Telomere attrition of the human abdominal aorta: relationships
with age and atherosclerosis
Koji Okuda
a, M. Yusuf Khan
b, Joan Skurnick
c, Masayuki Kimura
a, Hana Aviv
d,
Abraham Aviv
a,*
aHypertension Research Center,New Jersey Medical School,Uni6ersity of Medicine and Dentistry of New Jersey,185South Orange A6enue,
Newark,NJ07103-2714,USA
bDepartment of Pathology,New Jersey Medical School,Uni6ersity of Medicine and Dentistry of New Jersey,185South Orange A6enue,
Newark,NJ07103-2714,USA
cDepartment of Pre6enti6e Medicine and Community Health,New Jersey Medical School,Uni6ersity of Medicine and Dentistry of New Jersey,
185South Orange A6enue,Newark,NJ07103-2714,USA
dCenter of Human and Molecular Genetics,New Jersey Medical School,Uni6ersity of Medicine and Dentistry of New Jersey,
185South Orange A6enue,Newark,NJ07103-2714,USA
Received 15 March 1999; received in revised form 24 September 1999; accepted 3 November 1999
Abstract
Little is known about the turnover rate (i.e. the rate of replication and death) of cells in the intima and media of human arteries as a function of age and atherosclerosis. One indicator of the replicative history of cells is telomere length. In this work we explored the rate of telomere attrition as a function of age and atherosclerosis in cells of the human abdominal aorta. Telomere length, measured by the terminal restriction fragment using Southern analysis, was determined in the intima and media of the distal (infrarenal) versus proximal (suprarenal) segments of the abdominal aorta. Telomere length was then correlated with age and atherosclerotic grade. The rate of age-dependent telomere attrition was higher in both the intima and media of the distal versus proximal abdominal aorta. In addition, telomere length was negatively correlated with atherosclerotic grade. However, after adjustment for age, this relationship was not statistically significant. The high rate of age-dependent telomere attrition in the distal abdominal aorta probably reflects enhanced cellular turnover rate due to local factors such as an increase in shear wall stress in this vascular segment. © 1999 Elsevier Science Ireland Ltd. All rights reserved.
Keywords:Telomeres; Aorta; Human; Age; Atherosclerosis
www.elsevier.com/locate/atherosclerosis
1. Introduction
In industrialized societies, atherosclerosis progresses with age. The mechanisms that are responsible for this phenomenon have been the focus of intense investiga-tions for a number of decades (reviewed in [1,2]). An important question is whether the atherosclerotic pro-cess entails an increase in the turnover rate of cells of the intima and media, i.e. an increase in the rate of replication and death of endothelial and vascular smooth muscle cells of the arterial wall. One criterion of cellular replication is the rate of attrition
(shorten-ing) of telomeres, the ends of chromosomes. Due to the ‘end replication problem,’ telomeres undergo attrition with each replicative cycle of somatic cells (reviewed in [3,4]). Since telomere length is highly heritable [5], the two variables that determine the length of telomeres in cultures of somatic cells are the genetic endowment of these cells and their replicative history. However, telomeric length in somatic cells from humans inversely correlates not only with the replicative number in cul-ture [6 – 8] but also with the donor’s age [5 – 8], suggest-ing that telomere attrition, resultsuggest-ing from cellular replication, also occurs in vivo.
The present work has focused on age-dependent telomere attrition of the intima and media of the prox-imal (suprarenal) and distal (infrarenal) segments of the human abdominal aorta and their relationship to
* Corresponding author. Tel.: +1-973-9725280; fax: + 1-973-9725576.
E-mail address:[email protected] (A. Aviv).
atherosclerosis. These segments of the aorta were exam-ined because they are subjected to different levels of shear wall stress and express different degrees of atherosclerosis as a function of age [9,10]. Our findings indicate that age-dependent telomere attrition is faster in the distal than in proximal segment of the abdominal aorta and that atherosclerosis does not appear to accel-erate the rate of telomere attrition in the intima and media of these vascular segments.
2. Methods
2.1. Subjects
Aortic specimens were obtained from 51 subjects (23 males and 28 females, 37 White Americans, 14 African Americans) between ages of 1 month and 80 years. Vessels were obtained at autopsies, which were per-formed at the University Hospital by the Department of Pathology and the Union County Medical Examiner. Data summarizing the causes of death in this cohort are presented in Table 1. Tissues were obtained within 18 h after death. The bodies were maintained at 4°C until autopsy.
