BMC Public Health
2002, 2
Research article
Conceptual framework of public health surveillance and action and
its application in health sector reform
Scott JN McNabb*
1
, Stella Chungong
2
, Mike Ryan
2
, Tadesse Wuhib
3
,
Peter Nsubuga
4
, Wondi Alemu
5
, Vilma Carande-Kulis
6
and Guenael Rodier
2
Address: 1Division of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention, Centers for Disease Control and Prevention,
Atlanta, GA, USA, 2Division of Surveillance and Epidemic Preparedness, World Health Organization, Geneva, Switzerland, 3Division of HIV/AIDS
Prevention, National Center for HIV, STD, and TB Prevention, Centers for Disease Control and Prevention, Atlanta, GA, USA, 4Division of
International Health, Epidemiology Program Office, Centers for Disease Control and Prevention, Atlanta, GA, USA, 5World Health Organization,
Africa Region, Harare, Zimbabwe and 6Division of Prevention Research and Analytic Methods, Epidemiology Program Office, Centers for Disease
Control and Prevention, Atlanta, GA, USA
E-mail: Scott JN McNabb* - [email protected]; Stella Chungong - [email protected]; Mike Ryan - [email protected];
Tadesse Wuhib - [email protected]; Peter Nsubuga - [email protected]; Wondi Alemu - [email protected]; Vilma Carande-Kulis - [email protected]; Guenael Rodier - [email protected]
*Corresponding author
Abstract
Background: Because both public health surveillance and action are crucial, the authors initiated meetings at regional and national levels to assess and reform surveillance and action systems. These meetings emphasized improved epidemic preparedness, epidemic response, and highlighted standardized assessment and reform.
Methods: To standardize assessments, the authors designed a conceptual framework for surveillance and action that categorized the framework into eight core and four support activities, measured with indicators.
Results: In application, country-level reformers measure both the presence and performance of the six core activities comprising public health surveillance (detection, registration, reporting, confirmation, analyses, and feedback) and acute (epidemic-type) and planned (management-type) responses composing the two core activities of public health action. Four support activities – communications, supervision, training, and resource provision – enable these eight core processes. National, multiple systems can then be concurrently assessed at each level for effectiveness, technical efficiency, and cost.
Conclusions: This approach permits a cost analysis, highlights areas amenable to integration, and provides focused intervention. The final public health model becomes a district-focused, action-oriented integration of core and support activities with enhanced effectiveness, technical efficiency, and cost savings. This reform approach leads to sustained capacity development by an empowerment strategy defined as facilitated, process-oriented action steps transforming staff and the system.
Background
Because public health surveillance and action are crucial to effective public health practice, the World Health
Or-ganization (WHO) has initiated consensus meetings at the regional and national level to review and reform sur-veillance and action systems [1–4]. These meetings em-Published: 29 January 2002
BMC Public Health 2002, 2:2
Received: 8 October 2001 Accepted: 29 January 2002
This article is available from: http://www.biomedcentral.com/1471-2458/2/2
phasized improved epidemic preparedness and epidemic response. They also highlight the need to facilitate and standardize surveillance and action assessments and to in-clude integration strategies in the reform process.
In response, the WHO Regional Office for Africa (WHO/ AFRO) has recently initiated the Integrated Disease Sur-veillance (IDS) project [5,6]. This effort uses the concep-tual framework described in this report, which was effectively pilot tested and used to develop a 5-year plan of action (PoA) during the implementation of IDS in Tan-zania ([7] and Nsubuga P, Eseko N, Wuhib T, Chungong S, Ndayimrije N, and McNabb SJN; Centers for Disease Control and Prevention, Tanzanian Ministry of Health, and WHO; in press). WHO/AFRO have adapted, further pi-loted, and subsequently adopted this framework for pub-lic health surveillance assessments (Phase I of IDS) in Africa.
The importance of surveillance and action reform is fun-damental to reducing national and international threats of infectious diseases [8]. Renewed threats to health posed by emerging and re-emerging infectious diseases (IDs); worldwide efforts to eradicate polio and eradicate dracun-culialus and leishmaniasis; and the evolving drug-resist-ance of strains of tuberculosis, malaria, cholera, and
Streptococcus pneumoniae have prompted an evaluation of
the performance of national-level systems of public health surveillance and action [9–11]. In many countries, IDs continue to be substantial causes of mortality, morbidity, and rising health-care costs and must be carefully moni-tored and controlled ([12–14] and Wuhib T, Chorba TL, Davidiants V, MacKenzie M, and McNabb SJN; Centers for Disease Control and Prevention and Armenian Ministry of Health; unpublished manuscript). Any gaps, inaccura-cies, or delays in surveillance and ineffective or inefficient public health actions are revealed both by these renewed ID threats and closer evaluations.
