-Abstrak
Peningkntan
jwnlah
kasus HIV positif dan AIDS baikdi
lttdonesia naupundi
seluruh dunia hatrtpir pasti telah atau aknn nenyebabkan peningkatan hasil inajing susunan sarafpusatyang positif. llalaupun tidakada gunanya,nelakuknnskrining rutin dengan conrputeriTed to,nography (CT) atau ilngnetic resonance inaging (MRI) pada susunan saraf pusat penderita HIV positif yang tidak bergejala, kedua cara tadi (terutann MRI) sangat baik untuk nendeteksi dan penatalaksanaan kelainan susunan saraf pusa pada penderita yang bergeiala.Atrofi
otak adalah te,,ruan yang tersering (40%); kelainanini
biasanya ditenrukan pada ensefalitis HIV subakut, konpleks denensia AIDS dan beberapa infeksi oportunis. Massa intrakranial pada AIDS paling sering disebabknn toksoplas-nrosis dan linrfoma, jarang terjadi oleh sarkona Kaposi, tuberktlonn, abses akibat infeksi jatnur dan bakteri. Karena diagnosis dini toksoplosttrosis dan pengobatann)'a ),ang tepat dapat mengubah perjalanan penyakit tersebut secara berttnkna, perlutrkoli i,çk"i
parasit itu dibedakan dari lintfona. HaI ini dapat nenyulitkan, ,nengingat kedua penyakit tersebut tnetniliki banyalaciri
inajing yang sana. Seringkali suatu pengobatan antitoksoplasmosis yang dilakukan secara enpiris dapat tnenyelesaikan nasalah tersebu.t. Kelainan nasa kelabu otak sering ditenuknn pada ensefolitis HIV subakut, kompleks dentensia AIDS dan ensefalopati ntultifokal progresif; pada penyakit terakhir ini dapat terjadi penatnbahan intensitas gantbar (enhancetnent). Perubahan leptonteni-ngeal dan ependitnaljarang ditetnukan, tetapi dapat terjadi pada beberapa infeksi oportuttis dan neoplasnru. CT dapat tnendeteksi sebagian besar kelainan yang luas ini, tetapi pada kebanl,llsp kasus,MN
tebih unggul.Abstract
The increasing nunrbers of HlV-positive and AIDS cases, both itt Indonesia and worldwide, have caused or
will
altnost certai,.tly be attended by an increase of positi'te results of imaging studies of the central nervous syste,il (CNS). Wherea.s ir is useless to do routine screening with cranial CT or MRIfor
o$t,ttptotilatic HIV positive individuals, innging rnodalities and especially MRI are very good in detecting, and nnnitoring the CNS abnonnalities in qtnptonatic patients. Cerebral atrophl, is the tttost cottunonf nding (40%), and is usually seen in subacute HIV encephalitis, and the AIDS denentia cotttplex (ADC), as well as sottte of the opportwtisric infections. Intracranial /lasses are nost contrtronly caused by totoplasnosis and Iyttrphottn, and rarell,by Kaposi's sarcotna, tuberculotla,fu.ngal andbacterialabscesses. Sinceearll,diagnosisoftotoplastnosisandappropriatetherapycansignificantlyalterthecourseofthedisease, differentiaring this parasitic infectiottfrotn
lynphotnais
crucial. This can bedfficub
sinceboth
entities sharettnny
ittnging characteristics. An enpirical anti-toxoplosnosis drug therapy trial is oJten helpfut. White tnatter abnortnalities are co,,y,to,t itt subacute HIV encephalitis, ADC and progressive nultifocal leuco encephalopathl'(PML). Leptotneningeal and ependyttnl changes are rare, but can arise in conjunctiottwithsone of the oPportunistic infections and tteoltlastns. CTwill detect tnany of the tnore extensive abnornn6ties, but MRI is better in,ilost cases.Keywords : HIV, brain, CT,
MN,
infection, inutunocontpronised. Vol 4, Nol,
January-March, 1995Neuroimaging of
AIDS
Mardj ohan Hardj asudarma
I
and Marjadi
Har-dj asudarma2INTRODUCTION
The
acquired immune deficiency syndrome (AIDS)
is
rapidly
spreading
worldwide, with
devastatingconse-quences
reaching
far
beyond the medical effects.