2.2. Isolation of the intima and media
Aortas, extending from the superior celiac artery to the common iliac bifurcation, were placed flat on a cardboard with the endothelial surface up. The aortas
were then frozen at −40°C for a period of 2 weeks to
2 months. Intima was isolated from the proximal part (extending from celiac artery to just proximal to renal arteries) and the distal part (extending from just past the renal arteries to bifurcation point of iliac arteries) of the abdominal aorta. This was done in a partially thawed state using a carbon steel round blade (Havel’s, Inc.). In this condition, the intima could be more readily separated from the underlying media. Specimens were placed in separately labeled containers. Media samples, dissected clean of adventitia from proximal and distal parts of aorta, were also placed in separate containers.
2.3. Measurements of the terminal restriction fragment
(TRF) length
DNA was extracted by the following method: Tissue
was frozen in liquid nitrogen and specimens (:50 mg
each) were placed in an alloy tool steel mortar and pestle set (Fisher, Pittsburgh, PA). After grinding, 0.5
ml of buffer (NaCl 100 mmol/l, Tris 10 mmol/l, SDS
1.0%, EDTA 25 mmol/l; pH 8.0) was added and
speci-mens were thawed at 50°C. Proteinase K (0.2 mg/ml)
was added, and the mixture digested at 50°C overnight.
DNA was extracted with phenol/chloroform/isoamyl
alcohol and with chloroform/isoamyl alcohol,
precipi-tated and dissolved in 10 mmol/l Tris – HCl (pH 8.0)
and 1 mmol/l EDTA.
TRF was measured in DNA samples by a modifica-tion of a method described earlier [11]. The samples were digested overnight with restriction enzymes Hinf I (10 U) and Rsa I (10 U) (Boehringer Mannheim,
Indianapolis, IN). Eighteen DNA samples (:5 mg
each) and four DNA ladders (1 kb DNA ladder plus l
DNA/Hind III fragments; GIBCO, Grand Island, NY)
were resolved on a 0.5% agarose gel (20×20 cm) at 50
V (GNA-200 Pharmacia Biotech, Piscataway, NJ). Af-ter 16 h, the DNA was depurinated for 30 min in 0.25
N HCl, denatured for 30 min in 0.5 mol/l NaOH/1.5
mol/l NaCl and neutralized for 30 min in 0.5 mol/l Tris,
pH 8/1.5 M NaCl. The DNA was transferred for 1 h to
a positively charged nylon membrane (Boehringer Mannheim) using a vacuum blotter (Appligene, Oncor, Gaithersburg, MD). The membranes were then hy-bridized at 65°C with the telomeric probe (digoxigenin
3%-end labeled 5%-(CCTAAA)3) overnight in 5×SSC,
0.1% Sarkosyl, 0.02% SDS and 1% blocking reagent (Boehringer Mannheim). The membranes were washed
three times at room temperature in 2×SSC, 0.1% SDS
each for 15 min and once in 2×SSC for 15 min. The
digoxigenin-labeled probe was detected by the digoxi-genin luminescent detection procedure (Boehringer Mannheim) and exposed on X-ray film (for illustra-tions, and further details, see Fig. 1).
Two values were obtained from the analysis of the terminal restriction fragments. They included the mean TRF length of the distribution of TRF lengths and the lowest-quartile mean TRF length. The latter value was measured by truncating the distribution of the lowest 25th percentile (quartile) and computing the mean TRF from the shortest 25th percentile of TRF lengths. The mean TRF for the lowest quartile was obtained to explore the possibility that the population represents an admixture of rapidly dividing cells with consequently shorter telomeres and slowly dividing or nondividing cells with slow or no telomere attrition.
