South-East Asia Region (SEAR)
I. GBV CHALLENGE:
Gender-based violence is an act “that results in, or is likely to result in, physical, sexual
or psychological harm or suffering to women, including threats of such acts, coercion
or arbitrary deprivations of liberty, whether occurring in public or private life.”
- The United Nations Declaration on Violence Against Women.
The South-East Asia Region between 40-49 years could be faces a big challenge in subject to GBV from their eliminating gender-based intimate partners/ husbands. violence (GBV). Almost all GBV has also been found to Member States in the Region be prevalent among persons have highlighted GBV as a living with HIV and AIDS
public health problem. and disabilities with women
Regional Milestones
areas of surveillance, research, prevention, treatment and care for victims and advocacy ! SEARO policy brief on prevention of GBV for the prevention of violence.was developed in Kuta, Bali, July 2007. It
! WHO’s integrated plan of action for a includes (1) development of gender-sensitive
science-based public health approach to assessment tools of evidence and prevention;
violence prevention was endorsed in World (2) harmonization of related laws; (3)
Health Assembly resolution WHA 50.19 in systematic data collection on violence against
1997. w o m e n ( V A W ) ; ( 4 ) i m p r o v e
coordination/networking among ministries/ ! The Forty-ninth World Health Assembly stakeholders; (5) ensure adequate funds to resolution (WHA 49.25, 1996) declared support awareness, protection and prevention violence to be a leading worldwide public activities and (6) a high level of political health problem.
commitment.
! The Beijing Platform for Action (BPFA), ! The World Health Assembly has urged 1995 identified violence against women as WHO's Member States to pay increased one of the 12 areas of concern for women’s attention to gender-based violence as a public advancement.
health concern during disasters and crises.
! The Convention on the Elimination of All [Resolution WHA 58.1 (2005)]
Forms of Discrimination against Women
! The 111th session of WHO Executive Board (CEDAW), adopted in 1979 by the UN
in January 2003 endorsed the need for General Assembly defines discrimination developing guidelines for each of the against women in Article 1 and includes
recommendations and by strengthening gender-based violence.
efforts for prevention of violence and injuries. ! The 109th session of the WHO Executive
Board in January 2002 proposed tasks in the
WHO and partners are collaborating to decrease ! Disseminating information to countries and GBV through initiatives that help to identify, supporting national efforts to advance quantify and respond to the problem, including: women's rights and prevent violence.
! Building evidence on the scope and types of ! Collaborating with international agencies and
violence in different settings. organizations to deter violence against
women globally. ! Developing guidance for Member States and
health professionals to prevent violence and strengthen health sector responses to it.
II. WHO RESPONSE ON GBV
Gender and Women's Health Unit, SEARO seeks lifespan. GWH-SEARO is supporting Member to integrate gender concerns into policy and States in the development of policies, strategies programmes in the health and related sectors and and interventions that effectively address high-to promote increased attention high-to the health and priority and neglected health issues of women. It human rights of women throughout their is also supporting the creation of a body of
III. REGIONAL ACTIVITIES FOR COMBATING GBV
evidence on the impact of gender on health and Director, South-East Asia Region gave a of tools, norms and standards to improve the special message on ‘GBV primary gender responsiveness of health interventions prevention’.
and promote gender equity in health.
A multi-sectoral approach to combating GBV in ! International Women's Day (IWD) is marked
th
the Region has been promoted since 2008. A on March 8 every year to celebrate the regional consultation on a multi-sectoral economic, political and social achievements approach to gender and women health work was of women. The United Nations has celebrated attended by 10 Member States of the Region in International Women’s Day since 1975. IWD Colombo, Sri Lanka in 2008. Various GBV is part of the growing international women's activities have been included in the regional movement, which has been strengthened by
programme budget workplans. four global United Nations women's
conferences. The Day also provides an opportunity to reflect on the progress made, to call for change and to celebrate acts of GWH/SEARO has developed IEC materials for courage and determination by ordinary
the SEARO website to commemorate women who have played an extraordinary
international days (1) 16 days of activism against role in the history of women's rights. gender violence, 5 November – 10 December
! SEARO uses this international observance for yearly; and (2) International Women’s Day
highlighting the progress made by the (IWD) on 8 March yearly.
countries in supporting gender equality and The 16 days of activism against gender health equity.
violence:
! SEARO has published “International
! The 16 days of activism against gender Women’s day highlights 2007-2009” as violence is an international campaign documentation of website posting during originating from the First Women's Global 2007-2009. In 2009, Regional Director Leadership Institute sponsored by the Centre SEARO gave special message on the theme: for Women's Global Leadership in 1991. ‘Men and women united to end violence Participants chose the period 25 November – against women and girls’.
