Jean Benzel-Lindley, PhD, RN Assistant Director of the Nevada Nursing Career Institute, Las Vegas, Nevada. Jeana Wilcox, PhD, RN, CNS, CNE Associate Dean for Undergraduate Programs Associate Professor of Nursing.
ORGANIZATION
Gerontologic Nursing, Fifth Edition, was developed to provide today's students with a solid foundation to meet the future challenges of gerontologic nursing practice. The fifth edition has been revised to reflect the growth and change of gerontological nursing practice and the learning needs of today's student.
FEATURES
Common problems and conditions in each of the chapters are presented in a format that includes the definition, etiology, pathophysiology, and typical clinical presentation for each chapter. Each of these chapters focuses on the nursing management of problems and conditions.
Introduction to Gerontologic Nursing 1 Overview of Gerontologic Nursing, 1
2 Theories of Aging, 16
3 Legal and Ethical Issues, 29
4 Gerontologic Assessment, 54
Influences on Health and Illness 5 Cultural Influences, 83
6 Family Influences, 97
7 Socioeconomic and Environmental Influences, 120
8 Health Promotion and Illness/
Disability Prevention, 139
9 Health Care Delivery Settings and Older Adults, 153
Factors associated with institutionalization, 168 Medical and psychosocial models of care, 168 CLINICAL ASPECTS OF THE NURSING FACILITY, 169.
Wellness Issues 10 Nutrition, 181
11 Sleep and Activity, 202
12 Safety, 218
13 Sexuality and Aging, 241
Common Psychophysiologic Stressors
14 Pain, 255
15 Infection, 270
16 Chronic Illness and Rehabilitation, 281
17 Cancer, 296
18 Loss and End-of-Life Issues, 324
Diagnostic Studies and Pharmacologic Management
19 Laboratory and Diagnostic Tests, 344
20 Pharmacologic Management, 361
Nursing Care of Physiologic and Psychologic Disorders
21 Cardiovascular Function, 388
22 Respiratory Function, 422
23 Endocrine Function, 455
24 Gastrointestinal Function, 477
25 Musculoskeletal Function, 511
26 Urinary Function, 541
27 Cognitive and Neurologic Function, 561
28 Integumentary Function, 607
29 Sensory Function, 640
Index, 659
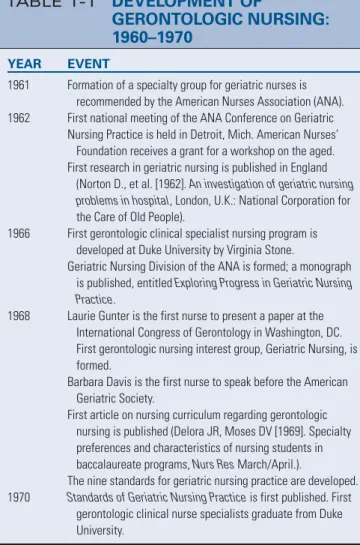
OF GERONTOLOGIC NURSING
History and Evolution
Overview of Gerontologic Nursing
Therefore, nursing professionals should expect to care for an ever-increasing number of patients with chronic and degenerative conditions. During World War II and the postwar years, the elderly population increased steadily, but articles on elder care were general and not particularly comprehensive (Burnside, 1988).
Professional Origins
Burnside discovered an anonymous column in the AJN titled "Care of the Elderly" that was written in 1925 and is now thought to be one of the earliest references to the need for a specialty in the care of the elderly.
Standards of Practice
Overview of Gerontologic Nursing 3
The first combined certification for the AGCNS Acute Care Exam and the AGCNS Primary Care Exam will occur beginning in 2014. Eligibility criteria for the application process to take one of the four certification exams can be found here. in section 1-1.
Roles
AGNP acute care or primary care activities include interventions for the promotion, maintenance and restoration of health. Health maintenance organizations (HMOs) are now including acute care or primary care AGNPs in their provider panels.
Terminology
Today, AGCNSs can practice in acute care hospitals, long-term care or home care settings, or independent practices. The Acute Care or Primary Care Adult Gerontological Nurse Practitioner (ACAGNP/PCAGNP) can be educationally prepared in several ways, but must be licensed as an RN.
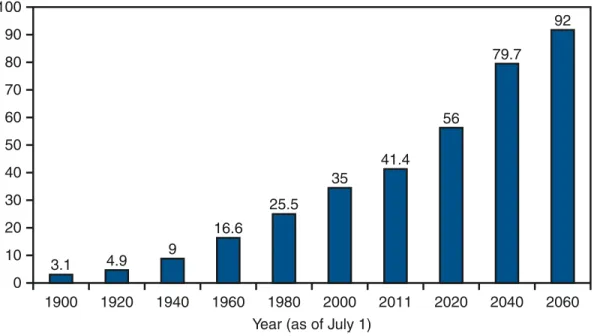
DEMOGRAPHIC PROFILE OF THE OLDER POPULATION
Overview of Gerontologic Nursing 5
Although grouping the elderly is useful in some circumstances, the nurse is cautioned against treating all persons older than 65 years as similar. Understanding how variables interact and affect older adults enables the nurse to provide individualized care.
The Older Population
Consequently, the nurse is encouraged to see each elderly patient as any other patient—a being with a rich and unique set of internal and external variables that ultimately influence how the person thinks and acts. Additionally, the nurse is encouraged to use the individual patient as a standard, comparing the patient's previous level and pattern of health and function with the current status.
Highlights of the Profile of Older Americans
Milestones for human growth and development are clearly defined for childhood through middle age, but few standards are so discreetly defined for older adulthood. In fact, most developmental norms described for later life categorize all older adults in the group over 65 years of age.
Gender and Marital Status
Race and Ethnicity
Living Arrangements
Geographic Distribution
Overview of Gerontologic Nursing 7
Throughout their later years, older adults tend to stay wherever they live, choosing not to move. Diminishing financial resources may necessitate a move to a more economical location; conversely, economic stability or prosperity may provide the opportunity to move to a retirement community or a location with a temperate climate and recreational offerings.
Education
Counter Migration describes the move some older adults make back to their home states after a previous migration to the Sunbelt states for retirement.
