83 Table 2.4 Occurrence of hip fractures in the Asian osteoporosis study 91 Table 2.5 Frequencies of hip fractures in white women in Dundee and Malmö. 167 Table 4.4 Population of eThekwini stratified by ethnicity, gender and age 168 Table 4.5 Ethnically adjusted incidence rates for hip fracture in the south.
Background to the study
- Introduction
- Epidemiology of osteoporotic hip fractures
- BMD and clinical risk factors for osteoporosis
- Problem statement
- Hypothesis
- Objectives
- Methodology
- Significance of study
- Outline of the study
The risk factors and outcomes of osteoporotic hip fractures are similar across ethnic groups. To determine the incidence of hip fractures in the public sector in the eThekwini Metropolitan area.
Literature review
Background
Structure of bone
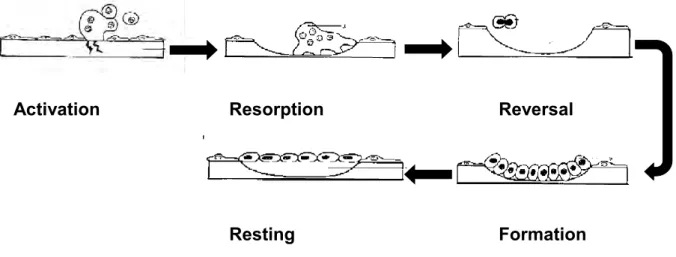
Bone growth, modeling and remodeling
In the kidneys, it decreases calcium excretion and increases the formation of 1,25(OH)2D3, which in turn increases intestinal calcium absorption. Estrogen deficiency results in rapid bone loss especially after menopause due to an increase in the rate of bone remodeling with an imbalance between resorption and formation of BSU, leading to the formation of unfilled bone cavities [112].
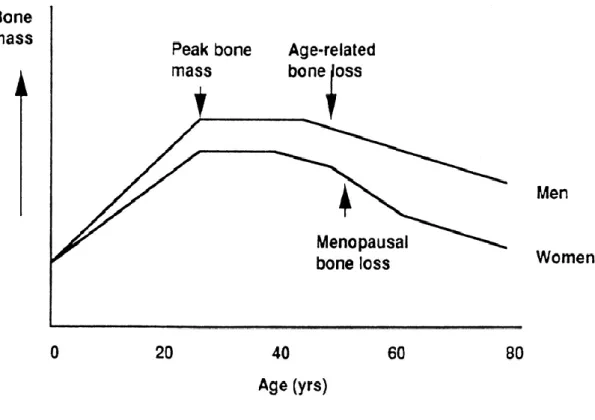
Changes in bone mass with ageing
Other systemic hormones that affect bone metabolism include growth hormone (GH), thyroid hormone, and leptin.
Definition of osteoporosis
Pathogenesis of osteoporosis
Classification of osteoporosis
The net effect is secondary hyperparathyroidism, which increases bone turnover and bone loss [98, 132]. Bone loss associated with menopause was first proposed by Albright et al., [124] and is due to both increased turnover and remodeling imbalance [134].
Consequences of osteoporosis
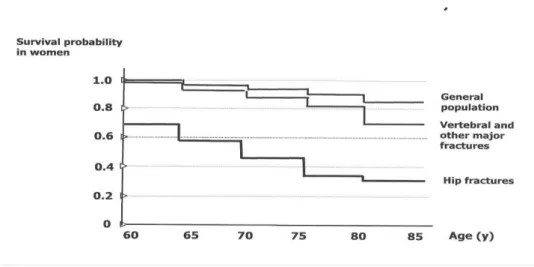
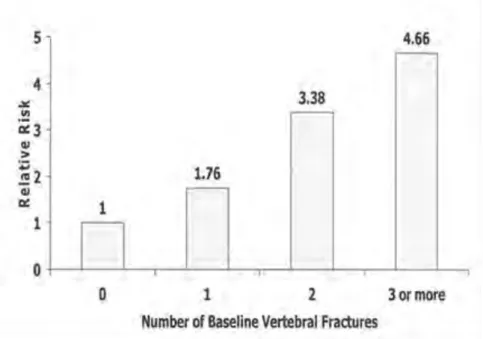
Several well-established risk factors for hip fractures exist [76] and include age, ethnicity, gender, genetics, family history [157], previous fractures, smoking [158] and alcohol [85, 147]. More importantly, compared to the general population, mortality is significantly higher with any osteoporotic fracture and highest in subjects with hip fractures (Fig.
