What are the social norms and common social practices among elderly men in the affected provinces. Qualitative approaches and involvement of anthropologists/sociologists specializing in the health sociology of the Chinese population may be beneficial. What is the age and gender distribution of severe acute respiratory diseases and key risk factors for respiratory diseases (eg smoking) in the underlying population in the affected provinces.
What is the age and gender distribution of health care utilization in the Chinese population of A(H5N1) cases in China (N=45), where the majority. Three main reasons can be considered for the current distribution of cases: (1) differential exposure between men and women due to gender-related practices and norms; (2) biological differences between men and women in the clinical course after exposure/. Baseline exposure data to LBM among the general population in affected areas are not available.
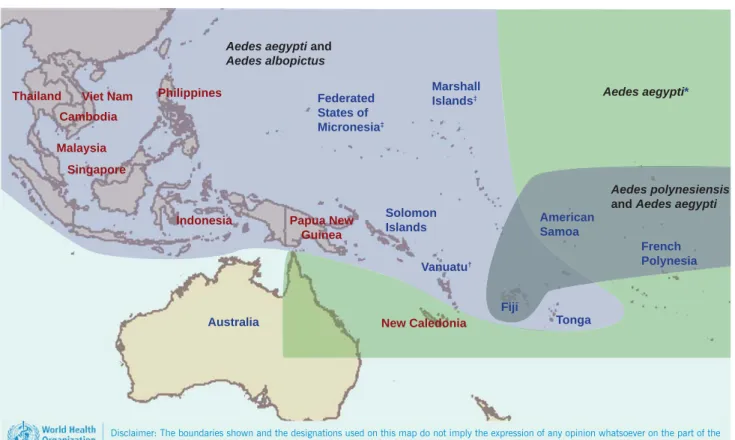
The decrease in the number of cases in Zhejiang and Jiangsu provinces also supports this hypothesis. The ECSA genotype has been the dominant strain throughout Asia and the islands and countries of the Indian Ocean during the last decade. The explosive outbreak of chikungunya in the Indian Ocean islands and the speed with which the related alphavirus, Ross River virus, swept across the Pacific in 1979 and 1980,16 is a reminder of the potential impact CHIKV could have in Oceania (Figure 1 ).
This could have important implications as more than 50% of Papua New Guinea's population lives in the highlands region.

RESULTS
DISCUSSION
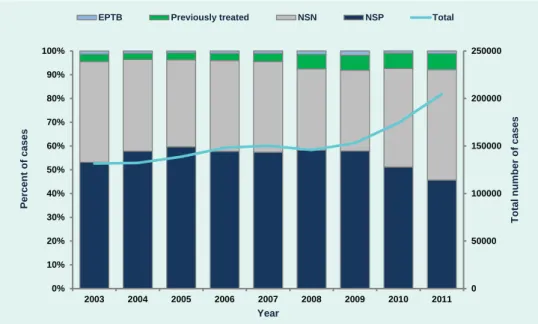
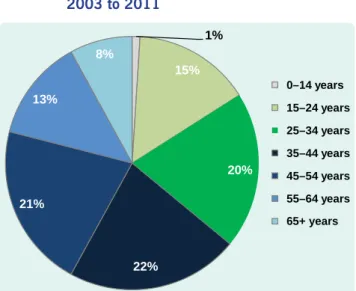
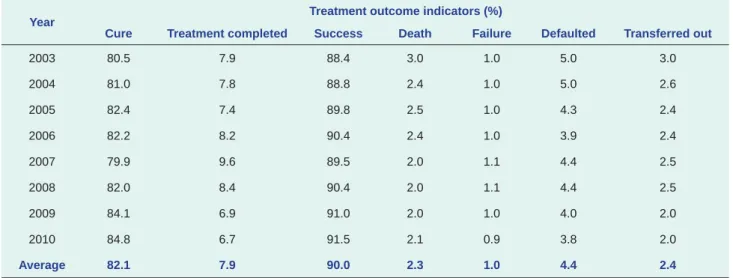
The increase in the number of new stain-negative cases in 2010 and 2011 reflects a change in program priorities to detect all forms of TB following new WHO recommendations issued at that time.9 He explains also the decrease in the percentage of new smear positive cases in 2011. The increasing trend in the number of previously treated cases from 2008 may be due to increased efforts to detect drug-resistant TB cases among these cases. The global target for treatment success rate is 85%,10 this has been exceeded in the Philippines with a diagnostic and treatment service specifically for.