Income and Poverty
Employment
HEALTH STATUS OF OLDER ADULTS
Self-Assessed Health and Chronic Disease
Functional Status
Overview of Gerontologic Nursing 9
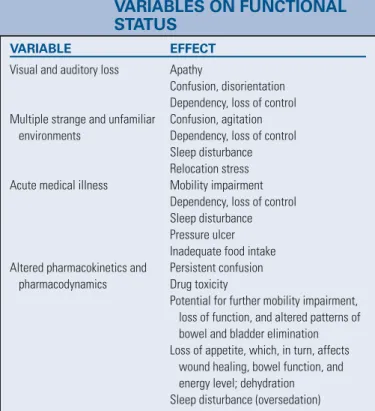
Assessment of the impact of chronic diseases and age-related declines in functional status enables the nurse to determine needs, plan interventions and evaluate outcomes. Chronic illness and disability can impair physical and emotional health, self-care ability and independence.
Health Care Expenditure and Use
The use of such measurement tools or scales to determine the effect of chronic disease and normal aging on physical, psychological, and social function provides objective information about a person's overall degree of health. Improving the health and functional status of older adults and preventing complications of chronic disease and disability can avoid the onset of physical frailty and cognitive impairment, two conditions that increase the likelihood of institutionalization.
Implications for Health Care Delivery
Acute Care Setting
It is imperative for emergency nurses to incorporate this knowledge and skills into their daily practice with older adult patients because hospitalized older adults in the future are likely to be even frailer than they are today.
Nursing Facilities
Home Care
Continuum of Care
Overview of Gerontologic Nursing 11
The health care network that develops for this population must integrate programs into coordinated systems of care that allow for freedom of movement along the continuum. The ripples extend in all directions.” The future is uncertain, but older adults and their caregivers eagerly await the new choices that will be presented in the hope of more effectively meeting the needs of a growing and demographically changing population.
IMPACT OF AN AGING POPULATION ON GERONTOLOGIC NURSING
Ageism
Nursing Education
Nurses with formal preparation in the field of gerontological nursing are imperative if students are to be adequately prepared to meet the needs of the older adult population. Assuring nursing students that they will be adequately prepared to practice in the future – a future that will undeniably include caring for older adults in a wide variety of settings.
Nursing Practice
Overview of Gerontologic Nursing 13
Consequently, future models of care must take greater account of the impact of many intervening variables on the health status of older adults. This will become increasingly important as nurses assume greater responsibility for the care and treatment of older adults in all settings.
Nursing Research
Despite the above trends, the traditional medical care model in the acute care setting and the nursing facility that focuses on the treatment of diseases and conditions continues to persist. Furthermore, even if older adults have individual problems, it is likely that they are intertwined with other variables.
SUMMARY
Care of the older person today is considerably different from what it was 55 years ago (1960). Cite examples of how and
Is it safe to assume that the care of these two women will be similar.
As a student, you are often assigned to care for older adults
Overview of Gerontologic Nursing 15
Institute of Medicine, Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing, at the Institute of Medicine.
Theories of Aging
Theories of Aging 17
Because individuals have unique genetic, social, psychological and economic factors woven into their lives, the course of aging varies from individual to individual. The recognition of the universal truths is what we try to discover through the theories of aging.
BIOLOGIC THEORIES OF AGING
Stochastic Theories Error Theory
Theories of Aging 19
Proponents of this theory cite microscopic signs of wear and tear found in striated and smooth muscle tissues and in nerve cells. If exercise has been shown to increase rather than decrease a person's level of functioning, critics argue, how can the wear and tear hypothesis be correct?
Nonstochastic Theories
According to Carnes, Staats, and Sonntag (2008), striated muscles, cardiac muscles, muscle fibers, nerve cells, and the brain are irreplaceable when destroyed by wear. This theory was developed during the Industrial Revolution, when people tried to explain and understand events in their world.
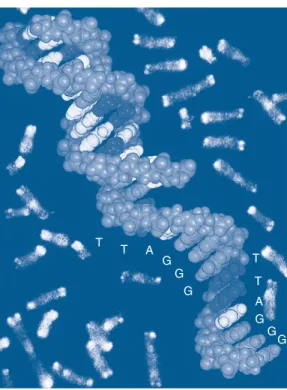
Emerging Theories
It has been observed that a decline, or even a disruption, occurs in many of the components of the neuroendocrine system during the lifespan. It has been found that with each cell division that occurs in cultured, normal human cells, a portion of the telomere is lost.
Implications for Nursing
Theories of Aging 21
Physical activity continues to play an important role in the lives of older adults. Activities to reduce stress and promote healthy coping mechanisms should be included in the patient education plan for older adults.
SOCIOLOGIC THEORIES OF AGING
Although aging causes a decline in the normal function of the immune system, older adults should not suffer unnecessarily from infections or diseases. Being aware of individual cultural preferences and sharing these with other health professionals will further promote positive interactions with older adults in all settings.
Disengagement Theory
Theories of Aging 23
Continuity Theory
Age Stratification Theory
Person–Environment Fit Theory
While these changes help younger members of society with limited physical abilities, they also benefit older adults. Older adults continue to be active, engage or disengage as they choose, and remain valued members of society.
PSYCHOLOGIC THEORIES OF AGING
These accommodations may encourage older adults to remain in the community, perhaps even in the family home, rather than prematurely institutionalize. Older adults continue to feel valued and seen as active members of society when they are allowed to maintain a sense of control over their living environment.
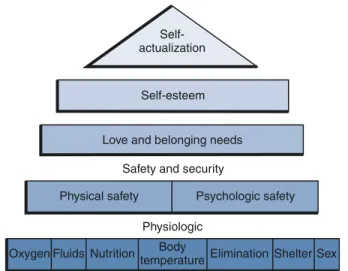
Maslow’s Hierarchy of Human Needs
Theories of Aging 25
Jung’s Theory of Individualism
Eight Stages of Life
Maslow's ideal self-actualized person is probably achieved by only about 1% of the population (Thomas & Chess, 1977). The onset of retirement and the end of the work role can reduce feelings of self-esteem.
Selective Optimization with Compensation
Theories of Aging 27
MORAL AND SPIRITUAL DEVELOPMENT
- Discuss how sociologic theories of aging may be influenced by changing societal values (e.g., advanced technology or a
- A 64-year-old woman believes that heart disease and poor circulation are inevitable consequences of growing older and
- A 77-year-old man frequently talks about how he wishes he were as strong and energetic as he was when he was
- What health promotion strategies would you recommend to encourage successful aging?
The not so close relationship between biological aging and age-related pathologies in humans.
Legal and Ethical Issues
PROFESSIONAL STANDARDS: THEIR ORIGIN AND LEGAL SIGNIFICANCE
However, the community standard of care cannot be lower or have fewer expectations than the federal standard. The published standards of professional organizations, which represent the opinions of experts in the field, are important in establishing the appropriate standard of care.
