Ker Department of Pediatric Critical Care, Cohen Children's Medical Center, New Hyde Park, NY, USA. Mastropietro Division of Pediatric Critical Care, Department of Pediatrics, Riley Hospital for Children ved Indiana University Health, Indianapolis, IN, USA.
Federico Fernandez Nievas Golisano Children’s Hospital, Upstate University of New York, Department of Pediatrics, Division of Pediatric
Mehta Boston Children's Hospital, Division of Critical Care Medicine, Department of Anesthesiology, Critical Care and Pain Medicine, Boston, MA, USA. Federico Fernandez Nievas Golisano Children's Hospital, Upstate University of New York, Department of Pediatrics, Division of Pediatrics.
Respiratory Controversies
Ventilator Management
Higher versus lower positive end-expiratory pressures in patients with acute respiratory distress syndrome. High-frequency oscillations in patients with acute lung injury and acute respiratory distress syndrome (ARDS): systematic review and meta-analysis.
Extracorporeal Membrane
Oxygenation for Acute Pediatric Respiratory Failure
In a single-center review of children requiring ECMO for acute respiratory failure from 1991 to 2002, Pettignano et al. Primary use of the venous approach for extracorporeal membrane oxygenation in pediatric acute respiratory failure.
Weaning and Extubation
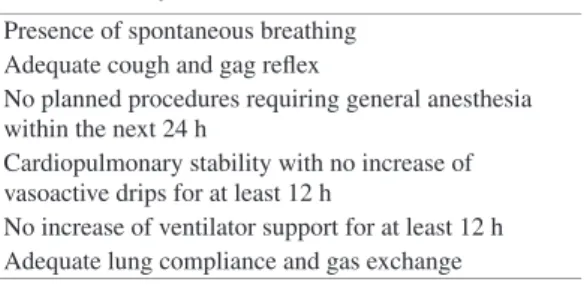
Readiness Assessment in Pediatric Patients
Postextubation stridor, indicating upper airway obstruction, is one of the most common causes of extubation failure in children. Clinical epidemiology of extubation failure in pediatric cardiac intensive care: a report from the Pediatric Cardiac Critical Care Consortium.
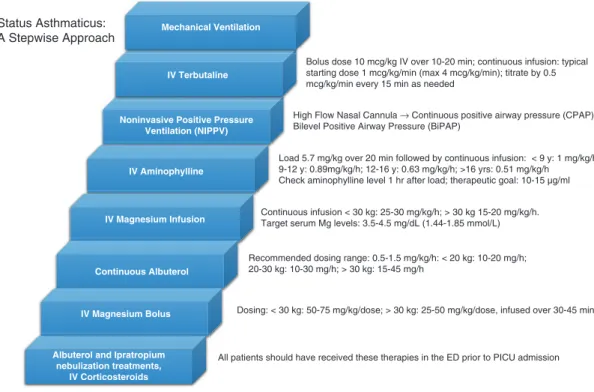
Management of Status Asthmaticus in Critically Ill
We have also summarized a suggested algorithmic approach to managing status asthma in Fig. Corticosteroids that are very potent with a rapid onset are more desirable for patients with status asthmaticus. Heliox has been recommended by some as a means of avoiding endotracheal intubation in patients with status asthmaticus [78-80].
Routine use of heliox in patients with status asthmaticus cannot therefore be recommended, and its use in mechanically ventilated patients should be avoided. Intermittent nebulization of ipratropium bromide is also recommended as first-line therapy for pediatric patients admitted with status asthmaticus. Convincing but not conclusive evidence exists to support the use of non-invasive positive pressure in children with status asthmaticus.
A prospective, randomized study of continuous versus intermittent nebulized albuterol for severe status asthmaticus in children. Nasal high flow in the management of children with status asthmaticus: a retrospective observational study. Safety, efficacy, and tolerability of early initiation of noninvasive positive pressure ventilation in pediatric patients admitted with status asthmaticus: a pilot study.