10 December, based on November 25 as International Day against Violence against Women and December 10, as International
Human Rights Day, in order to symbolically ! The development of multi-sectoral gender-link violence against women and human based violence prevention guidelines to rights and to emphasize that such violence is support One-Stop Crisis Centre (OSCC) in
a violation of human right. Thailand, has been finalized in 2009 by the
! SEARO uses this international observance for collaborative work of WHO regional and joint country activities and for evaluation of country offices with Ministry of Public the gender-based violence (GBV) situation Health, Thailand.
and efforts in the SEA Region through ! A policy dialogue on Gender Mainstreaming website posting, development of analysis and (GMS) in health with multi-sectoral approach publication to combat GBV in the Region. with Ministry of Health and Ministry of ! SEARO has published “Combating gender- Women and Child Development on
Gender-based violence (GBV) in the South-East Asia Based Violence has been initiated in India by
Region, 2009, as documentation of highlights collaborative work of NGO and WHO
2006-2008 messages on the website for the regional and country offices. above commemoration. In 2009, the Regional
International Women’s Day (IWD)
A. Information, education and
communication (IEC)
Regional Milestones
areas of surveillance, research, prevention, treatment and care for victims and advocacy ! SEARO policy brief on prevention of GBV for the prevention of violence.was developed in Kuta, Bali, July 2007. It
! WHO’s integrated plan of action for a includes (1) development of gender-sensitive
science-based public health approach to assessment tools of evidence and prevention;
violence prevention was endorsed in World (2) harmonization of related laws; (3)
Health Assembly resolution WHA 50.19 in systematic data collection on violence against
1997. w o m e n ( V A W ) ; ( 4 ) i m p r o v e
coordination/networking among ministries/ ! The Forty-ninth World Health Assembly stakeholders; (5) ensure adequate funds to resolution (WHA 49.25, 1996) declared support awareness, protection and prevention violence to be a leading worldwide public activities and (6) a high level of political health problem.
commitment.
! The Beijing Platform for Action (BPFA), ! The World Health Assembly has urged 1995 identified violence against women as WHO's Member States to pay increased one of the 12 areas of concern for women’s attention to gender-based violence as a public advancement.
health concern during disasters and crises.
! The Convention on the Elimination of All [Resolution WHA 58.1 (2005)]
Forms of Discrimination against Women
! The 111th session of WHO Executive Board (CEDAW), adopted in 1979 by the UN
in January 2003 endorsed the need for General Assembly defines discrimination developing guidelines for each of the against women in Article 1 and includes
recommendations and by strengthening gender-based violence.
efforts for prevention of violence and injuries. ! The 109th session of the WHO Executive
Board in January 2002 proposed tasks in the
WHO and partners are collaborating to decrease ! Disseminating information to countries and GBV through initiatives that help to identify, supporting national efforts to advance quantify and respond to the problem, including: women's rights and prevent violence.
! Building evidence on the scope and types of ! Collaborating with international agencies and
violence in different settings. organizations to deter violence against
women globally. ! Developing guidance for Member States and
health professionals to prevent violence and strengthen health sector responses to it.
II. WHO RESPONSE ON GBV
Gender and Women's Health Unit, SEARO seeks lifespan. GWH-SEARO is supporting Member to integrate gender concerns into policy and States in the development of policies, strategies programmes in the health and related sectors and and interventions that effectively address high-to promote increased attention high-to the health and priority and neglected health issues of women. It human rights of women throughout their is also supporting the creation of a body of
III. REGIONAL ACTIVITIES FOR COMBATING GBV
evidence on the impact of gender on health and Director, South-East Asia Region gave a of tools, norms and standards to improve the special message on ‘GBV primary gender responsiveness of health interventions prevention’.
and promote gender equity in health.
A multi-sectoral approach to combating GBV in ! International Women's Day (IWD) is marked
th
the Region has been promoted since 2008. A on March 8 every year to celebrate the regional consultation on a multi-sectoral economic, political and social achievements approach to gender and women health work was of women. The United Nations has celebrated attended by 10 Member States of the Region in International Women’s Day since 1975. IWD Colombo, Sri Lanka in 2008. Various GBV is part of the growing international women's activities have been included in the regional movement, which has been strengthened by
programme budget workplans. four global United Nations women's
conferences. The Day also provides an opportunity to reflect on the progress made, to call for change and to celebrate acts of GWH/SEARO has developed IEC materials for courage and determination by ordinary
the SEARO website to commemorate women who have played an extraordinary
international days (1) 16 days of activism against role in the history of women's rights. gender violence, 5 November – 10 December
! SEARO uses this international observance for yearly; and (2) International Women’s Day
highlighting the progress made by the (IWD) on 8 March yearly.
countries in supporting gender equality and The 16 days of activism against gender health equity.
violence:
! SEARO has published “International
! The 16 days of activism against gender Women’s day highlights 2007-2009” as violence is an international campaign documentation of website posting during originating from the First Women's Global 2007-2009. In 2009, Regional Director Leadership Institute sponsored by the Centre SEARO gave special message on the theme: for Women's Global Leadership in 1991. ‘Men and women united to end violence Participants chose the period 25 November – against women and girls’.
