.30 Individual learning
10.30-12.00 13.30-15.00 Small group discussion
Disc. Room Facilitaor
12.30-14.00 10.00-11.30 Individual learning
14.00-14.30 15.00-15.30 Plenary
Session Class room dr Susila Utama,SpPD-KPTI
14.30-15.00 15.30-16.00 Plenary
Session
Class room dr Yuli Gayatri, SpPD
31 Monday, Oct 24th 2016
08.00-15.00 09.00-16.00 Laboratory Practice 1:
Gram Stain Laboratory Microbiology Team
32 Tuesday, Oct 25th 2016
08.00-15.00 09.00-16.00 Laboratory Practice 2:
ZN stain Laboratory Microbiology Team
33 Wednesday, Oct 26th 2016
08.00-15.00 09.00-16.00 Laboratory Practice 3:
Fecal examination Parasitology Team
34 Thursday, Oct 27th 2016
08.00-15.00 09.00-16.00 Laboratory Practice 4: Parasit identification
Parasitology Team
Friday,
Oct 28th 2016 SILENT DAY
Monday,
Oct 31st 2016
INFECTION & INFECTIOUS DISEASES EXAMINATION
In the middle of block period, a meeting is designed among the student representatives of every small group discussion, facilitators and source person of the block. The meeting discuss about the ongoing teaching and learning process, quality of facilitator and lectures as a feedback to improve the next process.
MEETING OF THE FACILITATORS
All facilitators are invited to discuss all block activities with block contributors 1 week after meeting of student representatives.
ASSESSMENT METHOD
1. Assessment will be held twice, for basic microbiology & parasitology and infection & infectious diseases. Final mark is combination beteween this mark. The time provision is 100 minutes. The number of MCQ is 100 with passing point 70.
2. Assessment in this block consists of:
SGD : 5%
STUDENT PROJECT
Regulation:
TITLE Name: NIM:
Faculty of Medicine, Udayana University 2016
1. Introduction (Pendahuluan)
2. Content (Isi sesuai dengan judul paper) 3. Summary (Ringkasan)
4. References (Daftar pustaka): Vancouver style 5. Pages: 6-10, Spasi: 1.5, Time New Roman:12
TOPIC Regular Class (Class A)
GROUP DATE & TIME TITLE PEMBIMBING/
FASILITATOR
EVALUATOR
1 Tuesday, Sept 20th 2016, 08.30-09.00
Cerebral abses dr. Ni Made Susilawathi, Sp.S
Prof DR Dr Raka Sudewi, SpS(K)
2 09.00-09.30 Cerebral toxoplasmosis
dr. Ketut Agus Somia, Sp.PD-KPTI
3 09.30-10.00 Multi drug resisten (MDR) TB
dr. Tjok Istri Anom Saturti, Sp.PD
dr. Made Bagiada, SpPD-KP
4 10.00-10.30 Spondilitis TB dr. Putu Sudira, Sp.S 5 10.30-11.00 Acute infection
pancreatitis
dr. Agus Roy Rusly HH, Sp.BE-RE
dr. Agus Somia, SpPD-KPTI 6 11.00-11.30 Pes dr. IA Dewi Wiryanthini,
M.Biomed 11.30-12.30 BREAK
7 12.30-13.00 Leishmaniasis dr. IN Gede Wardana, M. Biomed
Dr. dr. Made Sudarmaja, M.Kes 8 13.00-13.30 Tripanosomiasis Prof. Dr. dr. I Putu
Adiatmika, M.Ked 9 13.30-14.00 Cytomegalovirus
infection
dr. I Wayan Juli Sumadi, Sp.PA
dr. NN Dwi Fatmawati, Sp.MK, Ph.D 10 14.00-14.30 Squamous cell
carcinoma (associated with HPV infection)
TOPIC English Class (Class B)
GROUP DATE & TIME TITLE PEMBIMBING/
FASILITATOR
EVALUATOR
1 Wednesday, Oct
5th 2016, 08.30-09.00
Nasopharyngeal carcinoma (associated with EBV infection)
dr. Komang Andi Dwi Saputra, Sp.THT-KL
dr. Made Agus Hendrayana, M.Ked
2 09.00-09.30 Hairy leukoplakia (associated with EBV infection)
dr. Henky, Sp.F, M.Beth
3 09.30-10.00 Korioretinitis dr. I Wayan Niryana, Sp.BS, M.Kes
dr. Kadek Swastika, M.Kes 4 10.00-10.30 Carcinoma servik
(associated with HPV infection)
dr. Ni Nyoman Metriani Nesa, Sp.A, M.Sc 5 10.30-11.00 Penyakit jantung
rematik
Dr. dr. BK
Satriyasa, M.Repro
dr W. Gustawan, SpA
6 11.00-11.30 Endoftalmitis Dr. dr. GN Indraguna P 11.30-12.30 BREAK
7 12.30-13.00 Hepatitis C dr. IA Rangga W, Sp.JP, FIHA, M.Biomed
dr. Ni Made Dewi Dian Sukmawati, Sp.PD 8 13.00-13.30 Abses payudara dr. I Wayan
Sugiritama, M.Kes 9 13.30-14.00 Epididimitis dr. Tjahya Aryasa
EM, Sp.An
dr. Ratih Karna, SpKK 10 14.00-14.30 Herpes genital tipe 2 Desak Ernawati,
LEARNING PROGRAM
LECTURE 1
INTRODUCTION OF BLOCK BASIC INFECTION AND INFECTIOUS DISEASES
Prof. Dr. dr. Tuti Parwati Merati, SpPD, KPTI
Abstract
Infections and infectious diseases are a great burden on many societies, including Indonesia. To reduce that burden an integrated approach is required, combining health promotion, disease prevention and patient treatment. The prerequisite for success in this fight is the participation of all health care professionals. Should know and understand terminology commonly use in the context of infectious disease.