Developing countries
suffer proprotionally
more
dueto
underfunding, insufficient equipment and trained
Neuroimaging of AIDS 37
personnel,
andoften
alack of understanding
asto
thegravity
of
the problem. Nevertheless,
an increasing
number of cases
will eventually
be exposed todiagnos-tic imaging. This ardiagnos-ticle
will review
theimaging
char-acteristics
of
AIDS
of
the central nervous
system(CNS) within the context of
an often confusing
and inadequateepidemiologic
andclinical
picture.
I
Departtnent of Radiology, Louisiana38
HardjasudantnandHardjasudarnwEPIDEMIOLOGY
The
number of
humanimmunodeficiency
virus (HIV)
positive
casesin
the United
Stateswas 1-2 million,
with
3million worldwide
in
1988.This
wasprojected
to increasetenfold in
4 years. There were 22,000AIDS
casesin
theU.S. in
1986,with
50,000 new casesbeing
reported
"rr"ry
y"u.. l'2 In tggz the World
Health
or-ganization (W.H.O) reported an excess of
500,000 casesworldwide and
felt
that the true number
wascloser
to
2
million.3
In
addition, an estimated
8-10million
adults and
1million children were
HIV-posi-.A
tlve.'
The
first
caseof AIDS in Indonesia
wasreported
in
1987.4By
l992,there
were
33AIDS
and
111HIV-positive cases.' These
figures
are believed
to
bespuriously
low, by
a factor
of
100
or
more, due
tounderdiagnosis
andunderreporting.6
A.
has beenob-served
in
other parts
of
the world, it
is
felt
that
thepattern of transmission
will
soon alsoinvolve women
and
the heterosexual
population
in
ever
increasing
numbers.5Following
HIV infection, seroconversion
takes2-6
months or more, whereas theincubation period for
AIDS is 6 months
to
15 yearsor longer,
with
a mean andmedian of approximately
l0
years. Tento l8%
of
people who
areHlV-positive
will
develop AIDS in
5 years,by l0
years this growsto50%. Another
54%will
develop
theAIDS related complex
(ARC) in 5
years, andof
lhese25%
will
haveAIDS in
3 years.There
iscontroversy regarding surveillance
criteria
developedby
the Centersfor
DiseaseControl (C.D.C.) for ARC
sinceit
can havelittle prognostic
value. In fact, patients candie from ARC without
everdeveloping
AIDS.
Forty
percent
of
AIDS/ARC
caseswill
developabnormalities of
the
CNS, and another 1O% will
presentwith
aCNS
lesion as thefirst
sign.At
autopsy,73-80% show
CNS lesions,
and7l
% havemore
thanone pathologic abnormality, suggesting that many
of
theCNS infections remain subclinical.
Although
therisk
becoming HIV infected
isnow
anoccupational
hazard, health careworkers
need to bereminded
that thepossibility of contracting
Hepatitis-Bfrom
an accidental needlestick is
15-75 times greaterthan AIDS. Optimal protection is always mandatory,
and
the
importance
of
being
vaccinaled
against
Hepatitis-B
cannot
beoveremphasized."'
NEUROIMAGING
Opportunistic infections involve
the CNS in
2O-4O7oof
AIDS
cases,and
tumors
in
5-15%. The so-called
"HlV-related"
category affects
30-607o,of which
theAIDS
dementiacomplex
(ADC)
is the mostprominent.