10 December, based on November 25 as International Day against Violence against Women and December 10, as International
Human Rights Day, in order to symbolically ! The development of multi-sectoral gender-link violence against women and human based violence prevention guidelines to rights and to emphasize that such violence is support One-Stop Crisis Centre (OSCC) in
a violation of human right. Thailand, has been finalized in 2009 by the
! SEARO uses this international observance for collaborative work of WHO regional and joint country activities and for evaluation of country offices with Ministry of Public the gender-based violence (GBV) situation Health, Thailand.
and efforts in the SEA Region through ! A policy dialogue on Gender Mainstreaming website posting, development of analysis and (GMS) in health with multi-sectoral approach publication to combat GBV in the Region. with Ministry of Health and Ministry of ! SEARO has published “Combating gender- Women and Child Development on
Gender-based violence (GBV) in the South-East Asia Based Violence has been initiated in India by
Region, 2009, as documentation of highlights collaborative work of NGO and WHO
2006-2008 messages on the website for the regional and country offices. above commemoration. In 2009, the Regional
International Women’s Day (IWD)
A. Information, education and
communication (IEC)
C. Supporting the development of
One-Millennium Development Goals including those related to education, maternal health, child mortality, universal primary education and others. GWH/SEARO promotes ! One-Stop Crisis Centre (OSCC) is a patient awareness on “investing in women and centered management centre characterized by girls”, The Region has also promoted an integrated and coordinated teamwork of awareness on “Ending impunity for violence multisectoral and interagency network for the against women and girls”. through message management of woman and child victims of on IWD.
violence and trafficking.
! An OSCC ideally adopts a three-prong approach- primary, secondary and tertiary in
! Primary prevention of GBV is done through advocating the prevention of domestic
early education for adolescents and gender violence. OSCC ensures existence of support
awareness campaigns for public. Primary for the survivors from all relevant sections
prevention for GBV needs to be started for and agencies through good networking and
schools and in the community to complement collaboration with various related
inter-the health sector’s response to secondary agencies such as social welfare, shelter, legal
prevention. aid assistance, court procedure, police
service, etc. As a result, victims have access ! The Regional Director, WHO, South-East to immediate services and assistance. Asia Region has stated in his message on IWD 2009 that primary prevention for GBV ! OSCCs have been implemented in the Region
needs to be started at schools and community to help victims of violence through hospital-
in complementing the health sector’s based activities. OSCCs are operational in
response to secondary prevention. Reviewing Bangladesh, Indonesia, Nepal, Sri Lanka and
the role of family protection units to support Thailand.
victim’s protection/ prevention and producing information, education and communication (IEC) material for the community are
! GWH-SEARO promotes integration of considered important to combat GBV.
gender perspectives into policies and
! SEARO launched a policy brief on
programmes in order to achieve the prevention of GBV in 2007. The policy brief
Millennium Development Goals, particularly on prevention of GBV from countries were Goal 3, on gender equality and women’s agreed to by 10 Member States in Kuta, Bali
empowerment. The MDG3 has been used as in July 2007. One of the recommendations of
referral to support GBV programmes and the policy brief was to ensure adequate funds activities in the region, including gender to support the awareness, protection and sensitive health care (GSHC). GSHC is prevention activities for GBV.
developed in Nepal for helping victims of
! Primary prevention of GBV is performed in GBV.
the region by Bangladesh, Indonesia, Nepal ! Investing in women and girls has a multiplier and Thailand through IEC material for
effect on productivity, efficiency, sustained schools. economic growth and family welfare and will
contribute to the achievement of the
IV. COUNTRIES’ EFFORTS IN COMBATING GBV
GWH-SEARO developed a questionnaire on Legislations/Policies/Programmes (2) Resources GBV in October 2009. (Annex 1). The (3) Research and (4) Evidence. The responses questionnaire was circulated among all the 11 received from 10 Member Countries - gender focal points of the 11 Member Countries Bangladesh, Bhutan, India, Indonesia, Maldives, of SEA Region. The questionnaire contains Myanmar, Nepal, Sri Lanka, Thailand and 23 questions under 4 clusters: (1) Timor-Leste.
A. Efforts of Member Countries in Combating GBV
3
Bangladesh India Indonesia Maldives Myanmar Nepal Sri Lanka Thailand Timor-Leste
Scale*
Legislation/policies/programmes Resources Research Evidence
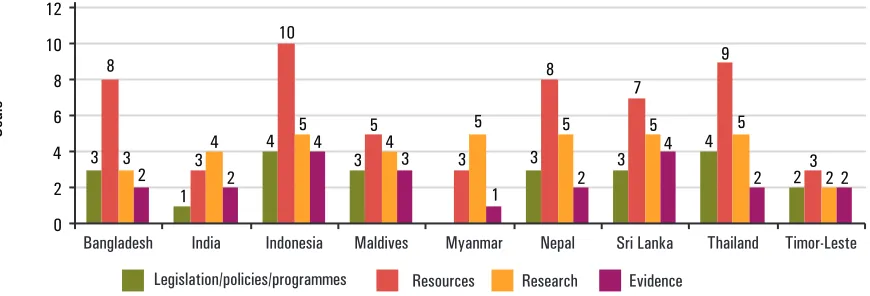
Figure 1: Efforts of Member Countries in Combating GBV, 2009
* The scale represents country-specific situation ! National action plan on GBV is present in 6 plotted against the maximum rating for 4 clusters countries: Bangladesh, Indonesia, Maldives, of indicators: (1) Legislations / policies / Nepal, Thailand and Timor-Leste. Bhutan has programmes (2) Resource (3) Research and (4) national plan of action for gender.