Infectious diseases are disorders or diseases caused by organisms — such as bacteria, viruses, fungi or parasites. Many organisms live in and on our bodies. They're normally harmless or even helpful, which we called them normal flora; but under certain conditions, some organisms may cause disease. This organisms called as pathogen as they can produced pathology to the body.
Infectious diseases are one of the leading causes of death worldwide. Infectious diseases can be spread directly or indirectly . Some infectious diseases can be passed from person to person. Some are transmitted by bites from insects or animals. And others are acquired by ingesting contaminated food or water or being exposed to organisms in the environment. Many infectious diseases become difficult to control if the infectious agents evolve resistance to commonly used drugs: For example, bacteria can accumulate mutations in their DNA or acquire new genes that allow them to survive contact with antibiotic drugs that would normally kill them.
Signs and symptoms vary depending on the organism causing the infection, but often include fever and fatigue. Mild infections may respond to rest and home remedies, while some life-threatening infections may require hospitalization.
Many infectious diseases, such as measles and chickenpox, can be prevented by vaccines but many other still do not have vaccine available. Other prevention mean such as frequent and thorough hand-washing helps protect from most infectious diseases.
Symptoms
Each infectious disease has its own specific signs and symptoms. General signs and symptoms common to a number of infectious diseases include: fever, fatigue, muscle aches, coughing and diarrhea
Transmission: an infection can be spread through direct and indirect contact Direct contact
An easy way to catch most infectious diseases is by coming in contact with a person or animal who has the infection. Three ways infectious diseases can be spread through direct contact are:
fluids from sexual contact. The person who passes the germ may have no symptoms of the disease, but may simply be a carrier.
Animal to person. Being bitten or scratched by an infected animal — even a pet — can make you sick and, in extreme circumstances, can be fatal. Handling animal waste can be hazardous, too. For example, you can acquire a toxoplasmosis infection by scooping your cat's litter box.
Mother to unborn baby. A pregnant woman may pass germs that cause infectious diseases to her unborn baby. Some germs can pass through the placenta. Germs in the vagina can be transmitted to the baby during birth.
Indirect contact
Touching : Disease-causing organisms also can be passed by indirect contact. Many germs can linger on an inanimate object, such as a tabletop, doorknob or faucet handle. When you touch a doorknob handled by someone ill with the flu or a cold, for example, you can pick up the germs he or she left behind. If you then touch your eyes, mouth or nose before washing your hands, you may become infected.
Vectors/insect bites - Some germs rely on insect carriers — such as mosquitoes, fleas, lice or ticks — to move from host to host. These carriers are known as vectors. Mosquitoes can carry the malaria parasite or West Nile virus, and deer ticks may carry the bacterium that causes Lyme disease.
Food/water contamination : disease-causing germs can infect you is through contaminated food and water. This mechanism of transmission allows germs to be spread to many people through a single source. E. coli, for example, is a bacterium present in or on certain foods — such as undercooked hamburger or unpasteurized fruit juice.
Risk factors
Anyone can catch infectious diseases easier than other people because the body immune system is not work well. This may occur if there are primary or secondary immune deficiency , such as : Taking steroids or other medications that suppress immune system, such as anti-rejection drugs for a transplanted organ, certain types of cancer or other disorders that affect the immune system, infection by HIV or AIDS. In addition, certain other medical conditions may predispose you to infection, including implanted medical devices, malnutrition and extremes of age, among others.
Complications
Most infectious diseases have only minor complications. But some infections — such as pneumonia, AIDS and meningitis — can become life-threatening. A few types of infections have been linked to a long-term increased risk of cancer: hepatitis B and C have been linked to liver cancer, human papillomavirus is linked to cervical cancer, Helicobacter pylori is linked to stomach cancer and peptic ulcers and In addition, some infectious diseases may become silent, only to appear again in the future — sometimes even decades later. For example, someone who's had a chickenpox infection may develop shingles much later in life.