Many countries recognize internal problems with poor performance – or lack – of public health surveillance and action [1]. At the national level, the use of duplicative, in-dependent, vertical public health surveillance systems (e.g., one system for tuberculosis, another system for ma-laria), while keeping surveillance close to action may re-sult in the redundant use of personnel, excessive costs, and ineffective or inefficient actions. Further, some high priority diseases may receive less attention because both technical and financial support for vertical surveillance systems may come from outside a country's borders. De-veloping countries' interests may not always be a top pri-ority for duplicative, independent, vertical surveillance systems. Such a situation results in the use of differing sur-veillance terminology, methods – including analyses and reporting procedures – and actions that overload health
workers. This may lead to discouragement and poor per-formance.
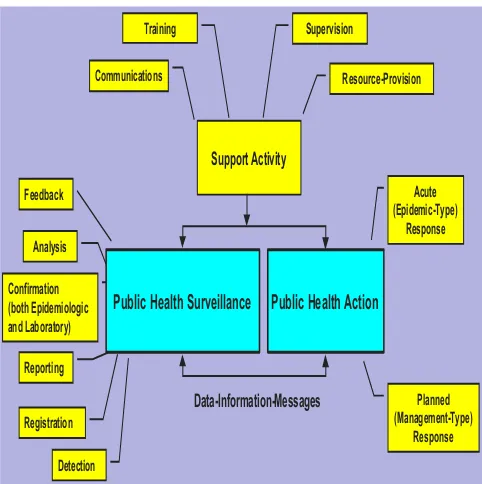
To facilitate and standardize national-level assessments and to create a user-friendly method of national-level re-form, we designed a conceptual framework in which sur-veillance and action reside as interdependent processes (Figure 1). This intuitive framework is not only an easy-to-use process of assessing surveillance and action, but also can be used as a pattern for reform. The two processes compose an open system, defined as the continual input of new case-patients [15]. We categorized this framework into eight core and four support activities that can be measured easily by using well-defined, country-specific indicators.
Methods
In the early years of modern public health (1940 – 1960), the term surveillance was applied to the collection, analysis, interpretation, and dissemination of (health outcome-specific) data to those who need to know[16]. Later, public health sur-veillance was defined as the ongoing systematic collection, analysis, and interpretation of outcome-specific data for use in the planning, implementation, and evaluation of public health practice[17]. Rephrasing the latter meaning, surveillance data are collected at the health facility – the first level of contact of the patient with the health system – then ana-lyzed, interpreted, and used for action.
Figure 1
Conceptual framework of public health surveillance and action
Support Activity
Detection Registration Reporting
Analysis
Confirmation (both Epidemiologic and Laboratory)
Acute (Epidemic-Type)
Response
Planned (Management-Type)
Response Public Health Surveillance Public Health Action
Communications
Training Supervision
Resource-Provision
Surveillance, per se, does not include the public health ac-tion(s) resulting from the interpretation of the data. Few envisaged the inherent responsibility of surveillance prac-titioners (i.e., those public health officials responsible for interpreting the data collected) for prevention and control actions. However, as early as 1963, the international pub-lic health community through the WHO recognized the importance of linking public health surveillance to public health action [18].
In this conceptual framework, public health surveillance comprises six core activities:
1. detection
2. registration
3. confirmation (both epidemiologic and laboratory)
4. reporting
5. analyses
6. feedback
Two core activities comprise public health action:
1. acute (epidemic-type) responses
2. planned (management-type) responses
All public health surveillance and action core activities are enabled by the four support activities of
1. communication
2. training
3. supervision
4. resource-provision
Case-patient detection (core activity #1) is the first step of this framework (Table 1). Defined as the public health cir-cumstance or event that identifies a (presumptive) case-patient as such by the public health system, case-case-patient detection usually occurs at the health-facility level. Al-though usually effected by a health-care provider (e.g., a private physician, nurse, community public health work-er, voluntework-er, or a paid MoH practitioner), the laboratory may also play a role in detection (see also core activity #3 below).
Specified descriptive variables are then entered or regis-tered into a public health record (core activity #2).
