DETERMINANTS OF WOMEN’S FOOD SAFETY AND HYGIENE PRACTICE AT THEIR
HOUSEHOLDS
SHABRINA AFROZE
DEPARTMENT OF AGRICULTURAL EXTENSION AND INFORMATION SYSTEM SHER-E-BANGLA AGRICULTURAL UNIVERSITY
SHER-E-BANGLA NAGAR, DHAKA-1207 BANGLADESH
June, 2021
DETERMINANTS OF WOMEN’S FOOD SAFETY AND HYGIENE PRACTICE AT THEIR HOUSEHOLDS
BY
SHABRINA AFROZE Reg. No. 14-05988
A thesis
Submitted to the Faculty of Agriculture Sher-e-Bangla Agricultural University, Dhaka In partial fulfillment of the requirements for the degree of
MASTER OF SCIENCE (MS) IN
AGRICULTURAL EXTENSION AND INFORMATION SYSTEM SEMESTER: JANUARY- JUNE, 2021
APPROVED BY:
_____________________________
Md. Mahbubul Alam, PhD Supervisor
Professor
Dept. of Agricultural Extension and Information System
Sher-e-Bangla Agricultural University
_____________________________
Dr. Muhammad Humayun Kabir Co-Supervisor
Professor Dept. of Agricultural Extension and Information System Sher-e-Bangla Agricultural University
(Prof. Mohammad Zamshed Alam) Chairman
Examination Committee
Dept. of Agricultural Extension and Information System Sher-e-Bangla Agricultural University
Department of Agricultural Extension and Information System Sher-e-Bangla Agricultural University
Sher-e-Bangla Nagar, Dhaka-1207, Bangladesh
CERTIFICATE
This is to certify that the thesis entitled “DETERMINANTS OF WOMEN’S FOOD SAFETY AND HYGIENE PRACTICE AT THEIR HOUSEHOLDS” submitted to the department of Agricultural Extension and Information System, Faculty of Agriculture, Sher-e-Bangla Agricultural University, Sher-e-Bangla Nagar, Dhaka in partial fulfillment of the requirements for the degree of Master of Science (M.S.) in Agricultural Extension, embodies the result of a piece of bona-fide research work carried out by Shabrina Afroze, Registration No. 14-05988 under my supervision and guidance. No part of the thesis has been submitted for any other degree or diploma.
I further certify that any help or source of information, as has been availed of during the course of this investigation has been duly acknowledged by the Author.
Dated: June, 2021
Dhaka, Bangladesh (Prof. Md. Mahbubul Alam, PhD) Supervisor
Professor
Department of Agricultural Extension and Information System
Sher-e-Bangla Agricultural University
DEDICATED TO
MY BELOVED
PARENTS AND
ELDER SISTER
i
ACKNOWLEDGEMENT
At first the author expresses her gratefulness to the Almighty Allah who has helped her to pursue her higher education in agriculture and for giving the potency for successful completion of this research work.
With deepest emotion the author wishes to express her pious gratitude, indebtedness, felicitation, sincere appreciation to her research Supervisor Professor Md. Mahbubul Alam, PhD, Department of Agricultural Extension and Information System, Sher-e- Bangla Agricultural University, Dhaka, Bangladesh for his discursive guidance, intense supervision and continuous encouragement during the entire period of the research work.
The author also highly grateful and obliged to her research Co-Supervisor Professor Dr. Muhammad Humayun Kabir, Department of Agricultural Extension and Information System, Sher-e-Bangla Agricultural University, Dhaka, Bangladesh for his continuous encouragement, innovative suggestions, and affectionate inspiration throughout the study period.
The author expresses her sincere respect to Prof. Mohammad Zamshed Alam, Chairman, Department of Agricultural Extension and Information System, Sher-e- Bangla Agricultural University, Dhaka for providing valuable advice and sympathetic consideration regarding to the research.
The author is also grateful to all the teachers of Department of Agricultural Extension and Information System, Sher-e-Bangla Agricultural University, Dhaka, Bangladesh, for their continuous encouragement and innovative suggestions. The author is grateful to Md. Helal Uddin, Area Manager, BRAC (HNPP), Kushtia for his cooperation during the field work. Special thanks to the women, who were respondents of the study area and gave their valuable time for interview during data collection. To wrap thing up, the author might want to express her genuine gratefulness to her parents and elder sister and the greater part of her well-wishers.
The Author
ii CONTENTS
CHAPTER Title PAGE NO.
ACKNOWLEDGEMENT i
CONTENTS ii-iii
LIST OF TABLES iv
LIST OF FIGURES v
LIST OF APPENDICES v