Diagnosis
Diagnosis can be made with clinical symptoms and signs. Because many of infectious disease have a very similar symptoms and signs, usually laboratory or imaging test would be needed to confirmed the diagnosis
Many infectious diseases have similar signs and symptoms. Samples of body fluids can sometimes reveal evidence of the particular microbe that's causing illness. Samples can get from blood, urine, throat swabs, stool sample, spinal tap (lumbar puncture). A technician obtains a sample with a standard procedure from each.
Imaging scans
Imaging procedures — such as X-rays, computerized tomography and magnetic resonance imaging — can help pinpoint diagnoses and rule out other conditions that may be causing the symptoms.
Biopsies
During a biopsy, a tiny sample of tissue is taken from an internal organ for testing. For example, a biopsy of lung tissue can be checked for a variety of fungi that can cause a type of pneumonia.
Treatment
Knowing what type of germ is causing the illness makes it easier to choose appropriate treatment such as : antibiotics, anti viral, anti fungal, and anti-parasitics.
However, the use of those agents should be use appropriately. The overuse of antibiotics has resulted in several types of bacteria developing resistance to one or more varieties of antibiotics. This makes these bacteria much more difficult to treat
As an alternative medicine, a number of products have been purported to help fend off common illnesses, such as the cold or flu. Cranberry, echinacea, garlic, ginseng, vitamin C, D and zinc are among other.. While some of these substances have appeared promising in early trials, follow-up studies may have had negative or inconclusive results. More research needs to be done.
Prevention
Infectious diseases can be prevented by vaccines but many other still do not have vaccine available. Prevention to infectious disease transmission with no vaccine available should use another approach. Personal protected equipment such as gown, masker, google, gloves, and shoes boot. Infectious disease transmitted by vectors should avoid to being bitten by mosquitoes or other insects may be useful, such as wearing long sleeve shirt, and putting mosquitos repellent. Other prevention means such as frequent and thorough hand-washing helps protect from most infectious diseases.
Learning tasks:
How do we know that a patient in our hospital is suffering from a kind of infectious disease? How he or she can get it?
What prevention do we need to do to avoid of getting any infectious diseases?
Self assessment:
Describe all common terminology use in the context of infectious diseases. Describe general clinical manifestation of infectious diseases.
LECTURE 2
GENERAL PARASITOLOGY
Dr. dr. Made Sudarmaja, M. Kes
Abstract
Parasitology: The study of PARASITES and their relationships to their HOSTS. Parasite : A living organism which receives nourishment and shelter from another organism where it lives. Host : An organism which harbours the parasites. Parasite depend on its location of infection divided into ectoparasites and endoparasites. Some term of parasites : facultative parasites, obligate parasites, incidental parasites, temporary parasites, permanent parasites, pathogen parasites and pseudoparasite. Host divided into definitive host and intermediate host. The study of Parasitology consist several aspect such as : epidemiology, habitat, morphology, life cycle, pathogenic effect, sign & symptom, diagnosis & laboratory diagnosis, treatment and prophylaxis. In The Indonesian Standard Competency of Doctor (SKDI = Standar Kompetensi Dokter Indonesia) shown that several diseases that caused by parasites must be competence by general practioner such as : Malaria, Filariasis, Toxoplasmosis, mikosis, Hookworm infection, Amoebiasis, Ascariasis, Trichuriasis, Enterobiasis, Strongyloidiasis, Schistosomiasis, Taeniasis, Scabies, Pediculosis capitis and Pthiriasis pubis
Learning task:
1. Explain differentiation between Hospes definitive and Hospes intermediate and give example hospes definitive and hospes intermediate!
2. Mention and explain the infective stage of several parasites that caused diseases in human
3. The preventive and control the parasites disesase must be based on life cycle of parasites. Why?
Self-Assessment
1. Amoebic dysentri caused by: A. Ascaris lumbricoides B. Necator americanus C. Trichuris trichiura D. Brugia malayi
E. Entamoeba histolytica
2. Tapeworm that transmitted with pork A. Taenia saginata
B. Taenia solium C. Hymenolepis nana D. Hymenolepis diminuta
3. Nematode that include of soil transmitted helminthes: A. Enterobius vermicularis
B. Taenia saginata C. Trichinella spiralis D. Brugia malayi E. Trichuris trichiura
LECTURE 3
ABSTRACT
The discipline of bacteriology evolved from the need of physicians to test and apply the germ theory of disease and from economic concerns relating to the spoilage of foods and wine. The initial advances in pathogenic bacteriology were derived from the identification and characterization of bacteria associated with specific diseases. During this period, great emphasis was placed on applying Koch's postulates to test proposed cause-and-effect relationships between bacteria and specific diseases. Today, most bacterial diseases of humans and their etiologic agents have been identified, although important variants continue to evolve and sometimes emerge, e.g., Legionnaire's Disease, tuberculosis and toxic shock syndrome.