Cardiovascular Controversies
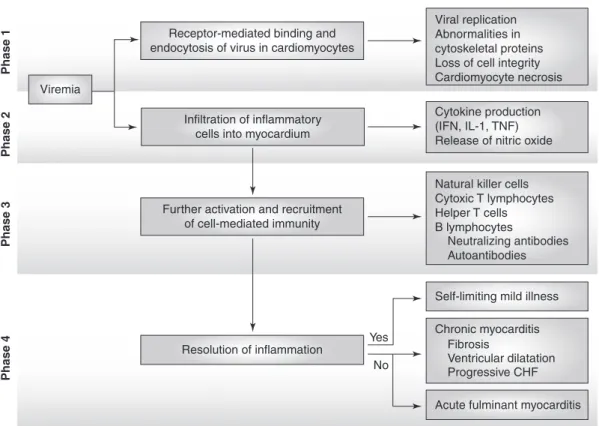
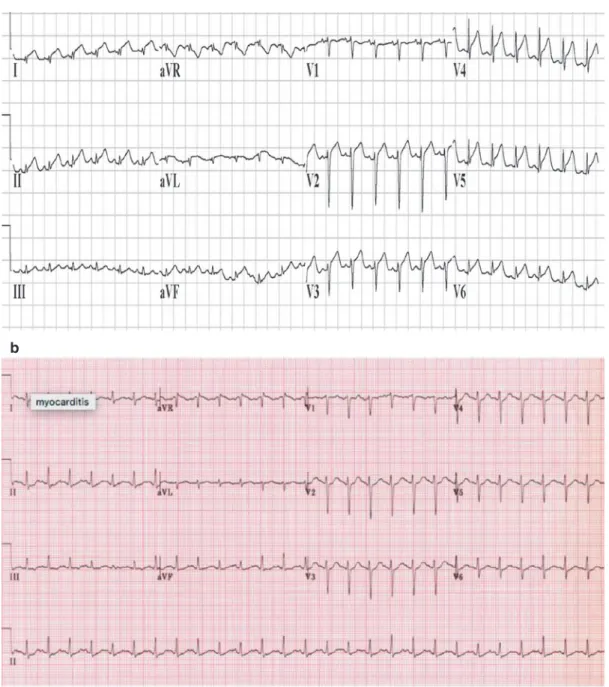
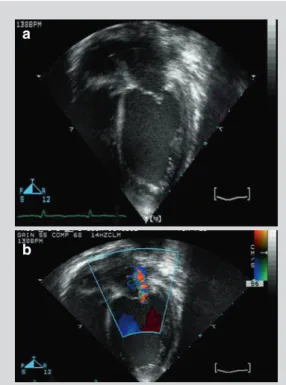
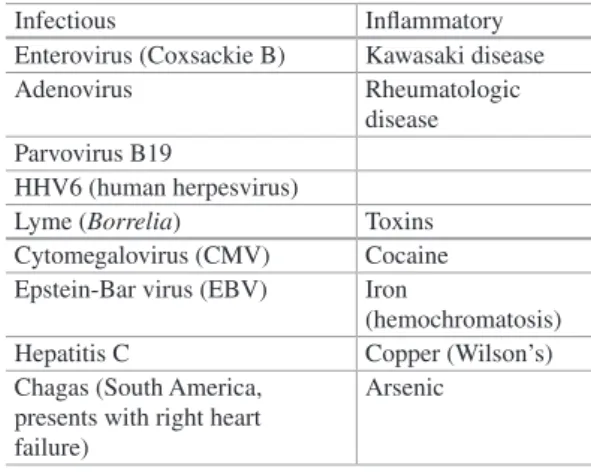
Medical Management of Acute Fulminant Myocarditis
Vasodilators: Nitroglycerin and nitroprusside can be used in patients with high or normal blood pressure. Inotropic agents: Patients with severe heart failure and decreased blood pressure may not benefit from vasodilators. In patients with fulminant myocarditis, survival rates associated with extracorporeal membrane oxygenation (ECMO) and ventricular assist devices (VAD) vary across studies.