ABBREVIATIONS vi
ABSTRACT vii
CHAPTER I INTRODUCTION 1-8
1.1 General Background of the Study 1-4
1.2 Statement of the Problem 4
1.3 Specific Objectives of the Study 4-5
1.4 Justification of the Study 5-6
1.5 Assumptions of the Study 6
1.6 Limitations of the Study 6
1.7 Definition of Terms 7-8
CHAPTER II REVIEW OF LITERATURE 9-18
2.1 Review of literature on food safety and hygiene 9-17
2.2 Conceptual framework of the study 18
CHAPTE III METHODOLOGY 19-30
3.1 Locale of the Study 19-21
3.2 Sampling Procedures and Sampling Size 22-23
3.3 Methods and Tools of Data Collection 23
3.3.1 Data Collection Method 23
3.3.2 Data Collection Tools 23-24
3.4 Measurement of Variables 24
3.4.1 Measurement of independent variables 24
3.4.1.1 Age 24
3.4.1.2 Education qualification 24
3.4.1.3 Family size 25
3.4.1.4 Annual family income 25
3.4.1.5 Mon Monthly hygiene purpose expenditure 25
3.4.1.6 Training on food safety and hygiene 25
3.4.1.7 Decision making ability 25-26
3.4.1.8 Media Contact 26
3.4.1.9 Organizational participation 26-27
3.4.1.10 Food safety and hygiene knowledge 27
3.4.1.11 Attitude towards food safety and hygiene 27
3.4.2 Measurement of Dependent Variable 28
3.5 3.5.1 3.5.2
Statement of Hypothesis Research Hypothesis Null Hypothesis
28 28-29
29
3.6 Data Processing and Analysis 29
3.6.1 Compilation of data 29
3.6.2 Categorization of data 29-30
3.7 Statistical Technique 30
iii
CHAPTER IV RESULTS AND DISCUSSION 31-44
4.1 Selected Characteristics of the Women 31
4.1.1 Age 32-33
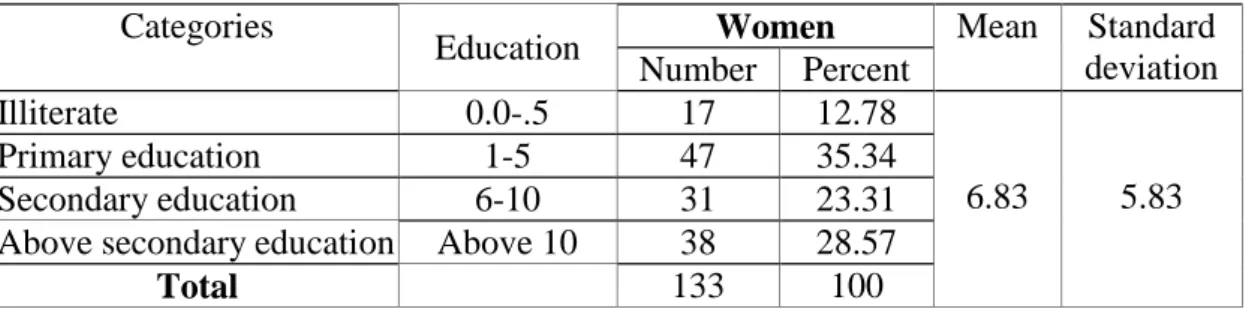
4.1.2 4.1.2 Education qualification 33
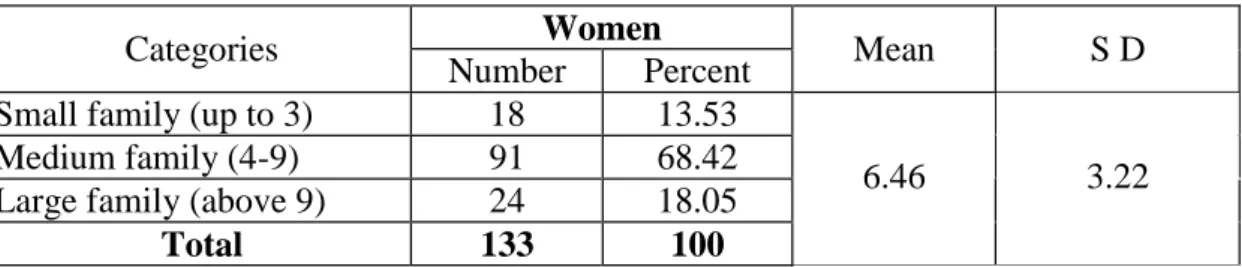
4.1.3 Family size 33-34
4.1.4 Annual family income 34
4.1.5 Monthly hygiene purpose expenditure 35
4.1.6 Training on food safety and hygiene 35-36
4.1.7 Decision making ability 36
4.1.8 Organizational participation 36-37
4.1.9 Media contact 37-38
4.1.10 Food safety and hygiene knowledge 38
4.1.11 Attitude towards food safety and hygiene 38-39
4.2 Food safety and hygiene practice 39
4.3 Contributing factors on women’s awareness on food safety and hygiene
40-41 4.3.1 Significant contribution of decision making ability to their
awareness on food safety and hygiene
41-42 4.3.2 Significant contribution of media contact to the women’s
awareness on food safety and hygiene
42-43 4.3.3 Significant contribution of food safety and hygiene
knowledge to their women’s awareness on food safety and hygiene
43
4.3.4 Significant contribution of attitude towards food safety and hygiene to their awareness on food safety and hygiene
44
CHAPTER V SUMMARY OF FINDINGS, CONCLUSIONS AND RECOMMENDATIONS
45-50
5.1 Summary of Findings 45
5.1.1 Selected characteristics of the women 45-46
5.1.2 Food safety and hygiene practice 46
5.1.3 Contributing factors on women’s awareness on food safety and hygiene
47
5.2 Conclusions 47-48
5.3 Recommendations 48
5.3.1 Recommendations for policy implications 48-49
5.3.2 Recommendations for further study 49-50
REFERENCES 51-61
APPENDICES 62-68
iv
LIST OF TABLES
Table Title Page No.
3.1 Sample distribution of women in selected unions of Kushtia sadar upazila
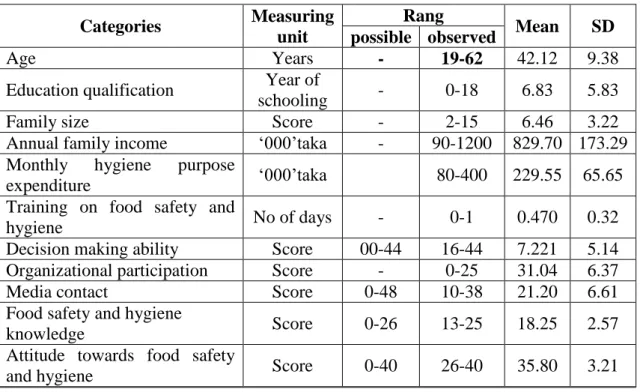
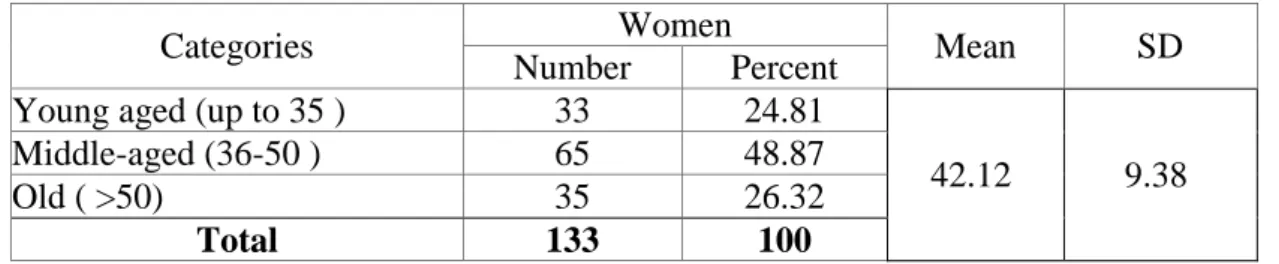
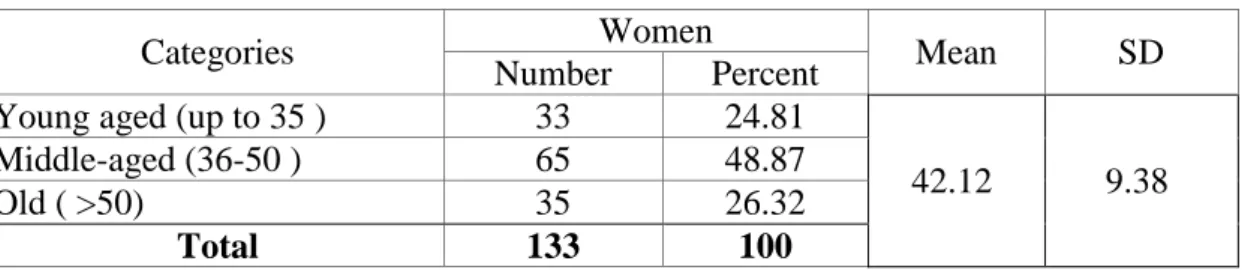
23 4.1 The salient features of the selected characteristics of the women 32 4.2 Distribution of the women according to their age 32 4.3 Classification of the women according to their education
qualification
33 4.4 Distribution of the women according to their family size 34 4.5 Classification of the respondents according to their income 34 4.6 Classification of the respondents according to their expenditure 35 4.7 Classification of the women according to their training on food
safety and hygiene
35 4.8 Distribution of the women according to their decision making
ability
36 4.9 Classification of the women according to their organizational
participation
37 4.10 Classification of women according to their media contact 37 4.11 Classification of women according to their knowledge 38 4.12 Classification of the respondents according to their attitude 39 4.13 Classification of the respondents according to their food safety
and hygiene practice
39 4.14 Multiple regression coefficients of contributing factors related to
the women’s awareness on food safety and hygiene
40
v
LIST OF FIGURES
Figure Title Page
No.
