Relationship Between Vascular Endothelial Growth
Factor and Severity of Hepatocellular Carcinoma
Arles*, Rino Alvani Gani**, Ari Fahrial Syam***, Hamzah Shatri****
*Department of Internal Medicine, Awal Bros Hospital, Pekanbaru**Division of Hepatobiliary, Department of Internal Medicine
Faculty of Medicine, University of Indonesia/Dr. Cipto Mangunkusumo General National Hospital, Jakarta ***Division of Gastroenterology, Department of Internal Medicine, Faculty of Medicine
University of Indonesia/Dr. Cipto Mangunkusumo General National Hospital, Jakarta ****Division of Psychosomatic, Department of Internal Medicine, Faculty of Medicine University of Indonesia/Dr. Cipto Mangunkusumo General National Hospital, Jakarta
Corresponding author:
Arles. Department of Internal Medicine, Awal Bros Hospital. Jl. Jendral Sudirman No. 117 Pekanbaru Indonesia. Phone: +62-76-147333; Facsimile: +62-76-147222. E-mail: [email protected]
ABSTRACT
Background:Severity of hepatocellular carcinoma (HCC) that is assessed using barcelona clinic liver cancer
(BCLC) classification is a main prognostic factor of hepatocellular carcinoma. Assessment of the serum level of vascular endothelial growth factor (VEGF) is considered to reflect the severity of HCC. However, there is still
no fundamental basis of the association of severity of HCC with the serum VEGF level. The objective of this study is to know the relationship between serum VEGF levels with the severity of HCC by assessing the average difference of serum VEGF level in various severity of HCC.
Method: This study was a cross sectional study to identify the association between serum VEGF levels with
the severity of HCC based on BCLC classification. This study was performed in Cipto Mangunkusumo Hospital
between January and May 2015. Statistical tests used to evaluate the association between serum VEGF level
with BCLC classification was one-way ANOVA analysis, and continued with post hoc Tukey Schaffe analysis. Results: A total of 61 subjects with HCC were included into this study. In this study, we did not find subjects
with stage 0 BCLC. The average of serum VEGF level in stage A BCLC was 288.26 ± 156.6 pg/mL; stage B BCLC: 434 ± 164.8 pg/mL; stage C BCLC: 785.57 ± 194.25 pg/mL; stage D BCLC: 1537.97 ± 660.62 pg/
mL. One-way ANOVA analysis showed significant difference (P < 0.001) between serum VEGF level and HCC severity based on BCLC classification. Post hoc Tukey Schaffe analysis showed the presence of significant difference between stage A and C BCLC (p < 0.05) and stage A and D BCLC (p < 0.001), stage B and D BCLC (p < 0.001), and stage C and D BCLC (p < 0.001). There was no significant difference between stage A and B
BCLC, and between stage B and C BCLC.
Conclusion: It was found that serum VEGF level increased in accordance to the HCC severity based on
BCLC classification, particularly for stage B BCLC and above.
ABSTRAK
Latar belakang: Derajat keparahan karsinoma hepatoselular (KHS) yang dinilai dengan klasifikasi barcelona
clinic liver cancer (BCLC) merupakan faktor prognostik utama KHS. Penilaian kadar serum vascular endothelial growth factor (VEGF) dianggap dapat mencerminkan tingkat keparahan KHS. Namun, belum ada landasan mengenai hubungan tingkat keparahan KHS dengan kadar serum VEGF. Tujuan penelitian ini adalah untuk mengetahui hubungan kadar serum VEGF dengan tingkat keparahan KHS dengan menilai perbedaan rerata kadar serum VEGF pada berbagai tingkat keparahan KHS.
Metode: Penelitian ini adalah studi potong lintang untuk menentukan hubungan antara kadar serum VEGF
dengan tingkat keparahan KHS berdasarkan klasifikasi BCLC. Penelitian ini dilakukan di Rumah Sakit Cipto
Mangunkusumo antara bulan Januari 2015 dan Mei 2015. Uji statistik yang digunakan untuk menilai hubungan
kadar serum VEGF dengan klasifikasi BCLC ialah analisis one-way ANOVA, dan dilanjutkan dengan analisis
post hoc Tukey Schaffe.