Major advances in bacteriology over the last century resulted in the development of many effective vaccines (e.g., pneumococcal polysaccharide vaccine, diphtheria toxoid, and tetanus toxoid) as well as of other vaccines (e.g., cholera, typhoid, and plague vaccines) that are less effective or have side effects. Another major advance was the discovery of antibiotics. These antimicrobial substances have not eradicated bacterial diseases, but they are powerful therapeutic tools. Their efficacy is reduced by the emergence of antibiotic resistant bacteria (now an important medical management problem) In reality, improvements in sanitation and water purification have a greater effect on the incidence of bacterial infections in a community than does the availability of antibiotics or bacterial vaccines. Nevertheless, many and serious bacterial diseases remain.
LEARNING TASK:
Define and apply major taxonomic group when classifying microorganisms (bacteria, fungi, parasites, and viruses)
Relate microbial cell structure and processes to growth, disease, survival, or other relevant phenotypes.
Be able to describe the principle of Koch’s postulate.
LECTURE 4
PATHOGENESIS OF BACTERIAL INFECTION
dr. Made Agus Hendrayana, M. Ked
ABSTRACT
The pathogenesis of bacterial infection includes initiation of the infectious process and the mechanisms that lead to the development of signs and symptoms of disease. The biochemical, structural, and genetic factors that play important roles in bacterial pathogenesis are introduced in this chapter and may be revisited in the organism-specific sections. Characteristics of bacteria that are pathogens include transmissibility, adherence to host cells, persistence, invasion of host cells and tissues, toxigenicity, and the ability to evade or survive the host's immune system. Resistance to antimicrobials and disinfectants can also contribute to virulence, or an organism's capacity to cause disease. Many infections caused by bacteria that are com-monly considered to be pathogens are inapparent or asymptomatic. Disease occurs if the bacteria or immunologic reactions to their presence cause sufficient harm to the person.
Learning Task Case:
A 15 years old female, a student at Junior High School, come to general practician complained that she has fever since 6 days. The fever is intermitten, commonly arise when aftenoon till night, but back to normal in the morning. She feels slightly discomfort at the abdominal. She also complained that not defecated since 4 days. Other physical examination results are normal. The practician ask for laboratory examination and culture. After few days, the laboratory analysis shown that she has typoid fever. The culture shown colonies of Salmonella typhi bacteria and significant as agent of infection.
What are Salmonella typhi’s virulence factors that can cause infection? Explain the microbial virulence factors that you know!
What are Salmonella typhi ’s virulence factors that can cause infection?
Explain the pathogenesis how Salmonella typhi can infect the human (from transmission until infection and cause the disease)!
Whether the virulence factors of each microbial is the same? Why? When any bacteriacalled as colonization bacteria?
Explain the differentiation between true pathogen and opportunistic pathogen! Explain the differentiation between exotoxins and endotoxin !
Describe how several pathogens are able to survive inside the macrophages ! Explain the routes of transmission that you know and give examples of each ! Explain why are important to know about the bacteria virulence factors
Self Assessment
Explain the meaning of this term above: Contamination
A. Colonization B. Invasion C. Infection D. Pathogen E. Carrier
F. Nonpathogenic
G. Opportunistic pathogen H. Pathogenicity:
L. Commensalism M. Parasitism N. Zoonoses
Give examples of attachment mechanism !
Reff :
Jawetz, Melnick, Adelberg. 2013 Chapter 9. Pathogenesis of Bacterial Infection in Medical Microbiology, 26th Edition by Vishal . The McGraw-Hill Companies. Lange Microbiology.
LECTURE 5
DIAGNOSIS OF MALARIA
Dr. dr. Made Sudarmaja, M.Kes
Abstract
Malaria remains a global health problem and also in Indonesia and can cause death, especially in high-risk such as infants, toddlers and pregnant women. Malaria Diagnosis is made by anamnesis, physical examination and laboratory tests. To get a definite diagnosis of malaria should be performed laboratory tests to find the malaria parasite in the blood. Examination and detection of the parasite causing-malaria in blood can be done by: a microscopic examination (blood smear), Rapid Diagnostic Test (RDT) and examination by PCR.
Blood smear using microscopic examination is the gold standard for the diagnosis of malaria. Examination of blood smear can be developed thick and thin blood smear. Examination of blood smear aims to found the Plasmodium (malaria parasite), plasmodium determine species and stage and parasite density. Examination using RDT aims to detect the presence of malaria parasite antigens using immunochromatography. PCR can only be done in health facilities that have the equipment for inspection biomoleculer.