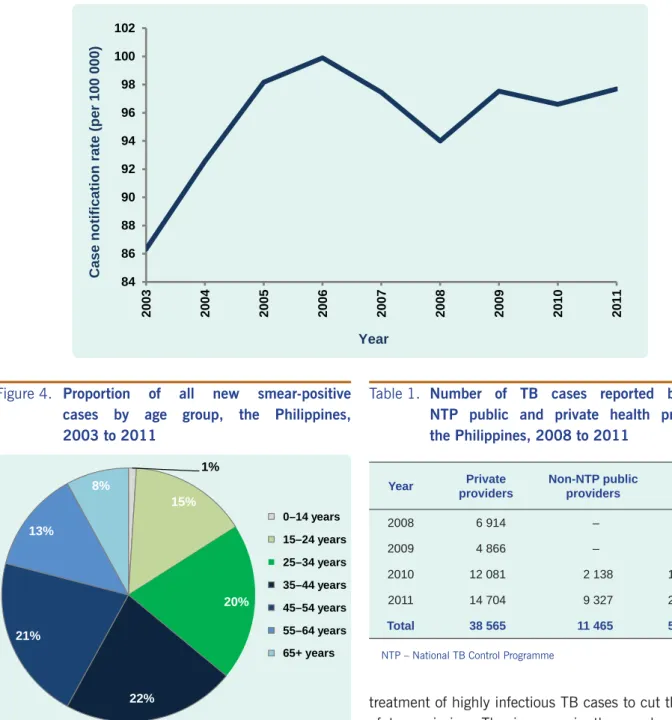
Number of TB cases reported by non-NTP public and private healthcare providers, the Philippines, 2008 to 2011. In this study, EPTB comprised only 1% of cases, compared to the 15% to 20% reported from other countries.12,13 The low detection of EPTB in the Philippines may be due to the limited ability of primary care facilities to diagnose these cases or because EPTB cases are diagnosed in hospitals that are not part of NTP. However, the continued high treatment success rate reflects ongoing efforts to improve case retention through various NTP strategies, such as the administration of DOT in workplaces, homes, and other acceptable locations in the community other than the.
There are some limitations in using NTP surveillance system data to report tuberculosis in the Philippines. Cases diagnosed and treated in health facilities outside the network of NTP providers, including private clinics and hospitals, are not included, so the surveillance system does not report the total number of TB cases in the Philippines.
CONCLUSION
However, women in the same age group were found to access health care more than their male counterparts. Qualitative assessments attributed this distribution to young women being more health-conscious and having greater health-seeking behaviour. Discussion: The excess of male dengue cases in the surveillance data appeared to be associated with a true higher risk of dengue rather than greater access to health care or health-seeking behavior in young men.
This investigation demonstrated the importance of assessing the reported surveillance data within the context of health care utilization behavior of the population under surveillance. Informal, unstructured key informant interviews were conducted among healthcare workers (Savannakhet Provincial Hospital staff, Savannakhet Provincial Epidemiology Unit staff, Othomphone District Health Office staff, Othomphone District Hospital staff and Phin Tai Health Center staff) and local community members (Ban Na village health) volunteer, Ban Na Lao People's Democratic Republic Women's Union Leader, Ban Na Primary school and Secondary School council and teachers). Key questions focused on why specific age and gender groups visited healthcare facilities more than others.
We describe both quantitative and qualitative estimates from the dengue surveillance system and from information on access to health care and health care-seeking behavior. Inpatient and outpatient data from 2010 and 2011 for the 10 most commonly admitted conditions were collected at Savannakhet Provincial Hospital and stratified by age and sex to assess the distribution of health care access by gender. This male excess was observed against a background of greater health care-seeking behavior among their female counterparts.
There was no indication that the excess of male pediatric patients was due to better education and thus better access to health care. This study highlighted the importance of assessing the surveillance data in the context of the health care utilization of the population under surveillance. If anything, when considering the underlying gender-specific health-seeking behavior, the number of dengue cases among young men may be underreported.