Case-patients may be detected but not be registered. Once reg-istered, case-patients either remain unconfirmed or be-come confirmed (core activity #3). Confirmation occurs through the evaluation of epidemiologic criteria and/or laboratory test results. Epidemiologic confirmation in-volves intensive case-patient investigation in the field (e.g. household or workplace). Laboratory tests help confirm or rule out diagnoses of registered case-patients. By detect-ing new, previously unreported case-patients through rou-tine laboratory testing, the laboratory itself can serve as a secondary or primary surveillance system by detecting, registering, and reporting case-patients. Some laboratories provide ongoing reporting of new health outcomes (e.g., antibiotic resistance).
Reporting (core activity #4) of case-patient data involves the movement of public health surveillance data collected from lower levels of the health system (e.g. health facili-ties) to higher ones (e.g., district or national offices).
Once data have been received at the appropriate health level, they are analyzed (core activity #5). Analyses should be done as close to the primary reporting level as possible so there is minimal delay in implementing the appropri-ate interventions to prevent disease. Interventions to im-prove data analyses might include training in analytic methods, including data presentation (standardized charts and graphs) and the establishment of indicator tar-gets designed for public health action. Often, reported data are numbers. Analyses of numbers produce results. Results of analyses of surveillance data are the end points of public health surveillance. However, for collected data to lead to action, they must be interpreted or transformed into public health information and then to public health messages that are used for public health action.
Feedback (core activity #6) is the flow of information and messages back to lower levels from higher ones. Targeted interventions to correct poor feedback might include such efforts as providing timely and regular messages from the national level to the health-facility level on the basis of lo-cally provided data. Even though public health surveil-lance and action are interdependent processes (Figure 1), they relate through inflow and outflow of data-informa-tion-message (i.e., interpretation) (Table 2).
This transformation of data to information to messages can been defined as a process, which is a series of actions or operations, always in motion, directed toward a particular goal
guide any modifications in the content or scope of surveil-lance.
Two core public health actions of acute (epidemic-type) (core activity #7) and planned (management-type) (core activity #8) responses rely upon messages derived from surveillance. Acute (epidemic-type) responses occur di-rectly, reactively, and generally include immediate public health actions (e.g., epidemic investigation, contact fol-low-up, or targeted interventions designed to stop the on-going transmission of disease). Planned (management-type) responses occur with periodicity over time and re-quire a vision of future needs. Examples of such responses include community public health education, purchasing next year's immunization supplies, ordering tuberculosis medication in anticipation of future needs, or reallocating public health personnel and resources in response to changing trends of disease. Public health actions, in turn, must be measured, evaluated, and the results used to not only measure and modify the control and prevention measures taken, but also to guide future modifications in public health surveillance.
Four support activities promote or improve the core activ-ities by enhancing their performance through more effi-cient and effective functioning (Table 1). Core activities can and do occur with or without support activities. Gen-erally, the more support, the better the performance.
Communication (support activity #1) usually proceeds from public health authorities. By definition, communica-tion is a process that involves at least two people in an effort to convey, receive, interpret, and agree upon the meaning of data,
information, or messages[20]. Communication includes the
provision of public health messages through public health bulletins within a country, or to other countries, and also to supra-national organizations (e.g., WHO, United Nations International Children's Emergency Fund, or the World Bank).
Training (support activity #2) and supervision (support activity #3) facilitates day-to-day operations. Interven-tions might include motivating public health workers through training and supervision and taking appropriate public health actions in a timely manner. Other interven-tions, such as training in decision-making, management, and communications could tie the development of analyt-ic skills and knowledge to applied broad publanalyt-ic health practice competencies. Resource-provision (support activ-ity #4) – e.g., the availabilactiv-ity of funds, trained personnel, and materials such as communications infrastructure (i.e., telephone, fax, or computer), electricity, gasoline, or vac-cine-promotes or improves all eight core activities.