Learning task
1. How to distinguish species of malaria by peripheral blood smear examination?
LECTURE 6
DIAGNOSIS OF FILARIASIS
Dr. dr. Made Sudarmaja, M.Kes
Abstract
Learning task
1. How to differentiated species caused filariasis in the examination of blood smears?
Self Assessment
1. Sexual reproduction of P vivax take place in: A. Human gut
B. Red blood cells C. Mosquito D. Liver cell
E. Human Leucocyts
2. The species of plasmodium is characterized by cressent shaped gametocytes and multiple ring forms whitin RBC:
A. P vivax B. P falciparum C. P ovale D. P malariae E. P knowlesi
3. The dormant parasite forms found in patient with vivax malaria are called: A. Thropozoites
B. Sporozoites C. Hypnozoites D. Gametocytes E. Merozoites
4. Sheated microfilaria, described as having two discrete nuclei in the tip of a pointed tail
A. W bancrofti B. B malayi C. Loa loa
D. Onchocerca volvulus
LECTURE 7, 8
TOXOPLASMOSIS & AMOEBIASIS
dr. Luh Ariwati
Entamoeba histolytica is a protozoan parasite responsible for a disease called amoebiasis. It occurs usually in the large intestine and causes internal inflammation as its name suggests (histo = tissue, lytic = destroying). Protozoa are unicellular organisms that have trophozoite form with one or more nuclei containing nucleoli or karyosome and bounded by a nuclear membrane and the usual eukaryotic cytoplasmic organelles including mitochondria ribosomes and endoplasmic reticulum. Trophozoite have a cell membrane but not cell wall. Most intestinal Protozoa also develop cyst that are more resistant than the fragile trophozoite to drying, cold or other environmental stresses.
Trophozoites can be identified under a microscope from biopsy samples taken during colonoscopy or surgery.
Toxoplasmosis well known as parasitic disease and have great impact due to their worldwide distribution. Toxoplasma is caused by a coccidian parasite, Toxoplasma gondii. It has a worldwide distribution and shows a broad host range from warm blooded animals to birds and reptiles. Man acquires the infection indirectly by ingesting oocysts from contaminated environments, by consuming Toxoplasma cysts from tissues of other intermediate hosts such as cow, goat, chicken, duck, rabbit, by blood transfusion or transplantation, or directly by transplacental infection
Human infection is generally asimptomatic and self limited except in immunocompromised host, infection can disseminated and fatal. The prevalence of antibody to toxoplasma in human and animal ranged from 2% to 75% in Southeast Asian Countries. Cats are the definitive host of T. gondii; they are the only animals that pass oocysts in their feces.
Learning Tasks
A previously healthy 28-year old man, who had recently returned from a trip to Lombok, was seen by his family physician for crampy abdominal pain, malaise, slight fever and bloody, mucoid diarrhea. Liquid stool specimens were collected and submitted for culture for enteric bacterial pathogens as well as parasites. Stool cultures were negative for bacterial pathogens, examination for ova and parasites was positive for motile trophozoites in the saline wet amount, and ameboid trophozoites with finely granular cytoplasm and ingested red blood cells in the permanent trichrome stain.
Describe the life cycle of parasites above ! Explain the pathogenesis of parasite above! Describe infective stages ofparasite above!
Describe the life cycle of Toxoplasma gondii
Explain transmission of Toxoplasma gondii infection Explain why toxoplasma infection became latency
LECTURE 9
SYSTEMIC FUNGAL INFECTION
dr. Luh Ariwati
Systemic Fungal infections have become increasingly frequent especially in immune compromised host such as AIDS, cancer patients, organ transplantation , and also as a consequent of the availability of advanced medical technology which allow to do more invasive treatment using more invasive instruments. The aetiology are : Predominant fungi : Candida (C): such as C. Albicans, C. glabrata, C. tropicalis and C.parapsilopsis, Aspergillus spp.and Cryptococcus spp., Emerging fungi : Fusarium spp., and Rhizopus spp. and Endemic fungi : Histoplasma capsulatum, Blastomyces dermatitidis and Coccidioides immitis
There is no specific sign and symptoms of systemic fungal infection. That is why suspected clinical diagnosis of systemic fungal infection is frequently late. Its resemble bacterial infections, such as severe sepsis, septic shock and multi organ failure. Alertness to this infection will comes late though sign and symptoms appear early. In many cases the diagnosis was done per exlusionem. Diagnosis should be considered in patient with risk factors has the signs of systemic infection despite adequate antibiotics.
Learning Tasks:
Describe the cause and the risk factors of Systemic Fungal Infection Describe the Laboratory diagnosis of candidiasis
Describe the morphologic different between Candida and Cryptococcus sp in direct microscopic examination
LECTURE 10, 11
ASCARIASIS
&
TRICHURIASIS
dr. Luh Ariwati
Infections with soil-transmitted helminths (STHs: Ascaris, Trichuris, Hookworm and Strongiloides), which are intestinal worms transmitted through contaminated soil, are the most common infections worldwide. Globally, more than 1 billion people are infected with one or more STHs, mainly in areas with warm and moist climates where sanitation and hygiene are poor. Infection with STH contributes to anemia, vitamin A deficiency, malnutrition and impaired growth, delayed development, and intestinal blockages.