Diagnosis of osteoporosis
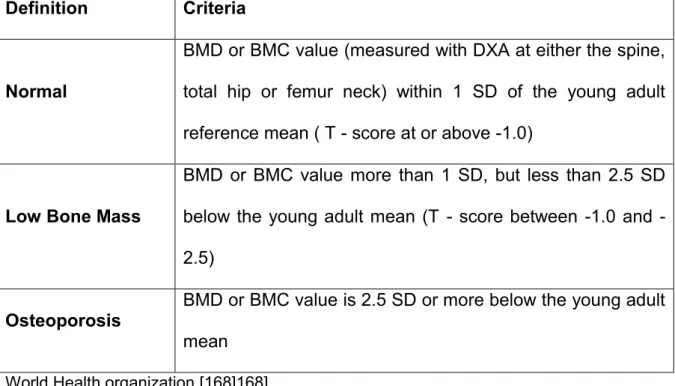
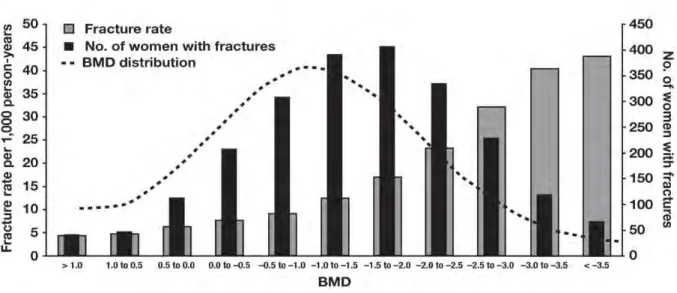
Although the number of fractures increases as BMD decreases, the majority of fractures occur at BMD within the normal or osteopenic range [171]. BMD or BMC value (measured by DXA at the spine, total hip or femoral neck) within 1 SD of the reference mean for young adults (T-score at or above -1.0).
Measurement of bone mineral density
The use of bone markers is further limited by interassay variability and lack of reproducibility. The IOF recommends that the use of bone markers be limited to subjects in whom clinical or BMD data are insufficient to make a diagnosis or to monitor treatment responses over short periods in selected individuals [175]. Biopsy of the iliac crest allows examination of trabecular bone, including cells, the degree of resorption and bone formation.
The use of bone biopsy is limited to case-by-case and research purposes [176].
Fracture risk assessment
These findings support the idea that other risk factors, such as bone turnover, bone geometry, and CRF, increase fracture risk independently of BMD. Bone microarchitecture and bone geometry contribute to bone strength and play a key role in the pathogenesis of osteoporotic fractures. The length of the hip axis, calculated as the distance from the greater trochanter to the inner edge of the pelvis, the width of the femoral neck.
In older women, longer HAL was associated with increased fracture risk, independent of age and BMD [200].