Hasil: Sebanyak 61 subyek KHS diikutkan dalam penelitian ini. Pada penelitian ini tidak ditemukan subyek dengan BCLC stage 0. Rerata kadar serum VEGF BCLC stage A adalah 288,26 ± 156,6 pg/mL; BCLC stage B: 434 ± 164,8 pg/mL; BCLC stage C: 785,57 ± 194,25 pg/mL; BCLC stage D: 1537,97 ± 660,62 pg/mL. Analisis
one-way ANOVA menunjukkan perbedaan bermakna (p < 0,001) antara kadar serum VEGF dengan tingkat keparahan KHS berdasarkan klasifikasi BCLC. Analisis post hoc dengan Tukey Schaffe menunjukkan adanya perbedaan bermakna antara BCLC stage A dan C (p < 0 ,05) serta BCLC stage A dan D (p < 0.001), BCLC stage B dan D (p < 0.001), dan BCLC stage C dan D (p < 0.001). Tidak ditemukan perbedaan bermakna antara
subyek dengan BCLC stage A dan B, dan antara BCLC stage B dan C.
Simpulan: Didapatkan kadar serum VEGF yang meningkat sesuai dengan tingkat keparahan KHS
berdasarkan klasifikasi BCLC terutama untuk BCLC stage B ke atas.
Kata kunci: Vascular endothelial growth factor (VEGF), keparahan karsinoma hepatoselular (KHS), barcelona clinic liver cancer (BCLC).
INTRODUCTION
Hepatocellular carcinoma (HCC) is the most severe primary liver cancer deriving from hepatocytes. Of all diagnosed liver tumour, 85% is HCC and 15% is other tumours.1 This primary liver cancer ranks sixth
as the most common malignancy in the world and ranks second as the cause of death with more than one million case fatalities per year.2,3 Approximately
70-80% patients with HCC have background of chronic liver disease, even those who suffer from HBV and HCV have risk of developing HCC 15 times and 17 times higher, respectively.4,5
The main prognostic factors of HCC are clinical pathological characteristics of the disease, which include HCC tumour size and degree of severity. One
of the HCC staging classifications, which is commonly
used, is staging by barcelona clinic liver cancer (BCLC).5,6 BCLC classification besides using
Child-Turcotte-Pugh classification to identify liver function,
also use tumour size and portal vein thrombosis criteria to reveal more accurate results. American Association for the Study of Liver Diseases (AASLD) and European Association for the Study of the Liver
(EASL) have agreed the use of BCLC classification as a
common staging system.2,6,7 The status of performance,
tumour size, metastasis, ascites, albumin and bilirubin level, prothrombin time, and portal vein thrombosis are the components used to evaluate the severity of HCC. Therefore, it is necessary to have an examination modality which could describe of staging or HCC severity rapidly.5,6
HCC is a tumour with high vascularisation which involves the expression of vascular endothelial growth factor (VEGF). VEGF plays role in tumour angiogenesis. VEGF expression in tumour cells is stimulated by hypoxia, oncogene (race), and inactivation of tumour suppressor gene (p53), and various cytokines. Activation of VEGF/VEGF receptor (VEGFR) stimulates mitogenesis, migration, differentiation, and vascular permeability, also mobilization of endothelial progenitor cells from the bone marrow to the peripheral circulation. VEGF activates endothelial cells through the effect of endothelial cells morphology changes, cytoskeleton changes, and stimulate the migration and growth of endothelial cells.8,9
prognostic in HCC patients. A meta-analysis study involving 16 studies showed the role of VEGF that
was statistically significant towards the survival in
general and disease-free survival in HCC, and that is correlated with the poor prognosis. 9,10,11 Whether the
level of VEGF is also associated with HCC severity as one of the main prognostic factors of HCC still need further studies. Examination of VEGF level is expected to be able to be marker of HCC severity in the future.
METHOD
This study was a cross sectional study to identify the association between VEGF with HCC severity based
on BCLC classification. This study was performed in
Hepatobiliary Division Polyclinic and Internal Medicine Inpatients Ward Cipto Mangunkusumo Hospital, Jakarta, as a national referral hospital in Indonesia. Study was performed from January to May 2015.