2.1 The Conceptual Framework of the Study 18
3.1 A map of Kushtia district showing Kushtia sadar upazila 20 3.2 A map of Kushtia sadar upazila showing the study area 21
LIST OF APPENDICES
SL. No. APPENDICES Page No.
Appendix -A English version of an interview schedule used for data collection
62-68
vi
ABBREVIATIONS
SPSS Statistical Package for Social Sciences
SAU Sher-e-Bangla Agricultural University
SAAO Sub Assistant Agriculture Officer
FAO Food and Agriculture Organization
et al. All Others
BBS Bangladesh Bureau of Statistics
β Multiple Regression
Ag. Ext. Ed. Agricultural Extension Education
Ag. Ext. and Info. Sys. Agricultural Extension and Information System
GDP Gross Domestic Product
DAE Department of Agricultural Extension
WHO World Health Organization
ICN International Conference on Nutrition
UNDPI Universal Declaration of Human Rights, United Nations Department of Public Information
CAREC Caribbean Epidemiology Centre
CDC Community Development Corporation
HFSQ HNPP
Home Food Safety Questionnaire
Health, Nutrition and Population Programme
PRECEDE Predisposing, Reinforcing, and Enabling
Constructs in Educational Diagnosis and Evaluation
BCBSNC Blue Cross and Blue Shield of North Carolina
NSNP National School Nutrition Program
CLI Crop Life International
GOs Government Organizations
NGOs Non- Government Organizations
FBDs Food Born Diseases
vii
DETERMINANTS OF WOMEN’S FOOD SAFETY AND HYGIENE PRACTICE AT THEIR HOUSEHOLDS
ABSTRACT
The major purpose of the study was to determine the extent of food safety and hygiene practices by women at their households. Attempts were also made to describe the selected characteristics of the women and to find out the contributing factors that affect women’s food safety and hygiene practices at their households. The study was undertaken purposively in Kushtia Sadar upazila under Kushtia district. Validated and well-structured interview schedule was used to collect data from 133 women during the period from 13 March to 14 April, 2021. Descriptive statistics, multiple regressions were used for analysis. The most 62.41 percent of the respondents had medium practice compared to 15.03 percent of the respondents had low practice and 22.56 percent of the respondents had high practice. Among 11 selected characteristics of the women’s four characteristics namely, decision making ability, media contact, food safety and hygiene knowledge and attitude towards food safety and hygiene of the respondents had significant positive contribution to their food safety and hygiene practices. The rest seven characteristics namely, age, education qualification , family members, annual family income, monthly hygiene purpose expenditure, training on food safety and hygiene and organizational participation had no significant contribution to their food safety and hygiene practices.
SHABRINA AFROZE
1 CHAPTER I INTRODUCTION
1.1 General Background of the Study
Food safety is a high profile issue facing consumers, agricultural marketers, farmers and governments. Health is strongly connected to the food. What one eats will actually affect one‘s health. Depending on that the food needs to follow the safety process from farm to fork. Food Safety (FS) is a wide term can cover many terms such as handling, storing as well as preparing foods to preventing or managing the infections related to the improper food safety and to provide a healthy diet that maintain the health of the community. While food hygiene indicates the contamination of food at any point of food safety line. In fact, the improper hygiene can lead to sever medical conditions that may result to death. The World Health Organization (WHO, 2015) estimates that 600 million food-borne diseases (FBDs) each year were related to poor food safety and hygiene practice with 420,000 deaths, the majority attributed to meat-related vulnerabilities (Brandwagt D. et al., 2018) and about, 76 million FBDs caused 325,000 hospitalizations in the USA which led to 5000 deaths (Navarro-Garcia, 2015).
In addition, during the year 2002, food quality and health-policy measures were established by the European Food Safety Authority (EFSA) in Parma, Italy. It has been widely demonstrated that the private home setting is considered the first place in which foodborne diseases develop due to poor personal and/ or environmental hygiene with an increased risk of infection (Istituto Superiore di Sanità, 2003;
Comodo et al., 2000; Fara and Proietti, 2000; Griffith et al. 1998; Istituto Superiore di Sanità 2006; Kagan et al., 2002; Redmond and Griffith, 2003 and Scott, 2001).
According to WHO, over 30–40% of foodborne disease cases occur in the home and in Italy, approximately 30,000 cases/year have been observed: 55– 75% due to outbreaks and 25–40% attributable to homemade preparation (Istituto Superiore di Sanità, 2006). Foodborne diseases are progressively increasing and the number of reported cases are underestimated due to the lack of outbreak reports in the home setting (Redmond and Griffith, 2003; Tauxe, 2002 and Istituto Superiore di Sanità, 2003).
2
The Centre for Disease Control diseases is rising in developing countries, as well as in the developed (Griffith et al., 1998). The transmission and Prevention (CDC) estimated that food-borne diseases caused approximately 76 million illnesses annually among the United States of America‘s 290 million residents, as well as 325,000 hospitalizations (Kennedy et al., 2005 and Mama and Alemu, 2016.). The incidence of food-borne diseases is rising in developing countries, as well as in the developed world (Griffith et al., 1998).
As a developing country, Bangladesh is also facing the issue of food safety and hygiene which is due to a cause of households‘ lack of awareness of food safety and hygiene management. Food safety is a growing concern for consumers and professionals in the food and food service sectors (Scheule and Sneed, 2001). It has been defined as the condition and measure that are necessary during production, processing, storage, distribution and preparation of food to ensure that it is safe sound wholesome, and fit for human consumption (WHO, 1984). Foodborne illness is of public health importance as both developed and developing countries are affected. For most instances, food preparation is done at the households place. Therefore, occurrence of foodborne diseases however more prevalent in developing countries due to poor awareness of women about food safety. This study draws upon data collection from a women‘s survey conducted in a selected area of Bangladesh with a view to determining to the extent food safety issues are important as far as individual women‘s awareness are concerned.
In the context of Bangladesh food safety is an important public health issue to prevent or control food-borne illnesses. The transmission of food-borne diseases is aggravated by unsafe food handling practices of food handlers. Approximately 10 to 20% of food-borne diseases outbreaks are because of contamination by food handlers. The role of food handlers in homes, usually mothers, in ensuring food safety at the household level is well accepted but an understanding of the status of their food handling knowledge and practices is needed. However, household food safety practice, particularly of mothers, is rarely studied, and the associated factors are poorly understood. It is high time to understand the interaction of the prevailing food safety, knowledge, and practices of food handlers in reducing foodborne outbreaks.