Risk factors for osteoporosis and osteoporotic fractures
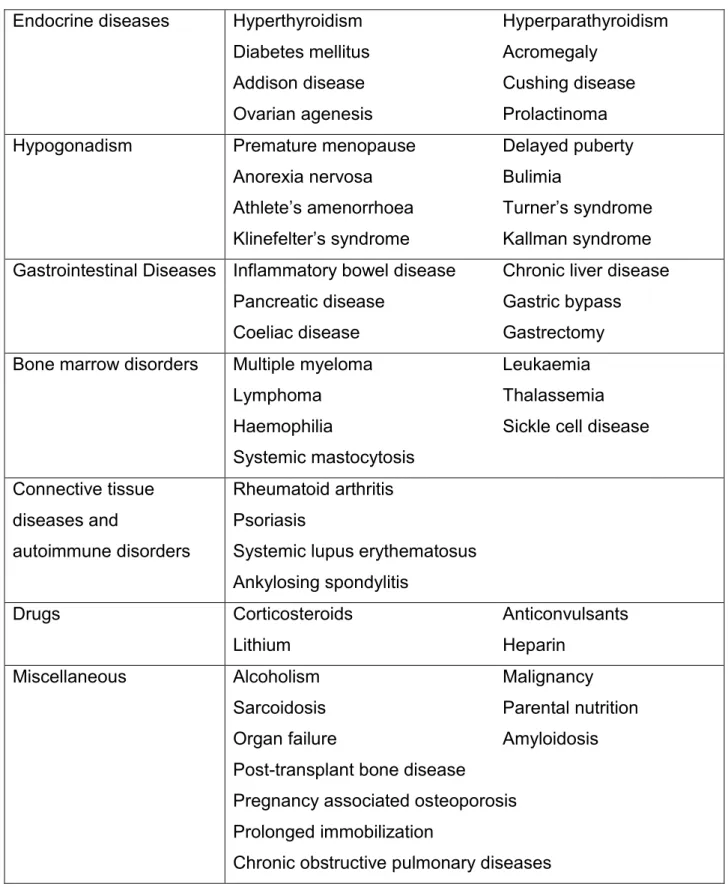
The COLIA 1 Sp 1 polymorphism is associated with decreased BMD and increased risk of vertebral fractures, independent of BMD [211]. An increase in the age-adjusted risk of hip fracture has been reported with lower BMI, independent of age and sex, but dependent on BMD [76, 232]. A number of medical conditions (table) are associated with osteoporosis, while rheumatoid arthritis (RA), diabetes mellitus type 2 (DM), neurological diseases and visual impairment are also independently associated with an increased risk of fracture.
In the Framingham Eye Study, poor visual acuity, cataract and retinopathy were associated with an increased risk of fracture [271].
Cumulative risk factor assessment
Additional clinical risk factors have limited predictive value for future fracture risk [147], as risk factors are not consistent between studies and between developed and developing countries. Clinical risk factors for osteoporosis independent of BMD were identified from 12 large prospective studies (comprising 60,000 women and men) from the United States, Europe, Asia and Australia (Appendix 2.A) [310]. Following recommendations from the IOF and WHO, the fracture risk is expressed as a short-term absolute risk, i.e.
Limitations of FRAX® include: it is not suitable for younger patients with secondary osteoporosis; it excludes important risk factors such as falls, requires technological.
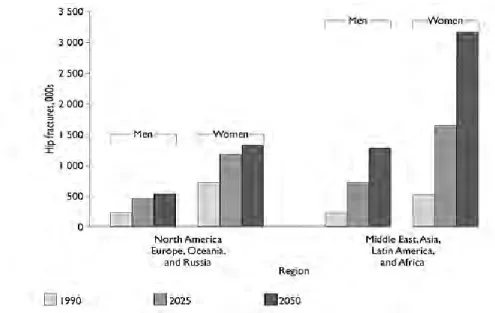
Epidemiology of osteoporosis, hip and vertebral fractures
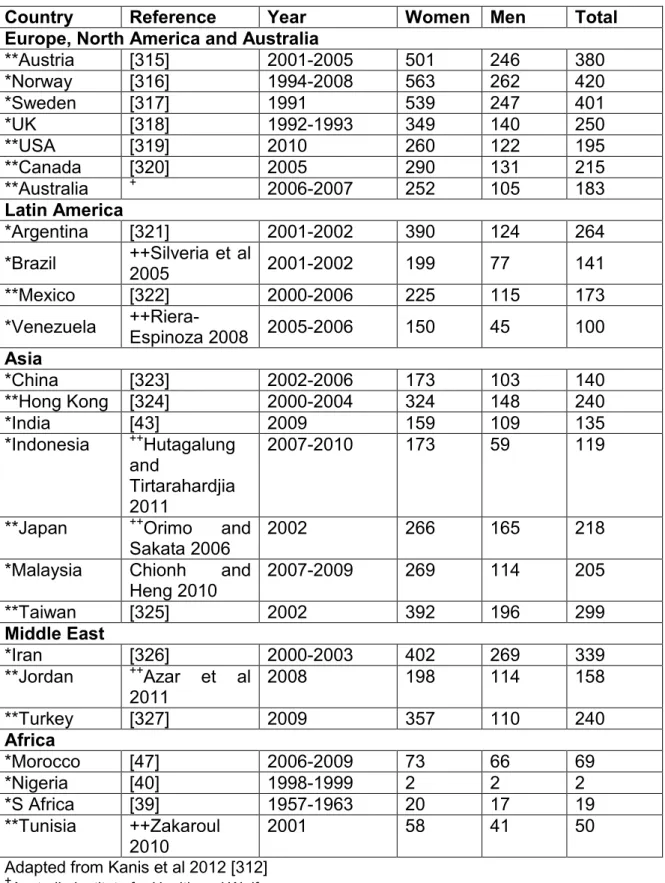
In the Latin American Vertebral Osteoporosis Study (LAVOS), the number of VFs increased with age [360]. Ethnic differences in osteoporosis prevalence and hip fracture rates within and between countries in Asia have been reported. Urbanization is thought to play a role in the higher hip fracture rates in Hong Kong and Singapore [35, 90].