Med J Indones
Cerebrovascular accidents
(CVA)
are reported
in
3-70%.rInfections
Toxoplasmosis, cryptococcal
meningitis, progressive
multifocal
leukoencephalopathy
(PML),
cyto-megalovirus (CMV), cysticercosis,
amebicmeningitis,
nocardia, E.coli, T.pallidum,
and others.Toxoplasmosis
In the adult
AIDS
patient, Toxoplasma gondii
cancause a fulminant necrotizing encephalitis. It
is
themost frequent opportunistic
brain infection, and
themost
common cause
of
an intracranial
mass in
AIDS.I'7
Toxoplasma lesions
aremost commonly
lo-catedin
the basalganglia
and at thegray-white matter
junction
of
the cerebrum, Cerebellar and
brain
stemlesions are much less
common. Magnetic
resonanceimaging (MRI) is more sensitive
in detecting
old
andnew toxoplasma lesions.
On long
TR|IE
images
the lesions,which
areoften multiple,
areof variable signal
intensity,
and canusually
beidentified
asnodular
foci
surrounded by edema. Enhancement patterns
areusually ring-like, although small lesions
can
appearsolid, on both computed
tomography (CT) and MRI.
From the
clinical
standpoint,
the
most important
pathologic entity which
may have asimilar
appearancein lymphoma, especially
if
there isjust
asingle
lesion.When toxoplasma encephalitis
is
suspected based onclinical and
imaging data, empirical
treatment
is
in-itiated. If effective,
follow-up imaging studies
will
document
a decreasein the
degreeof
edema anden-hancement
of
the lesions
in
2-4 weeks.
If not, other
causes,especially lymphoma should
be considered.In
certain
cases,stereotactic
brain biopsy may be
indi-cated.Old or
healedtoxoplasma lesions
canmineral-ize. C'| is usually better to
detect thesecaicifications,
thanMRI.7
PML
a
Vol 4, No
l,
January-March, 199550%
of
cases, there can be extension across the corpuscallosum,
mass
effect, and
enhancement.SEven
thewhite matter
lesions tend to be more
variable
in
ap-pearance.In one series,
all
lesions
were
asymmetri-cal.r'7'9
Cryptococcosis
On
MRI,
punctate hyperintensities are
found,
repre-senting cryptococcomas
or Virchow-Robin
spacesdi-lated
by
the infectious organism. Contrast
enhan-cement isuncommon,
andalthough
MRI
is
moresen-sitive
than
CT, both
modalities underestimate
thepathologic extent
of
the disease. l0CMV
This
organism
is often asymptomatic, and
seldom
demonstrable
on either
CT
or
MRI. CT
may
show
enhancing subependymal lesions.
MRI has
beenreported
to showperiventricular hyperintensity.
CMV
is
also the mostcommon
causativeorganism
in
retinal
infections
in AIDS.l'7
Herpes
Both
HSV-I
and
HSV-II
can
cause
encephalitis
in
AIDS
patients. There is apredilection
for
thetemporal
lobes,
which
areusually unilaterally involved.
When
both temporal
lobes areaffected,
thefinding
ispracti-cally
pathognomonic.
In
AIDS, herpes
infection
of
otherportions
of
thebrain
has beenreported.l'7
Neoplasma
Lymphoma
is
most common,
whereas
Kaposi's
sar-comais very
rare.Lymphoma
Both primary
and secondary
lymphoma occur
in
the CNS, theformer
much morefrequently
than the latter. IPrimary lymphoma
usedto
be
very
rare
in
the
CNS,but
its
incidence
hastripled
dueto its frequent
occur-rence
in
AIDS.
Almost
all
are of the non-Hodgkin
variety. In contradistrinction to
secondary lymphoma
which
is
usually
extra-axial (subarachnoidal;
ex-tradural), primary
lymphoma
is most commonly
parenchymal (intracerebral). Primary lymphoma
is thenumber
two
causeof
anintracranial
massin AIDS, it
usually
enhancesin
a ring-like
pattern,
and may
bemultiple
in up to 50%
of
cases.Thus,
differentiation
from
toxoplasma encephalitis
can bedifficuit.