3
Food safety is a global public health threat with frequent incidence of foodborne diseases. Additionally, the COVID-19 outbreak has put more pressure on global public health; everyone related to food supply chain are facing an ongoing challenge to improve and to extreme food safety and hygiene due to the pandemic. In this context, foodborne diseases are responsible for major economic costs for a country. In this regard, the application of the Hazard Analysis and Critical Control Point (HACCP) system can improve food safety; however its strength and success in preventing foodborne illnesses depend on it being applied correctly along with the provision of a sanitary infrastructure and the application of principles of good hygiene practices. Current evidence suggests that a substantial number of foodborne illnesses occur through poor food handling practices. Pathogens may appear in food, for instance, through food purchases from unsafe sources, inadequate cooking or reheating, holding food at room temperature, cross-contamination, poor personal hygiene, or improper food handling practices frequently contribute to food borne illnesses.
Food borne illnesses were estimated to be the cause of 76 million illnesses, 325,000 hospitalizations, and 5000 deaths in the United States each year (De Waal, 2003;
Mead et al., 1999). The Caribbean Epidemiology Centre (CAREC, 2002) reported that there were 2597 reported cases of food-borne illness in 2000 and 1905 cases in 2001 (as up to 8th February, 2002) for CAREC member countries.
The wide attention given to food safety is also due to the upward trend of foodborne illness incidence rates over the past 20 years both locally (Abdul- Mutalib, Syafinaz, Meftahuddin, 2002; MoH, 2012; Sharifa Ezat, Netty, & Sangaran, 2013; Soon et al., 2011) and internationally (CDC, 2014). In the United States, it was estimated that 9.4 million episodes of foodborne illness were caused by 31 major pathogens, which led to 55961 hospitalizations and 1351 deaths (Scallan et al., 2011).
Food safety knowledge, attitude, and practice are playing a fundamental role in food poisoning outbreaks prevention and control. Women plays an important role in food related sectors at home in Bangladesh. It needs to take an attempt to increase both knowledge and awareness of women towards food safety and hygiene so their practice
4
level in the household should be improved and they play an important role to fight against diseases.
1.2 Statement of the Problem
Food safety has received much emphasis by agencies worldwide due to the threat of contracting foodborne illnesses. Foodborne illnesses cover a wide range of diseases and are a growing public health concern, which has caused morbidity and mortality worldwide. Food borne illness occurs as a result of consuming food contaminated with microorganisms or their toxins, cross-contamination from enter toxigenic staphylococci through unhygienic handling practices and, or Hepatitis A infected food handlers (Baş, Ersun, & Kivanç, 2006; WHO, 2007). Contamination of food may occur at any point along the food production chain before it reaches the end consumer. Food safety, according to Scallan et al. (2011) is defined as the conditions and measures that are necessary along the food production chain to ensure that it is safe, sound and fit for human consumption. Food is considered safe when it is free from chemical, biological or physical hazards that may result in illnesses or even death to the consumers. Food safety is a concern as it poses risks to the population, especially to vulnerable groups such as infants and young children, elderly individuals and those with immunodeficiency disorder (Soon, Singh & Baines, 2011). This study attempted of find out the answers of the following research questions:
• What were the personal characteristics of the women, who were involved as respondent?
• To what extent of the food safety and hygiene practices by women?
• What are the factors that significantly influence women‘s food safety and hygiene practices?
1.3 Specific Objectives of the Study
In view of the problems stated above the following specific objectives are framed out in order to give proper direction to the research work:
(i) To describe the following selected characteristics of the women. The characteristics were:
a. Age,
b. Education qualification,
5 c. Family members,
d. Annual family income,
e. Monthly hygiene purpose expenditure, f. Training on food safety and hygiene, g. Decision making ability,
h. Organizational participation, i. Media contact,
j. Food safety and hygiene knowledge,
k. Attitude towards food safety and hygiene issues,
(ii) To determine the extent of food safety and hygiene practice by the women at their households,
(iii) To explore the contributing factors that affect food safety and hygiene practice by women at their households.
1.4 Justification of the Study
Food safety issues related to foodborne diseases are important because of the direct health and economic burdens imposed, and the indirect impact on the development and productivity of people. Foodborne illnesses tend to create extensive cost to the food industry and the economy at large; hence, food safety and hygiene practices continue to be a matter that requires attention (Egan, Raats, Grubb, Eves, Lumbers, Dean & Adams, 2007). Providing effective training could assist with increased awareness of food safety and hygiene practices particularly in the areas of cross- contamination, temperature control, storage, and personal hygiene that will guarantee food safety and quality. Equipping food handlers with training on food safety and hygiene practices is crucial as this knowledge has a significant role in decreasing and hopefully avoiding food poisoning through production and distribution of safe food (Lazarevic, Stojanovic, Bogdanovic & Dolicanin, 2013). These outbreaks raise several concerns, one of which relates to the level of awareness and knowledge of food handlers on good hygiene practices and the importance of food safety. A study conducted in Accra, Ghana, revealed that food handlers can undergo training and found may have acceptable knowledge on hygiene and food practices, but the knowledge gained is not always practiced (Annor & Baiden, 2011). The findings of this research will be acceptable in the selected area. Thus, the findings of the study
6
will have great importance to the women of Bangladesh.
1.5 Assumptions of the Study
An assumption is the supposition that an apparent fact or principle is true in the light of the available evidence (Goode and Hatt, 1952). The researcher had taken the following assumptions into consideration during carrying out the study:
1. The respondents had enough capability to provide proper response of the question furnished in the interview schedule.
2. The respondents were provided views and opinions included in the sample representative of the whole population of the study area.
3. The items, questions and scale of measurement of the variables were reasonably authentic to present the actual condition of the respondents.
4. The findings of the study would give clear concept of the household food safety and hygiene practice.
5. The data furnished by the respondents were free from bias.
6. The researcher was capable to adjust with the social and cultural environment of the study area. So, the respondents could provide their information correctly.
1.6 Limitations of the Study
It is necessary to impose certain limitations to make the research manageable and meaningful. Thus, during the entire research the most challenging limitations were:
1. The research was confined to the two villages of Kushtia Sadar upazila under Kushtia district.
2. Data were collected from a small group of respondents taken as the sample of the study because of time and resource constrains.
3. The researcher had to face many difficulties during data collection. All the data were recall data. So, the researcher had to depend on the data as given by the respondents.
4. Only 11 characteristics of the women were selected as independent variables.
5. For information about the study, the researcher has to depend on the data furnished by the selected respondent‘s instant memory during the interview time.
6. Time allocation and budget was also limitation in the study.
7 1.7 Definition of Terms
Determinants: An element that identifies or determines the nature of something or that fixes or conditions an outcome or a determinant can be defined as a factor, indicator or cause that makes something happen or leads directly to a decision.
Respondent: Randomly selected people considered to be presentable of the population are known as respondents. They are the people from whom a social research worker usually gets most data required for her research. In this study the respondents were the village level women.
Age: Age of a respondent defined as the span of her life and is operationally measured by the number of years from her birth to the time of interview.
Education qualification: Academic qualification referred to the development of desirable change in knowledge, skills and attitude in an individual through reading, writing and other related activities. It was measured in terms of years of schooling completed by and individual at the time of interview.
Family size: Family size referred to the number including the respondent himself, his wife, children and other permanent dependents, which lived and lived together in a family unit.