However, there was an unexplained lower incidence of hip and VFs in the older African subjects [385].
Outcome post hip and vertebral fractures
Furthermore, the risk of mortality after fracture was twice that of age-matched controls with the greatest risk seen in the first six months after fracture [184]. While there is agreement that the highest MR is seen in the first six months [405], data on the duration of excessive MR associated with hip fractures are inconsistent with durations ranging from two to twenty years [406]. In the US, 10.3% of hip fracture subjects will experience a second hip fracture in the next three years.
The risk of a subsequent fracture is highest in the first year: 51% of hip fractures occur in the first six months and 75% in the first year [434].
Management of hip fractures
In the immediate post-fracture phase, a clear increase in bone turnover has been observed, resulting in a decrease in BMD in the opposite hip of between 4.6 and 7% over the next year. Despite these conflicting findings and that surgery within 48 hours may be difficult due to operational and cost factors, it has become widely accepted that early surgical repair is recommended and these timing guidelines have also been incorporated into the treatment guidelines for acute hip fractures in SA. by the National Osteoporosis Foundation of SA (NOFSA) [87]. The rate of new VF can be reduced by 40–60% in the first year with appropriate treatment [149].
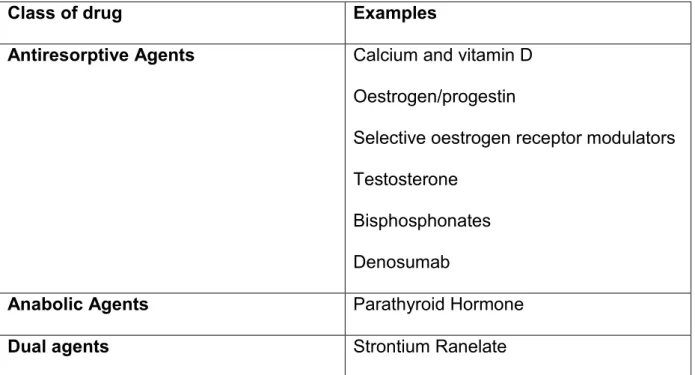
Worryingly, even in the presence of a prior fragility fracture, less than 30% of subjects receive calcium and vitamin D supplements, which are inexpensive and readily available [444].
Health care costs
Similarly, there is little data on the costs of hip fractures in Africa and the Middle East. Costs are generally highest in the first six months to one year, mainly accounted for by hospitalization costs [20, 22] and fall below pre-fracture levels only from year 3 to year 4 [451 ], by which time a significant number of individuals with hip fractures will have died. Length of hospital stay is the most important contributor to cost and can account for up to 84% of the total cost of hip fractures.
However, treating all postmenopausal women at risk for osteoporosis will result in substantial treatment and equate to the cost of treating hip fractures [26].