Evidence ! A health policy on GBV is present in 5
countries: Indonesia, Maldives, Nepal, Sri Lanka and Thailand.
! Multi-sectoral action plan is present in 5 There are 9 Member States who have some form
countries: Bangladesh, Indonesia, Maldives, of legislation, policies and programmes for
Sri Lanka and Thailand. combating GBV (Figure 1); though only 5
countries put special attention in health policy. Further analysis showed that although having
! 9 Member Countries of the Region have National action plan on GBV, Nepal and Timor resources on GBV in various forms.
Leste do not put it as multi-sectoral activity yet.
! Specific guidelines on GBV for health ! Legislation on GBV is present in 7 countries: providers are present in Indonesia, Nepal, Sri
Bangladesh, India, Indonesia, Nepal, Sri Lanka and Thailand. Lanka, Thailand and Timor-Leste.
Legislations / policies / programmes for
combating GBV
C. Supporting the development of
One-Millennium Development Goals including those related to education, maternal health, child mortality, universal primary education and others. GWH/SEARO promotes ! One-Stop Crisis Centre (OSCC) is a patient awareness on “investing in women and centered management centre characterized by girls”, The Region has also promoted an integrated and coordinated teamwork of awareness on “Ending impunity for violence multisectoral and interagency network for the against women and girls”. through message management of woman and child victims of on IWD.
violence and trafficking.
! An OSCC ideally adopts a three-prong approach- primary, secondary and tertiary in
! Primary prevention of GBV is done through advocating the prevention of domestic
early education for adolescents and gender violence. OSCC ensures existence of support
awareness campaigns for public. Primary for the survivors from all relevant sections
prevention for GBV needs to be started for and agencies through good networking and
schools and in the community to complement collaboration with various related
inter-the health sector’s response to secondary agencies such as social welfare, shelter, legal
prevention. aid assistance, court procedure, police
service, etc. As a result, victims have access ! The Regional Director, WHO, South-East to immediate services and assistance. Asia Region has stated in his message on IWD 2009 that primary prevention for GBV ! OSCCs have been implemented in the Region
needs to be started at schools and community to help victims of violence through hospital-
in complementing the health sector’s based activities. OSCCs are operational in
response to secondary prevention. Reviewing Bangladesh, Indonesia, Nepal, Sri Lanka and
the role of family protection units to support Thailand.
victim’s protection/ prevention and producing information, education and communication (IEC) material for the community are
! GWH-SEARO promotes integration of considered important to combat GBV.
gender perspectives into policies and
! SEARO launched a policy brief on
programmes in order to achieve the prevention of GBV in 2007. The policy brief
Millennium Development Goals, particularly on prevention of GBV from countries were Goal 3, on gender equality and women’s agreed to by 10 Member States in Kuta, Bali
empowerment. The MDG3 has been used as in July 2007. One of the recommendations of
referral to support GBV programmes and the policy brief was to ensure adequate funds activities in the region, including gender to support the awareness, protection and sensitive health care (GSHC). GSHC is prevention activities for GBV.
developed in Nepal for helping victims of
! Primary prevention of GBV is performed in GBV.
the region by Bangladesh, Indonesia, Nepal ! Investing in women and girls has a multiplier and Thailand through IEC material for
effect on productivity, efficiency, sustained schools. economic growth and family welfare and will
contribute to the achievement of the
IV. COUNTRIES’ EFFORTS IN COMBATING GBV
GWH-SEARO developed a questionnaire on Legislations/Policies/Programmes (2) Resources GBV in October 2009. (Annex 1). The (3) Research and (4) Evidence. The responses questionnaire was circulated among all the 11 received from 10 Member Countries - gender focal points of the 11 Member Countries Bangladesh, Bhutan, India, Indonesia, Maldives, of SEA Region. The questionnaire contains Myanmar, Nepal, Sri Lanka, Thailand and 23 questions under 4 clusters: (1) Timor-Leste.
A. Efforts of Member Countries in Combating GBV
3
Bangladesh India Indonesia Maldives Myanmar Nepal Sri Lanka Thailand Timor-Leste
Scale*
Legislation/policies/programmes Resources Research Evidence
Figure 1: Efforts of Member Countries in Combating GBV, 2009
* The scale represents country-specific situation ! National action plan on GBV is present in 6 plotted against the maximum rating for 4 clusters countries: Bangladesh, Indonesia, Maldives, of indicators: (1) Legislations / policies / Nepal, Thailand and Timor-Leste. Bhutan has programmes (2) Resource (3) Research and (4) national plan of action for gender.
