DOI: 10.1542/peds.2009-0430
2009;124;e793-e802; originally published online Sep 14, 2009;
Pediatrics
M. Grummer-Strawn
Melissa Bartick, Alison Stuebe, Katherine R. Shealy, Marsha Walker and Laurence
Hospital
Closing the Quality Gap: Promoting Evidence-Based Breastfeeding Care in the
http://www.pediatrics.org/cgi/content/full/124/4/e793
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Closing the Quality Gap: Promoting Evidence-Based
Breastfeeding Care in the Hospital
abstract
Evidence shows that hospital-based practices affect breastfeeding du-ration and exclusivity throughout the first year of life. However, a 2007 CDC survey of US maternity facilities documented poor adherence with evidence-based practice. Of a possible score of 100 points, the average hospital scored only 63 with great regional disparities. Inappropriate provision and promotion of infant formula were common, despite evi-dence that such practices reduce breastfeeding success. Twenty-four percent of facilities reported regularly giving non– breast milk supple-ments to more than half of all healthy, full-term infants. Metrics avail-able for measuring quality of breastfeeding care, range from compre-hensive Baby-Friendly Hospital Certification to compliance with individual steps such as the rate of in-hospital exclusive breastfeeding. Other approaches to improving quality of breastfeeding care include (1) education of hospital decision-makers (eg, through publications, seminars, professional organization statements, benchmark reports to hospitals, and national grassroots campaigns), (2) recognition of excellence, such as through Baby-Friendly hospital designation, (3) oversight by accrediting organizations such as the Joint Commission or state hospital authorities, (4) public reporting of indicators of the quality of breastfeeding care, (5) pay-for-performance incentives, in which Medicaid or other third-party payers provide additional financial compensation to individual hospitals that meet certain quality stan-dards, and (6) regional collaboratives, in which staff from different hospitals work together to learn from each other and meet quality improvement goals at their home institutions. Such efforts, as well as strong central leadership, could affect both initiation and duration of breastfeeding, with substantial, lasting benefits for maternal and child health.Pediatrics2009;124:e793–e802
Breastfeeding significantly predicts health outcomes for both mothers and children. In 2007, the Agency for Healthcare Research and Quality published a summary of systematic reviews and meta-analyses on breastfeeding and health outcomes in developed countries and deter-mined that early cessation of breastfeeding increases infants’ risks for childhood obesity, gastroenteritis, necrotizing enterocolitis, leukemia, otitis media, severe lower respiratory infections, sudden infant death syndrome, and types 1 and 2 diabetes. Early cessation of breastfeeding is linked with higher rates of maternal disease: breast and ovarian cancers, type 2 diabetes, and postpartum depression.1Infants who are
not breastfed incur up to $475 more health costs in the first year compared with those who are exclusively breastfed for 3 months2
($671 in 2008 dollars3). Because many effects of breastfeeding are
dose-AUTHORS:Melissa Bartick, MD, MSc,a,bAlison Stuebe, MD, MSc,cKatherine R. Shealy, MPH, IBCLC, RLC,dMarsha Walker, RN, IBCLC,eand Laurence M. Grummer-Strawn, PhDd
bDepartment of Medicine, Harvard Medical School, Boston,
Massachusetts;aDepartment of Medicine, Cambridge Health
Alliance, Cambridge, Massachusetts;cDepartment of Obstetrics
and Gynecology, Division of Maternal and Fetal Medicine, University of North Carolina School of Medicine, Chapel Hill, North Carolina;dDivision of Nutrition, Physical Activity, and
Obesity, Centers for Disease Control and Prevention, Atlanta, Georgia; andeNational Alliance for Breastfeeding Advocacy,
Weston, Massachusetts
KEY WORDS
breastfeeding, hospitals, maternity, health care quality, quality indicators, quality improvement, health care, infant, newborn
ABBREVIATIONS
CDC—Centers for Disease Control and Prevention BFHI—Baby-Friendly Hospital Initiative
AAP—American Academy of Pediatrics WHO—World Health Organization UNICEF—United Nations Children’s Fund P4P—pay for performance
mPINC—Maternity Practices in Infant Feeding and Care NQF—National Quality Forum
AAFP—American Academy of Family Physicians HEDIS—Health Plan Employer Data and Information Set
The findings and conclusions in this report are those of the authors and do not necessarily represent views of the Centers for Disease Control and Prevention.
www.pediatrics.org/cgi/doi/10.1542/peds.2009-0430
doi:10.1542/peds.2009-0430
Accepted for publication May 29, 2009
Address correspondence to Melissa Bartick, MD, MSc, Harvard Medical School, Cambridge Health Alliance, 1493 Cambridge St, Cambridge, MA 02139. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e793
. Provided by Indonesia:AAP Sponsored on July 17, 2010
www.pediatrics.org
dependent, increasing breastfeeding du-ration can have a substantial impact on public health.
Evidence shows that hospital practices affect breastfeeding duration and ex-clusivity throughout the first year of life,4–7yet quality of breastfeeding care
in the United States is poor. In a 2007 Centers for Disease Control and Pre-vention (CDC) survey of ⬎80% of US maternity facilities, the mean score for implementation of evidence-based breastfeeding care was 63 of 100 pos-sible points.8 The 10 evidence-based
steps of the Baby-Friendly Hospital Ini-tiative (BFHI) are known to increase duration and exclusivity of breastfeed-ing when implemented, yet fewer than 3% of US hospitals are designated as such.9In some countries, all hospitals
are Baby-Friendly, and these countries have strong government support, cen-tralized leadership, and support from the medical profession.10The paucity
of US Baby-Friendly hospitals reflects an endemic problem throughout American health care: there is a signif-icant gap between evidence-based rec-ommendations and actual practice, as detailed in the Institute of Medicine’s 2001 report, Crossing the Quality Chasm.11Closing this quality gap will
empower mothers to meet breastfeed-ing recommendations.