A study of 514 patients with acute fulminant myocarditis from the PHIS database reported a mortality rate of 7.3%. The study showed better outcomes (death, transplantation and echocardiographic normalization 3 years after presentation) in patients with myocarditis compared to patients with idiopathic dilated cardiomyopathy (P. Proposed diagnostic and therapeutic algorithm for patients with suspected acute myocarditis considering biomarkers, imaging with cardiac magnetic resonance (cMRI) and endomyocardial biopsies (EMB).
Proposed diagnostic and therapeutic algorithm for patients with suspected acute myocarditis considering blood markers, cardiac magnetic resonance imaging (cMRI) and endomyocardial biopsy (EMB). Diagnostic performance of cardiovascular magnetic resonance in patients with suspected acute myocarditis: comparison of different approaches. Continuous intravenous dobutamine is associated with an increased risk of death in patients with advanced 5 Medical Management of Acute Fulminant Myocarditis.
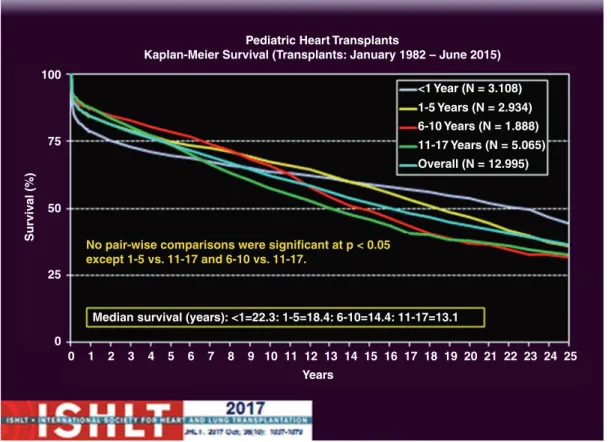
Pediatric Cardiac Transplantation and Mechanical Assist Devices
The use of Berlin Heart EXCOR carries an almost 30% risk of stroke with varying degrees of neurological dysfunction [10]. The use of CentriMag and PediMag devices connected to Berlin cardiac cannulas has been described in small case series [12–14]. Patients and their caregivers can be trained in the day-to-day management of the HVAD.
When right heart function is marginal, underfilling of the Berlin Heart EXCOR may occur, increasing the risk of pump thrombosis and associated morbidities, including stroke. The device is widely used in Europe and has been implanted in the United States as part of the Momentum 3 trial [18]. Early in the Berlin Heart IDE EXCOR study, a protocol was established to standardize anticoagulation management across all patients in the study (Tables 6.1 and 6.2).
Results of the HeartWare Left Ventricular Assist System Postmarketing Evaluation Registry (ReVOLVE). The first successful use of the Levitronix PediMag ventricular assist device as a biventricular bridge for transplantation in an infant. Registry of the International Society for Heart and Lung Transplantation: Seventeenth Official Report on Pediatric Heart Transplantation - 2014; main topic: retransplantation.
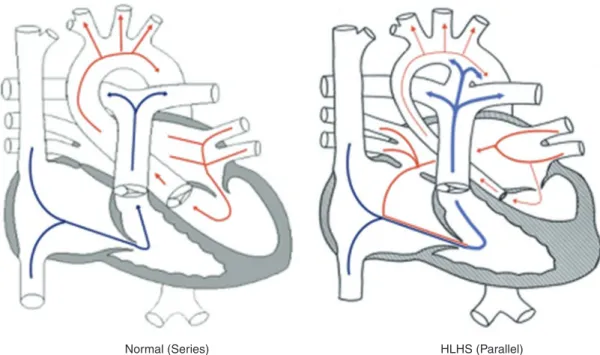
Surgical Management of Hypoplastic Left Heart
Adapted from Pasquali et al. [13]) (DHCA deep hypothermic circulatory arrest, ECMO extracorporeal membrane oxygenation, intensive care unit, HCT hematocrit, RCP retrograde cerebral perfusion). Depending on the size, age and shape of the patient, a hybrid Norwood procedure was recommended. However, there is controversy regarding the ideal size of the conduit [64] and the location of the latter anastomosis [65].