Evidence ! A health policy on GBV is present in 5
countries: Indonesia, Maldives, Nepal, Sri Lanka and Thailand.
! Multi-sectoral action plan is present in 5 There are 9 Member States who have some form
countries: Bangladesh, Indonesia, Maldives, of legislation, policies and programmes for
Sri Lanka and Thailand. combating GBV (Figure 1); though only 5
countries put special attention in health policy. Further analysis showed that although having
! 9 Member Countries of the Region have National action plan on GBV, Nepal and Timor resources on GBV in various forms.
Leste do not put it as multi-sectoral activity yet.
! Specific guidelines on GBV for health ! Legislation on GBV is present in 7 countries: providers are present in Indonesia, Nepal, Sri
Bangladesh, India, Indonesia, Nepal, Sri Lanka and Thailand. Lanka, Thailand and Timor-Leste.
Legislations / policies / programmes for
combating GBV
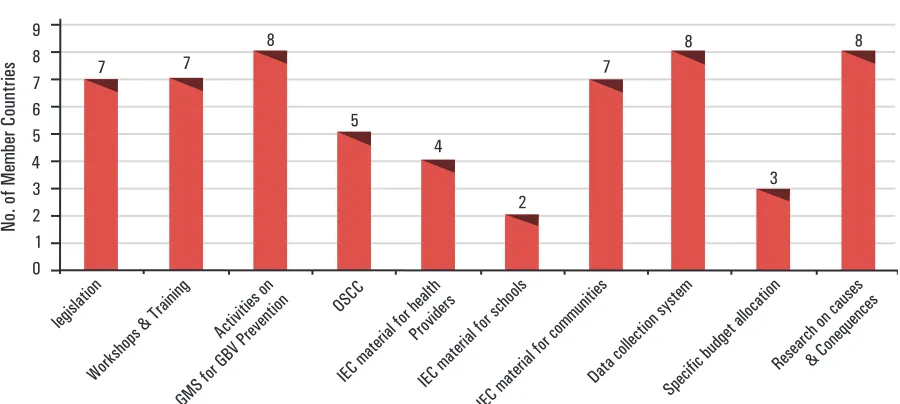
! Workshops and trainings on GBV for ! Facilities for helping the victims of GBV
health providers have been conducted in (such as police stations, legal aids centres, Bangladesh, Indonesia, Maldives, Myanmar, social support groups, shelter homes, Nepal, Sri Lanka and Thailand. (Figure 2) counseling centres, religious leaders’ groups, community leaders’ groups and self-help ! Activities on gender mainstreaming for the
groups) are present in 9 member countries - prevention of GBV have been carried out in
Bangladesh, India, Indonesia, Maldives, Bangladesh, India, Indonesia, Maldives,
Myanmar, Nepal, Sri Lanka, Thailand and Nepal, Sri Lanka, Thailand and Timor-Leste.
Timor Leste. (Figure 2)
! A specific budget allocation for GBV is ! One-Stop Crisis Centre services (OSCC)
present in Indonesia, Maldives and Thailand. for victims of GBV are present in
(Figure 2) Bangladesh, Indonesia, Nepal, Sri Lanka and
Thailand. (Figure 2)
! Data collection system for GBV [Hospitals, ! Research on the cause and consequences of NGOs Legal aids centres, Social support GBV have been conducted in Bangladesh, centers and Police stations] exists in India, Indonesia, Maldives, Myanmar, Nepal, Bangladesh, India, Indonesia, Maldives, Sri Lanka and Thailand. (Figure 2)
Myanmar, Nepal, Sri Lanka and Thailand.
! Research on the costs of GBV has been
(Figure 2) conducted in Indonesia and Thailand.
! IEC materials on GBV for health
! Research on the effective prevention
providers are available in Bangladesh, measures for GBV has been conducted in Indonesia, Nepal and Thailand. (Figure 2) Indonesia, Nepal and Sri Lanka.
! IEC materials on GBV for schools are available in Bangladesh and Indonesia.
! The practice of female foeticide is present in (Figure 2)
India. ! IEC materials on GBV for communities are
! The practice of female genital mutilation/ available in Bangladesh, India, Indonesia,
cutting (FGM/C) is present in Indonesia and Nepal, Sri Lanka, Thailand and Timor Leste.
Sri Lanka. (Figure 2)
Research on GBV
Evidence on GBV
B. Profile of Member Countries related to GBV
7 7
Research on causes & Conequences
No. of Member Countries
Figure 2: Profile of Member Countries on some of the activities related to GBV, 2009 * The score for female genital mutilation in Sri Lanka is zero according to The global gender gap report 2009, Geneva.