Such data would have provided an indication of gender differences in health care-seeking behavior and severity of condition at the time of accessing health care. Also, as gender norms, behavior and access to health care seeking may vary not only between countries but within countries (particularly in the Lao People's Democratic Republic between different ethnic groups and urban versus rural subpopulations),10,14, 20 these findings should not be generalized. Despite these limitations, health care access data and behavioral information indicate that there is unlikely to be an excess of male dengue cases among them.

MATERIALS AND METHODS
Case-series comparisons indicated that women with NTD-affected pregnancies in 2009 and 2010 were less likely to be Caucasian compared to women who had NTD-affected pregnancies in the period 2003-2008. Women with NTD-affected pregnancies in 2009 and 2010 compared with women with NTD-affected pregnancies in the period 2003–2008 were similar. Regional analysis indicated that women with NTD-affected pregnancies in 2009 and 2010 were more likely to have been born in the Middle East and Africa region (P = 0.04).
There was no significant difference in the number of hot days (no hot days compared to at least one hot day) during early pregnancy for women with NTD-affected pregnancies in 2009 and 2010 compared to the 2003-2008 period. This study aimed to examine an observed increase in the number of NTD affected pregnancies reported in South Australia in 2009 and 2010 using routinely collected surveillance data. Women with NTD-affected pregnancies in 2009 and 2010 were less likely to be Caucasian compared to women with NTD-affected pregnancies in 2003-2008.
Women born in the Middle East and African region were more likely in 2009 and 2010 than women born in the Oceania region to have NTD-affected pregnancies. It is likely that the increase in NTD reports reflected a real increase in the number of NTD-affected pregnancies and warranted further investigation. Women with NTD-affected pregnancies in 2009 and 2010 in this study were less likely to be Caucasian and more likely to have been born in the Middle East and African region compared to women who had NTD-affected pregnancies during 2003-2008.
Of women with NTD-affected pregnancies in 2009 and 2010, 69% reported taking folic acid (8% reported not taking folic acid during pregnancy; 23% had missing data). In conclusion, a small but significant increase in the number of women born in the Middle East and African region contributed in part to the observed increase in reports of NTD-affected pregnancies in South Australia in 2009 and 2010. Association of selected persistent organic pollutants substances in the placenta with the risk of neural tube defects.
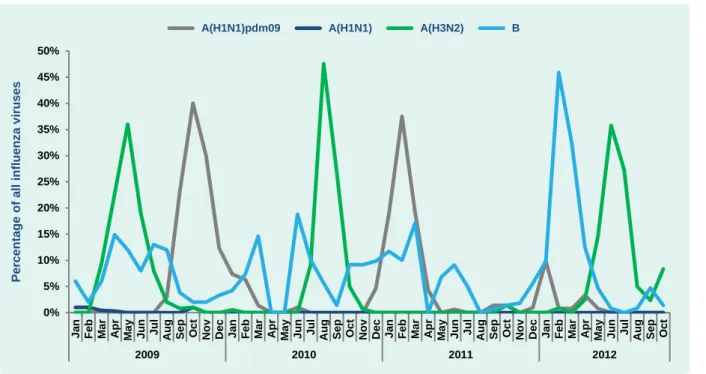
To assess the web-based risk communication response in the WHO Western Pacific Region to the A(H7N9) event in China, we collected public health-related information on A(H7N9) from the countries and territories in the region for the period 30 April to 2 May 2013. A systematic search of government websites for each of the 37 countries and territories of the WHO Western Pacific Region was conducted using Google. Based on officially reported surveillance data, dengue continued to show persistent activity in the Western Pacific region.
This report provides a descriptive summary of dengue cases reported in 2011 by indicator-based surveillance systems from countries and territories in the Western Pacific region. A brief summary of dengue outbreaks in the Federated States of Micronesia and the Marshall Islands is included. Dengue cases, including imported cases, and dengue-attributable deaths in the Western Pacific region, for 2011*.
Number of reported dengue cases and case fatality rates in the Western Pacific Region, 1991 to 2011.