OVERVIEW OF RELEVANT LAWS Sources of Law
A standard of care is a guideline for nursing practice and establishes an expectation for the nurse to provide safe and appropriate care (Potter & Perry, 2004). Because it is a well-known and long-standing organization, the standards established by the TJC are often referenced in court cases and used to review health care facilities to determine the appropriate standard of care.
Federal and State Laws
Legal and Ethical Issues 31 term nursing facility for Medicaid purposes (as of the OBRA’s
The survey and certification procedures and the process by which CMS evaluates and determines whether a provider is in compliance with Medicare and Medicaid requirements are the responsibility of the Office of Healthcare Standards and Quality within CMS.
Health Insurance Portability and Accountability Act of 1996 (HIPAA)
ELDER ABUSE AND PROTECTIVE SERVICES
Legal and Ethical Issues 33
Nurses must at all times be aware of their responsibility to respect and preserve the autonomy and individual rights of older adults. This presents both a tremendous opportunity and a legally recognizable and irrefutable responsibility to advocate on their behalf.
NURSING FACILITY REFORM
All people, including older adults, have the right to decide what is to be done about them, as well as the right to exercise maximum control over their personal environment and living conditions. The nurse is often the health professional closest to elderly patients and may therefore be in the best position to communicate and understand their wishes.
OBRA’s Three Major Parts
Provision of Service Requirements Quality of Care
Legal and Ethical Issues 35
A "dose reduction trial" consists of a reduction in the dose of the drug along with observations. CMS is committed to seeing that every nursing facility implements and complies with the letter and spirit of OBRA's requirements.
Legal and Ethical Issues 37
Proposed Legislative Changes
AUTONOMY AND SELF-DETERMINATION
Every person of mature years and of sound mind has a right to determine what should be done with his own body.6 The right to self-determination therefore has a long-standing basis in common or jurisprudence and has roots under the right to liberty guaranteed by the US Therefore, more frequent discussions of the need to preserve the right to self-determination occur among older adults.
Do Not Resuscitate Orders
Legal and Ethical Issues 39
Whatever policy is adopted must be well communicated to the staff and strictly adhered to. These factors must be consistent with applicable state law; thus, it is necessary to examine the DNR provisions of the jurisdiction.
Advance Medical Directives
Because the nurse may be the only health care professional present in the nursing home at any given time, it is imperative for the nurse to request that the facility have a detailed and specific policy to provide the necessary guidance. The policy should be approved through all appropriate channels (see Standard CP 1.5.18 and its subsections; . Long Term Care Standards Manual, 1989).
Legal Tools
This is called a resilience, which comes into effect in the future upon the occurrence of a specific event – in this case the patient's incompetence. Because the specifics of the laws vary from state to state, it is important that the nurse is aware of the laws in the state in which he or she practices.
Decision Diagram
Legal and Ethical Issues 41
It can also be any other person whom the court deems to best serve the patient's interests. In any case, the laws of the jurisdiction should be reviewed to see if a specific form or document is required.
Conflicts between Directives and Family Desires
This refers to a conservator of the person, as opposed to a conservator of property, who deals with matters relating to an individual's property and assets and so is not the subject of this discussion (see Chapter 18, for further discussion at the end of 2010). life issues). An example of a typical LW document is presented in Box 3-3, and an example of a healthcare agent appointment document is presented in Box 3-4.
THE PATIENT SELF-DETERMINATION ACT
Background: The Cruzan Case
Clear and Convincing Proof
Legal and Ethical Issues 43 The Four Significant Provisions of the PSDA
This information must include (1) the individual's rights under state law, whether statutory or case law; and (2) the provider's or organization's written policies regarding the protection of those rights. States must prepare a written description of AMD legislation in their jurisdictions and distribute materials to providers to provide to patients in accordance with PSDA requirements.
Nurses’ Responsibilities
The information must be provided by hospitals at the time of admission, nursing facilities at the time of admission as a resident, hospice programs at the time of initial receipt of hospice care, health care facilities at the time of enrollment, and home health care. health authorities, before the individual comes under the care of the authorities. The DHHS Secretary was also required to develop and implement a national campaign to inform the public about the opportunity to perform AMDs and the patient's right to participate and direct his or her health care decisions .
Problems and Ethical Dilemmas Associated with Implementation of the PSDA
If the patient or resident is incapacitated upon admission, the requested information may be provided to a family member or responsible party, but the material must be provided to the patient or resident when they are no longer incapacitated. This ensures that the patient's wishes are respected and maintains the integrity of the physician and practitioner.
VALUES HISTORY
It is important that the nurse facilitates this process using the professional skills and insight required to comply with the PSDA in such circumstances (Stillman et al., 2005). The nurse should be alert to opportunities to obtain information from both patients and their families or caregivers to gauge their level of understanding.
NURSES’ ETHICAL CODE AND END-OF-LIFE CARE
Legal and Ethical Issues 45
The state nursing association can take action against a nurse who has committed a violation of the code of ethics. Care for the terminally ill and dying must be done with professional and ethical considerations.
Ethical Dilemmas and Considerations Euthanasia, Suicide, and Assisted Suicide
Maintaining mutual respect among practitioners in this field is undoubtedly one of the best ways to bring respect to the profession and to yourself. The research review board's diligent efforts consider not only these laws and regulations, but also their application to the specific benefits of the proposed research.
Organ Donation
Only a full review of the research, including legal analysis, determines whether a waiver of informed consent can be justified. A nurse involved in any aspect of human research should ask to see the details of the proposed study and the deliberations and decision of the institutional review board.
Ethics Committees
Legal and Ethical Issues 47
- You are the nurse in charge of a wing of a nursing facility
This chapter presents the legal and ethical issues associated with nursing care for the elderly. During the initial assessment, inform homebound elderly people and their caregivers about the rights of home care patients.
Legal and Ethical Issues 49
The purpose of this form is to help you think about and write down what is important to you about your health. If at some point you become unable to make health care decisions for yourself, your thoughts as expressed on this form can help others make a decision for you that is consistent with what you would have chosen.
APPENDIX 3A Values History Form
- Written Legal Documents
- Wishes Concerning Specific Medical Procedures
- Legal and Ethical Issues 51 Cardiopulmonary Resuscitation (CPR)
- General Comments
- Your Overall Attitude toward Your Health
- Your Perception of the Role of Your Doctor and Other Health Caregivers
- Your Thoughts about Independence and Control
- Your Personal Relationships
- Your Overall Attitude toward Life
- Your Attitude toward Illness, Dying, and Death
- Your Religious Background and Beliefs
- Legal and Ethical Issues 53
- Your Living Environment
- Your Wishes Concerning Your Funeral
Do you want to make general comments about the value of independence and control in your life? Do you have any general comments to make about your relationship to illness, dying, and death?