Ascariasis is a Soil-transmitted helminthiasis (STH) infection caused by the roundworm Ascaris lumbricoides (A. lumbricoides). Ascariasis, one of the most common STH infections, affects an estimated 1 billion people worldwide. About half of the populations in tropical and subtropical areas are infected with this parasite, which causes an estimated 20,000 deaths each year. While mild cases of ascariasis often show no symptoms, heavy infections can cause intestinal blockage and impair growth in children. Ascariasis infection is highly prevalent and geographically widespread. Many factors, including the large number of eggs produced by a female worm, the properties of the eggs, environmental conditions, and poor socioeconomic settings facilitate the spread of the parasite and thus determine the geographic distribution of the disease.
Whipworm (Trichuris trichiura) is the third most common roundworm found in humans. The name "whipworm" refers to the shape of the worm; the worms look like whips with wider "handles" at the posterior end. Globally, nearly 800 million people are infected with whipworms, which are highly prevalent in children. Heavy infections could lead to short-term symptoms such as diarrhea and anemia and longer-short-term symptoms such as growth retardation and impaired cognitive development. Coinfection of whipworm with Giardia, Entamoeba histolytica, Ascaris lumbricoides, and hookworm is common.
Whipworm infection, known as trichuriasis, is prevalent in both temperate and tropical zones of the world. However, infections follow a clustered distribution and are more frequently found in areas with tropical weather and poor sanitation practices. Whipworm infection occurs through ingestion of whipworm eggs, which can be found in fecally contaminated dry goods, such as beans, rice, and various grains, and in crops grown in soil fertilized with sewage. Humans are infected when such produce is consumed raw or food is contaminated by handlers.
Learning Tasks:
Differentiate the morphological characteristics of A.lumbricoides and T. trichiura Describe their life cycles and identify each of their infective stages
Describe their pathogenesis and clinical manifestations
Identify their stages of development which are useful from the viewpoint of diagnosis purpose and try to figure their morphological characteristics
Define their epidemiological standpoints and list the factors that are closely related to the transmission of the infections
Manage appropriately the diagnosis, treatment, and prevention measures.
LECTURE 12, 13, 14
HOOKWORM INFECTION, STRONGYLOIDIASIS AND ENTEROBIASIS
Dr. dr. Made Sudarmaja, M.Kes
Abstract
Hookworm infection is an infection by a parasitic blood sucking roundworm Ancylostoma duodenale and Necator americanus. Hookworm infection is a soil-transmitted helminthiasis and therefore classified as a neglected tropical diseases.These worms live in the small intestine of human. Hookworm infection affects more than half a billion people in the world. In developing countries, hookworm infection is rarely fatal, but anemia can be significant in a heavily infected individual. Ancylostomiasis is the disease caused when Ancylostomaduodenale hookworms, present in large numbers, produce an iron deficiency anemia by sucking blood from the host's intestinal walls.Diagnosis of Ancylostomiasis and Necatoriasisdepends on finding characteristic worm eggs on microscopic examination of the stools
and stool tests. The drug Ivermectin is widely used in the treatment of strongyloidiasis. Other drugs that are effective are albendazole and thiabendazole (25 mg/kg twice daily for 5 days—400 mg maximum (generally)).
Enterobiasis is an infection caused by Enterobiusvermicularis. Enterobiusvermicularis (Oxyurisvermicularis) also called human pinworm habits in caecum or in large intestinal. Adult females has lenght 8 to 13 mm, adult male: 2 to 5 mm. The infective stage of this worm is embryonated egg. The infection will be occurs through 3 routes:
Self-infection occurs by transferring infective eggs to the mouth with hands that have scratched the perianal area
Person-to-person transmission can also occur through handling of contaminated clothes or bed linens. Enterobiasis may also be acquired through surfaces in the environment that are contaminated with pinworm eggs (e.g. , curtains, carpeting). Some small number of eggs may become airborne and inhaled. These would be swallowed and follow the same development as ingested eggs. Following ingestion of infective eggs, the larvae hatch in the small intestine
Retroinfection, or the migration of newly hatched larvae from the anal skin back into the rectum, may occur but the frequency with which this happens is unknown.