Table 1 Causes of deatha
N Cause of death
17 Cardiovascular (sudden death, MI, PE)
Polysubstance abuse 17
12 Trauma (MVA, homicide, burns)
4 Disseminated cancer
Massive hepatic necrosis (allograft) 1
aN, number of subjects; MI, myocardial infarction; PE, pulmonary
Fig. 1. Illustration of an autoradiogram showing the terminal restric-tion fragments (TRF) from media (Med) and intima (Int) of the proximal (Prox) and distal (Dist) abdominal aorta (A), and a densit-ometrical scan of the TRF length (B). The mean TRF length was calculated as follows: TRF=ODi/(ODi/MWi), where: ODi is optical density at a given position in the lane and MWiis molecular weight at that position; this formula [12] accounts for the fact that longer telomeres bind more labeled probes and consequently appear darker on the X-ray film. The mean of the duplicates measured in different gels of each sample was used for data analysis. The four lanes on the left are donors’ samples. The extreme lane on the right is a molecular weight reference ladder. Panel B illustrates a densito-metrical scan of the TRF length for the 2nd lane from the left in the upper panel (an intima sample from the proximal abdominal aorta). The mean TRF length of the entire distribution of TRF lengths (scanned between 3 and 20 kb) is 11.42 kb (right arrow on the x-axis). The mean of TRF lengths in the lowest-quartile is 7.23 kb (left arrow on thex-axis). The mean TRF of the lowest-quartile was derived from truncating the distribution at the lowest 25th percentile and computing the mean TRF length from this quartile.
2.4. Grading of atherosclerosis
Atherosclerotic lesions were graded according to a modification of a previously reported visual grading system [13] as follows:
1. Fatty streaks (Grade 1 lesions): These included flat non-palpable pale gray linear lesions that stained distinctly with Sudan IV.
2. Fibro-atheromatous plaques (Grade II lesions): These included soft to firm, pale gray, glistening elevated lesions.
3. Complicated plaques (Grade III lesions): These in-cluded flat or raised pigmented (hemorrhagic) ulcer-ated lesions with or without calcifications.
2.5. Statistical analysis
Data analysis addressed the following major research questions: (1) Is TRF length from cells of the intima and media of the proximal and distal segments of the abdominal aorta correlated with age? (2) Is TRF length in the intima and media related to the grade of atherosclerosis at proximal or distal sites? Linear re-gression and rank correlation analyses were used to estimate and test the strength of associations. Partial correlations were computed to adjust for age. The
criterion for statistical significance was two-tailed PB
0.05; the criterion for entry into stepwise models was
PB0.15. All calculations were performed with SAS
statistical software (SAS Institute, Cary, NC). Analyses were performed using overall TRF length and were repeated using the lowest-quartile mean TRF. Because of technical reasons, TRF length was not always avail-able in the two segments of the abdominal aorta. For this reason, the number of measurements for the intima and media of the two vascular segments are indicated in the tables and figures.
3. Results
3.1. TRF length and age
TRF length, measured in tissues (intima and media) from the distal abdominal aorta, showed a strong in-verse correlation with age (Table 2; Fig. 2A,B). Linear regressions of lowest-quartile mean TRF length of the distal media, distal intima and proximal intima on age also demonstrated a significant negative correlation (Table 2; Fig. 3A,B). Furthermore, the slopes of the regression were nearly identical to those estimated using the total TRF length. For instance, for distal intima segments, decrease in total TRF length per year of
age=0.028 kb/year (Fig. 2A) compared with decrease
in lowest-quartile TRF length=0.026 kb/year (Fig.
Table 2
Relationships between TRF length (expressed in kb) of the intima and media of the abdominal aorta and agea
Linear correlation Tissue Site N TRF length (mean9S.D.)
rscoeff. P-value
Lowest 25% Whole pop. Lowest 25% Whole pop.
Whole pop. Lowest 25%
6.0090.73 −0.30 −0.45
Intima Proximal 48 10.3690.84 0.04 0.001
6.1290.81 −0.55 −0.64 0.0001
10.4590.99 0.0001
Intima Distal 47
Intima Proximal–Distal 44 0.0390.53 −0.0590.53 0.33 0.16 0.03 0.29
1.0090.09 0.35 0.19 0.02
1.0190.05 0.22
Intima Proximal/Distal 44
6.6390.64 −0.15 −0.13 0.32
Media Proximal 48 10.6390.75 0.38
6.2990.79 −0.50 −0.60 0.0003
10.6190.98 0.0001
Media Distal 47
0.1790.64
Media Proximal–Distal 44 0.1790.51 0.42 0.40 0.004 0.008
1.0390.11 0.45 0.41 0.002
1.0290.05 0.005
Media Proximal/Distal 44
aN, number of samples; whole pop., the entire population; lowest 25%, lowest quartile of the population.
Fig. 2. Relationship between age and the mean TRF length of the intima (A) and media (B) of the distal abdominal aorta.