All major medical organizations, in-cluding the American Academy of Pedi-atrics (AAP) and the World Health Organization (WHO), recommend 6 months of exclusive breastfeeding and continued breastfeeding with appro-priate complementary foods for at least the first 1 to 2 years12–14;
how-ever, only ⬃12% of US infants are breastfed exclusively for 6 months, and only⬃21% are breastfed for 12 months.15Rates of any and exclusive
breastfeeding drop precipitously in the first 2 weeks of life despite fami-lies’ frequent contact with the health care system.
The WHO/United Nations Children’s Fund (UNICEF) Global Strategy for In-fant and Young Child Feeding and the American Public Health Association urge immediate steps to improve breastfeeding rates.14,16The American
Public Health Association notes the wide gap in the United States between evidence-based care recommenda-tions and current typical care. In this article, we review data on quality of breastfeeding care in US hospitals, and we outline approaches to speed-ing adoption of best practices. We used a PubMed search from January 1997 through April 2009 to identify English-language research done using the term “breastfeed*” with the following search terms: quality improvement, quality management, performance in-centives, and pay for performance (P4P).
THE QUALITY GAP
Created in 1991, the BFHI is currently the gold standard for evidence-based breastfeeding care in hospitals (Table 1). Data continue to accumulate show-ing that adherence to the Ten Steps predicts breastfeeding duration and exclusivity, long after hospital dis-charge.4–7,17–19 Breastfeeding within
the first hour of life, exclusive breast-feeding in the hospital, and having a written breastfeeding policy are the steps generally found to have a the greatest influence on success.4,18,20,21
The more steps that are practiced, the higher duration and exclusivity of breastfeeding at 2 months.4,6
DiGiro-lamo et al20showed that breastfeeding
women who did not experience any of the Ten Steps were 8 times more likely to fail at breastfeeding by 6 weeks compared with those who experienced at least 6 of the steps. Individual steps also affect outcomes. For example, 1 hospital-based intervention to reduce formula supplementation of breastfed newborns found that breastfeeding at 6 months increased to 87%, versus 66% beforehand.22
Despite strong evidence for the Ten Steps, hospital compliance in the United States is poor. The 2007 CDC survey Maternity Practices in Infant Feeding and Care (mPINC)8 sought to
survey all US maternity units, with standardized questions based on their implementation of the evidence-based steps described in the BFHI. The CDC survey addressed these issues from the Ten Steps: (1) breastfeeding within the first hour of life, (2) breastfeeding on demand, (3) showing mothers how to breastfeed, (4) prenatal education, (5) absence of pacifiers, (6) rooming in day and night, (7) absence of formula supplementation without a medical indication, (8) training of staff, (9) breastfeeding support at discharge, and (10) having a written breastfeed-ing policy that is conveyed to all staff.
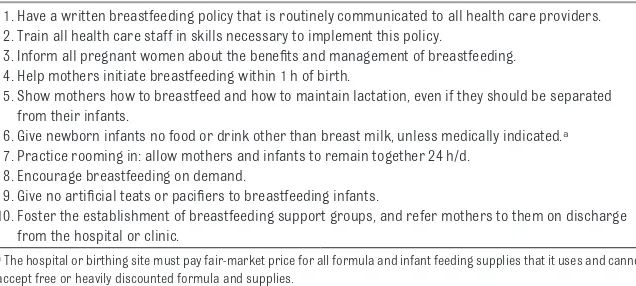
TABLE 1 WHO/UNICEF Ten Steps to Successful Breastfeeding
1. Have a written breastfeeding policy that is routinely communicated to all health care providers. 2. Train all health care staff in skills necessary to implement this policy.
3. Inform all pregnant women about the benefits and management of breastfeeding. 4. Help mothers initiate breastfeeding within 1 h of birth.
5. Show mothers how to breastfeed and how to maintain lactation, even if they should be separated from their infants.
6. Give newborn infants no food or drink other than breast milk, unless medically indicated.a 7. Practice rooming in: allow mothers and infants to remain together 24 h/d.
8. Encourage breastfeeding on demand.
9. Give no artificial teats or pacifiers to breastfeeding infants.
10. Foster the establishment of breastfeeding support groups, and refer mothers to them on discharge from the hospital or clinic.
aThe hospital or birthing site must pay fair-market price for all formula and infant feeding supplies that it uses and cannot
On the basis of a standard script, 1 re-spondent from each maternity center answered the survey. To encourage candid responses, respondents were assured that their data would not be publicly reported. Instead, each facility was given a report comparing its re-sults with benchmarks for other hos-pitals of similar size nationally and with other hospitals in the same state. Of a possible score of 100 points, the average hospital scored only 63, with the mean total scores ranging from 48 (Arkansas) to 81 (New Hampshire and Vermont). Great regional disparities were found, with the southern states performing worse than the northeast-ern and westnortheast-ern regions. Although 88% of facilities reported that they taught most mothers techniques of breastfeeding, practices that are known to be detrimental to breastfeed-ing were common. For example, 65% of facilities advised women to limit the duration of suckling at each breast-feeding, and 45% reported giving paci-fiers to healthy term infants.