Diagnostic: found specific egg using perianal swab (under microscope examination)
Learning task:
1. Please explain the life cycle of Hookworm, Strongyloides stercoralis and Enterobius vermicularis!
2. Describe the prevention based on the life cucle from hookworm infections, strongyloidiasis and enterobiasis!
3. Explain symptoms and sign of hookworm infections, strongyloidiasis and enterobiasis!
Self Assessment:
1. The “scoth tape test” is used to diagnose infection with: A. Ancylostoma duodenale
B. Strongyloides stercoralis C. Necator americanus D. Enterobius vermicularis
2. The parasite is capable of autoinfection with may leadto hyperinfection syndrome: A. Ancylostoma duodenale
B. Strongyloides stercoralis C. Necator americanus D. Enterobius vermicularis
3. The eggs of this helmiths is planoconvex and contain tad pole like larva: A. Ancylostoma duodenale
B. Strongyloides stercoralis C. Necator americanus D. Enterobius vermicularis
LECTURE 15, 16
Abstract
Cutaneous larva migrans caused by the larvae of animal hookworms. Humans normally become infected with the hookworm larvae by walking barefoot on a beach, or by contact with soil that is contaminated with animal faeces Cutaneous larva migrans is most commonly found in tropical and subtropical geographic areas and the southwestern United States. It has become an endemic in the Caribbean, Central America, South America, Southeast Asia, and Africa. However, the ease and the increasing incidence of foreign travel by the world's population have no longer confined cutaneous larva migrans to these areas. Cutaneous larva migrans is caused by the larvae of animal hookworms, of which Ancylostoma braziliense is the species most frequently found in humans [2, 3]. These hookworms generally live in the intestines of domestic pets such as dogs and cats and shed their eggs via feces to soil (usually sandy areas of beaches or under houses). Humans are infected in tropical and subtropical areas of endemicity by contact with contaminated soil. The hookworm larva burrows through intact skin but remains confined to the upper dermis, since humans are incidental hostsCreeping eruption usually appears 1–5 days after skin penetration, but the incubation period may be ≥1 month. Typically, a serpiginous, erythematous track appears in the skin and is associated with intense itchiness and mild swelling. Usual locations are the foot and buttocks, although any skin surface coming in contact with contaminated soil can be affected.
Pediculosis is an infestation of the hairy parts of the body or clothing with the eggs, larvae or adults of lice. Lice infestation remains a major problem throughout the world, making the diagnosis and treatment of louse infestation a common task in general medical practice. Lice on human comprice three types, namely the body louse (Pediculus humanus), the head louse (Pediculus capitis) and the pubic louse (Pthirus pubis). Head, body and pubic lice are blood-sucking ectoparasites that are species of Anoplura. They are usually transmitted directly, by person-to-person contact, but they may also be transmitted indirectly, via the clothing, towelling and bedding of infested persons. Infestations occur throughout the world, particularly where there is overcrowding. Poor hygiene tends to increase the incidence of body lice infestations.
Learning task 1
A 10-year-old girl accompany by her family come to the health center complaining of itchy head. Itching is already being felt since one month ago. Patients living in the dorms, some of the children who lived there also had the same complaint. On physical examination was found in scalp hair looks dull and contain white objects.
What is the etiology of that case? Describe the life cycle that species!
Describe the mode of transmission of that case!
How to manage that case? Please explain the treatment and prevention.
Learning task 2
A man 30 years old came to the clinic with complaints of redness track appears in the skin of left foot since 3 days ago. These symptom associated with intense itchiness and mild swelling. Last week he went to beach and walking around without slippers. On local examination found erythematous track on left foot.
What is the diagnosis of that case?
What are the possibility agents cause that case? Describe the mode of transmission of that case
How to manage that case? Please explain the treatment and prevention
LECTURE 17, 18, 19
SCHISTOSOMIASIS, TAENIASIS, SISTISERKOSIS
dr. Kadek Swastika, M.Kes
Abstract
Schistosomiasis is an acute and chronic disease caused by parasitic worms. Schistosomiasis is caused by digenetic blood trematodes. The three main species infecting humans are Schistosoma haematobium, S. japonicum, and S. mansoni. Estimates show that at least 258 million people required preventive treatment in 2014. Preventive treatment, which should be repeated over a number of years, will reduce and prevent morbidity. Transmission occurs when people suffering from schistosomiasis contaminate freshwater sources with their excreta containing parasite eggs which hatch in water. People become infected when larval forms of the parasite – released by freshwater snails – penetrate the skin during contact with infested water. In the body, the larvae develop into adult schistosomes. Adult worms live in the blood vessels where the females release eggs. Some of the eggs are passed out of the body in the faeces or urine to continue the parasite’s life-cycle. Others become trapped in body tissues, causing immune reactions and progressive damage to organs. Schistosomiasis is diagnosed through the detection of parasite eggs in stool or urine specimens. Antibodies and/or antigens detected in blood or urine samples are also indications of infection. The WHO strategy for schistosomiasis control focuses on reducing disease through periodic, targeted treatment with praziquantel through the large-scale treatment (preventive chemotherapy) of affected populations.