The completion of the conduit is then performed in a similar manner to the extracardiac conduit described above [66, 67]. Tworetzky W, Wilkins-Haug L, Jennings RW, van der Velde ME, Marshall AC, Marx GR, et al. Selamet Tierney ES, Wald RM, McElhinney DB, Marshall AC, Benson CB, Colan SD, et al.
Marshall AC, van der Velde ME, Tworetzky W, Gomez CA, Wilkins-Haug L, Benson CB, et al.
Gastrointestinal Controversies
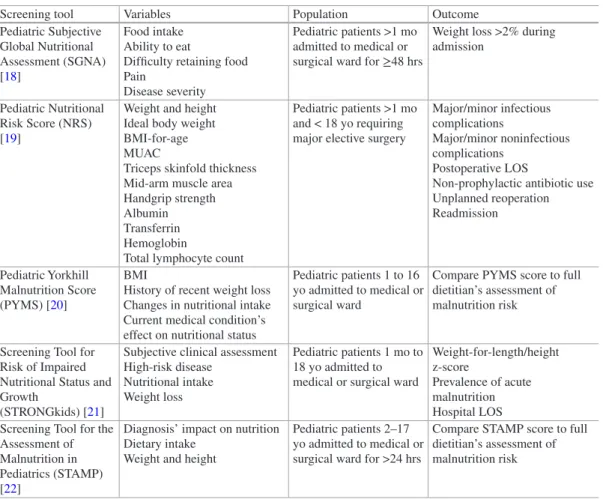
Nutritional Support in the Pediatric ICU
Indirect calorimetry (IC) remains the gold standard and current ASPEN/SCCM guideline recommendation to measure resting energy expenditure in critically ill children. Clinical outcomes in critically ill children prescribed glutamine did not differ compared to controls;. Feeding practices and their relationship to clinical outcomes in critically ill children – an international multicentre cohort study*.
Nutritional status based on body mass index is associated with morbidity and mortality in ventilated critically ill children in the PICU. Pitfalls in predicting resting energy requirements in critically ill children: a comparison of predictive methods with indirect calorimetry. Gastrointestinal versus small intestinal feeding in critically ill children receiving mechanical ventilation: a randomized controlled trial.
Effectiveness and safety of a protocol to promote early intra-gastric feeding in critically ill children. Optimization of energy supply with supplementary parenteral nutrition in critically ill patients: a randomized controlled clinical trial. Early enteral immunization administration in critically ill children: results of a blinded randomized controlled clinical trial.
Medical Management of Acute Liver Failure
In a large retrospective review of patients from the American Acute Liver Failure Study Group (ALFSG), AKI was observed in nearly 47% of patients with ALF [49]. Acute liver failure in children: the first 348 patients in the Pediatric Acute Liver Failure Study Group. The contribution of transjugular liver biopsy in patients with a clinical picture of acute liver failure.
Complications and use of intracranial pressure monitoring in patients with acute liver failure and severe encephalopathy. Effects of antimicrobial prophylaxis and bloodstream infections in patients with acute liver failure: a retrospective cohort study. Noninvasive monitoring of cerebral perfusion pressure in patients with acute liver failure using transcranial doppler ultrasound.
Risk factors and outcomes of acute kidney injury in patients with acute liver failure. High-volume plasma exchange in patients with acute liver failure: an open-label randomized controlled trial. Albumin dialysis with an acellular artificial liver support device in patients with acute liver failure: a randomized, controlled trial.