Inappropriate provision and promo-tion of infant formula were common, despite evidence that such practices reduce breastfeeding success.4–6,23
Twenty-four percent of facilities re-ported regularly giving non– breast milk supplements to more than half of all healthy, term infants. These results are consistent data from the Infant Feeding Practices Study II, which found that 41% of breastfed infants are sup-plemented with infant formula in the hospital.15,24,25 Inappropriate
supple-mentation has been associated with shorter duration of breastfeeding in multiple studies,7,20,26,27and it also
in-curs health risks that are associated with nonexclusive breastfeeding.1,28
Moreover, the majority of facilities re-ported that they participate in formula company marketing programs. Multi-ple studies have shown that formula marketing packs reduce duration of
exclusive breastfeeding.23,29,30
Nonethe-less, fully 70% of facilities reported giv-ing commercial discharge packs that contain infant formula to breastfeed-ing mothers. A separate study found that 93% of hospitals give out any com-mercial discharge packs to at least some mothers.31
The mPINC study results provide the first national, systematically collected data on the substantial gap between best practices and routinely provided maternity care. Underuse of these evidence-based practices leads to pre-mature weaning, with adverse conse-quences for maternal and infant health.
BARRIERS TO QUALITY IMPROVEMENT
Changes to Clinical Routine
Optimizing breastfeeding support will require cultural changes in patterns of care in hospitals. For example, on a busy postpartum unit, it is much eas-ier to offer a bottle than to diagnose and resolve breastfeeding problems. Similarly, removing the infant from the mother’s room to perform a variety of procedures (eg, photographs, new-born screening, examinations) may be convenient for a busy hospital, but this practice interferes with the mother’s ability to breastfeed on demand. These issues are substantial barriers to im-plementing Baby-Friendly practices, as a national survey showed: hospitals re-ported that the most difficult steps to implement were steps 6 (no sup-plements), 2 (staff training), and 7 (rooming in).
Formula Marketing
Doing away with hospital-based mar-keting of infant formula and paying fair market value for formula have posed a particular barriers to implementing evidence-based care.19Typically, most
US hospitals receive their well-infant formulas free of charge from
brand-name manufacturers and in return are expected to distribute commercial dis-charge packs that market that brand, thereby implying endorsement from the hospital. In Baby-Friendly hospi-tals, the cost of purchasing formula is passed on in the room and board charge, the same way food for other patients is handled.
Safety-net hospitals such as Boston Medical Center and San Francisco Gen-eral Hospital have been able to achieve Baby-Friendly status and pay for for-mula. Implementing BFHI also de-creases costs of unused products such as pacifiers, nipples, and dis-charge packs and saves on labor costs and storage space required for dis-charge packs.32 Formula companies
have been known to overestimate vastly the amount of formula that a hospital requires, grossly inflating projected costs.32 If hospitals wait to
pay for formula until they have imple-mented the other steps, then the need for purchased formula is reduced.32,33
It may be helpful for hospital leaders to know that severing ties from the for-mula industry is consistent with re-cent recommendations that the health professions distance them-selves from industry to avoid con-flicts of interest that could compro-mise patient care.34,35
Attitudes and Beliefs
To implement elements of the BFHI, supporters must negotiate varying at-titudes and beliefs about breastfeed-ing. Norms for infant feeding have changed dramatically in the past 3 de-cades. Some senior staff members, many of whom have formula-fed their own children, firmly believe that for-mula feeding is substantially equiva-lent to breastfeeding.36A recent study
found that 45% of pediatricians sur-veyed agreed with the statement that breastfeeding and formula feeding are equally acceptable methods for
feed-SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e795
. Provided by Indonesia:AAP Sponsored on July 17, 2010
www.pediatrics.org
ing infants.37Others view infant
feed-ing as a consumer choice, not a modi-fiable health behavior, and they are reluctant to “push” mothers to breast-feed. Efforts to change breastfeeding practices will have to address this ten-sion between reinforcing medical rec-ommendations and respecting patient autonomy. Moreover, many providers argue that maternity care has little or no impact on breastfeeding success, and they will need to be convinced that practice changes matter. Finally, pro-viders may lack the skills to address basic breastfeeding needs, because breastfeeding training in medical and nursing education is limited, at best.38
Achieving 18 to 21 hours of training for perinatal nurses has been described as a significant barrier to achieving Baby-Friendly certification, although this is the minimum recommenda-tion.19This results in clinicians’ leaving
simple breastfeeding problems unre-solved or relegating them to lactation consultants, whose expertise is better used for more complex issues.
METRICS FOR QUALITY ASSESSMENT
Several metrics are available for mea-suring quality of breastfeeding care, ranging from comprehensive BFHI cer-tification to compliance with individual steps, such as paying market value for infant formula. Other metrics include the distribution of formula company discharge packs, mPINC scores, pres-ence of an evidpres-ence-based written breastfeeding policy, and the rate of in-hospital exclusive breastfeeding among breastfeeding infants. Each metric has its advantages and disad-vantages (Table 2).
The rate of in-hospital exclusive breastfeeding among breastfed in-fants is especially promising for sev-eral reasons. First, it can be measured as part of existing infrastructure for collecting neonatal data, via genetic
screening surveys or by modifying and implementing the US Standard Certifi-cate of Live Birth to collect this infor-mation. Second, to score high on exclu-sive breastfeeding, a hospital would need to have successfully imple-mented many of the other Ten Steps that are known to decrease the use of supplementation and improve breast-feeding success, such as rooming in, breastfeeding in the first hour of life, and curtailment of formula marketing. Finally, in-hospital exclusivity is pa-tient centered, because its association with improved breastfeeding duration helps women meet their own breast-feeding goals. The National Quality Fo-rum (NQF) recently endorsed the rate of in-hospital exclusive breastfeeding as a consensus standard for perinatal care.39
APPROACHES TO IMPROVING QUALITY OF CARE
To date, there have been few published reports on approaches to improving quality of care around breastfeeding. Potential approaches include educa-tion of hospital decision-makers, rec-ognition of excellence, oversight by accrediting organizations, public re-porting, P4P incentives, and regional collaboratives.