human Taenia are recognized : Taenia solium, Taenia saginata and Taenia asiatica. All three spesies are important public health problems in endemic areas as foodborne zoonoses. The beef tapeworm occurs wherever people eat cured or undercooked beef infected with taenia saginata, and the pork tapeworm occurs wherever people eat cured or undercooked pork infected with taenia solium.Cysticercosis is caused by the larval stage of tapeworm Taenia solium. Taenia solium is endemic in all area of world where pigs are raised under conditions in which they have access to human fecal material. Highly endemic area of Taeniasis/Cysticercosis are in Latin America, Eastern Europe, sub-Saharan Africa, India, also recognized in Indonesia, Southeast Asia, China, Korea. In Indonesia there are three endemic provinces for taeniasis/cysticercosis : Bali, Papua and North Sumatra. Others provinces also reported this cases such as East Nusa Tenggara, Lampung, North Sulawesi, Southeast Sulawesi, and West Kalimantan.
Learning Task
A man 47 years old came to Primary Health care with the complained discomfort on his stomach since one month ago and sometimes accompanied with diarrhea, No fever. He is a Balinese and work as a social worker. Physical examination found temperature 37,1 ° C, Blood pressure 120/80 mmHg. Stool examination found an oval egg size 35 µm, with radially striated brown sell and six hooked onchospere
What other information you need to complete the diagnosis? What is the possibility diagnosis and how to manage this patient What is additional examination you need to know the species?
On gravid proglotids found 11 uterine branch, Please Describe the life cycle of this species!
What is possibility complication caused by this spesies? And how it can be occur?
LECTURE 20, 21
GRAM POSITIVE AND NEGATIVE BACTERIA
dr. Made Agus Hendrayana, M. Ked
ABSTRACT
Danish scientist Hans Christian Gram devised a method to differentiate two types of bacteria based on the structural differences in their cell walls. In his test, bacteria that retain the crystal violet dye do so because of a thick layer of peptidoglycan and are called Gram-positive bacteria. In contrast, Gram-negative bacteria do not retain the violet dye and are colored red or pink. Compared with Gram-positive bacteria, Gram-negative bacteria are more resistant against antibodies because of their impenetrable cell wall. These bacteria have a wide variety of applications ranging from medical treatment to industrial use
many Gram-positive bacteria are non-pathogenic. Not only do gram-negative bacteria tend to be harmful to humans, they are also more resistant to antibiotics.
LEARNING TASK Case:
A 25 years old male, collage student, come to clinic complained that there are infected wound on his right foot. The wound is ooze yeloow pus. The wound obtained a week ago due to fall while playing soccer. Four days ago he went to the doctor and been given some medicine but is not getting better.
After physical examination, the doctor ask for laboratory examination as Gram staining for the pus. After few minttes, the Gram staining result sight at the microscope is visible colonies of blue bacteria, spherical shape and clusters like grapes fruit.
1. What bacteria that visible at the microscope for this case?
2. Explain the differences in the characteristics of gram-negative and gram-positive bacteria !
3. Explain why each bacteria produce different colors in Gram staining !
4. Identify each five (5) examples of Gram Positive and Gram Negative Bacteria ! 5. Describe the structure of Gram-negative bacteria cell wall !
6. . Describe the structure of Gram-positif bacteria cell wall !
7. Explain the benefits of knowing the classification of bacteria based on the results of gram staining !
Self Assessment:
Explain the steps of Gram staining !
Reff :
Jawetz, Melnick, Adelberg. 2013 Chapter 3. Classification of Bacteria in Medical Microbiology, 26th Edition by Vishal . The McGraw-Hill Companies. Lange Microbiology.
LECTURE 22
MYCOBACTERIUM
IB Nyoman Putra Dwija, S.Si, M. Biotech
ABSTRACT
Genus of Mycobacterium consist of many species that potentially pathogen such as Mycobacterium complex (M.tuberculosis, M.bovis, M.africanum), M.leprae and M.ulcerans. All the member of the genus has the similar properties Which is thin, slightly curved or straight rod-shaped (0.2-0.4 X 2 – 10 µm), non motile, grow slowly, aerobe, non sporoforming, non motile and pigment of the colony are varies from non pigmented to pigmented.
once the bacteria stained, it’s dificult to decolorization even with acidified alcohol (3% HCL), and so called Acid fast bacilli. HIV Pandemic and emerging of MDR/XDR-TB is another problem that treathed a human health.
Another member of genus of Mycobacterium is Mycobacterium leprae,the etiologic agent of Leprosy (Hansen diseases). Majority of the cases found in South and Southeast Asia, Africa and Latin America,with number of cases average 600.000-700.000 annualy. Leprosy is a chronic, granulomatous and delibitating diseases. General manifestation is anasthetic skin lesion and peripheral neuropathy with tickening of the nerve. Bacilli can be found from few (Tuberculoid leprosy) to massive number of bacteria (Lepromatous leprosy). Since the bacteria is dificult tu culture, diagnosis is based on finding of the diseases sign with suporte