Media contact: These terms referred to an individual‘s access to or contact to the communication media and sources being used for dispersion of new technologies among farmers.
Family annual income: Family annual income was defined as the total earning of a respondent and members of his/ her family both from agricultural and other sources (business, service etc.) during a year. It was expressed in taka.
8
Monthly hygiene purpose expenditure: It referred as the total spent of an individual to hygiene purpose in each month. It has been expressed as taka per month.
Training received on Food Safety and Hygiene: Training experience of a women was defined as the number of days she had so far received training. It was used to refer to the completion of an activity by the women which was offered by the government, semi- govt. or non- government organizations to improve their knowledge and changing attitude of a women for proper food safety and hygiene practice in their household activities.
Decision making ability: Decision making ability of a respondent referred to the extent of ability to make decision with 5 different aspects, viz., decision is taken solely by me, decision is taken jointly with husband, decision is taken jointly with another member of the household, decision is taken by husband, decision is taken by another member of the household. In the present study 11 selected items of decisions were considered for decision making.
Organizational participation: Organizational participation referred to the degree to which an individual was involved with selected organizations as different types of membership like ordinary member, executive member and executive officer for a specific period of time.
Food safety and hygiene knowledge: Knowledge is operationally defined for the purpose of this investigation as those behaviors or test situations, which emphasized the remembering either by recognition or recall of ideas. It refers to the amount of understood information possessed by the women‘s on various household practices aspects of food safety and hygiene.
Attitude towards food safety and hygiene issues: Thurstone (1946) defined attitude as ‗the degree of positive and negative effect associated with psychological object like symbol, phrase, slogan, person, institution, or ideas towards which people can differ in varying degrees‘. In the present study, attitude towards food safety and hygiene referred to the knowledge and practice tendency towards household activities.
9
Food safety and hygiene practices: Food safety and hygiene practices are referred to as the extent of use of various activities related to food safety and hygiene by women at their household. Such as- washing hand with soap before eating and preparing food and after toilet, boil milk before use, etc.
10 CHAPTER II LITERATURE REVIEW
A literature review is a survey of scholarly sources on a specific topic. This chapter deals with a brief review of previous research studies relating to the food safety and hygiene. Conducting a literature review involves collecting, evaluating and analyzing publications (such as books and journal articles) that relate to research questions. The researcher made an elaborated search of available literature for this research. The relevant information regarding this food safety and hygiene is limited in number.
However, the researcher has tried her best to collect needful information through searching relevant studies. Unfortunately, few research works were found directly related to the food safety and hygiene. From the literature review, the conceptual background for determinants of food safety may be built. A number of studies have analyzed the food safety at national level in Bangladesh. This present chapter has portrayed some reviews of interlinked knowledge on this aspect that is endeavored.
The interlinked reviews easily portrayed basic objectives of the study as far as possible. All the reviews in this chapter are from secondary sources and no new or original experimental work is reported there. However, research works related to food safety and hygiene practice in different aspects of some important food safety and hygiene are presented below.
2.1 Review of Literature on Food Safety and Hygiene
Review of literature provides the clear and concise direction of the researcher for conducting the experiment. With aim to get clear and concise direction this Chapter deals with the review of past research works that relates to this investigation directly or indirectly. The reviews are conveniently presented based on the major objectives of the study. This study was mainly concerned with women‘s food safety and hygiene practice towards the contribution of the selected characteristics of the women‘s.
Despite frantic search, the researcher found only a few literatures related to this study.
The researcher came across with some subject matter specialist opinions and has tried his best to collect necessary information through searching relevant studies, thesis, journal, articles, periodicals, bulletins, leaflets, websites etc. However, a brief review
11
of the available literature has been incorporated in the light of the objectives of this study are present below:
A survey which was conducted to measure consumers knowledge, risk perception and practices of food safety in the Caribbean, revealed that although consumers were aware of correct safety practices, many still did not attribute certain illnesses to being foodborne and thought it was possibly due to their own actions (Jackson et al., 2003).
This was coupled with significantly higher proportion of consumers as compared to non-consumers, who were aware that the product could cause food-poisoning and definitely posed a health risk to those who ate doubles. Changes in food consumption patterns have led to increased consumption of foods outside the home (Riethmuller &
Morrison, 1995). Certain processes or handling practices by consumers in the home have been identified as being essential or critical in preventing food-borne illness (Altekruse, et al., 1995). Bryan (1988) identified the most common food handling mistakes: serving contaminated raw food; cooking, heating, or re-heating foods inadequately; obtaining food from unsafe sources; cooling food inappropriately;
allowing too much of a time lapse. Research on adult food safety education, food preparation practices and perceived risk of foodborne illness has guided educational programs and material development (Ellis, Sebranek, & Sneed, 2003).
Earlier studies Rahmanet al. (2016) have showed that knowledge of food safety is associated with food safety practice. Attitude plays a significant role in food safety practice (Chekol, 2019; Rahman et al., 2016; Ismail et al., 2016; Lee et al, 2017; Lim et al., 2016)
Food safety knowledge, attitude, and practice are factors playing a fundamental role in food poisoning outbreaks prevention and control (Sharif and Al- Malki, 2010.)
Food safety knowledge is largely obtained through training in food safety. This includes attending certified training course where participants were exposed on the importance of time temperature control, personal hygiene, safe food handling and causes of foodborne illnesses. Other sources of food safety knowledge are from printed education materials and the use of new media where information on food safety can be found at the tip of the finger. In order to have good food handling
12
practices, the food handlers must be trained and have knowledge in food safety. Some studies have shown that increased knowledge on food safety will result in positive food handling practices (Abdul- Mutalib et al., 2012; Toh & Birchenough, 2000).
However, there are also studies that show that having good level of knowledge did not always result in positive behavior towards hygienic practices (Akabanda et al., 2017;
Clayton, et al., 2002). This suggests that transfer of knowledge to practices is not predictable.
The term attitude used by Abate (1999) means ―a settled opinion‖ and ―behavior reflecting this‖. Venes (2001) defined attitude as behavior based on conscious or unconscious mental views developed through cumulative experience.
Practice may be defined as the activities of an individual that he/she performed followed by some instructions in order to fulfill some wants that he/she needed‖
(Alam, 2003). Karl Sweiby (2003) noted Practice as a method, procedure, process, or rule used in a particular field or profession; a set of these regarded as standard.
According to Oxford dictionary ―Practice is the actual application or use of an idea, belief, or method as opposed to theories relating to it.‖ From oxford dictionary it is also found that ―practice is the facts, information, and skills acquired through experience or education; the theoretical or practical understanding of a subject‖. There is a proverb that ―practice makes a man perfect‖ in the same way more practice increase knowledge and attitude (positive or negative) to a specific subjects.
Significant associations observed between literacy level/standard of living of the respondents and certain food safety practices are in conjunction with similar studies (Unusan, 2007). This may be due to the fact that there are other factors such as sanitation, availability of protected water supply and environmental conditions (UNICEF, 2004) which are essentially beyond the control of the respondents.
However, a review of improved water supplies and sanitation facilities in control of diarrhoeal diseases among young children has shown that even under the most favorable circumstances the rate of morbidity is reduced only by 27% (Esrey, 1985).