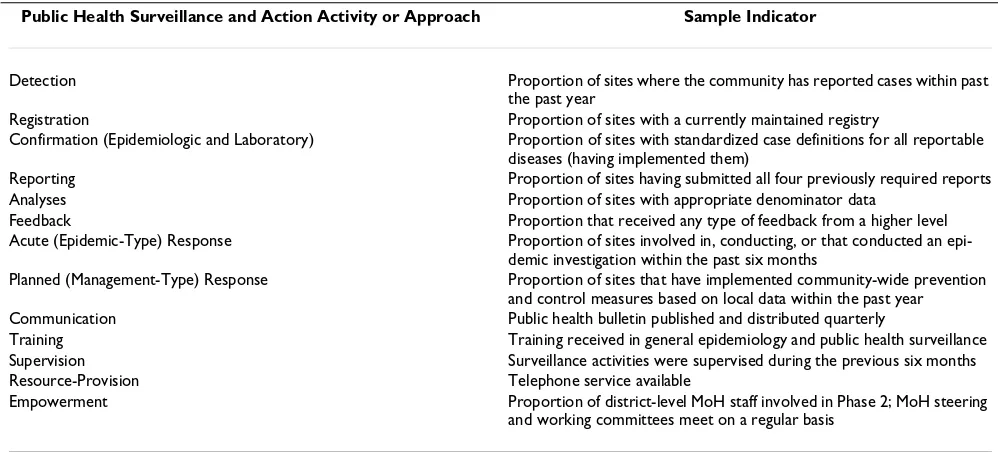
The framework uses the concepts, goals, and objectives of surveillance and action to provide the development of flexible, yet objective, indicators, by each core and sup-port activity and by health-care level, for any country (Ta-ble 3). Indicators – used here as measures of performance – can be customized to adapt to surveillance systems throughout the world.
Results
The authors propose the application of this conceptual framework of public health surveillance and action using a five-phase approach to national-level reform. Using the framework of eight core and four support activities as a road map, public health practitioners can assess the
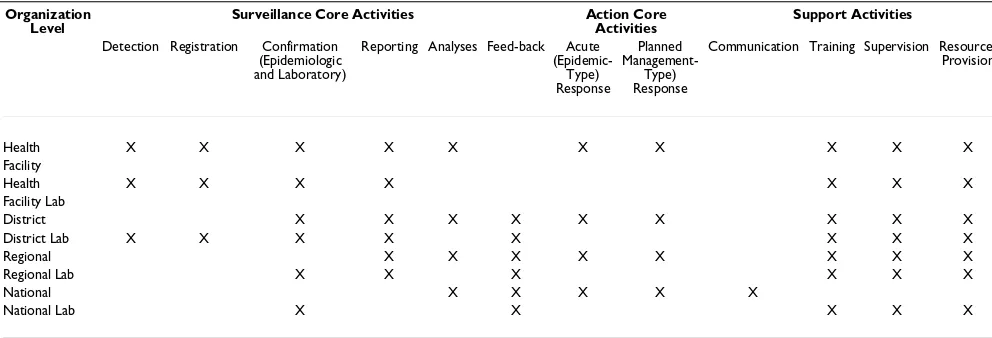
exist-Table 1: Idealized Distribution of Public Health Surveillance and Action Core and Support Activities in a Country with a District-Ori-ented •1 Public Health Structure, by Organizational Level.
Organization Level
Surveillance Core Activities Action Core Activities
Support Activities
Detection Registration Confirmation (Epidemiologic and Laboratory)
Reporting Analyses Feed-back Acute
(Epidemic-Type) Response
Planned
Management-Type) Response
Communication Training Supervision Resource-Provision
Health X X X X X X X X X X Facility
Health X X X X X X X
Facility Lab
District X X X X X X X X X District Lab X X X X X X X X Regional X X X X X X X X Regional Lab X X X X X X National X X X X X
National Lab X X X X X
ing surveillance and action system, propose a model for a future system, and develop and implement a plan of ac-tion (PoA) to achieve the model through a series of proc-ess-oriented action steps. These action steps yield not only measurable outputs and outcomes (by virtue of objectives with indicators), but also develop measurable sustained capacity among MoH staff (by virtue of objectives with in-dicators).
This five-phase approach begins with Phase 1 – prepara-tion for the reform effort and ends with the full imple-mentation of the reform model. Phase 5 involves the evaluation and monitoring of the entire process toward achieving the country-level, district-oriented reform mod-el. Each process-oriented phase yields specific and meas-urable outputs and outcomes, monitored by objectives that guide the next steps.
Phase 1 – preparation
The overall design and implementation of all phases should proceed under the direction of a MoH steering committee (advisory board) that includes high-level deci-sion makers and also representatives from the health facil-ity and district level. The WHO Country Representative can serve as a link between the MoH and other partners. This steering committee should gain consensus and sup-port from other MoH officials, donor organizations, non-governmental organizations (NGOs), and other key play-ers to explain findings, gain undplay-erstanding and support for the process and to build consensus on reform. The out-come of this phase is a commitment to the entire reform process. The steering committee will
• provide each organization with copies of reports; • discuss major findings, interpretations, and conclusions; • identify the specific interests and suggestions for im-provement from stake holders;
• respond to questions; and
• invite participation in processes and debriefings.