OPTIONAL QUESTIONS
Do you want to make general comments regarding your finances and health care costs? Do you wish to make general comments on how you would like your funeral and burial or cremation to be arranged or carried out.
SUGGESTIONS FOR USE
The nursing process is a problem-solving process that represents the organizational framework for nursing practice. If the assessment approach does not maintain a nursing focus, the sequential steps of the nursing process—diagnosis, planning, implementation, and evaluation—cannot be accomplished.
Gerontologic Assessment
Gerontologic Assessment 55
A comprehensive, nursing-focused assessment of these responses provides a database of a patient's ability to meet the full range of physical and psychosocial needs. In 2004, Nursing: Scope and Standards of Practice resumed a revision process that resulted in the ANA's expectations of the professional role in which all registered nurses should practice.
SPECIAL CONSIDERATIONS AFFECTING ASSESSMENT
The ANA (2004) stated, "The goal is to improve the health and well-being of all individuals, communities, and populations through the significant and visible contributions of registered nurses using standards-based practice." Registered nurses use the nursing process to plan and provide individualized care to their healthcare consumers.
INTERRELATIONSHIP BETWEEN PHYSICAL AND PSYCHOSOCIAL ASPECTS OF AGING
Furthermore, the cause of one problem is often best understood in light of its associated problems. Careful consideration of the interrelationships between physical and psychosocial aspects in each patient situation is therefore essential.
NATURE OF DISEASE AND DISABILITY AND THEIR EFFECTS ON FUNCTIONAL STATUS
Decreased Efficiency of Homeostatic Mechanisms
Lack of Standards for Health and Illness Norms
Gerontologic Assessment 57
To compensate for the lack of definitive standards, the nurse must first assume heterogeneity rather than homogeneity when caring for the elderly. The experiences of the elderly represent a rich and broad background that the nurse can use to develop an individualized plan of care.
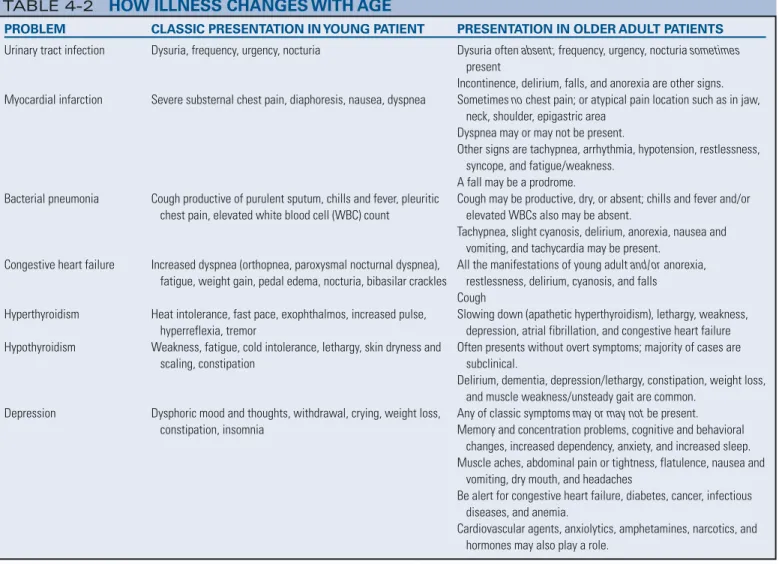
Altered Presentation of and Response to Specific Diseases
Gerontologic Assessment 59
Assessment can be complex due to the multiple characteristics associated with an ACS and dementia. Therefore, the nurse must have a clear understanding of the differences between an ACS and dementia and must recognize that only subtle evidence may be present to indicate the existence of a problem.
TAILORING THE NURSING ASSESSMENT TO THE OLDER PERSON
Use body language, touch, eye contact and speech to promote the patient's maximum degree of participation. Be aware of the patient's emotional state and concerns; fear, anxiety and boredom can lead to inaccurate assessment conclusions regarding functional ability.
THE HEALTH HISTORY
Maximize the use of silence to allow the patient time to collect thoughts before responding. Interview family, friends, and significant others involved in the patient's care to validate assessment data.
The Interviewer
Gerontologic Assessment 63
For example, a belief that older adults do not engage in sexual relationships may result in the nurse failing to interview the patient about sexual health conditions (see Chapter 13). Regardless of the nurse's good intentions, older adults may perceive the use of such terms as overly familiar, ill-mannered, or inappropriate.
Gerontologic Assessment 65
The Patient
The Health History Format
Gerontologic Assessment 67
Any nursing interventions for the patient must be planned with consideration of the living environment. The chief complaint, stated in the patient's own words, enables the nurse to identify specifically why the patient is seeking health care.
Gerontologic Assessment 69
To reduce confusion and ensure the collection of accurate data, the nurse should ask the patient for only one piece of information at a time. Information obtained here alerts the nurse on what to focus on during the physical examination.
The Physical Assessment Approach and Sequence
Gerontologic Assessment 71
Equipment and Skills
ADDITIONAL ASSESSMENT MEASURES
Functional Status Assessment
Gerontologic Assessment 75
Research is being conducted to determine the effectiveness of this age-specific, comprehensive approach to reducing morbidity and mortality associated with hospitalization of older adults. Nurses practicing in all settings should begin to incorporate the tools already mentioned, as well as others described in the comprehensive text by Kane and Kane (1981), into routine assessments to determine a patient's baseline functional ability.
Cognitive or Affective Assessment
Gerontologic Assessment 77
Each item is rated using a four-point scale to indicate the intensity of the symptom. The instruments described here for assessing cognitive and affective status are valuable screening tools that the nurse can use to supplement other assessments.
Social Assessment
Gerontologic Assessment 79
2 Someone who would take care of the subject for a short time (from a few weeks to six months). 1 Someone who would help the subject from time to time (taking him to the doctor or fixing lunch, etc.) Did not respond.
LABORATORY DATA
Gerontologic Assessment 81
To compensate for the lack of definitive standards for what is "normal" in older adults, the nurse can compare. A brief portable mental status questionnaire for the assessment of organic brain deficit in elderly patients.