Education of Hospital Decision-Makers
There are a variety of opportunities to educate and motivate key hospital decision-makers to adopt evidence-based practices. Lactation consultants and nongovernmental organizations are often contracted by hospitals to as-sist with quality improvement around breastfeeding. Regional meetings or a summit of key leaders could help to educate stakeholders and improve networking opportunities and buy-in, and these sessions could include train-ing on implementation of best prac-tices. Sharing peer-reviewed publica-tions about the evidence for the Ten
Steps and about implementing them can be influential, as can Web-based resources. Often, an individual who already works in the hospital leads this type of educational effort, with the regional effort from an outside organization.
The mPINC survey was explicitly de-signed to educate decision-makers and stimulate hospitals to implement evidence-based best practices. The CDC shared survey results with all 2690 participating hospitals and birth centers, assigning each facility a set of scores that compared their own prac-tices with evidence-based pracprac-tices, highlighting those that are most prob-lematic. The individualized reports compared each hospital’s scores with those in other facilities across their state and the country and with those of a similar size. These “benchmark reports” included references to the scientific literature explaining how each practice affects breastfeeding success. The CDC plans to repeat the survey every 2 years so that hospi-tals can engage in continuous quality improvement.
Grassroots movements can also serve as a catalyst to draw the attention of decision-makers around a specific hospital practice. A growing body of ev-idence shows that commercial dis-charge packs are associated with de-creased exclusive breastfeeding.29,40,41
The Ban the Bags campaign (http:// banthebags.org) has drawn attention to the risks of hospital-based formula promotion, attracting national press coverage and encouraging hospitals to reevaluate this practice.8,42In addition,
state breastfeeding coalitions and departments of public health have awarded certificates to “bag-free” hos-pitals, helping incentivize efforts to im-prove quality of care.
TABLE 2 Metrics That Can Be Used for Public Reporting and/or P4P Incentives and Related Advantages and Disadvantages
Facility Metric (Measure) Method Advantages Disadvantages Comments Breastfed infants who receive
only breast milk during the maternity stay (proportion of breastfed infants)
1. Feeding status as indicated in newborn genetic screening or birth certificate documentation 1. Rates of EBF in hospital predict overall breastfeeding duration
1. Feasibility of data collection varies across states
1. The NQF has endorsed using EBF in the hospital as a quality measure in part on the basis of success in California of using this metric
2. Infant formula dispensed from Pyxis system
2. High EBF rates reflect presence of many of the Ten Steps
2. In states without current data collection infrastructure, adoption would require either amendments to the birth certificate or genetic screening forms or periodic chart audit/review
2. This metric could easily be assessed and adopted by HEDIS and was recently adopted by Joint Commission
3. Prevalence determined from chart audit/ review
3. Generally appropriately excludes those for whom breastfeeding is
contraindicated (eg, HIV positive, dependent on drugs of abuse), allowing for comparability across facilities and patient populations
3. Political and economic influence from the infant formula industry could make establishment of Pyxis dispensation and tracking of infant formula more difficult
Baby-Friendly status (yes/no) Facility designation by Baby-Friendly USA 1. Requires no new assessment infrastructure
1. Less than 3% of US hospitals are currently designated Baby-Friendly, so it is not considered a normative standard yet
Federal oversight and/or a system for recognizing partial implementation of the Ten Steps may be necessary for hospitals to be able to pursue 2. Specifically identifies compliance with
evidence-based practice and care process measures
2. Designation does not recognize partial implementation
financial incentives to implementing the Ten Steps
3. Ensures standardized compliance with the Ten Steps
4. Status is widely regarded and recognized
mPINC survey score (score out of 100)
Facility score based on responses to CDC survey
Provides a national, standard measure of hospital practices and care processes
1. Because individual facility scores are confidential, disclosure would be voluntary
Facilities’ mPINC scores could provide a baseline for regional collaboratives to use to assess included in the Ten Steps 2. Disclosure could affect accuracy of future survey
results
progress by using quality improvement strategies
3. Scores are based on 1 individual’s report of typical practices and care processes at each hospital and have not been externally validated Written breastfeeding policy
including core evidence-based breastfeeding practices (yes/no)
Facility documentation of written policy Assessment is straightforward via either inquiry to facility or use of existing mPINC data
Written policies may not reflect actual practice; there may be issues with accurate reporting
The Academy of Breastfeeding Medicine has a freely available model policy and provides a template for hospitals to implement evidence-based practices
Distributes formula company discharge packs (yes/no)
Facility self-report 1. Assessment is straightforward via inquiry to facility
Addresses only 1 of the important barriers to breastfeeding
Facilities that have received awards for becoming “Bag-Free Hospitals” have improved visibility 2. Reflects base level of commitment to
supporting breastfeeding
and recognition of the adverse effects of direct formula marketing to patients
3. Reflects independence from inappropriate marketing to patients Price paid for infant formula
(price per unit purchased
Facility self-report 1. Assessment is straightforward via review of purchase contracts
Definition of “fair-market price” may be difficult to establish
Growing awareness of the impact of “free” or discounted brand-name pharmaceuticals has relative to fair-market
price or 0关received free of
2. Reflects a commitment to supporting breastfeeding
drawn attention to ethical concerns about hospital marketing of branded products charge from
manufacturer兴)
3. Reflects reduced influence from infant formula manufacturers
EBF indicates exclusive breastfeeding.