C. Country Indication on GBV
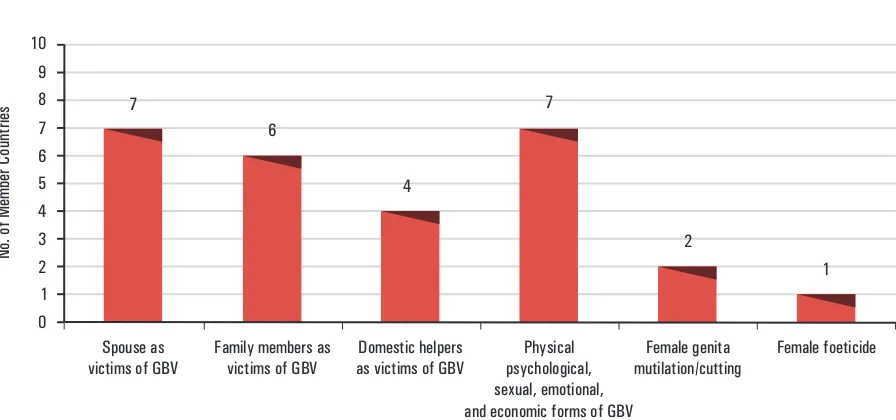
! Most of the Member Countries have spouse genital mutilation/cutting is practiced in as the victims of GBV. GBV is mostly Indonesia and Sri Lanka * and female present in physical, psychological, sexual, foeticide is practiced in India (Figure 3) emotional and economic forms. Female
Spouse as
victims of GBV Family members as victims of GBV as victims of GBVDomestic helpers psychological,Physical sexual, emotional, and economic forms of GBV
Female genita
Figure 3:Number of Member Countries with victims of GBV, forms of GBV, female genital mutilation/cutting and female foeticide, 2009
4 women in the public arena
Joblessness Jealously
! Workshops and trainings on GBV for ! Facilities for helping the victims of GBV
health providers have been conducted in (such as police stations, legal aids centres, Bangladesh, Indonesia, Maldives, Myanmar, social support groups, shelter homes, Nepal, Sri Lanka and Thailand. (Figure 2) counseling centres, religious leaders’ groups, community leaders’ groups and self-help ! Activities on gender mainstreaming for the
groups) are present in 9 member countries - prevention of GBV have been carried out in
Bangladesh, India, Indonesia, Maldives, Bangladesh, India, Indonesia, Maldives,
Myanmar, Nepal, Sri Lanka, Thailand and Nepal, Sri Lanka, Thailand and Timor-Leste.
Timor Leste. (Figure 2)
! A specific budget allocation for GBV is ! One-Stop Crisis Centre services (OSCC)
present in Indonesia, Maldives and Thailand. for victims of GBV are present in
(Figure 2) Bangladesh, Indonesia, Nepal, Sri Lanka and
Thailand. (Figure 2)
! Data collection system for GBV [Hospitals, ! Research on the cause and consequences of NGOs Legal aids centres, Social support GBV have been conducted in Bangladesh, centers and Police stations] exists in India, Indonesia, Maldives, Myanmar, Nepal, Bangladesh, India, Indonesia, Maldives, Sri Lanka and Thailand. (Figure 2)
Myanmar, Nepal, Sri Lanka and Thailand.
! Research on the costs of GBV has been
(Figure 2) conducted in Indonesia and Thailand.
! IEC materials on GBV for health
! Research on the effective prevention
providers are available in Bangladesh, measures for GBV has been conducted in Indonesia, Nepal and Thailand. (Figure 2) Indonesia, Nepal and Sri Lanka.
! IEC materials on GBV for schools are available in Bangladesh and Indonesia.
! The practice of female foeticide is present in (Figure 2)
India. ! IEC materials on GBV for communities are
! The practice of female genital mutilation/ available in Bangladesh, India, Indonesia,
cutting (FGM/C) is present in Indonesia and Nepal, Sri Lanka, Thailand and Timor Leste.
Sri Lanka. (Figure 2)
Research on GBV
Evidence on GBV
B. Profile of Member Countries related to GBV
7 7
Research on causes & Conequences
No. of Member Countries
Figure 2: Profile of Member Countries on some of the activities related to GBV, 2009 * The score for female genital mutilation in Sri Lanka is zero according to The global gender gap report 2009, Geneva.