Cultural Influences
DIVERSITY OF THE OLDER ADULT POPULATION IN THE UNITED STATES
States vary depending on global politics; older adults are continually reunited with their adult children; they can live in the household of their adult children, where they help with housework and care for the younger children in the family, and are cared for in return. Now and in the future, nurses can provide care to older adults from multiple ethnic groups in one day.
CULTURALLY SENSITIVE GERONTOLOGIC NURSING CARE
It is likely that many of these older adults do not speak the same language as the nurse.

Awareness
Knowledge
Cultural Concepts
Cultural Influences 87
Culture is universal, adaptive and exists at the micro level of the individual or family and at the macro level in the form of a region, a country or a specific group. Incorporate this data into the plan of care to meet the cultural needs of the individual and family.
Cultural Influences 89
Beliefs about Health and Illness
Cultural Influences 91
According to the theory of hot and cold, the disease can be defined as "hot" or "cold". The treatment provided (including food) must be balanced with the disease to be effective. In most cultures, older adults are likely to self-medicate informally for known or chronic illnesses that have been successfully treated in the past, based on one or more of the beliefs just described.
Transcending Cultural Concepts
Others may only have access to this private information with the express permission of the owner. The nurse's main concern is the woman's health, and the woman's concern is her family.
SKILLS
The Health Insurance Portability and Accountability Act (HIPAA) further codified the role of the individual as the ultimate “owner” of health information (National Institutes of Health, 2014). Body language is more important than spoken words because that is where the true meaning of the communication is considered to lie.
Handshake
Cultural Influences 93
Eye Contact
Interpreters
PUTTING IT TOGETHER
Leininger
Cultural care reform or restructuring refers to those supportive, supporting, facilitating or enabling professional actions and decisions that help patients rearrange, change or greatly change their life paths for new, different and beneficial health care patterns, while maintaining their cultural values and beliefs and still providing beneficial or healthier ways of life than existed before the changes were established (Leininger, 1991). This theory can be used with individuals, families, groups, communities and institutions in diverse healthcare delivery systems.
The Explanatory Model
Cultural Influences 95
The LEARN Model
- In what ways do you value diversity in the world around you?
- What are the limitations of using only race or ethnicity in identifying older patients?
- Interview two or more older patients from the same ethnic group and discuss their cultural adaptation
- Identify your ethnocentric views toward certain groups and the basis on which you have formulated them
- What knowledge must the nurse possess to avoid stereotyp- ing or generalizing about older patients?
- How would you respond to a colleague who just made a racist remark or joke?
- How would you recognize cultural conflict? How would you respond to it?
- What are the nurse’s responsibilities when discussing the use of alternative healing practices, medicines, and nutri-
- What responsibilities do you have with an older patient who does not speak English?
Interview two or more elderly patients from the same ethnic group and discuss their cultural adjustment. What specific cultural nursing skills are needed when caring for older patients from a different ethnic group.
Family Influences
Family Influences 99
Likewise, less than half of American workers are considered “eligible” under the law (Yang & Grimm, 2013).
COMMON LATE-LIFE FAMILY ISSUES AND DECISIONS
Changes in Living Arrangements
Is my family member concerned about the impact of the costs on his or my personal financial resources? Are the requirements of community agencies – financial disclosure, application process, interviews – too much for my family member.
Making a Decision About a Care Facility
Family Influences 101
The decision to move an elderly family member into a care facility is difficult for most families. Guilt can arise from a variety of sources, including (1) pressure and comments from others (“I would never put my mother in a care facility” or “If you really loved me, you would take care of me”); (2) family tradition and values (“My family has always believed in taking care of themselves – and that means providing care to family members at home”); (3) the meaning of placement in a nursing home ('I'm leaving my husband', 'I should be able to take care of my mother. She took care of me when I needed care', or 'You don't put someone you love in a nursing home”); and (4) promises (“I promised Mom that I would always take care of Dad,” or “When I got married, I promised 'till death do us part”).
Financial and Legal Concerns
Cultural considerations may also influence feelings about placement. A common feeling family express when faced with care facility placement is guilt. For many people, walking into a care facility for the first time is not easy.
End-of-Life Health Care Decisions
Family Influences 103
Nursing care at end-of-life by health professionals differs greatly from that provided by family members. Families generally do not have the same life experiences to draw on in these situations.
The Issue of Driving
For health professionals, there is usually a wealth of experience available to draw from and support colleagues to share in the burdens. Complex treatment regimens must be balanced with complex interpersonal relationships with the patient and other family members.
Family Caregiving
Family Influences 105
The next questions were: "Where did they realistically expect to go if they were bedridden, or who would they actually expect to take care of them?" The last question was: "What was the discrepancy between what they wanted and what likely to happen if we remained confined to the bed?”, if at all. As nursing home placement becomes a reality for older adults, nurses must be aware of the personal and family dynamics involved in the decision-making process.
INTERVENTIONS TO SUPPORT FAMILY CAREGIVERS
Family Influences 107
This includes making legal and financial plans and considering changes in the current care situation, including possible placement of nursing facilities. It is important to discuss the barriers that caregivers may face in the real world and ways to overcome these barriers.
Respite Programs
Men, on the other hand, may feel less confident in the role of caregiver and may perceive that they lack the skills needed to care for someone else. Just as employees benefit from regular vacations and breaks, caregivers benefit from a "break" from work.
Support Groups
Family Influences 109 BOX 6-4 VIDEO RESPITE: AN INNOVATIVE CAREGIVER RESOURCE
Questions, pauses and feedback from 'the visitor' stimulate the involvement and conversation of the person with a memory disorder. As one caregiver said, “The DVDs make me feel like I'm doing something positive for mom.”
Family Meetings
Balance - supports group members learn to balance their own needs against those of their relatives. Individuality - group members understand that although some issues are the same, each person's circumstances may be unique.
WORKING WITH FAMILIES OF OLDER ADULTS
CONSIDERATIONS AND STRATEGIES Identifying Who the Patient Is and Who
Family Influences 111
However, it is easy to become frustrated and angry – and eventually experience burnout – if older people or families choose a course of action that the nurse feels is not best. Remember that nurses have not failed when an older person or family chooses an option that differs from the nurse's recommendation.
Assessing the Family
Family Influences 113
Providing care for a family member can be more difficult if the caregiver has been the dependent in the relationship. Other useful areas to assess are a caregiver's coping style; caregiver support system; the caregiver's assessment of the adequacy of his/her support system; the care needs of the older person, including behavioral and emotional problems, and the caregiver's perception of these care needs; and financial resources.