Phase 2 – assessment of public health surveillance and ac-tion
To assess the current status of surveillance and action, the MoH uses indicators (Table 3) to measure the existing presence and performance of the multiple, independent, and vertical public health surveillance and action systems using the eight core and four support activities. This as-sessment involves a structured examination at all health levels: national, regional, district, and health-facility. The indicators are captured by questions (both in interview and observation format) and framed into health-level spe-cific questionnaires. The outputs from Phase 2 are objec-tive findings that guide practitioners in the development of a comprehensive PoA with targeted interventions con-ceptualized, planned, and budgeted during Phase 3.
Phase 2 could proceed under the direction of a working committee appointed by the steering committee. The group would also include representation from outside technical partners (e.g., WHO) and the national, regional, district and health-facility levels. The Phase 2 working committee will complete the initial analyses of the assess-ment data and prepare a draft report of the findings to be presented to the steering committee. A draft report is left with the MOH and includes recommendations. Finaliza-tion of the document is then done by the MoH.
Phase 3 – development of a Plan of Action (PoA)
Following completion of Phase 2, the MoH will review the objective findings and develop a detailed PoA using cross-cutting and surveillance themes. Cross-cross-cutting themes may include integration, district-level focus, budget, ac-tion-oriented approach, and advocacy.
Phase 3 should proceed under the direction of another working committee, appointed by the steering committee. This working committee should involve staff from the Phase 2 working committee and key stakeholders from the various vertical programs involved.
The working committee of Phase 3 develops a first-draft PoA based on the comprehensive review of the assessment findings. The working committee is empowered to envi-sion the final reform model, determine the major weak-nesses that should be addressed to achieve it, and identify the appropriate action steps. This workshop process is conducted using the conceptual framework of the step-wise surveillance core and support functions as a road map, beginning with case-patient detection and working through all eight core and four support activities, with the reform model in full view.
The working committee then identifies the process-orient-ed action steps to achieve each specific objective, includ-ing implementation indicators, time-lines, the
Table 2: Example of Data-Information-Message
Data: There are 100 case-patients and five fatalities of measles in Region X in one month, with an incidence of 90/10,000 persons. Information: This is a 50% increase in measles over last year at this time.
Message1: There is an epidemic of measles in Region X that requires immediate public health action. Every infant in Region X can be vacci-nated for less money than it takes to treat the 100 case-patients and five fatalities.
1 Messages are subjective statements about information. They enable
organization or group primarily responsible for imple-mentation, required resources, and means of overcoming potential obstacles (Table 4).
Phase 4 – implementation
Phase 4 focuses on carrying out the process-oriented ac-tion steps developed and described in the PoA as neces-sary to achieve goals and objectives. Phase 4 is the most critical and difficult phase, and often requires financial support from outside agencies. Advocacy both within and beyond the MoH is critical to final approval of the PoA. Once formally approved by the MoH, in many countries, advocacy to donors is critical. These activities are process-es and include specific outcomprocess-es and indicators that measure progressive change at all levels. They are conduct-ed over the life of the project, beginning with the comple-tion of Phase 3 in the first year.
Phase 5 – monitoring and evaluation
During Phase 5, there is a determination of whether the planned changes are occurring by measuring progress. Monitoring and evaluation provides guidance to not only overall reform progress, but also helps identify problem areas in implementation of the PoA. This phase is con-ducted over the entire lifespan of the project, beginning with the initiation of Phase 1 in the first year.
Discussion
The authors describe here a conceptual framework of the interdependent processes of public health surveillance and action. These two processes comprise eight core and
four support activities. The presence and performance of these activities can be measured using well-defined indi-cators that yield information. The information can then guide a comprehensive national-level reform by identify-ing gaps and opportunities for integration and by target-ing interventions designed to improve the technical efficiency and effectiveness of both public health surveil-lance and action. These efforts will reduce costs.
Thacker and Klaucke et al. advanced public health surveil-lance in 1988 with their strategy for surveilsurveil-lance assess-ment [21,22]. Their strategy includes an evaluation of the components of public health importance, objectives and usefulness, operation of the system, cost, and system at-tributes (simplicity, flexibility, acceptability, sensitivity, predictive value positive, representativeness, and timeli-ness). It involves both qualitative (e.g., simplicity) and quantitative (e.g., predictive value positive) measure-ments [23,24]. This evaluation strategy is primarily dis-ease specific and may not be practical when applied to national-level public health surveillance and action re-form efforts that involve the evaluation and consequential modification of entire country-level, multiple surveillance systems.