Study subjects were HCC patients aged more than 18 years old who visited Cipto Mangunkusumo Hospital during the study period. Sample was obtained through non-probability consecutive sampling method. Exclusion criteria were hepatic encephalopathy stage III and IV, severe sepsis, kidney failure, heart failure, presence of other tumour besides in the liver, severe hematemesis melena, HCC patients who had received curative or palliative management, and other diseases which increase the level of VEGF. After HCC diagnosis
was confirmed, patients’ disease severity was assessed
using the BCLC criteria. Further, patients had their blood drawn for 3.5 cc for VEGF level examination in the laboratory.
Data analysis was performed using SPSS 20 for windows software. Study results were presented in the form of univariate analysis, to describe the distribution of
component characteristic BCLC classification and VEGF
level. Statistical tests being used were one-way ANOVA, which was further continued with post hoc Tukey Schaffe
analysis. It was concluded to be significant if we found
p value < 0.05. This study had received ethical clearance from ethical commission of human biomedical research Faculty of Medicine University of Indonesia with ethical clearance letter No. 28/UN2.F1/ETIK/2014.
RESULTS
This study included 61 subjects with HCC who
fulfilled inclusion criteria, who further underwent
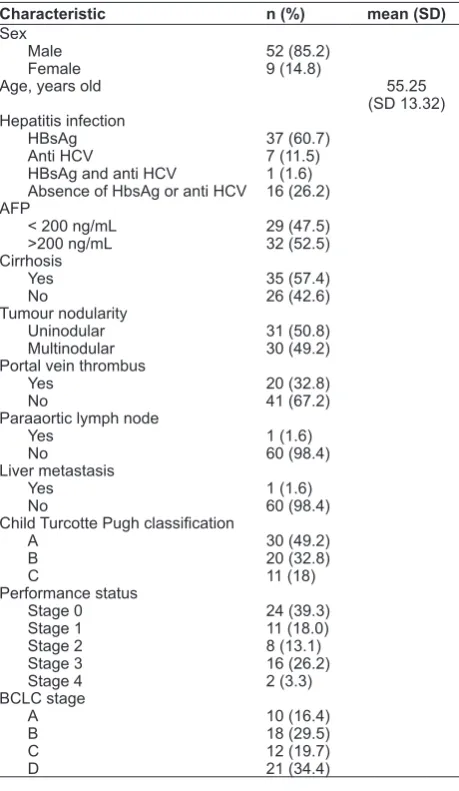
VEGF serum sample examination. Subjects consisted of 52 males and 9 females with the average age of 55
± 13 years old. Of overall study subjects, data obtained was positive HbsAg in 61% subjects, positive anti-HCV in 11% subjects, combination of positive HbsAg and anti HCV in 2% subjects, and absence of HbsAg or anti HCV in 26% subjects. Study subjects who had AFP value less than 200 ng/mL were 47%. CT scan results revealed study subjects with liver cirrhosis as much as 57%. Uninodular tumour was found in 51% subjects, while portal vein thrombus was found in 33% subjects. Metastasis to the lungs and lymph nodes was only found in 2% of study subjects.
Liver function measurement using
Child-Turcotte-Pugh (CP) classification revealed that most subjects had CP A classification, which was 49%, while most
study subjects’ performance status was stage 0, which
was 39%. HCC severity using BCLC classification
showed the distribution of subjects with stage A 16%, stage B 30%, stage C 20%, and stage D 34%, and no stage 0 was found. Complete characteristics of study subjects could be seen in Table 1.