Encouraging Families to Plan in Advance of Need
Does the older family member give mixed messages about how independent or dependent he or she is? It helps if family members try to imagine what a situation looks and feels like from the older person's perspective.
Involving the Older Person in Decision Making
Family members often express concern by using “you” messages, that is, telling the person what to do or not to do. Family members may also need help with active listening and empathy, that is, with understanding the feelings and emotional needs of the elderly person.
Validating Feelings
Family Influences 115
The increasing vulnerability of an elderly relative can become a daily reminder of that person's mortality—and of a caregiver's own mortality. A nurse should emphasize that feelings are neither good nor bad; It's how family members respond to their feelings that makes a difference.
Addressing Feelings of Guilt
It may not be easy to accept that "my husband is no longer the strong and powerful man he once was," or "my mother who crochets beautifully now doesn't know what to do with a crochet." It is especially painful when a family member is no longer recognized by the person with Alzheimer's disease or a related disorder. Because feelings, beliefs, and attitudes influence behavior, it is important to address the belief systems and feelings of family members.
Emphasizing Goodness of Intent of Actions
Family members may also need to adjust their perception of the sick person, and this can be emotionally painful. When emotions are not addressed, decisions are more likely to be made on the basis of guilt, promises and "shoulds and shouldn'ts" rather than on the circumstances and what is best for everyone.
Recognizing the Nurse’s Role as Permission Giver
It's okay not to love (or like) the elderly person who needs care. Relatives should ask: "If my health deteriorates or I die, what will happen to my family member?".
Recommending a Decision-Making Model to Families
- Gathering Information
- Formulating Options
- Evaluating Options
- Creating a Plan
- Family Influences 117
- Implementing the Plan
- Reassessing
- Think about your own family relationships. What individual and family values might influence your care of an older adult
- Family Influences 119
Providing high-quality care for older adults requires recognizing the role of the family and assessing and responding to the needs of family members, especially caregivers. When working with older adults, it is as important to address the needs of the family as it is to focus on the needs of the older person.
Socioeconomic and Environmental Influences
Socioeconomic and Environmental Influences 121
To be an effective advocate, the nurse must understand the factors that shape the older consumer's perception of the environment, socioeconomic status, and access to health care.
SOCIOECONOMIC FACTORS Age Cohorts
Income Sources
Socioeconomic and Environmental Influences 123
Most women in this age group have not worked outside the home, so their income depends on spousal pensions or social security benefits. Together, these factors reduce the income range of most people in this age group.
Surviving spouses without work experience receive approximately two-thirds of the total income earned before their spouse's death (Wapner et al., 1990).
Poverty
Socioeconomic and Environmental Influences 125 Health Status
Nurses work with older adults to prolong independence by encouraging self-management of chronic conditions. Education and support help older adults make informed choices, practice positive health behaviors, and take responsibility for caring for a chronic condition.
Insurance Coverage
Those older adults who are still working can still be covered by their employers' health insurance plans. For eligible older adults residing in nursing facilities, coverage covers health care-related care and other services not available in the community due to their mental or physical conditions.
Support Systems
Socioeconomic and Environmental Influences 127
These roles can become blurred in older adults' marriages as illnesses and disabilities increase, forcing role changes. About half of older adults in the United States live within 25 miles of a child; although this figure varies, depending on marital status and employment (Pollak, 2010).
Benefits and Entitlements
These individuals are more likely to believe that others will help if needed. Friends and family of depressed or negative older adults may find it difficult to keep in touch with them because of the behavior these older adults exhibit.
Area Agencies on Aging
As the population has aged, the large number of veterans from World War II has put a strain on VA health care facilities. Veterans seeking health care due to a war-related injury or illness are given priority.
Conservators and Guardians
Those who need long-term care are now being referred back to their communities for that care until an opening is available at a VA health center. With the large number of amputees with loss of one or more limbs, this group of veterans will become another large group in need of geriatric care in the future (Figure 7-3).
ENVIRONMENTAL INFLUENCES
Socioeconomic and Environmental Influences 129
Geographic Location of Residence
Transportation
Housing
Socioeconomic and Environmental Influences 131
Older people may move because of the loss of a spouse, health, home, or functional independence. Depression, withdrawal, confusion, increased dependency, low life satisfaction, and increased health problems can result from a move, especially if older adults are unprepared or the move is unexpected.
Criminal Victimization
Socioeconomic and Environmental Influences 133
Volunteer action programs, such as a neighborhood watch, help with prevention and also make older people feel safer. It is important that older people have control over their environment and have a voice in the community.
ADVOCACY
Socioeconomic and Environmental Influences 135
- A 69-year-old chronically ill woman has few financial resources, no formal education, and only one child who
Older adults' perception of the healthcare system as a whole is influenced by experience. The nurse can also encourage the older adult's informal support systems of friends and family.
Socioeconomic and Environmental Influences 137
APPENDIX 7A Resources
ORGANIZATIONS OF PROFESSIONALS WORKING IN THE FIELD OF AGING
ORGANIZATIONS OF BOTH PROFESSIONALS AND OLDER ADULTS
The goal of health promotion and disease prevention is to reduce the potential years of life lost due to premature death and to ensure a higher quality of remaining life. Health promotion and disease prevention activities include primary prevention, or preventing diseases before they occur, and secondary prevention, which is detecting diseases at their early stages.
Health Promotion and Illness/Disability Prevention
Health Promotion and Illness/Disability Prevention 141
MODELS OF HEALTH PROMOTION
BARRIERS TO HEALTH PROMOTION AND DISEASE PREVENTION
Health Care Professionals’ Barriers to Health Promotion
Older Adults’ Barriers to Health Promotion
In addition, older adults incur costs for many preventive services because Medicare does not cover them all (Table 8-2). It is therefore useful to use an individualized approach to health promotion in older adults (Resnick & McLeskey, 2008).
HEALTH PROTECTION
Therefore, it appears that there may be sample-specific differences in which factors influence health-promoting behavior. This creates barriers to programs; for example, some programs require older adults to give up personal and family privacy to obtain individual services.
DISEASE PREVENTION Primary Preventive Measures
Health Promotion and Illness/Disability Prevention 143
Polypharmacy is the use of large amounts of different drugs to relieve symptoms of a medical condition or symptoms resulting from drug treatment (Lacasse, 2011). Polypharmacy is complicated by the use of generic drugs or the substitution of over-the-counter drugs that are less potent than prescription drugs.