The Thacker and Klaucke model is used most effectively when a single health indicator (e.g., tuberculosis, hepatitis A, or malaria) is being evaluated. It is less useful to evalu-ate (concurrently) multiple surveillance systems or when the surveillance systems being assessed monitor multiple health indicators. For example, this model does not allow
Table 3: Sample Indicators Measuring the Performance of Public Health Surveillance and Action Core and Support Activities
Public Health Surveillance and Action Activity or Approach Sample Indicator
Detection Proportion of sites where the community has reported cases within past the past year
Registration Proportion of sites with a currently maintained registry
Confirmation (Epidemiologic and Laboratory) Proportion of sites with standardized case definitions for all reportable diseases (having implemented them)
Reporting Proportion of sites having submitted all four previously required reports Analyses Proportion of sites with appropriate denominator data
Feedback Proportion that received any type of feedback from a higher level Acute (Epidemic-Type) Response Proportion of sites involved in, conducting, or that conducted an
epi-demic investigation within the past six months
Planned (Management-Type) Response Proportion of sites that have implemented community-wide prevention and control measures based on local data within the past year Communication Public health bulletin published and distributed quarterly
Training Training received in general epidemiology and public health surveillance Supervision Surveillance activities were supervised during the previous six months Resource-Provision Telephone service available
sensitivity or predictive value positive to be calculated for a surveillance system that captures multiple health indica-tors simultaneously. It does not identify areas amenable to integration.
The authors' goal has been to develop an evaluation tool and provide a road map for national-level reform efforts. The framework proposed here provides specific and objec-tive data to measure the structure (i.e., a description of the number and distribution of regional, district, and health facilities), presence (i.e., system existing at the respective health-care level), and performance (i.e., meeting the minimum standards established by the MoH and required by the indicator chosen at each health-care level) of mul-tiple public health surveillance systems at a national level. The framework is comprehensive, organized, consistent, flexible, diagnostic, action-driven and oriented, and easy for MoH staff to use. Further, it is designed to build sus-tained capacity and can be used to economically evaluate both the current and reformed efforts.
The framework also promotes a "public health action-led" rather than "surveillance (data)-led" model that closely meets the expressed needs of many MoHs [25]. It meets the goal of public health surveillance; namely, to use pub-lic health information to guide the system to take the ap-propriate public health action [26]. The framework is most useful in an applied context. Those countries in the process of political and economic reform or those that do not already have a well-established surveillance infrastruc-ture may more easily use this approach than countries with well-established surveillance systems. It is intuitive for MoH field staff who might not have extensive training in surveillance (Nsubuga P, Eseko N, Wuhib T, Chungong S, Ndayimrije N, McNabb SJN; Centers for Disease Con-trol and Prevention, Tanzanian Ministry of Health, and WHO; in press), and it permits economic analyses of sur-veillance and action (Carande-Kulis V, Aldrich M,
Messio-nier M, and McNabb SJN; Centers for Disease Control and Prevention; unpublished manuscript).
A model of public health surveillance and action reform must adapt to the ongoing political, economic, and social realities of three concurrent movements: 1) decentraliza-tion, 2) integradecentraliza-tion, and 3) primary health-care delivery [27,28]. Funded in large part by international donors, these movements drive the reform model of public health. Decentralization of public health practice accompanies the peripherally shifting movement of other governmen-tal functions [27,28]. During decentralization, political power, authority, responsibility, resources, communica-tions and transportation capacity, person power, and au-tonomy shift peripherally to a highly focused, more efficient and autonomous district level (one serving 250,000 – 500,000 persons). Public health surveillance systems have traditionally existed in a top-heavy and dis-ease-specific (or vertical) form. With the governmental shift toward decentralization, the integration of public health-related activities, management responsibilities, and services becomes critical to the efficient performance of public health practice.
With the integration of health-care services, information needs and uses and public health responses can change. The movement toward the integration of surveillance and action implies the ultimate focus of reform should move from a program-specific focus (e.g., infectious diseases) toward integration with other health problems (e.g., ma-ternal and infant mortality). Accompanying decentraliza-tion and integradecentraliza-tion is emphasis on developing a primary health-care model by restructuring and combining essen-tial health services, including public health services at the district level. This model has the flexibility to include non-infectious disease health outcomes.