In this scenario it should be realized that food safety education is a powerful and practical means improving public health and enables people to make informed choices (Motarjemi & Moaref, 2000). The present study highlights the need for educating the
13
mothers on usage of soap for washing hands, the need for proper storage and re- heating of cooked foods. The findings of the study also highlight the need to spread awareness about checking quality symbols and information on food labels. At the same time, reporting to the health authorities in case of food poisoning or adulteration needs to be inculcated among the people. Television appears to be the preferred source for food safety education. (UNICEF, 2004)
Our finding asserts with previous studies done in Ethiopia, Malaysia, and Ghana (Rahman et al., 2012; Azanaw et al., 2019; Amegah et al., 2020). The probable justification is that SCFHs who have completed food safety training courses had gained the talents and awareness necessary to handle food safely and sustain great ethics of self-cleanness and hygiene practices. Our finding affirms the assertion that training upsurges understanding of food safety which might reflect into hygiene practices (Akabanda et al., 2017). Hence, a lack of or in adequate training of SCFHs on food safety may inadvertently result in poor hygiene practices, thereby encouraging food contamination (Tabit and Teffo, 2020; Amegah et al., 2020). This implies providing food safety training to food handles is important to keep consumers from food poisoning and other well being dangers that could arise from eating unsafe food.
Youn and Sneed (2003) and Ansari-Lari, Soodbakhsh and Lakzadeh (2010) pointed out that high proportion of reported foodborne disease outbreaks were caused by mishandling in foodservice establishments, food processing operations and homes.
Proper cooking and processing can reduce the risk of foodborne illness. It has also been found that almost 70% of food poisoning outbreaks were caused by time and temperature abuse and cross-contamination (Baş, Ersun & Kivanç, 2006). This includes preparing food way in advance, incorrect thawing method, improper food holding temperature and malfunction cooling equipment (Bou-Mitri, et al., 2018; Liz Martins & Rocha, 2014; Osaili et al., 2013). Many basic food handling practices were also found to be missing in the routines of food handlers in schools. In Clayton and Griffith (2004), observations on food handling represents the most accurate and reliable method to assess food handlers‘ practices on food safety.
14
A survey in West Indies, wherein 69% of respondents did not notify any Public Health Department of a suspected or contaminated or tampered product and only 8%
reported on the default food product ‗sometimes‘. In yet another study in Jamaica, the majority of urban householders had never contacted their local Health Department or Ministry of Health (Knight et al., 2003).
Research by Abdul- Mutalib et al. (2012) showed that food handlers often had poor personal hygiene practices such as improper hand washing technique. This is seconded by other studies that have shown the same results (Baş, Ersun, & Kivanç, 2006; Tan et al., 2013). Rebouças et al. (2016) have observed improper practices such as handling and distributing foods without using gloves and talking while handling food. Hands plays an important role in transporting pathogenic microorganisms, therefore effective hand washing will prevent such things to happen.
Esfarjani et al. (2016) conducted a study on development of a home food safety questionnaire based on the precede model: targeting Iranian women and found that this study was the first attempt to design and develop a home food safety questionnaire (HFSQ), in the conceptual framework of the PRECEDE (predisposing, reinforcing, and enabling constructs in educational diagnosis and evaluation) model, and to assess its validity and reliability. The HFSQ was developed by reviewing electronic databases and 12 focus group discussions with 96 women volunteers. Ten panel members reviewed the questionnaire, and the content validity ratio and content validity index were computed. Twenty women completed the HFSQ, and face validity was assessed. Women who were responsible for food handling in their households were selected randomly from 10 health centers and completed the HFSQ based on the PRECEDE model.
A study carried out in West Indies, it was reported that 88.1% of consumers washed their hands thoroughly with soap before and after preparing meals while only 10.7%
did so ‗sometimes‘ (Surujlal & Badrie, 2004). In the National Australian food safety telephone survey, most people (82.3%) reported that they washed their hands with soap or detergents and almost the same proportion felt it was very important to wash hands before and after preparing meals (Jay, Comar, & Govenlock, 1999). It is known that poor hand washing practices inevitably lead to retention on the hands of bacterial
15
and viral pathogens, which are obtained from handling raw produce (Snelling, Kerr,
& Heritage, 1991) or from toilet activities or changing infants‘ nappies (Moterjemi, Kaferstein, Moy, & Quevedo, 1993). In the present study, though over 90% of the respondents reported of washing hands after using the toilet and cleaning child‘s stools, but usage of soap for washing hands was reported by less than a third of them.
It is known that home food safety is controlled through the education of the consumer (Unusan, 2007), hence associations were made between literacy level of the respondents and usage of soap for washing hands. The association was found to be highly significant (p < 0.01). Similarly, chi-square test showed that the standard of living also had a significant (p < 0.01) association with usage of soap, i.e., the better the standard of living index, more was the usage of soap.)
Meador et al. (2006) conducted a study and found that focuses on the planning efforts by Blue Cross and Blue Shield of North Carolina (BCBSNC) to address the problem of underutilization of preventive health care services among adult male members— an issue that has received comparatively little attention in the health behavior arena.
BCBSNC planners used the PRECEDE planning process to define issues relevant to the target population and determine appropriate intervention strategies. Increasing perceived susceptibility and severity to disease, perceived benefits of screening, physician recommendation for screening, and health knowledge/awareness emerged as intervention priorities. The PRECEDE planning process yielded important evidence- based information and strategies to address men‘s underuse of preventive services and led BCBSNC to adopt new systems for planning interventions to promote the health of its members.
Research evidence suggests that inappropriate hygiene practices result from lack of knowledge, ignorance as well as negligence of food handlers at schools; and this has led to an increased outbreak of foodborne illnesses (Afolaranmi et al., 2015; Da Cunha, Stedefeldt & De Rosso, 2012). However, many countries in Africa have been undergoing modernization of their food safety systems in the last decades. This has often included developing coordination mechanisms across Ministries and Departments with mandates for food safety, establishing standard bureaus, upgrading laboratory facilities, updating and harmonizing standards and strengthening export capacity. Although many African countries subscribe to Codex Alimentarius
16
standards, resource challenges have limited their enforcement. Furthermore, food safety is not prioritized in developing countries; consequently, millions of people get sick, and hundreds of thousands die from consuming food that is unsafe (Fung, Wang
& Menon, 2018).
However, reports show that consumers are unaware of their domestic contribution to risks of food contamination (Losasso, et al., 2012) since they are more concerned about hygiene standards outside the home setting (Eves; et al., 2010; Miles et al., 2004).
The microorganisms normally present on the surface of raw fruits and vegetables may consist of chance contaminants from the soil or dust, or bacteria or fungi (Beuchat, 1998). Contaminated or uncooked raw foods can cause harmful microorganisms to be passed to safe foods and can cause a foodborne illness (National Assessment Institute, 1998). Added to these, pesticides used during cultivation can remain as residues in vegetables and fruits, the effect of which can be minimized by washing them thoroughly in running water (NIN, 1998). In the present study, significant association (p < 0.05) was found between the SLI of the respondents and the habit of washing vegetables before cutting or peeling, but such association was not significant in case of washing of fruit.