SPECIAL
. Provided by Indonesia:AAP Sponsored on July 17, 2010
www.pediatrics.org
AAP policy statement on breastfeed-ing13outlines appropriate peripartum
procedures to facilitate the initiation of breastfeeding, as does the state-ment from the American Academy of Family Physicians (AAFP).12The
Acad-emy of Breastfeeding Medicine has de-veloped a model hospital policy to guide hospitals.43
Recognition of Excellence
Several recognition programs honor hospitals that practice evidence-based breastfeeding care. The oldest and most rigorous form of recognition is Baby-Friendly designation. To qualify as Baby-Friendly, a facility must apply for a certificate of intent, implement the Ten Steps, and undergo a site visit. Baby-Friendly remains the gold stan-dard because of its strong evidence base and its origins from WHO and UNICEF. Baby-Friendly status is highly regarded by health professionals but is largely unknown to the general public.
Hospitals often are able to achieve the Ten Steps by using standard quality management techniques, such as the “plan-do-check-act” model.44
Imple-menting certain practices, such as skin-to-skin contact immediately after birth, and increased staff training may allow other steps to fall into place more readily.
In addition to BFHI, several states have developed recognition programs for excellence in breastfeeding care. The Texas Department of State Health Ser-vices has its own recognition program, the “Texas Ten Step.” This program is based on the BFHI, but compliance is self-reported, and the program does not require hospitals to purchase for-mula at fair-market value. The pro-gram offers staff training and encour-ages hospitals ultimately to obtain the BFHI designation. As of April 2009, 68 of 190 hospitals had the Texas Ten Step certification,45but only 2 Texas
hospi-tals are designated as Baby-Friendly9
and only 6 have reported eliminating commercial discharge packs.46 Other
state departments of health, such as Oregon’s, have publicly recognized hospitals that have eliminated com-mercial discharge bags, and Massa-chusetts is now following suit by rec-ognizing bag-free hospitals and other improvements in breastfeed-ing outcomes.
Oversight by Accrediting Organizations
Accrediting organizations have con-siderable leverage in modifying hospi-tal practices. The Joint Commission, which accredits most US hospitals, has set quality measures in many ar-eas, with many more expected to fol-low. All of these metrics are publicly reported and the subject of consider-able attention by hospital administra-tors nationwide. Until recently, no quality metric related to breastfeeding was available from the Joint Commis-sion. However, on July 20, 2009, the Joint Commission announced that it was adding ‘exclusive breast milk feed-ing’ as a new hospital Core Measure for perinatal care, effective April 2010.47 It is likely that this new Core
Measure could have a tremendous im-pact on hospital practice and breast-feeding outcomes. It is likely that add-ing a breastfeedadd-ing metric, such as the exclusivity rate, to the Joint Commis-sion Core Measures could have a tre-mendous impact on hospital practice and breastfeeding outcomes.
State regulations, promulgated by state health departments, also repre-sent an opportunity to improve breast-feeding practices; however, often states do not have the resources or the polit-ical power to implement strong regu-lations or enforce compliance with them. For example, in 2005, the Massa-chusetts Department of Public Health approved sweeping new perinatal
reg-ulations that included a first-in-the-nation requirement to discontinue hospital distribution of commercial discharge packs, but before the regu-lation could be implemented, it was re-tracted by the governor.
Public Reporting
Public reporting of quality metrics also encourages hospitals to practice evidence-based care, because patients are attracted to hospitals that consis-tently show better performance. The California WIC Association together with the University of California Davis Human Lactation Center have success-fully used public reporting to drive quality improvement.48 They publicly
reported the “gap” between any and exclusive breastfeeding for each of the state’s maternity hospitals. These data were collected at the time of genetic screening, and chart review suggests that it is accurate (M.J. Heinig, written communication, April 2009). In some maternity centers,⬎99% of breastfed infants were receiving formula, clearly far more than is medically indicated. After the first public report, 12 hospi-tals were able to increase their exclu-sive breastfeeding rates by at least 50%, and 5 more than doubled their rates.48Some hospitals now handle
Health Plan Employer Data and Information Set
Health Plan Employer Data and Infor-mation Set (HEDIS) is another venue for public reporting of breastfeeding care quality. This data set is used by ⬎90% of America’s health plans to measure performance on important dimensions of care and service.49
Many health plans report HEDIS data to employers or use their results to make improvements in their quality of care and service. Thus far, HEDIS has not included breastfeeding measures. A breastfeeding metric included as a HEDIS measure may be helpful to initiate, track, and measure ongoing efforts to improve lactation care and services.
Pay for Performance
P4P plans offer additional financial compensation to individual providers, groups, or hospitals for meeting cer-tain quality standards. Premier, Inc, and the federal Centers for Medicaid and Medicare Services recently com-pleted a demonstration project of P4P to hospitals and found that those that received extra payment did modestly better than those that were subjected to public reporting alone.50
Although there have been some rare insurance initiatives that reward mothers who breastfeed, to our knowl-edge, there have been no public or pri-vate insurance initiatives in the United States to reward hospitals or doctors who have higher breastfeeding rates among their patients. Incentives can take the form of bonuses or withholds and can be either outcome measures (eg, hospital rates of exclusive breast-feeding) or process measures (eg, im-plementation of BFHI). In northern It-aly, hospitals successfully increased in breastfeeding rates after an initiative of withholding 0.5% of payment for all diagnosis-related groups for failure to meet some specific breastfeeding pro-cess objectives set by the local health
authorities.51 Breastfeeding was 1 of
several quality objectives, and failure to meet the other objectives resulted in additional diagnosis-related group withholdings.