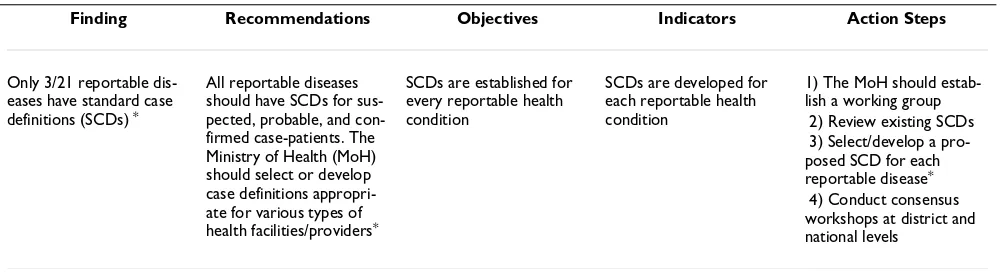
Table 4: Example of Taking One Finding from Phase 2 and Developing a Detailed Plan of Action
Finding Recommendations Objectives Indicators Action Steps
Only 3/21 reportable dis-eases have standard case definitions (SCDs) *
All reportable diseases should have SCDs for sus-pected, probable, and con-firmed case-patients. The Ministry of Health (MoH) should select or develop case definitions appropri-ate for various types of health facilities/providers*
SCDs are established for every reportable health condition
SCDs are developed for each reportable health condition
1) The MoH should estab-lish a working group 2) Review existing SCDs 3) Select/develop a pro-posed SCD for each reportable disease*
4) Conduct consensus workshops at district and national levels
* This information can be developed in much greater detail, e.g. tiered case definitions (e.g. suspect, probable, and confirmed) can be developed for
What then does the public health reform model envision, and how should it be achieved? Directed through process-oriented action steps, the conceptual framework of public health core and support activities described here provides the underpinning for the practical outworking of reform. Its application envisages the creation, over time, of an in-tegrated, district-focused, and action-oriented system of public health practice, including both reformed public health surveillance and action with enhanced effective-ness, technical efficiency, and cost savings. This vision should be achieved by an empowerment approach that leads to sustained capacity development.
If sustained capacity development is desired, empower-ment should be the central underlying strategy of public health practice reform. Defined as a series of facilitated process-oriented actions leading to transformation (i.e., improvement in public health judgment and performance and increased competency in various areas of public health practice), empowerment builds sustained capacity. Beginning from phase 1, the respective MoH staff should lead each phase of reform. The active involvement and central role of the respective MoH staff in each phase in-creases the likelihood of ownership, acceptability, and rel-evance to local conditions of the final model of reform that is adapted.
The processes of public health surveillance reform, which lead to sustained capacity development, are as important as the final reformed model itself. This transformation process is focused on people as well as systems. Indeed, the sustained development of capacity is measured by MoH practitioners who are empowered and trained to
• think independently;
• react appropriately to changing public health circum-stances; and
• develop new public health strategies.
The application of reform may require additional donor funding, often from external international sources. Tech-nical and financial assistance can come from other exter-nal facilitator-partners (e.g. WHO, United States Agency for International Development, United Nations Founda-tion, and the Centers for Disease Control and Preven-tion), but their role should be limited to the provision of tools, resources, critiques or other technical guidance. It requires time to implement reform strategies in an objec-tive-based PoA.
Abbreviations
(IDs) infectious diseases
(IDS) Integrated Disease Surveillance
(MoH) ministry of health
(NGO) non-governmental organizations
(PoA) plan of action
(SCD) standardized case definitions
(WHO) World Health Organization
(WHO/AFRO) Regional Office for Africa
Competing interests
We certify that we have participated sufficiently in the conception and design of this work, as well as its execu-tion and the analyses of the data. Further, we have collab-oratively written the manuscript and take public responsibility for it. We believe the manuscript represents valid work. We have reviewed the final version of the sub-mitted manuscript and approve it for publication. Neither this manuscript nor one with substantially similar content under our authorship has been published or is being con-sidered for publication elsewhere. If requested, we shall produce the data upon which the manuscript is based for examination by the editors.
We certify that we have no affiliations with or involve-ment in any organization or entity with a direct financial interest in the subject matter or materials discussed in the manuscript. Drs. McNabb, Wuhib, Nsubuga, and Carande-Kulis were employees of the U.S. federal govern-ment when this work was performed and prepared for publication; therefore, it is not protected by the Copyright Act, and there is no copyright of which the ownership can be transferred. Dr. McNabb serves as corresponding au-thor; his address is listed below.