Proper education and training on the basic principles of food safety are emphasized in prior literature since they could contribute to reducing the incidence of foodborne illnesses if the messages are specifically targeted at consumers‘ needs and habits (Altekruse, Yang, Timbo & Angulo, 1999). Previous studies have focused on effective strategies for improving consumer behavior in the food hygiene context (Miles et al., 2004; Redmond & Griffith, 2003) but inadequate research has been conducted on school-based food safety education. Food safety education of school children is thought to be essential but adequate training in food hygiene practices of food handlers is also very important as children seldom prepare their meals on their own. Therefore, food safety and hygiene are vital for the prevention of food contamination which results in food poisoning. Good hygiene practices are known as the prerequisite methods and procedures whereupon the safety of food and the
17
management quality systems are formed. These practices are essential for personnel handling food as they need to ensure that food is safe for ingestion. This requires that everyday food handlers must guarantee that the food is hygienic and safe throughout the preparation stages.
Ramful (2017) alleged that good hygiene practices ensure that food handlers keep the highest level of personal hygiene, and wear appropriate protective clothing. These include head covering, appropriate footwear, regular hand washing, frequent glove changes, no jewellery, watches, or any other items in the food handling areas.
Thigeel (2010) asserted that knowledge of preparation and good hygiene practices of individuals that directly handle food (both preparation and serving), plays a vital role in avoiding most foodborne diseases.
At the household level, Shaikh (2007) probed the household food safety in rural households of Sindh. The study concluded that household income, food prices and women specific variables such as age and time allocation influence household food safety.
Badrie et al. (2006) conducted a survey on 121 consumers who handled meat on food safety knowledge and handling practices at homes. Most (P < 0.01; 83.2%) categorized food safety as very important. Consumers differed (P < 0.05) in their perception as to the most feared food hazard. Escherichia coli (89.7%) and Salmonella (85.7%) were most known (P < 0.01) of microbial types. Restaurant (55.0%) was regarded to be the most likely place where food poisoning could occur. There was no distinct (P > 0.05) trust in food safety authorities. The study highlighted gaps in food safety knowledge and critical violations in food handling.
The national hygiene survey 2014 of Bangladesh found that less than half of household latrines had soap and water available for hand washing (ICDDR, B, 2014), It was also found that more than half of the women do not wash their hand before feeding their child (Hossain et al., 2019. However, it is difficult to generalize that men maintain better hygiene than women. A contrast result published in Lancet reports that overall, 54% of world‘s population maintains good personal hygiene, which is
18
higher among women (59.5%) than men (44.5%) (Lubys, et al, 2005). Evidence showed that hand washing can reduce the occurrence of diarrheal diseases by 14- 40%
(Hoque, 2003).
2.2 Conceptual Framework of the Study
In scientific research, conceptual framework is selection and measurement of variables. The conceptual framework of Rosenberg and Hovland (1960) was done by framing the structural arrangement for the dependent and independent variables. This study is concerned with the determinants of women‘s food safety and hygiene practice at their households. After consulting with the relevant experts and reviewing of past related literatures, 11 (eleven) selected characteristics of the women were considered as the independent variables, which might have contribution on women‘s food safety and hygiene practices. Based on this discussion the conceptual framework of this study has been formulated as shown in figure 2.1.
Figure 2.1 The conceptual framework of the study INDEPENDENT VARIABLES
DEPENDENT VARIABLE
Age
Education qualification
Family member
Annual family income
Monthly hygiene purpose expenditure
Training on food safety and hygiene
Decision making ability
Organizational participation
Media contact
Food safety and hygiene knowledge
Attitude towards food safety and hygiene
Women‘s food safety and
hygiene practice
19
CHAPTER III METHODOLOGY
In conducting a research study, methodological issue is one of the prime considerations for yielding of valid and reliable findings. Appropriate methodology enables the researcher to collect valid and reliable information and to analyze the information properly in order to arrive at correct conclusions. However, the methods and operational procedures followed in conducting this study has been described in the subsequent sections of this Chapter.
3.1 Locale of the Study
The study was conducted at Kushtia sadar upazila under Kushtia district. Kushtia district is a district in the Khulna administrative division of western Bangladesh.
Kushtia District has an area of 1608.80 square kilometres and is bounded by Rajshahi, Natore, Pabna districts to the North, by Chuadanga, Jhenaidah districts to the South, by Rajbari District to the East, and by West Bengal and Meherpur District to the West. The average high temperature is 37.8 °C and the average low is 9.2 °C. Annual rainfall averages 1,467 millimetres. Kushtia sadar upazila of Kushtia district, having an area of 318 square kilometers and consists of 15 unions. The unions are: Hatashharipur, Barkhada, Mazampur, Bottail, Alampur, Ziaraakhi, Ailchara, Patikabari, Jhaudia, Ujangram, Abdulpur, Harinarayanpur, Monohardia, Goswamidurgapur.
20
Figure 3.1 A map of Kushtia district showing Kushtia sadar upazila
21
Figure 3.2 A map of Kushtia sadar upazila showing the study area
22 3.2 Sampling Procedures and Sample Size
The sample for this study was drawn from all the women involved in food safety and hygiene practices. Multi-stages random sampling procedure was used for the selection of sample household heads. In the first stage, Kushtia district was selected purposely.
In the second stage, Kushtia sadar upazila and two potential unions belong to this upazila randomly selected.
People who permanently reside in the selected union constituted the active population of the locality. An update list of all women from selected villages was prepared with the help of respective local village leaders. The list comprised a total of 133 rural women. These women constituted the population of this study. There were 523 women in Kathulia and 602 in Bottoil. Eleven (11) percent of the population from each selected village was randomly selected as representative sample by using random number table. 3.1. Thus, the sample size consists of Kathulia 62 and Bottoil 71, making the total sample size of 133 women‘s. A reserve list of 13 rural women at the rate of 10 percent of the population was prepared by the same method to use in case of the individual included in the original samples were not available or not found at the time of data collection. The distribution of the women‘s included in the population, sample and those in the reserve list appears in Table 3.1.The total number of food safety and hygiene practices in these unions was 1125; whereas 523 and 602 family heads were listed from Alampur and Bottoil unions of Kushtia sadar upazila respectively. Thus, 1125 number of food safety and hygiene practices women constituted the population size of the study which is shown in the following Table 3.1.
According to the modified formula of Yamane (1967), the sample size was 133.
Accordingly, the required sample size at 95% confidence level with degree of variability of 5% and level of precision equal to 8% are used to obtain a sample size required which represents a true population (Table 3.1).
……… (1)
Where, n = sample size, N= population size (sampling frame) and e = level of precision considered 8%.
23
Table 3.1: Sample distribution of women in selected unions of Kushtia sadar upazila
Union Villages Population Sample Reserve list
Alampur Kathulia 523 62 6
Bottoil Bottoil 602 71 7
Total 1125 133 13
* n was calculated from the total number of ‗N‘, not from the ‗N‘ separately for each union.
** The distribution of samples to each union was done randomly.
A reserve list of 13 women (10% of the sample size) were also prepared so that this list could be used during the interview in case of any mislead, misconduct, mismatch or unavailability of the respondents counted on the original list.