Table 1. Characteristics of Study Subjects
Characteristic n (%) mean (SD)
Sex
Absence of HbsAg or anti HCV
Based on one-way ANOVA analysis, there was
a significant different in the average of VEGF level based on BCLC classification (p < 0.001). Subjects
group with stage A BCLC had average VEGF level of 288.26 ± 156.6 pg/mL, stage B BCLC group had average VEGF level of 434.96 ± 164.8 pg/mL, stage C BCLC had average VEGF level of 785.57 ± 194.25 pg/mL, and stage D BCLC group had average VEGF level of 1537.97 ± 660.62 pg/mL. Thus, it could be seen that the higher the staging of BCLC, the higher the VEGF level. From the post hoc analysis, we found
significant difference of VEGF level between stage
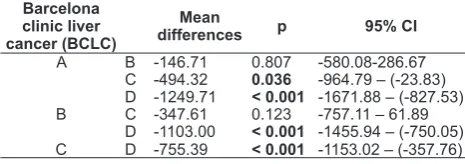
A and C BCLC (95% CI: 23.83-964.79), between stage A and D BCLC (95% CI: 827.53-1671.88), and between stage B and D (95% CI: 750.05-1455.94), and stage C and D BCLC (95% CI: 357.76-1153.02). This intervariables relationship was shown in Figure 1.
Figure 1. Mean differences of serum VEGF level with HCC severity based on BCLC classification in the post hoc Tukey Schaffe analysis.
p<0.001
p<0.05
p<0.001 p<0.001
Figure 1. Mean differences of serum VEGF level with HCC severity based on BCLC classification in the post hoc Tukey Schaffe analysis.
Table 2. VEGF level mean differences from Post Hoc Turkey analysis
A B -146.71 0.807 -580.08-286.67 C -494.32 0.036 -964.79 – (-23.83) D -1249.71 < 0.001 -1671.88 – (-827.53) B C -347.61 0.123 -757.11 – 61.89
D -1103.00 < 0.001 -1455.94 – (-750.05) C D -755.39 < 0.001 -1153.02 – (-357.76)
Another finding that was also important to be reported in this study was portal vein thrombosis. In this study, as much as 20 (32.8%) HCC subjects had portal vein thrombosis, with the average serum VEGF level of 1048.21 + 741.07 pg/mL. (Table 2).
Table 3. VEGF serum level with or without portal vein thrombosis
Variable
Average of VEGF level (pg/mL)
Study results showed that serum VEGF was correlated with HCC severity. The high VEGF level is also usually found in patients with vascular invasion or metastasis, thus this increase indicated poor prognosis in HCC patients. Therefore, VEGF has the potential to help predicting the occurring tumour differentiation and vascular invasion.12,13
Various mechanisms could regulate the expression of serum VEGF level in HCC; one of the most important mechanisms is hypoxia. Study revealed that hypoxia inducible factor-1 (HIF-1) was the main mediator in response towards the hypoxia. After being released, VEGF would then bind to VEGFR which consisted of VEGFR1 and VEGFR2 and further cause the activation of VEGF/VEGFR axis which stimulated tyrosine kinase pathway.14
Clinical implication of this study results is very important because it provides evidence that examination of serum VEGF level in HCC which is supported by physical examination, liver function test, and USG, we can predict the severity of HCC
based on BCLC classification. Hence, we can plan
the appropriate further management in HCC patients, particularly for internists who work far from referral hospital. In this study, we did not find any HCC subject with stage 0 BCLC. This happened because patients came with the tumour size of more than 2 cm. Meanwhile, there were only 10 subjects with initial
stage (A) BCLC in this study. These findings were
different from the study performed by Kaseb et al.15 In 2010, there were a total of 288 subjects, of which 21 subjects had stage 0 BCLC.