Although P4P has been widely imple-mented in internal medicine, the liter-ature on its effectiveness is mixed. Many organizations have published guidelines in response to criticisms, including the AAP,52the AAFP, the
Amer-ican Medical Association,53 and the
Joint Commission.54 The AAP
recom-mends that measures be scientifically valid and linked to evidence-based best practices. Moreover, they should be feasible so that data collection does not cause undue burden on the clini-cian, patients, and families. They con-cur with AAFP recommendations to of-fer positive physician incentives and support the physician–patient rela-tionship. The American Medical Associ-ation recommends 4 principles in de-termining proper metrics for P4P: (1) metrics should ensure quality of care; (2) they should foster the relation-ship between patient and provider; (3) they should used accurate and fair data reporting; and (4) they should provide fair and equitable program incentives.53
Breastfeeding best practices may be particularly well-suited to a P4P ap-proach, as compared with some other quality indicators. Insurers could offer incentives for outcomes, such as the exclusivity rate, or for structure and process measures, such as BFHI certi-fication. Hospitals could use P4P reve-nue to fund implementation of some practices, such as ensuring adequate staff training and paying fair-market value for infant formula, and could help move more hospitals to Baby-Friendly status.
P4P incentives for breastfeeding sup-port are likely to save money for insur-ers, especially in the long-term. Infants who are formula fed have higher
health expenditures for certain acute illness.2,3 Chronic pediatric diseases
are very costly, as are maternal malig-nancies and diabetes. Financial incen-tives may draw enough hospitals to ap-ply for certification that a tipping point will be reached, in which BFHI status becomes competitive and achievable. Because training in breastfeeding is not uniform and because research shows that many providers feel un-comfortable managing breastfeeding problems,38 another quality metric
may consist of documenting continu-ing education for physicians and office nurses specifically in breastfeeding.
Regional Collaboratives
In a regional collaborative, staff from different hospitals work together to learn from each other and meet com-mon quality improvement goals at their home institutions. Typically, key stakeholders and “champions” learn what their peers elsewhere are doing and seek guidance about implement-ing change. Two studies have shown that a local collaborative approach can improve quality of care with various quality issues.55,56
Mercier et al56improved newborn
pre-ventive services in Vermont maternity hospitals over 13 evidence-based pa-rameters, including assessment of breastfeeding adequacy and risk for hyperbilirubinemia. The authors in-vited all maternity hospitals in the state to work together to improve their performance. During the intervention, documentation of breastfeeding as-sessment improved from 49% to 81%.
Statewide collaborative approaches, such as those taken in Vermont, are likely to replicate success in other states. Collaborative approaches de-pend on the will and funding of state departments of public health or other strong leaders to organize and spear-head them but ultimately use a “bot-tom up” approach to effect change
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e799
. Provided by Indonesia:AAP Sponsored on July 17, 2010
www.pediatrics.org
in individual institutions, achieving buy-in and sustainability. If such ef-forts can increase breastfeeding, then they may be cost-effective in saving the state Medicaid dollars. The approach in Northern Italy also had collaborative elements and a bottom-up approach, which may ex-plain part of its success. Greater Los Angeles has a collaborative around breastfeeding in the 12 counties in that region and has 18 Baby-Friendly hospitals there. The MADLAC pro-gram in El Salvador was a national collaborative with strong central
leadership that was associated with significant increases in implementa-tion of the Ten Steps and in duraimplementa-tion of exclusive breastfeeding.57
CONCLUSIONS
Breastfeeding is an important public health issue. Most hospitals fall far short of implementing evidence-based best practices; as a result, current US breastfeeding rates remain well below Healthy People 2010 goals. Despite this quality gap, there are limited incen-tives for hospitals or providers to im-plement best practices. Potential
ap-proaches to quality improvement include education of hospital decision-makers, recognition of excellence, oversight by accrediting organiza-tions, public reporting, P4P incentives, and regional collaboratives. Wide-spread implementation of BFHI in the United States would be most likely to occur with strong centralized leader-ship, as in other successful countries. Such efforts to improve quality of care could affect both initiation and dura-tion of breastfeeding, with substantial, lasting benefits for maternal and child health.
REFERENCES
1. Ip S, Chung M, Raman G, et al. Breastfeeding and maternal and infant health outcomes in devel-oped countries. In:Evidence Report/Technology Assessment Number 153. Agency for Healthcare Research and Quality; April 2007