Assessment and management of osteoporosis in South Africa
Summary of literature review
Methodology
Ethical approval
Study design
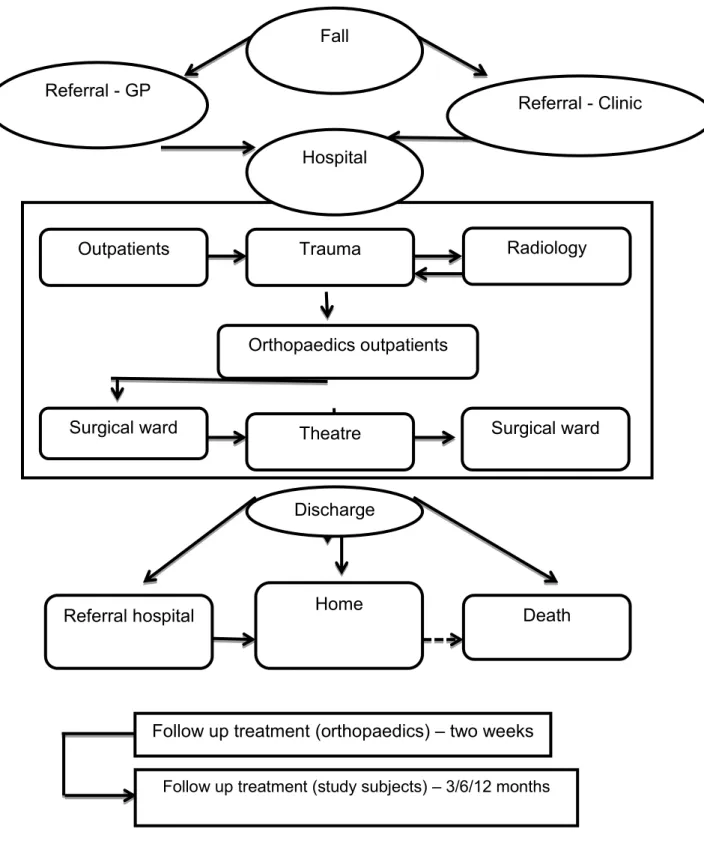
The first phase was a comparative study of subjects aged 60 years and over, with minimal trauma hip fractures admitted to public sector hospitals in the eThekwini catchment area. The subjects were assessed for the presence of established risk factors for osteoporosis and falls and the immediate outcome after hip fracture including health care cost utilization. The second phase was a one-year longitudinal study to determine the outcomes (morbidity and mortality) of the hip fracture subjects.
Study area
This study was conducted in the coastal city of eThekwini (formerly known as Durban) which is the largest city in the province of KZN and has an ethnically mixed population of 3 468 087 people. The African population consists of Nguni (Zulu Xhosa, Ndebele, Swazi), Sotho-Tswana, Tsonga and Venda. Whites include English-speaking descendants from the British Isles, Africans who are descended from Dutch, German and French Huguenots, and immigrant descendants from the rest of Europe.
The city enjoys plenty of sunshine, and the climate is tropical with hot, humid summers and warm winters [468].
Study sites
Sample selection
Recruitment
Sample Size
Inclusion and exclusion criteria
Case identification
These subjects were pre-identified by the study coordinator and only subjects who accepted the study were referred to the investigator. Control cases were recruited consecutively and within one year of hip fracture subject enrollment. All subjects with hip fractures admitted to the selected hospital during the study period were seen within the week of admission.
All subjects admitted with a hip fracture were enrolled, and no subject had died before the initial examination.
Data collection instruments
Sixty-four subjects with hip fractures were unable to stand independently and weigh accurately at the time of discharge. A score above 4 cm predicts a poor outcome and correlates with other functional measures in subjects after hip fracture. Separate anteroposterior (AP) and lateral radiographic views of the spine were obtained using a standardized protocol in 122 subjects with hip fractures at their three-month visit and 197 control subjects on the day of enrollment.
The Hologic Discovery A densitometer was used to measure BMD of the spine and opposite hip in subjects with hip fracture.
Outcomes post hip fracture: Mortality and morbidity
Numerous studies have shown that actual bone size affects areal bone mass measurements, especially in different ethnic groups. Several techniques have been proposed to adjust bone mass measurements for volumetric differences in body size. The number of deaths in the year after fracture was recorded and the date and probable cause of death was documented.
The mortality rate was calculated as the number of deaths compared to survivors at one year, excluding subjects lost to follow-up.