3.3 Methods and Tools of Data Collection 3.3.1 Data Collection Method
Data were collected personally by the researcher herself through face to face interview with the randomly selected women‘s with the help of an interview schedule.
The researcher made all possible efforts to collect pertinent and authentic information.
The survey was used to collect quantitative data that allow to answer the framed research questions and to gain an understanding of the determinants of food safety and hygiene practice.
3.3.2 Data Collection Tools
A structured interview schedule was prepared to reach the objectives of the study containing mostly closed questions. The questions in this schedule were formulated in a simple and unambiguous way and arranged in a logical order to make it more attractive and comprehensive. The instrument was first developed in English and then translated into Bengali. The survey tool was initially constructed based on extensive literature reviews and pre-tested. The schedule was pretested with 15 randomly selected women‘s in the study area in identifying faulty questions and statements.
Thus, necessary additions, deletions, modifications and adjustments were made
24
accordingly in the schedule. The questionnaires were also checked for validity by supervisors and other experts at Sher-e-Bangla Agricultural University (SAU).
Finally, based on background information, the interview schedule was finalized. Data was gathered by the researcher personally. During data collection, necessary cooperation was obtained from field staff of different GOs, NGOs and local leaders.
The field data collection was started from 15 March and completed on 14 April, 2021.
3.4 Measurement of Variables
A variable is any characteristic, which can assume varying, or different values in successive individual cases (Ezekiel and Fox, 1959). An organized research usually contains at least two important variables, viz. an independent and a dependent variable. An independent variable is that factor which is maintained by the researcher in his attempt to ascertain its relationship to an observed phenomenon. A dependent variable is that factor which appears, disappears or varies as the researcher introduces, removes or varies the independent variable (Townsend, 1953). According to the relevant research area, the researcher selected 11 characteristics of the women‘s as the independent variable and food safety and hygiene practice as the dependent variable.
It was pertinent to follow a methodological procedure for measuring the variables in order to conduct the study in accordance with the objectives already formulated. The procedures for measuring the variables are described below:
3.4.1 Measurement of independent variables 3.4.1.1 Age
The age of the respondents was measured in terms of years, on the basis of the responses of the respondents. Age was measured by the period of time from the birth of a respondent to the day of interviewing.
3.4.1.2 Education qualification
Education qualification of a respondent is measured in term of grades (classes) passed by are respondent. One score was assigned for one year of successful schooling. For example, if a respondent passed the final examination of class six, his education score was taken as ‗6‘; if a respondent had education outside the school and if the level of education was through equivalent to that of class four of the school, then her
25
education score was taken as ‗4‘ as the same way illiterate person was given a score zero. A score of 0.5 was assigned for those who don‘t read and write but can sign her name only.
3.4.1.3 Family size
Family members were operationally measured by assigning a score of one for each member of the family who jointly lived and ate together. The members included the respondent herself, her husband, children and other dependent members.
3.4.1.4 Annual family income
Annual family income indicates total earning of a women and the members of his/ her family both from agriculture and other socially acceptable regular means such as business, service etc. during last year. The value of all the agricultural products encompassing crops, livestock, vegetables etc. were taken into consideration. For calculation, a score of one (1) was assigned for each one thousand (1000) taka of the annual income of a family.
3.4.1.5 Monthly hygiene purpose expenditure
Monthly hygiene purpose expenditure of a respondent was measured in thousands taka on the basis of total monthly hygiene purpose expenditure of the respondents for her family member.
3.4.1.6 Training on food safety and hygiene
Training on food safety and hygiene was determined by the total number of days a respondent received training in her entire life on food safety and hygiene from different organizations. In a measuring score of 1 was assigned for each days of training. This variable appears in item number 6 in the interview schedule as presented in Appendix-A.
3.4.1.7 Decision making ability
Decision making ability was measured as one‘s extent of taking different decisions.
Each respondent was asked to indicate her nature of decision making ability for 11 selected decision making items with five alternative responses. Following scores were assigned for each of 11 decision making items with five alternative responses:
26
Nature of decision making ability Scores assigned
Decision is taken solely by me 4
Decision is taken jointly with husband 3
Decision is taken jointly with another member of the household
2
Decision is taken by husband 1
Decision is taken by another member of the household 0
Finally, decision making ability score of respondent was computed by adding all the scores obtained by her against all the 11 selected decision making items. Thus, the decision making ability scores of the respondent farmers could range from 0 to 44 where ―0‖ indicated no decision making ability and ―44‖ indicated highest decision making ability.
3.4.1.8 Media contact
The media contact of a respondent was measured by computing an extension contact score on the basis of her extent of contact with 12 selected media. The respondents were asked to mention her response to five alternative nature of contact for each media. The score for each respondent was determined by adding her responses to all the items on the basis of her frequency of contact as not at all, rarely, occasionally, frequently and regularly with a score of 0, 1, 2, 3 and 4 respectively. Media contact score of the respondents could range from 0 to 48, where 0 indicating no contact and 48 indicating high media contact.
3.4.1.9 Organizational participation
Organizational participation of respondents was measured on the basis of the nature of their participation in 9 selected organizations. Organizational participation score = P x D
Where, P- Participation Score
D- Duration (no. of years). Following scores were assigned for nature of participation:
Nature of participation Scores assigned
No participation 0
Ordinary Member 1
Executive Member 2
Executive Officer (President, Secretary, Treasurer) 3
27
Finally, organizational participation score of a respondent was computed by adding all the scores obtained by her against all the selected organizations.
3.4.1.10 Food safety and hygiene knowledge
Food safety and hygiene knowledge of the women referred to the knowledge gained by the respondent in food safety and hygiene knowledge activities. A scale consisting of 13 questions was used to determine the food safety and hygiene knowledge score of the respondents. The questions were selected from different dimensions of food safety and hygiene knowledge after thorough consultation with the relevant experts and review of relevant literatures as shown in Appendix A. The score allotted for each question was 2. A respondent could get 2 marks against each question for correct response and 0 for wrong or no response and partial score was assigned for partially correct answer. Thus, food safety and hygiene knowledge score of the respondents could range from 0 to 26, where 0 indicated no knowledge and 26 indicated high food safety and hygiene knowledge.
3.4.1.11 Attitude towards food safety and hygiene
Attitude towards food safety and hygiene was measured by developing an attitude scale through Puttaswamy (1977) given scale that developed a scale to measure the attitude of village extension workers towards training and visit system in Indian context. Here five-point Likert method of summated ratings was used to find out the attitude food safety and hygiene.
Eight statements expressing attitude towards food safety and hygiene were constructed. Out of these ten statements those were positive. Scoring was done by assigning 5, 4, 3, 2 and 1 scores to the five alternative responses as "strongly agreed", "agreed", "neither agree nor disagree", "disagreed", and "strongly disagreed", respectively in case of a statement. However, attitude towards food safety and hygiene of women was obtained by summing up her scores for all the eight statements in item no. 11 in the interview schedule. Attitude score, thus, obtained for a respondent could range from 8 to 40, where 8 indicated no attitude and 40 indicated highest level of attitude.