Other differences were also seen in the cause of HCC in this study. The most common cause HCC in this study was hepatitis B infection, different from the study conducted by Kaseb et al.24 In 2011, the most common cause of HCC was hepatitis C infection. Percentage of HCC which was complicated by liver cirrhosis was not different from this study. Yegin et al in 2013 stated that HCC often found in later stage, which was seen by the high rate of portal vein thrombus or
even stage C and D based on BCLC classification.16
of HCC based on BCLC classification. Serum VEGF
level increased in accordance to HCC severity based
on BCLC classification, particularly for stage B and
above. Further, in post hoc analysis, we found there
were no significant difference between stage A and B
and between stage B and C BCLC. There were only
significant differences in the average of VEGF levels
between stage A and C, stage A and D, stage B and D, and stage C and D. Therefore, we can predict the prognosis and further therapy in HCC patients. The results of this study was in accordance with the study performed by Kaseb et al in 288 HCC subjects, in
which there was significant difference in serum VEGF level in every degree of BCLC classification.15 A study
conducted by Yegin et al towards 78 HCC subjects
also revealed that there was no significant difference
in the serum VEGF level between stage A and B and
between stage B and C and D, but there was significant
difference of serum VEGF level between stage A and C and D.16
Another study conducted by Abdelbaki et al towards 40 HCC subjects, with control groups consisted of 40 healthy individuals and 40 subjects with liver cirrhosis in the other group, reported that the results of serum
VEGF in stage A BCLC was significantly different to stage B BCLC, and stage B was significantly different
towards stage C and D. Additionally, it was also found
that the higher the classification of BCLC was, the higher the serum VEGF level. Significant different
results were also found in serum VEGF level of HCC subjects with liver cirrhosis and healthy individuals.17
However, this was not in line with the study results of Gadelhak et al in their study towards 94 subjects, consisting of 67 HCC subjects and 27 cirrhosis subjects.
In this study, there was no significant difference in
serum VEGF levels between HCC severities based
on BCLC classification. This was thought to happen
because in the study performed by Gadelhak et al, most tumours have reached 50% of the liver size.18
Increased serum VEGF level could happen as a marker of vascular invasion, metastasis, and possibility of tumour recurrence after resection have been performed, causing the high serum VEGF level as a poor prognosis predictor in HCC. Therefore, the serum VEGF level was associated with the low rate of survival and disease-free survival.11,12,13
In this study, 20 HCC subjects were found to have portal vein thrombus (32.8%), with the average of serum VEGF level of 1048.21+741.07 pg/ml. Ghonaim et al19 in 2013 conducted a study towards 25 HCC patients and found 9 (36%) subjects with portal
vein thrombus with the average serum VEGF level of 2300+600 pg/mL. Difference in these results was possibly caused by the average larger size of HCC in the study conducted by Ghonaim et al.
Based on the results of statistical test above, anti-VEGF or VEGFR inhibitor (receptor) seemed to be potential to become a treatment of choice in
HCC with stage B BCLC classification. Sorafenib
was a monoclonal antibody acting as a tyrosine kinase (VGEFR) inhibitor. This drug could be used as a monotherapy in HCC or in combination with transarterial chemoembolization (TACE) in stage B BCLC; other drugs which could be used were bevacizumab, a monoclonal antibody that acted as an anti-VEGF.7,20 Abdel-Rahman et al performed a meta-analysis to 11 studies found that combination of TACE and Sorafenib were much better compared to monotherapy of TACE or Sorafenib alone. Administration of tyrosine kinase inhibitor or anti-VEGF in patients who received TACE had a vast
benefits, seen from several cases in which TACE
had been performed, there were continuous increase of VEGF following 7 days post TACE. Because the increase of VEGF was a marker of worsening condition, sorafenib or bevacizumab was expected to be able to suppress VEGF and improved liver condition.14,21,22
Limitations of this study were small sample size, no stage 0 BCLC was found. The correlation obtained was only in one period of time. This is different with other studies which included larger sample size and found subjects with stage 0 BCLC.
CONCLUSION
We found increased of serum VEGF level in accordance with HCC severity based on BCLC classification, particularly for stage B BCLC and above. Serum VEGF level was associated with HCC severity based on BCLC classification. Increased serum VEGF level may reveal the poor prognosis in HCC patients, therefore holistic and comprehensive management are needed.
REFERENCES
1. Budihusodo U. Karsinoma Hati. In: Sudoyo AW, Setiyohadi B, Alwi I, Simadibrata M, Setiati S, eds. Buku Ajar Ilmu Penyakit Dalam. 5th ed. Jakarta: Interna Publ 2009.p.685-91.
3. Omata M, Lesmana LA, Tateishi R, Chen PJ, Ling SM,
Yoshida H, et al. Asian Pacific Association for the Study of
the Liver Consensus Recommendations on Hepatocellular Carcinoma. Jakarta: Perhimpunan Peneliti Hati Indonesia, 2010.
4. Sanyal AJ, Yoon SK, Lencioni R. The etiology of hepatocellular carcinoma and consequences for treatment. Oncologist 2010;15:14- 22.