References
1. An integrated approach to communicable disease surveil-lance.Weekly Epidemiological Record 2000, 75:1-8
2. World Health Organization: International health regulations. Geneva: World Health Organization, 1983
3. World Health Organization: Disease surveillance – WHO's role. Weekly Epidemiological Record 1998, 73:333-4
4. World Health Organization: Report on infectious diseases – re-moving obstacles to healthy development.Geneva: WHO, 1999 5. World Health Organization, Regional Office for Africa: Integrated disease surveillance strategy, a regional strategy for commu-nicable diseases 1999–2003.Harare: World Health Organization Re-gional Office for Africa, 1999
6. World Health Organization: Regional Office for Africa.Regional Committee Resolution AFR/RC 48/R2, 1999
7. Tanzania Ministry of Health: Proceedings of a workshop on a plan of action for surveillance reform. Dar-es-Salaam Tanza-nia Ministry of Health, 1999
Publish with BioMed Central and every scientist can read your work free of charge
"BioMedcentral will be the most significant development for disseminating the results of biomedical research in our lifetime."
Paul Nurse, Director-General, Imperial Cancer Research Fund
Publish with BMCand your research papers will be: available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours - you keep the copyright
[email protected] Submit your manuscript here:
http://www.biomedcentral.com/manuscript/
BioMedcentral.com
Agency Strategic Objective 4.5. Washington, DC: U.S. Government Printing Office, 1998
9. Institute of Medicine: Emerging infections: microbial threats to health in the United States. Washington (DC)National Acade-my Press, 1992
10. World Health Organization: World Health Report 1996. Fight-ing disease, fosterFight-ing development.Geneva: World Health Organ-ization, 1996
11. Plotkin BJ, Kimball AM: Designing an international policy and le-gal framework for the control of emerging infectious diseas-es: first steps.Emerging Infectious Diseases 1998, 4:362-5
12. Wuhib T, Davidiants V, Parise M, McNabb SJN: Epidemic of malar-ia – Armenmalar-ia, 1997.MMWR 1998, 47:526-8
13. Balasanian M, McNabb SJN: Epidemic investigation of diphthe-ria, Republic of Armenia, 1990 – 1996.JID 2000, 181:S69-S72 14. Kembabanova G, Ivanova R, Deschevoi S, Vitek C, McNabb SJN:
Ep-idemic investigation of diphtheria, Republic of Kazakhstan, 1990–1996.JID 2000, 181:S94-S97
15. Odum HT: Introduction to energy systems.In: Ecological and gen-eral systems: an introduction to systems ecology. 1994
16. Langmuir AD: The surveillance of communicable diseases of national importance.N Engl J Med 1963, 268:182-92
17. Thacker SB, Berkelman RL: Public health surveillance in the United States.Epidemiol Rev 1988, 10:164-90
18. World Health Organization: Report for Drafting Committee. Terminology of malaria and of malaria eradication.Geneva: World Health Organization, 1963
19. Hiebert RE, Ungurait DE, Bohn TW: The process of communica-tion. In: Mass media: an introduction to modern communication III.
198215-29
20. Churchill RE: Using surveillance information in communica-tions, marketing, and advocacy.In: Principles and practice of public health surveillance. 2000
21. Thacker SB, Parrish RG, Trowbridge FL: A method for evaluating systems of epidemiological surveillance.World Health Statistics Quarterly 1988, 41:11-8
22. Klaucke DN, Buehler JW, Thacker SB, Parrish RG, et al: Guidelines for evaluating surveillance systems.MMWR 1988, (S-5):1-18 23. Harkess JR, Gildon BA, Archer PW, Istre GR: Is passive
lance always insensitive? An evaluation of shigellosis surveil-lance in Oklahoma.Am J Epidemiol 1988, 128:878-81
24. Modesitt SK, Hulman S, Fleming D: Evaluation of active versus passive AIDS surveillance in Oregon.Am J Public Health 1990,
80:463-4
25. Sandiford P, Annett H, Cibulskis R: What can information sys-tems do for primary health care? an international perspec-tive.Soc Sci Med 1992, 34:1077-87
26. Thacker SB: In: Principles and practice of public health surveillance. 2000 27. McNabb SJN, Chorba TL, Cherniack MG: Public health concerns in the countries of Central and Eastern Europe and the New Independent States.Current Issues in Public Health 1995, 1:136-45 28. Cherniack MG, Chorba TL, McNabb SJN: Demographic features