C. Country Indication on GBV
! Most of the Member Countries have spouse genital mutilation/cutting is practiced in as the victims of GBV. GBV is mostly Indonesia and Sri Lanka * and female present in physical, psychological, sexual, foeticide is practiced in India (Figure 3) emotional and economic forms. Female
Spouse as
victims of GBV Family members as victims of GBV as victims of GBVDomestic helpers psychological,Physical sexual, emotional, and economic forms of GBV
Female genita
Figure 3:Number of Member Countries with victims of GBV, forms of GBV, female genital mutilation/cutting and female foeticide, 2009
4 women in the public arena
Joblessness Jealously
! Mental disturbances, disability and attempts related to women’s health after GBV in the suicide are some of the common findings Member Countries (Figure 5)
Mental
disturbances Suicide Attempts atsuicide miscamiangesAbortin and Disabilty Death 9
8 7 6 5 4 3 2 1 0 10
No. of Member Countries
8
4 4
6
7
5
Figure 5: Women’s health after GBV in the Member Countries, 2009
_
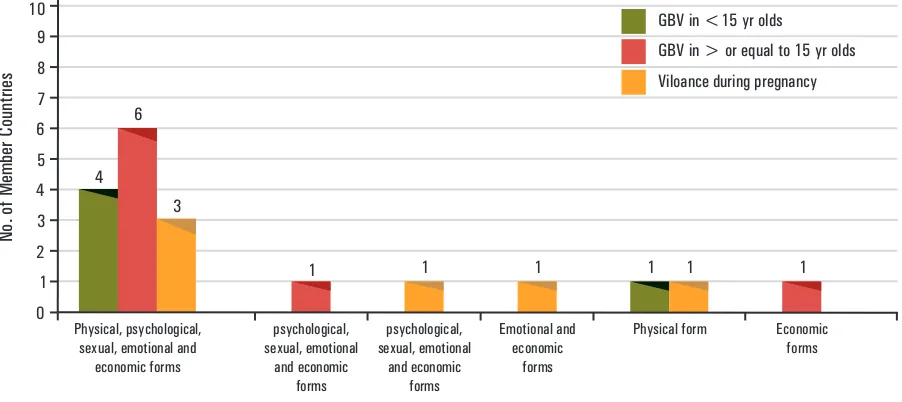
! Physical, psychological, sexual, emotional among > 15 year olds and in violence during and economic forms of GBV are present in pregnancy (Figure 6)
the Member Countries among <15 yr olds,
Physical, psychological, sexual, emotional and
economic forms 4
6
3
1 1 1 1 1 1
psychological, sexual, emotional
and economic forms
psychological, sexual, emotional
and economic forms
Emotional and economic
forms
Physical form Economic forms GBV in <15 yr olds
GBV in > or equal to 15 yr olds 9
8 7 6 5 4 3 2 1 0 10
No. of Member Countries
Viloance during pregnancy
Figure 6: Number of Member Countries with GBV in various forms, 2009
V. Conculsion
! WHO SEARO is combating Gender-Based
Violence in the region by promoting multi-sectoral activities for GBV primary prevention; and encouraging Member States in developing IEC materials; OSCC and related legislation/policy/ programme, research and training in relation to GBV. It is hoped that collaborative work among Gender, women and health with other technical units and country offices will become more productive in supporting all actions in combating and eliminating GBV in the South-East Asia Region.
! Mental disturbances, disability and attempts related to women’s health after GBV in the suicide are some of the common findings Member Countries (Figure 5)
Mental
disturbances Suicide Attempts atsuicide miscamiangesAbortin and Disabilty Death 9
8 7 6 5 4 3 2 1 0 10
No. of Member Countries
8
4 4
6
7
5
Figure 5: Women’s health after GBV in the Member Countries, 2009
_
! Physical, psychological, sexual, emotional among > 15 year olds and in violence during and economic forms of GBV are present in pregnancy (Figure 6)
the Member Countries among <15 yr olds,
Physical, psychological, sexual, emotional and
economic forms 4
6
3
1 1 1 1 1 1
psychological, sexual, emotional
and economic forms
psychological, sexual, emotional
and economic forms
Emotional and economic
forms
Physical form Economic forms GBV in <15 yr olds
GBV in > or equal to 15 yr olds 9
8 7 6 5 4 3 2 1 0 10
No. of Member Countries
Viloance during pregnancy
Figure 6: Number of Member Countries with GBV in various forms, 2009
V. Conculsion
! WHO SEARO is combating Gender-Based
Violence in the region by promoting multi-sectoral activities for GBV primary prevention; and encouraging Member States in developing IEC materials; OSCC and related legislation/policy/ programme, research and training in relation to GBV. It is hoped that collaborative work among Gender, women and health with other technical units and country offices will become more productive in supporting all actions in combating and eliminating GBV in the South-East Asia Region.