2. Ball TM, Wright AL. Health care costs of formula-feeding in the first year of life.Pediatrics.
1999;103(4 pt 2):870 – 876
3. US Bureau of Labor Statistics. Inflation calculator. Available at: www.bls.gov/data/ inflation㛭calculator.htm. Accessed April 8, 2009
4. DiGirolamo A, Grummer-Strawn L, Fein S. Maternity care practices: implications for breastfeed-ing.Birth.2001;28(2):94 –100
5. Kramer MS, Aboud F, Mironova E, et al. Breastfeeding and child cognitive development: new evidence from a large randomized trial.Arch Gen Psychiatry.2008;65(5):578 –584
6. Murray EK, Ricketts S, Dellaport J. Hospital practices that increase breastfeeding duration: re-sults from a population-based study.Birth.2007;34(3):202–211
7. World Health Organization, Division of Child Health and Development.Evidence for the Ten Steps to Successful Breastfeeding (Revised). Geneva, Switzerland: World Health Organization; 1998 8. Centers for Disease Control and Prevention. Breastfeeding-related maternity practices at
hospi-tals and birth centers: United States, 2007.MMWR Morb Mortal Wkly Rep.2008;57(23):621– 625 9. BFHI USA. 83 US Baby-Friendly hospitals and birth centers as of July 2009. Available at:
www.babyfriendlyusa.org/eng/03.html. Accessed August 10, 2009
10. Hofvander Y. Breastfeeding and the Baby Friendly Hospitals Initiative (BFHI): organization, re-sponse and outcome in Sweden and other countries.Acta Paediatr.2005;94(8):1012–1016 11. Institute of Medicine, Committee on Quality of Health Care in America.Crossing the Quality Chasm:
A New Healthy System for the 21st Century. Washington, DC: National Academy of Sciences; 2001 12. American Academy of Family Physicians. Breastfeeding, family physicians supporting (position paper). Available at: www.aafp.org/online/en/home/policy/policies/b/breastfeedingpositionpaper.html. Ac-cessed January 20, 2009
13. Gartner LM, Morton J, Lawrence RA, et al. Breastfeeding and the use of human milk.Pediatrics.
2005;115(2):496 –506
14. WHO/UNICEF.WHO/UNICEF Global Strategy for Infant and Young Child Feeding. Geneva, Switzerland: World Health Organization; 2003
15. Centers for Disease Control and Prevention. Breastfeeding among U.S. children born 1999 –2005, CDC National Immunization Survey. Available at: http://cdc.gov/breastfeeding/data/NIS㛭data/ index.htm. Accessed August 12, 2008
16. American Public Health Association. Policy No. 200714: a call to action on breastfeeding: a funda-mental public health issue. Available at: www.apha.org/advocacy/policy/policysearch/ default.htm?id⫽1360. Accessed February 14, 2009
18. Rosenberg KD, Stull JD, Adler MR, Kasehagen LJ, Crivelli-Kovach A. Impact of hospital policies on breastfeeding outcomes.Breastfeed Med.2008;3(2):110 –116
19. Merewood A, Mehta SD, Chamberlain LB, Philipp BL, Bauchner H. Breastfeeding rates in US Baby-Friendly hospitals: results of a national survey.Pediatrics.2005;116(3):628 – 634
20. DiGirolamo AM, Grummer-Strawn LM, Fein SB. Effect of maternity-care practices on breastfeeding.
Pediatrics.2008;122(suppl 2):S43–S49
21. Grizzard TA, Bartick M, Nikolov M, Griffin BA, Lee KG. Policies and practices related to breastfeeding in Massachusetts: hospital implementation of the ten steps to successful breastfeeding.Matern Child Health J.2006;10(3):247–263
22. Nylander G, Lindemann R, Helsing E, Bendvold E. Unsupplemented breastfeeding in the maternity ward: positive long-term effects.Acta Obstet Gynecol Scand.1991;70(3):205–209
23. Rosenberg KD, Eastham CA, Kasehagen LJ, Sandoval AP. Marketing infant formula through hospitals: the impact of commercial hospital discharge packs on breastfeeding.Am J Public Health.2008;98(2):290 –295
24. Grummer-Strawn LM, Scanlon KS, Fein SB. Infant feeding and feeding transitions during the first year of life.Pediatrics.2008;122(suppl 2):S36 –S42
25. Centers for Disease Control and Prevention. Infant Feeding Practices Study II. Available at: www.cdc.gov/ifps. Accessed January 20, 2009
26. Gray-Donald K, Kramer MS, Munday S, Leduc DG. Effect of formula supplementation in the hospital on the duration of breast-feeding: a controlled clinical trial.Pediatrics.1985;75(3):514 –518 27. Blomquist HK, Jonsbo F, Serenius F, Persson LA. Supplementary feeding in the maternity ward
shortens the duration of breast feeding.Acta Paediatr.1994;83(11):1122–1126
28. Kramer MS, Kakuma R. The optimal duration of exclusive breastfeeding: a systematic review.Adv Exp Med Biol.2004;554:63–77
29. Donnelly A, Snowden H, Renfrew M, Woolridge M. Commercial hospital discharge packs for breast-feeding women.Cochrane Database Syst Rev.2000;(2):CD002075
30. Howard C, Howard F, Lawrence R, et al. Office prenatal formula advertising and its effect on breastfeeding patterns.Obstet Gynecol.2000;95(2):296 –203
31. Merewood A, Grossman X, Singleton M, et al. Formula freebies from the hospital: patterns of sample pack distribution in 50 US states.Proceedings of the Annual Meeting of the American Public Health Association; 2008. Available at: http://apha.confex.com/apha/136am/webprogram/ Paper170961.html. Accessed August 10, 2009