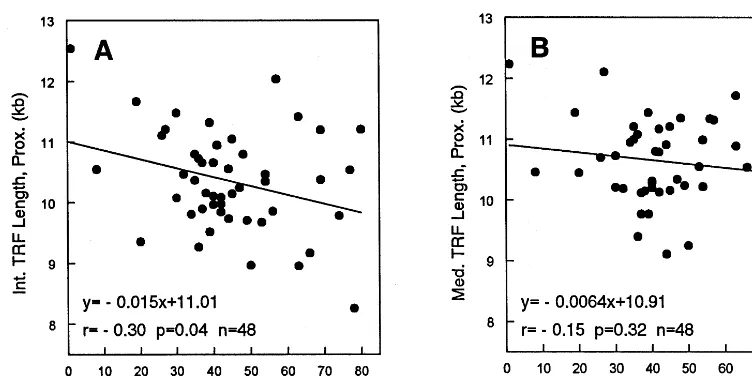
Fig. 4. Relationship between age and the mean TRF length of the intima (A) and media (B) of the proximal abdominal aorta.
Fig. 5. Relationship between age and the difference (D) in the mean TRF length between the proximal minus the distal abdominal aorta for the intima (A) and the media (B).
length=0.025 kb/year (Fig. 2B) and decrease in
lowest-quartile TRF length=0.024 kb/year (Fig. 3B). A
signifi-cant inverse correlation between TRF length and age was also observed for the intima but not for the media of the proximal abdominal aorta (Table 2; Fig. 4A,B). The same was also observed for mean TRF lengths of the lowest quartiles of the intima and media of the proximal segments (Table 2). Such similarities suggest that attri-tion occurs at a uniform rate among cells.
Although TRF length was not significantly greater in the intima and the media from the proximal segment as compared with the corresponding tissues from distal segments of the abdominal aorta, differences in the TRF length between proximal and distal segments were posi-tively correlated with age (Table 2; Fig. 5A,B), indicating that TRF lengths at distal segments underwent more rapid attrition with age than did lengths at proximal segments. The same patterns of correlations with age
were observed when analyses were restricted to the lowest-quartile mean, representing a population with the shortest TRF length (although this was not statistically significant for the intima; Table 2).
3.2. TRF length and atherosclerosis
Atherosclerotic lesions were graded from 0 (no lesions) to 3. Sixty percent of the specimens from the distal aorta had positive scores, evenly distributed from 1 to 3 (Table 3). TRF lengths from both the distal intima and media were significantly lower as atherosclerotic grade
in-creased (Spearman rank correlation coefficient rs=
−0.48,P=0.0007;rs= −0.40,P=0.005, respectively;
Table 4). However, adjustment for age reduced the degree of association to non-significant levels (intima: partialrs= −0.28,P=0.06; media: partialrs= −0.18,
lowest-quar-Table 3
Atherosclerosis grades of the abdominal aortaa
%
aN, number of samples.
non-linear relationship was investigated via stepwise linear regressions, with five candidate covariates: age,
age2, the inverse of age in years (where infants under 1
year were assigned the value 1), and atherosclerosis grade in proximal and distal segments. The best-fitting models (Table 5) for TRF length for the intima and media in the proximal abdominal aorta included the inverse of age as a significant covariate. The best fitting models for TRF length for the intima and media of the distal abdominal aorta included age, with a significant negative regression coefficient. Neither model indicated that atherosclerotic grade was a significant covariate for TRF length.
4. Discussion
The main findings of this work were as follows: (1) the intima of both the proximal and distal segments of the abdominal aorta manifested age-dependent attrition in TRF length, with a higher attrition rate in the distal than proximal segments of the abdominal aorta, (2) whereas the media of the proximal segment of the abdominal aorta showed no significant age-dependent attrition rate in TRF length, the media of the distal abdominal aorta did show significant attrition in TRF length with age, similar to that of the intima in this vascular segment,
(3) as with other somatic tissues [5 – 7], after
an adjustment for age, the TRF length of
tile mean TRF lengths from distal segments with atherosclerotic grade were slightly stronger than those of the mean TRF for the entire population, but not
signifi-cantly so (r= −0.55, P=0.0001 for the intima, and
r= −0.51, P=0.0003 for the media; Table 4). After
adjustment for age, the association between the lowest-quartile TRF length and atherosclerotic grade was not statistically significant. No relationship was observed between atherosclerosis grade and TRF length of the intima and media from the proximal aorta.