Secondary Preventive Measures
However, it should be noted that the Centers for Disease Control and Prevention (CDC) does not recommend routine revaccination of immunocompetent older adults; Persons age 65 and older should be given a second vaccine only if they received the vaccine more than 5 years ago and were younger than age 65 at the time of the primary vaccination (CDC, 2008). The USPSTF also provides guidelines regarding screening for cardiovascular disease, osteoporosis, diabetes, and obesity (USPSTF, 2008).
Tertiary Preventive Measures
Health Promotion and Illness/Disability Prevention 145
THE NURSE’S ROLE IN HEALTH PROMOTION AND DISEASE PREVENTION
Requisite Knowledge
Regionally, a nurse can begin to get involved by contacting the state department on aging regarding rules and regulations for the care of older adults. Meetings with legislators can be an opportunity for a nurse to express opinions regarding health issues.
Assessment
Another way to get involved is by attending and interacting at state legislature meetings and hearings. Some states have designated an annual nurse lobbying day in the state capital.
Self-Perception or Self-Concept Pattern
This education may include (1) becoming aware of current and changing social policy, (2) studying the facts and the opinions of leaders on all sides of an issue, (3) interacting with civic groups, political party groups and senior citizen groups to speak. , (4) to testify before the legislature as an advocate for healthy aging, (5) be informed about the issues and know social and political hot buttons, (6) put the best foot forward with lobbying, (7) issues and techniques of negotiation and compromise, and (8) active support of the role of the advanced practice nurse working with physicians as a primary provider of health care.
Roles or Relationships Pattern
Health Perception or Health Management Pattern
Health Promotion and Illness/Disability Prevention 147
Nutritional or Metabolic Pattern
Coping or Stress-Tolerance Pattern
Cognitive or Perceptual Pattern
Value or Belief Pattern
Description: This pattern includes health promotion information that encourages the older adult to achieve the recommended 30 minutes of daily physical activity on most days of the week. In addition, assess daily routines and activities, including exercise patterns, leisure habits, recreation, and hobbies; and inquire about any limitations or changes to these patterns.
Rest or Sleep Pattern
Subjective: Screening for safety related to exercise and physical activity using screening measures such as the Exercise Assessment and Screening for You (EASY) (EASY Screening Group, 2007; Resnick et al., 2008; Sherrington, Tiedemann, Fairhall, Close & Lord, 2011 ). Assess for pain, fatigue and fear of falling and fall potential, and take a falls history.
Sexuality or Reproductive Pattern
The EASY determines whether it is safe for an individual to start an exercise program immediately and, depending on accompanying conditions, matches the individual with a useful exercise program that can be printed from the web, thus providing him or her with a hard copy in use. Assess self-care ability by observing and asking the patient about self-care activities such as bathing, dressing, toileting and feeding, if possible.
Elimination Pattern
Planning
Implementation
Health Promotion and Illness/Disability Prevention 149
Seeking activities, places, and means to convey health promotion information to a group of older adults is an example of implementing a proactive attitude. Annual health promotion screenings may be incorporated into programs that provide vaccinations to older adults and may include screenings for bowel cancer, diabetes, osteoporosis, and macular degeneration, as appropriate.
Evaluation
SUPPORTING EMPOWERMENT OF OLDER ADULTS
Health Promotion and Illness/Disability Prevention 151
- Several nurses have volunteered to give flu shots to older adults at a senior center. When the line to receive the injec-
Exercise to prevent falls in older adults: an updated meta-analysis and best practice recommendations. Perceptions and beliefs about the role of physical activity and nutrition on brain health in older adults.
WEBSITES
Testing the Senior Self-Efficacy Pilot Project (SESEP) for use with urban minority older adults. A new screening paradigm and tool: the Exercise/Physical Activity Assessment and Screening for You (EASY).
Health Care Delivery Settings and Older Adults
A discussion of home and community health care for older adults includes topics related to the health care needs of community-dwelling older adults, community-based services, and the role of home health agencies and hospice nurses in community-based care for this population. A health care facility is the predominant setting in which long-term care is provided for people who require regular or ongoing skilled nursing care.
CHARACTERISTICS OF OLDER ADULTS IN ACUTE CARE
CHARACTERISTICS OF THE ACUTE CARE ENVIRONMENT
Philosophy of Care
Risks of Hospitalization Adverse Drug Reactions
Health Care Delivery Settings and Older Adults 155
Older adults generally are more vulnerable to infections because of physiological changes in the immune system and underlying chronic diseases (see Chapter 15). Older adults are at increased risk for colonization and infection with antibiotic-resistant strains of organisms (Merck Manual of Geriatrics, 2013), such as methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE).
Safety Features
Other common sites of infection in hospitalized elderly are skin, soft tissue, wounds, gastrointestinal tract, and blood. When older adults are hospitalized, immobilization due to forced bed rest or restraint often results in functional incapacity.
NURSING IN THE ACUTE CARE SETTING
Hospital-acquired pneumonia is the second most common HCAI, symptoms in older adults are often mental changes or confusion making diagnosis more challenging (Dougdale, 2012). Gerontological nurses must be leaders in advocating for more appropriate care and treatment of hospitalized older adults to prevent or at least reduce the incidence of iatrogenic disease.
Nursing-Specific Competency and Expertise
The quality of the nursing care provided is influenced by the philosophy of nursing, the nursing-specific competence and expertise of the nursing staff, and the various aspects of the nursing role implemented in acute care.
Critical Care and Trauma Care
Health Care Delivery Settings and Older Adults 157
Two additional issues for the critical care of older adults are prevention of nutritional compromise and recognition of adverse drug reactions. Up to 65% of hospitalized older adults are malnourished on admission or acquire nutritional deficits during their hospital stay (Monkhouse, 2013).
HOME CARE AND HOSPICE
Thermoregulatory mechanisms become impaired as a person ages, and older adults with trauma are particularly vulnerable. Research supports the fact that older adults are at greater risk of complications and higher mortality, even when the injuries are not severe (Legome & Shockley, 2011).
FACTORS AFFECTING THE HEALTH CARE NEEDS OF NONINSTITUTIONALIZED OLDER
Home health continues to be a way of helping the older adult with a physical or cognitive impairment to stay at home. Due to changes in reimbursement for federal programs that provide services to older adults and limited funding for state programs, home nurses are challenged to use interventions that are both effective and cost-effective.
Cognitive Function
Housing Options for Older Adults
Health Care Delivery Settings and Older Adults 159
COMMUNITY-BASED SERVICES
Use of Community and Home-Based Services by Older Adults
The type of services needed, the availability of the services, the cost of the services, and the requirements to qualify for the services are determined by a home health agency. In other situations, case management services are provided by formal organizations such as home health agencies or managed care agencies.