Sr.No. Don’t Know No Yes
I. Legislation on GBV
II. GBV–related policies/guidelines/ programmes and research
III. Facilities and resources for GBV
1. Domestic Violence Act / Bill/ related legal and judicial processes
1. National action plan on GBV If yes, please specify. Health policy on GBV
Multi-sectoral action plan on GBV
2. Specific guidelines for health providers on GBV interventions 3. Workshops/trainings on GBV for health providers
If Yes, please specify
No. of health providers trained/sensitized No. of workshops/trainings held
4. Activity / task on gender main streaming for prevention of GBV 5. Research on GBV
If yes, please specify if the finding been documented for the following: Cause and consequences of GBV
Costs of GBV
Effective prevention measures for GBV 6. Data collection system for GBV
If Yes, please specify. Hospitals
NGOs
Legal aids centres Social support centers Police stations
1. Use of One-Stop Crisis Centre services (OSCC) for GBV prevention and handling in health facility
2. IEC materials on GBV for health providers 3. IEC materials on GBV for schools 4. IEC materials on GBV for communities 5. Budget allocation for GBV in health facilities 6. Facilities for helping victims of GBV
If yes, please specify. Police department Legal aids centres Social support groups Shelter homes
Counseling centres Religious leaders’ groups Community leaders’ groups Self –help groups
Annex 1
GWH WHO/SEARO
Questionnaire
Country Situation on Gender-Based Violence (GBV)
Introduction
This questionnaire is aimed at collecting information on GBV from countries based on the documents, research and other relevant sources. Total questions of the four sections: 23; approximate time taken to complete the questionnaire: 20 minutes
Please kindly respond by putting a in one or more of the appropriate box or write in the spaces provided
Name of the country __________________
IV. GBV – specific details
1. Findings on GBV If Yes, please specify Spouse as victims Family members as victims Domestic helpers as victims 2. Findings on type of GBV
If Yes, please specify. Physical
Psychological Sexual Emotional Economical
3. Violence during pregnancy If Yes, please specify. Physical
Psychological Sexual Emotional Economical
4. GBV in less than 15 year olds If Yes, please specify. Physical
Psychological Sexual Emotional Economical
5. GBV in more than or equal to 15 year olds If Yes, please specify.
Physical Psychological Sexual Emotional Economical
6. Cases of female genital mutilation 7. Cases of female genital cutting 8. Cases of female foeticide
9. Findings related to the cause of GBV If Yes, please specify.
Increasing participation of women in the public arena Joblessness
Jealousy
Dowry-related issues Communication gap Customs
Patriarchal family systems
10. Findings related to women’s health after GBV If Yes, please specify.
Mental disturbances Suicide
Attempts at suicide Abortion and miscarriages Disability
Death
Thank you for taking the time to complete this questionnaire
Sr.No. Don’t Know No Yes
Sr.No. Don’t Know No Yes
I. Legislation on GBV
II. GBV–related policies/guidelines/ programmes and research
III. Facilities and resources for GBV
1. Domestic Violence Act / Bill/ related legal and judicial processes
1. National action plan on GBV If yes, please specify. Health policy on GBV
Multi-sectoral action plan on GBV
2. Specific guidelines for health providers on GBV interventions 3. Workshops/trainings on GBV for health providers
If Yes, please specify
No. of health providers trained/sensitized No. of workshops/trainings held
4. Activity / task on gender main streaming for prevention of GBV 5. Research on GBV
If yes, please specify if the finding been documented for the following: Cause and consequences of GBV
Costs of GBV
Effective prevention measures for GBV 6. Data collection system for GBV
If Yes, please specify. Hospitals
NGOs
Legal aids centres Social support centers Police stations
1. Use of One-Stop Crisis Centre services (OSCC) for GBV prevention and handling in health facility
2. IEC materials on GBV for health providers 3. IEC materials on GBV for schools 4. IEC materials on GBV for communities 5. Budget allocation for GBV in health facilities 6. Facilities for helping victims of GBV
If yes, please specify. Police department Legal aids centres Social support groups Shelter homes
Counseling centres Religious leaders’ groups Community leaders’ groups Self –help groups
Annex 1
GWH WHO/SEARO
Questionnaire
Country Situation on Gender-Based Violence (GBV)
Introduction
This questionnaire is aimed at collecting information on GBV from countries based on the documents, research and other relevant sources. Total questions of the four sections: 23; approximate time taken to complete the questionnaire: 20 minutes
Please kindly respond by putting a in one or more of the appropriate box or write in the spaces provided
Name of the country __________________
IV. GBV – specific details
1. Findings on GBV If Yes, please specify Spouse as victims Family members as victims Domestic helpers as victims 2. Findings on type of GBV
If Yes, please specify. Physical
Psychological Sexual Emotional Economical
3. Violence during pregnancy If Yes, please specify. Physical
Psychological Sexual Emotional Economical
4. GBV in less than 15 year olds If Yes, please specify. Physical
Psychological Sexual Emotional Economical
5. GBV in more than or equal to 15 year olds If Yes, please specify.
Physical Psychological Sexual Emotional Economical
6. Cases of female genital mutilation 7. Cases of female genital cutting 8. Cases of female foeticide
9. Findings related to the cause of GBV If Yes, please specify.
Increasing participation of women in the public arena Joblessness
Jealousy
Dowry-related issues Communication gap Customs
Patriarchal family systems
10. Findings related to women’s health after GBV If Yes, please specify.
Mental disturbances Suicide
Attempts at suicide Abortion and miscarriages Disability
Death
Thank you for taking the time to complete this questionnaire
Sr.No. Don’t Know No Yes
Further query please contact:
Gender, Women and Health (GWH)
Department of Health System Development
World Health Organization Regional Office for the South-East Asia Region
(WHO/SEARO)