32. Merewood A, Philipp BL. Becoming Baby-Friendly: overcoming the issue of accepting free formula.
J Hum Lact.2000;16(4):279 –282
33. Turner-Maffei C, Cadwell K, eds.Overcoming Barriers to Implementing the Ten Steps to Successful Breastfeeding.E. Sandwich, MA: Baby-Friendly USA; 2004
34. Brennan TA, Rothman DJ, Blank L, et al. Health industry practices that create conflicts of interest: a policy proposal for academic medical centers.JAMA.2006;295(4):429 – 433
35. Rothman DJ, McDonald WJ, Berkowitz CD, et al. Professional medical associations and their relationships with industry: a proposal for controlling conflict of interest.JAMA.2009;301(13): 1367–1372
36. Li R, Rock VJ, Grummer-Strawn L. Changes in public attitudes toward breastfeeding in the United States, 1999 –2003.J Am Diet Assoc.2007;107(1):122–127
37. Feldman-Winter LB, Schanler RJ, O’Connor KG, Lawrence RA. Pediatricians and the promotion and support of breastfeeding.Arch Pediatr Adolesc Med.2008;162(12):1142–1149
38. Taveras EM, Li R, Grummer-Strawn L, et al. Opinions and practices of clinicians associated with continuation of exclusive breastfeeding. Pediatrics. 2004;113(4). Available at: www. pediatrics.org/cgi/content/full/113/4/e283
39. National Quality Forum. National Quality Forum Endorses National Consensus standards for peri-natal care. Available at: www.qualityforum.org/news/releases/102708-endorsed-measures-pc.asp. Accessed December 23, 2008
40. Government Accountability Office Report to Congressional Addressees. Breastfeeding: Some Strategies Used to Market Infant Formula May Discourage Breastfeeding; State Contracts Should Better Protect Against Misuse of WIC Name. Washington, DC: United States Government; 2006 41. Shealy K, Li R, Benton-Davis S, Grummer-Strawn L.The CDC Guide to Breastfeeding Interventions.
Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2005
42. Merewood A, Fonrose R, Singleton M, et al. From Maine to Mississippi: hospital distribution of formula sample packs along the Eastern Seaboard. Arch Pediatr Adolesc Med.2008;162(9): 823– 827
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 4, October 2009 e801
. Provided by Indonesia:AAP Sponsored on July 17, 2010
www.pediatrics.org
43. Academy of Breastfeeding Medicine. Protocol #7: model breastfeeding policy. Available at: www.bfmed.org. Accessed November 2, 2008
44. Fletcher DM. Achieving Baby Friendly through a quality management approach.Aust Coll Midwives Inc J.1997;10(3):21–26
45. Texas Department of State Health Services.Texas Ten Step: Supporting the Health of Future Texans. Austin, TX: Texas Department of State Health Services; 2009. Available at: www.dshs.state.tx.us/wichd/ lactate/txfact_facilities.shtm. Accessed August 10, 2009
46. Ban the Bags. Bag-free hospitals. Available at: http://banthebags.org/bag-free-hospitals. Ac-cessed August 10, 2009
47. The Joint Commission. National hospital inpatient quality measures—Perinatal Care Core Measure Set, updated July 20, 2009. Available at: www.jointcommission.org/PerformanceMeasurement/ PerformanceMeasurement/Perinatal⫹Care⫹Core⫹Measure⫹Set.html. Accessed July 23, 2009 48. California WIC Association, UC Davis Human Lactation Center. Depends on where you are born:
California must close the gap in exclusive breastfeeding rates. In:Joint Report of CWA and UC Davis Human Lactation Center; 2008. Available at: www.calwic.org/bfreport_2008.aspx. Accessed January 27, 2009
49. National Committee for Quality Assurance. HEDIS & quality measurement. Available at: www.ncqa.org/tabid/59/Default.aspx. Accessed January 21, 2009
50. Lindenauer PK, Remus D, Roman S, et al. Public reporting and pay for performance in hospital quality improvement.N Engl J Med.2007;356(5):486 – 496
51. Cattaneo A, Borgnolo G, Simon G. Breastfeeding by objectives.Eur J Public Health.2001;11(4): 397– 401
52. Hodgson ES, Simpson L, Lannon CM. Principles for the development and use of quality measures.
Pediatrics.2008;121(2):411– 418
53. American Medical Association. Guidelines for Pay-for-Performance Programs. Available at: www.ama-assn.org/ama1/pub/upload/mm/368/guidelines4pay62705.pdf. Accessed August 12, 2008
54. Joint Commission. Public policy: principles for the construct of pay-for-performance programs. Available at: www.jointcommission.org/PublicPolicy/pay.htm. Accessed August 12, 2008 55. Mandl KD, Tronick EZ, Brennan TA, Alpert HR, Homer CJ. Infant health care use and maternal
depression.Arch Pediatr Adolesc Med.1999;153(8):808 – 813
56. Mercier CE, Barry SE, Paul K, et al. Improving newborn preventive services at the birth hospitalization: a collaborative, hospital-based quality-improvement project.Pediatrics.2007; 120(3):481– 488
DOI: 10.1542/peds.2009-0430
2009;124;e793-e802; originally published online Sep 14, 2009;
Pediatrics
M. Grummer-Strawn
Melissa Bartick, Alison Stuebe, Katherine R. Shealy, Marsha Walker and Laurence
Hospital
Closing the Quality Gap: Promoting Evidence-Based Breastfeeding Care in the
& Services
Updated Information
http://www.pediatrics.org/cgi/content/full/124/4/e793
including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/124/4/e793#BIBL
at:
This article cites 30 articles, 18 of which you can access for free
Citations
es
http://www.pediatrics.org/cgi/content/full/124/4/e793#otherarticl
This article has been cited by 1 HighWire-hosted articles:
Subspecialty Collections
m
http://www.pediatrics.org/cgi/collection/nutrition_and_metabolis Nutrition & Metabolism
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtml
tables) or in its entirety can be found online at:
Information about reproducing this article in parts (figures,
Reprints
http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
. Provided by Indonesia:AAP Sponsored on July 17, 2010
www.pediatrics.org