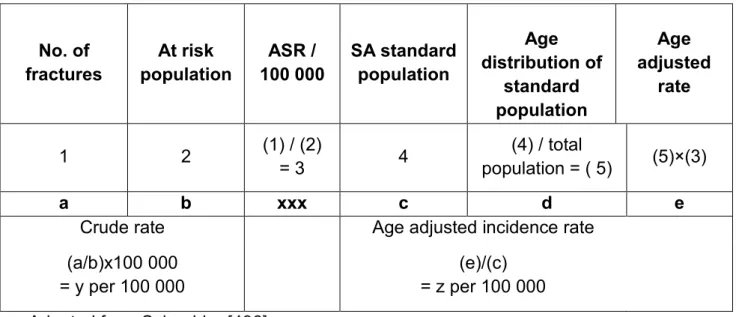
Incidence rate calculation
Due to small numbers, the ASR for the colored group and white men was not calculated [467]. Age-specific rates were calculated at 5-year intervals and the coefficient of increase or decrease calculated with increasing age by dividing the ASR of the older group by the ASR of the younger group. Statistics South Africa website: www.statssa.gov.za Statistics South Africa support: [email protected][467].
Calculation of health care costs associated with acute hip fracture
The acute costs of admission and treatment were calculated for 200 subjects enrolled in the prospective study. Using these data, the individual total costs incurred in the treatment of each patient were calculated. The other important area where uncertainty may have arisen was the estimate of hospital costs.
The study sample represents both males and females of different ethnic groups in the eThekwini area.
Data management
Data analysis
In cases where frequencies were small, the exact test was used to determine the p-value. In the case-control study, matched conditional logistic regression analysis was used to examine the relationship between hip fracture and control subjects and risk factors. Matched conditional logistic regression analysis was used to determine risk factors for osteoporosis and compare functional activities and hematological and biochemical results.
The financial burden of hip fracture was calculated using the bottom-up approach as detailed in Section 3.13.
Results
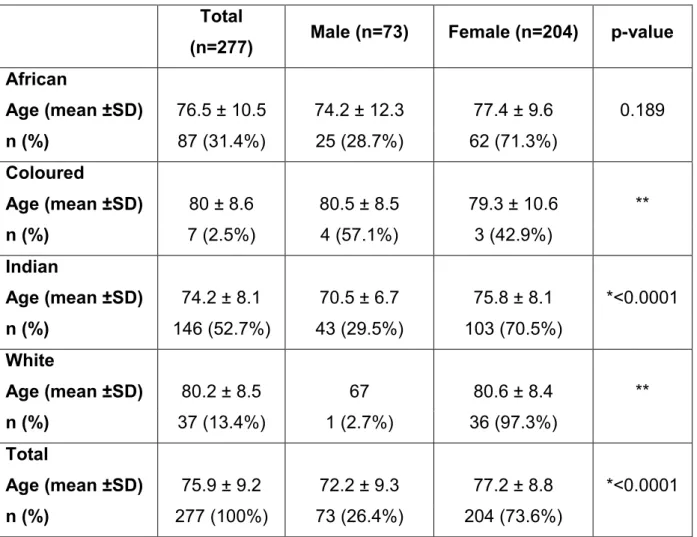
Demographic characteristics of 277 subjects with minimal trauma
There was no significant difference in height, but hip fracture subjects had a significantly lower weight compared to controls kg vs. Control subjects with osteoporosis were not enrolled in the study and a previous history of osteoporosis was obtained in 3.5% of hip fracture subjects. There was no difference in parity between the hip fracture and control groups of children vs.
There was no significant difference in the number of falls (single or multiple) in the previous year or last two years between hip fracture and control subjects.
Case control study; Assessment of risk factors for hip fractures
Outcomes post hip fracture
Health care costs associated with acute hip fracture management in the public
Summary of Results
Discussion
Introduction
Demographic profile
Incidence of osteoporotic hip fractures
Clinical risk factors for osteoporotic hip fractures
Bone mineral density
Morphometric vertebral fractures
Biochemical and haematological parameters
Hip fractures in men
Outcomes post fracture
Mortality
Morbidity
Summary and recommendations based on discussion
Conclusions
Introduction
Main Findings and Contributions to the Field
Study Limitation
Recommendations from the study