A suggestion that age and TRF length in the media and intima of the proximal abdominal aorta might have a
Table 4
Correlation of TRF length and atherosclerosis gradea
N
Site Rank correlation adjusted for age
Tissue Rank correlation
Whole pop. Whole pop. Lowest 25% Whole pop. Lowest 25%
Proximal
Intima 48 −0.07 −0.11 0.65 0.47 0.04 0.11 0.81 0.47
−0.48
Intima Distal 47 −0.55 0.0007 0.0001 −0.28 −0.26 0.06 0.08
Proximal 48 0.11 −0.03 0.95
Media 0.47 0.85 0.12 0.01 0.43
Distal
Media 47 −0.40 −0.51 0.005 0.0003 −0.18 −0.24 0.23 0.10
aN, number of samples; whole pop., the entire population; lowest 25%, lowest quartile of the population.
Table 5
Stepwise regression of TRF length on age and atherosclerosis gradea
Coeff. estimate
aEstimates are for best-fitting model by stepwise selection. Candidate covariates were: age, age2, 1/age, atherosclerotic grade of proximal
both the intima and media showed substantial scatter among human beings, and (4) atherosclerotic grade correlated inversely with the TRF length of both the intima and media of the distal abdominal aorta. How-ever, these correlations disappeared after adjustment for age. The latest finding suggests that atherosclerosis does not alter the rate of telomere attrition as a func-tion of age. Yet one cannot exclude the possibility that the higher rate of telomere attrition in the distal seg-ment of the abdominal aorta enhances the rate of senescence of endothelial cells in this segment. Altered function of the senescent cells might increase the predilection to atherosclerosis in this vascular segment. For instance, senescent endothelial cells produce plas-minogen activator inhibition type 1 [14] — a substance which decreases fibrinolytic activity, and the synthesis of plasmin activator inhibitor 1 is increased in cellular elements of atherosclerotic plaques [15].
In the present study, we took advantage of the differential thawing of the intima in relation to the media to separate the endothelium from the underlying media and thereby reduce cross contamination of the intima by the media. However, such a separation is not perfect and it is particularly difficult in areas of grade III atherosclerosis. Of a lesser concern is a potential cross contamination of the vascular media by cells from the intima, since the effects of such a contamination on the overall TRF length of the media is expected to be minimal. However, the media in grade III atheroscle-rotic lesions comprises not only vascular smooth muscle cells but to some extent also infiltrates of macrophages and monocytes as well as other cells [1,16]. Thus, the TRF length in the media from grade III atherosclerotic tissue might reflect some contribution of cells other than vascular smooth muscle cells.
Chang and Harley [8] have compared the TRF length as a function of age in the intima and media of the internal thoracic aorta and the iliac artery. The authors found that the rate of age-dependent telomere attrition was higher in the intima of the iliac artery than in the intima of the internal thoracic aorta, and that there was no difference in age-dependent telomere attrition be-tween the media of these two arterial segments. The authors proposed that the higher rate of age-dependent telomere attrition of the intima, but not the media, in the iliac artery indicates a higher turnover rate of endothelial cells in the iliac artery than in the thoracic aorta. This was attributed to hemodynamic factors that might act differently in the iliac artery than in the internal thoracic aorta. It is noteworthy, however, that the anatomical distance of the internal thoracic aorta from the iliac artery and the size differences of these vascular segments might have accounted for the differ-ences in TRF length observed between the two blood vessels as a function of age. It is possible, for instance, that the turnover rate of endothelial cells positively
relates to the caliber of arteries. Second, atherosclerosis, which is common in the distal abdominal aorta and iliac arteries of humans, might promote structural re-modeling of the vascular wall that includes not only the intima but also the media. This process is associated with attenuation of the media, as well as phenotypic transformation and proliferation of vascular smooth muscle cells [1,16]. It is therefore expected that arterial segments which are prone to or express atherosclerosis should manifest altered, age-dependent rates of telom-ere attrition of not only endothelial cells but also vascular smooth muscle cells. These considerations un-derlie the present investigation.