Profile of Community- and Home-Based Services Area Agencies on Aging
Health Care Delivery Settings and Older Adults 161
Adult day care services provide a variety of health and social services to older adults living alone or with their families in the community. In addition, many facilities that serve older adults (eg, adult day care services, senior centers, and health facilities) have their own transportation services.
HOME HEALTH CARE
The central reporting station then contacts pre-designated persons or the police, who respond to the emergency. They are not recommended for persons with dementia as resetting the device is very difficult and the device may activate too often without emergency response.
Home Health Agency
A PERS consists of a small device that is worn on the body and, when activated, will send an alarm to a central monitoring station. Because these devices are relatively expensive, they are not a practical alternative for older adults in lower-income groups.
Proprietary Agencies
Facility-Based Agencies
Health Care Delivery Settings and Older Adults 163
With the introduction of Medicare and Medicaid in 1966, nurses were able to offer more home care to the sick and disabled. What defines a home care facility from a Medicare perspective is whether it receives a facility overhead allowance.
Visiting Nurse Associations
Hospital-based home care agencies were few in number until the passage of Medicare reform (OBRA, in 1987), when hospitals began to be paid for patients receiving Medicare benefits based on DRGs. According to The Joint Commission (2012), a facility-based home care agency shows evidence of an organizational and functional relationship between the home care agency and the facility or public representation of the home care agency as a facility service.
Benefits of Home Care
With shorter lengths of stay, hospitals have established home care agencies or affiliated with existing home care agencies to provide options for patients going home with existing health care needs.
CONTINUITY OF CARE
What really matters is that the client is assessed for home care needs before he or she leaves the hospital. Identification of the primary care physician (PCP) or the PCMH who will sign the home care orders.
Role of the Home Care Agency
Health Care Delivery Settings and Older Adults 165
Some tasks are carried out according to geographical areas, the client's special needs or the nurse's specialty.
IMPLEMENTING THE PLAN OF TREATMENT The Nurse’s Role
Role of the Home Health Aide
OASIS
HOSPICE
Hospice Philosophy
Health Care Delivery Settings and Older Adults 167
Depending on the needs of the dying person and their family, other levels of care are available. For example, a dying person and their family may initially choose to care for the dying person at home with hospice support.
OVERVIEW OF LONG-TERM CARE Definition
Family members care for the dying person 24 hours a day, and the hospice team consults and supports the family in their commitment to caring for the hospice client. The transition between care locations should be seamless with the help of the hospice team.
Factors Associated with Institutionalization
Long-term care settings can be classified on a continuum based on the complexity of care provided and the amount of skilled care and services required by residents. They stay for a short time to recover from an acute illness, injury or surgery and then return home.
Medical and Psychosocial Models of Care
Health Care Delivery Settings and Older Adults 169
The baccalaureate-prepared nurse is in a wonderful position to combine his or her knowledge of medicine, nursing, psychology, and sociology into a model that provides truly individualized care to each resident in the nursing facility.
CLINICAL ASPECTS OF THE NURSING FACILITY Resident Rights
Resident Assessment
The RAC signs and certifies the completion of the assessment, but not the accuracy of the assessment data (CMS, 2012b). The overall goal of the RAI is to provide an ongoing, comprehensive assessment of the resident, with an emphasis on functional abilities and physical and psychosocial profile.
Skin Care
Contributions to the RAI are also made by the dietary supervisor, social worker, recreational therapist, medical records clerk, and physical and occupational therapists.
Incontinence
Health Care Delivery Settings and Older Adults 171
Intermittent self-catheterization may be appropriate for residents who are cognitively intact and have adequate manual dexterity. Residents who are terminally ill and those with skin breakdown may also benefit from catheterization.
Nutrition
However, residents with dementia and other cognitive impairments may not benefit from these interventions. Long-term indwelling catheterization is indicated for residents who are unable to empty their bladder and who have not responded to other treatments.
Medications
Treatment programs are resident-oriented and focus on creating changes in lower urinary tract function. These approaches focus on changing caregiver and resident behavior to minimize incontinence.
Rehabilitation
Since the enactment of the OBRA, increasing emphasis has been placed on monitoring the clinical manifestations of polypharmacy, the occurrence of adverse events, and the overuse of “as needed” (prn) drug orders. The routine use of certain medications, including long-acting benzodiazepines, hypnotics, sedatives, anxiolytics, and antipsychotics, has been restricted since the OBRA came into effect.
Infection Control
Health Care Delivery Settings and Older Adults 173
The infection control nurse is the facility's source of information related to the infection control program. Each department and each employee has the responsibility to know and follow the policies and procedures outlined in the infection control program.
Mental Health
Typically, a nurse is designated as the infection control nurse and is responsible for coordinating surveillance, data collection activities, and ongoing educational sessions for the facility (Chami et al., 2011). It is this person's responsibility to obtain and use current information from CDC, OSHA, CMS, and state health departments to ensure that the facility's infection control program is effective and meets standards.
End-of-Life Care
An infection control committee, composed of staff members representing each department, meets monthly or quarterly to review data describing the prevalence and incidence of infection. The policies and procedures include hand washing, standard precautions, respiratory protection, the Bloodborne Pathogen Standard, linen handling, housekeeping, hazardous waste disposal, and the appropriate use of disinfectants, antiseptics, and germicides.
MANAGEMENT ASPECTS OF THE NURSING FACILITY
Special attention is given to residents at high risk of infection (e.g., those who are immobilized, have invasive devices or procedures, have pressure ulcers, have recently been discharged from the hospital, have impaired mental status, or have a nutritional disorder). Personal protective equipment such as gloves, goggles, face shields, aprons, shoe covers and surgical caps must be provided free of charge to employees; they should also be instructed on when and how to use this equipment.
The Nursing Department
Of the RN workforce, 8% work in long-term care facilities (Bureau of Labor Statistics, 2012). The nurse often takes a leadership role in developing policies and procedures, assessing residents' care needs, developing and implementing care plans, and evaluating outcomes.
Nursing Care Delivery Systems
Certified nursing assistants are the largest group of employees in nursing departments and facilities as a whole; Nursing assistants provide up to 80% of the direct care for long-term care residents (National Career Nursing Assistant Network, 2012). However, nurses who choose long-term care as a career must be prepared to operate in a highly regulated industry.
SPECIALTY CARE SETTINGS Assisted Living Programs