5. Marrero JA. Epidemiology of hepatocellular carcinoma and cholangiocarcinoma. In: Hussain HK, Francis IR, eds. Primary Carcinomas of The Liver. Cambridge: Cambridge University Press 2010.p.1-9
6. Dancygier H. Hepatocellular Carcinoma. In: Dancygier H, eds. Clinical Hepatology – Principles and Practice of Hepatobiliary Diseases. 2nded. Berlin: Springer-Verlag 2010.p.1307-12. 7. Bruix J, Sherman M. Management of hepatocellular
carcinoma: an update. Hepatology 2011;53:1020-2. 8. Farhat. VEGF pada karsinoma nasofaring. Majalah Kedokteran
Nusantara 2009;42:59-65.
9. Schoenleber SJ, Kurtz DM, Talwalkar JA, Roberts LR, Gores GJ. Prognostic role of vascular endothelial growth factor in hepatocellular carcinoma: systematic review and meta-analysis. Br J Cancer 2009;100:1385-92.
10. Poon RT, Lau C, Pang R, Ng KK, Yuen J, Fan ST. High serum vascular endothelial growth factor levels predict poor prognosis after radiofrequency ablation of hepatocellular carcinoma: importance of tumor biomarker in ablative therapies. Ann Surg Oncol 2007;14:1835-45.
11. Zhan P, Qian Q, Yu LK. Serum VEGF level is associated with the outcome of patients with hepatocellular carcinoma: a meta-analysis. Hepatobiliary Surg Nutr 2013;2:209-15.
12. Mukozu T, Nagai H, Matsui D, Kanekawa T, Sumino Y. Serum VEGF as a tumor marker in patients with HCV-related liver cirrhosis and hepatocellular carcinoma. Anticancer Res 2013;33:1013-22.
13. Strauss L, Volland D, Kunkel M, Reichert TE. Dual role of VEGF family members in the pathogenesis of head and neck cancer (HNSCC): possible link between angiogenesis and immune tolerance. Med Sci Monit 2005;11: 280-92.
14. Kaseb AO, Hanbali A, Cotant M, Hassan MM, Wollner I, Philip PA. Vascular endothelial growth factor in the management of hepatocellular carcinoma: a review of literature. Cancer 2009;115:4895-906.
15. Kaseb AO, Hassan MM, Lin E, Xiao L, Kumar V, Pathak P, et al. V- CLIP: integrating plasma vascular endothelial growth factor into a new scoring system to stratify patients with advanced hepatocellular carcinoma for clinical trials. Cancer 2011;117:2478-88.
16. Yegin EG, Siykhymbayev A, Eren F, Bekiroglu N, Ozdogan OC. Prognostic implication of serum vascular endothelial growth factor in advanced hepatocellular carcinoma staging. Ann Hepatol 2013;12:915-25.
17. Abdelbaki L, Gizawy SE, Abdalazeem K, Hafez MZE, Bakry R, El- Gezawy EM et al. Serum vascular endothelial growth factor and angiostatin as potential markers in patients with hepatocellular carcinoma. Life Sci J 2012;9:3846-51. 18. Gadelhak NA, Gadelhak SA, El-Morsi DA, Abdelaziz MM,
Abbas AT. Prognostic significance of three hepatitis markers
(p53 antibodies, vascular endothelial growth factor and alpha-feto protein) in patients with hepatocellular carcinoma. Mansoura J Forensic Med Clin Toxicol 2007;15:61-78.
19. Ghonaim M and El-Edel R. Significance of serum vascular
endothelial growth factor in chronic liver disease and hepatocellular carcinoma: an exploratory study. Ibnosina J Med BS 2013;5:288-95.
20. Tabernero J. The role of VEGF and EGFR inhibition: implications for combining anti-VEGF and anti-EGFR agents. Mol Cancer Res 2007;5:203-20.
21. Abdel RO, Elsayed ZA. Combination trans arterial chemoembolization (TACE) plus sorafenib for the management of unresectable hepatocellular carcinoma: a systematic review of the literature. Dig Dis Sci 2013;58:3389-96.