The results of our work support the conclusion of Chang and Harley [8] that the endothelium in major human arterial vessels manifests an age-dependent attri-tion rate, which probably reflects the turnover rate of vascular endothelial cells. However, our work also shows that the media of the distal abdominal aorta manifests an age-dependent telomere attrition. In their report, Chang and Harley [8] indicated that the rates of TRF attrition in the intima of the internal thoracic aorta and the iliac artery as a function of age were
−87 and −147 bp per year, respectively. These
attri-tion rates are substantially higher than those found in our work for the intima of the proximal and distal
segments of the abdominal aorta, namely −14.7 and
−27.6 bp per year, respectively. Possible reasons for
these quantitative differences might arise from the dif-ferent vascular segments and difdif-ferent human popula-tions that have been examined in the two studies. It is noteworthy, however, that the attrition rates in the TRF length of the study by Chang and Harley were computed based on findings from four subjects, ages 40 – 74 years. Given the substantial variability among human beings in TRF length after adjustment for the donor’s age [5 – 7,11], an accurate assessment of age-de-pendent attrition in TRF length in a cross population study can be derived only from a relatively large num-ber of subjects.
Acknowledgements
K. Okuda is a post-doctoral fellow of the American Heart Association, New Jersey Affiliate. This work was partially supported by an NIH grant HL47906 and by a grant from the Foundation of the University of Medicine and Dentistry of New Jersey.
References
[1] Ross R. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature 1993;362:801 – 9.
[2] Diaz MN, Frei B, Vita JA, Keaney JF Jr. Antioxidants and atherosclerotic heart disease. New Engl J Med 1997;337:408 – 16. [3] Blackburn EH. Telomeres: no end in sight. Cell 1994;77:621 – 3. [4] Greider CW. Telomeres and senescence: the history, the
experi-ment, the future. Curr Biol 1998;8:R178 – 81.
[5] Slagboom PE, Droog S, Boomsma DI. Genetic determination of telomere size in humans: a twin study of three age groups. Am J Hum Genet 1994;55:876 – 82.
[6] Allsopp RC, Vaziri H, Patterson C, Goldstein S, Younglai EV, Futcher AB, Greider CW, Harley CB. Telomere length predicts replicative capacity of human fibroblasts. Proc Natl Acad Sci USA 1992;89:10114 – 8.
[7] Weng N-P, Levine BL, June CH, Hodes RJ. Human naive and memory T lymphocytes differ in telomeric length and replicative potential. Proc Natl Acad Sci USA 1995;92:11091 – 4.
[8] Chang E, Harley CB. Telomere length and replicative aging in human vascular tissues. Proc Natl Acad Sci USA 1995;92:11190 – 4.
[9] Nguyen ND, Haque AK. Effect of hemodynamic factors on atherosclerosis in the abdominal aorta. Atherosclerosis 1990;84:33 – 9.
[10] Moore JE, Xu C, Glagov S, Zarins CK, Ku DN. Fluid wall shear stress measurements in a model of the human abdominal aorta: oscillatory behavior and relationship to atherosclerosis. Atherosclerosis 1994;110:225 – 40.
[11] Jeanclos E, Krolewski A, Skurnick J, Kimura M, Aviv H, Warram JH, Aviv A. Shortened telomere length in white blood cells of patients with IDDM. Diabetes 1998;47:482 – 6. [12] Harley CB, Futcher AB, Greider CW. Telomeres shorten during
ageing of human fibroblasts. Nature (Lond) 1990;345:458 – 60. [13] Guzman MA, McMahan CA, McGill HC Jr, Strong JP, Tejada
C, Restrepo C, Eggen DA, Robertson WB, Solberg LA. Selected methodologic aspects of the International Atherosclerosis Pro-ject. Lab Invest 1968;18:479 – 97.
[14] Comi P, Chiaramonte R, Maier JAM. Senescence-dependent regulation of type 1 plasminogen activator inhibitor in human vascular endothelial cells. Exp Cell Res 1995;219:304 – 8. [15] Lupo F, Bergonzelli GE, Heim DA, Cousin E, Genton CY,
Bachmann F, Kruithof KO. Localization and production of plasminogen activator inhibitor-1 in human healthy and atherosclerotic arteries. Arterioscler Thromb 1993;13:1090 – 100. [16] van der Wal AC, Becker AE, Das PK. Medial thinning and atherosclerosis — evidence for involvement of a local inflamma-tory effect. Atherosclerosis 1993;103:55 – 64.
![Fig. 1. Illustration of an autoradiogram showing the terminal restric-tion fragments (TRF) from media (Med) and intima (Int) of thederived from truncating the distribution at the lowest 25th percentileweight at that position; this formula [12] accounts for](https://thumb-ap.123doks.com/thumbv2/123dok/3148477.1384443/3.612.52.226.46.500/illustration-autoradiogram-terminal-fragments-thederived-truncating-distribution-percentileweight.webp)