![Table 9.1 Diagnostic evaluation [85]](https://thumb-ap.123doks.com/thumbv2/azdoknet/10578395.0/164.756.82.685.101.694/table-9-1-diagnostic-evaluation-85.webp)
Renal Controversies
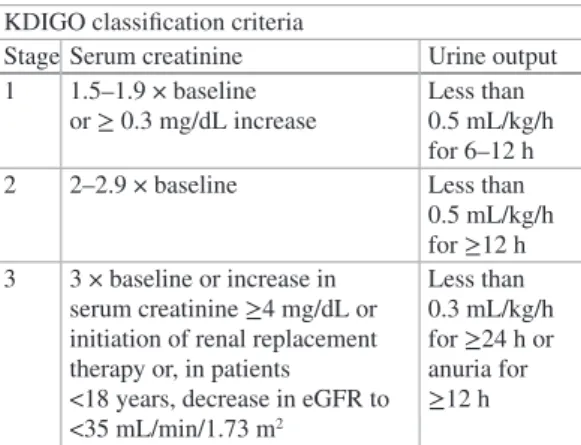
Diagnosis and Management of Acute Kidney Injury in Critical
Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Incidence, risk factors, and outcomes of acute kidney injury after pediatric cardiac surgery: a prospective multicenter study. Risk factors and outcomes of acute kidney injury in neonates undergoing complex cardiac surgery.
Long-term risk of chronic kidney disease in children surviving episodes of acute kidney injury in the intensive care unit: a prospective cohort study. Acute kidney injury in patients with acute lung injury: impact of fluid overload on the classification of acute kidney injury and associated outcomes. A comparison of RIFLE with and without urine output criteria for acute kidney injury in critically ill patients.
Urinary TIMP-2 and IGFBP7 as early biomarkers of acute kidney injury and renal repair after cardiac surgery. Development and standardization of a furosemide stress test to predict the severity of acute kidney injury. Derivation and validation of the renal angina index to improve the prediction of acute kidney injury in critically ill children.
Management of Fluid Overload in the Pediatric ICU
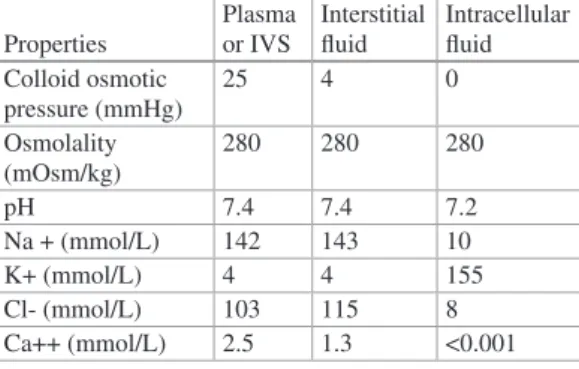
Fluid movement across the capillary bed was previously described primarily through the Starling principle, which relies on the assumptions that capillary and postcapillary venules behave as semipermeable membranes that absorb fluid from the interstitial space. As fluid moves along the length of the capillary bed toward the end of the venule, filtration will eventually lead to a relatively increased concentration of proteins within the intravascular space and thus an increase in intravascular oncotic pressure relative to the interstitial fluid. This differential in oncotic pressure at the venule end of the capillary is greater than the hydrostatic differential, and thus there is a change in flow based on an overall pressure gradient that leads to fluid absorption back into the intravascular space [4].
Starling's concept of filtration and absorption for fluid movement is shown in Fig. Although Starling's principles of fluid movement are generally considered the standard, in 2004 Adamson and colleagues revised the Starling equation and theorized that non-fenestrated capillaries filter fluid along their entire length into the interstitial space and that absorption through venules does not occur despite the rise of capillary oncotic pressure, which cannot. Image created by Grace Ker). showing the relationship between oncotic pressures in the capillary bed at the end of a venule. In the precapillary arterioles, the hydrostatic pressure is greater than the oncotic pressure, which promotes the flow of water into the interstitial fluid.
In the postcapillary venules, the oncotic pressure is greater than the hydrostatic pressure, which promotes the movement of water out of the interstitial fluid and back into the venules. This slight decrease in oncotic pressure is the result of the dilution of postvenular protein content by water returning to the intravascular space. At the arterial end, hydrostatic pressure exceeds oncotic pressure with relative movement of water into the interstitial fluid via filtration. the oncotic pressure is greater than the hydrostatic pressure, which then favors the movement of fluid into the vasculature via absorption.