On
the other hand, when asingle lesion
isfound
onMRI, it
isNeuroinaging of
AIDS
39four
times more
likely
to
belymphoma
thantoxoplas-mosis."
The preceding
is
also in stark contrast
to
primary
lymphoma
in non-AIDS
patient,
in
which
thelesion
ishardly
evermultiple,
andwhere
theenhance-ment
is
often
homogenous
and intense.l'll
Parenchymal lymphoma
is
classically found
in
the deepgray matter,
periventricular
areaand the
corpuscallosum.
Up to
three quatersof
these masses extend to the ependymallining
of theventricles,
the meninges,or
both.
The
massesdo not calcify
and
hematomaformation
is rare.The
lesions areoften
is so intenseto
gray matter on
all spin-echo
sequences, afinding
often
encountered
with
small
cell,
hypercellular
tumors.HIV
related
Very
common:
ADC.
Rare: vacuolar myelopathy
(thethoracic spinal cord
is
most
severely
affected),
and asepticmeningitis
(sometimeswith
facial
nerveinvol-vement; usually
self limited,
but may recur).
ADC
Direct infection of
the
brain
by
HIV
causes subacuteencephalitis,
and the presenceof
multinucleated giant
cells,
scattered orclustered
in microglial
nodules,first
in
thewhite
matter, and later
in
the basalganglia
andcerebral cortex. They
arealso found
in
thebrainstem,
cerebellum and
spinal cord. Although
MRI
is
better
than
CT,
magnetic
imaging
will
detect abnormalities
at a relatively
late
stageof
the disease,l2 most
com-monly
in the
form
of
enlargement
of
the sulci
andventricles (atrophy),
andsmall patchy hyperintensities
which
may progress, enlarge, and become confluent.
The hyperintense Iesions represent areas ofdemyelina-tion
andvacuolization. Cerebral atrophy
itself is
very
common
in AIDS, occuring in
4O7oof
cases, and canalso be seen
in
otherbrain infections
such astoxoplas-mosis and
CMV.
Subacute
HIV
encephalitis
in
theAIDS
patient
who clinically
hasdementia,
is
called
the
AIDS
dementia complex,
or
ADC.
On
MRI,
widespread,diffuse involvement of
a large areacorre-lates
well with ADC.
Patchy
or
punctate lesions
canalso be found
in
ADC, but are
less
"o--on.
13Th"
lesions do not enhance, and tend to be moresymmetri-cal
thanin PML.I'7
CVA
Cerebrovascular
occlusive
disease, intracranial
hemorrhage andvasculitis
have been reportedin
AIDS
patients"usually
in
conjunction
with
opportunistic
-40 H ardj asuda n t
n
and H ardj as u.d arna
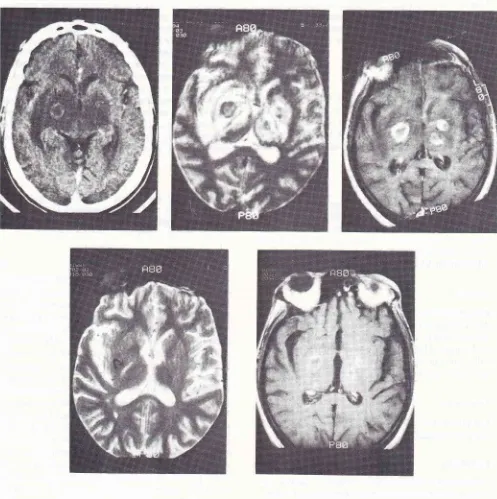
Med J IndonesFigure l.Contrast-augnented CT (a) shows bilateral thalatnic and basal ganglia swelling.
A
ring-enhancing lesiotr is present on theright (arrow). Despite notion artifacts caused by the restless patient, the lesions are better depicted by M RI, especially on the Iefi side
[image:4.595.66.563.93.592.2]7
Vol 4, No
I,
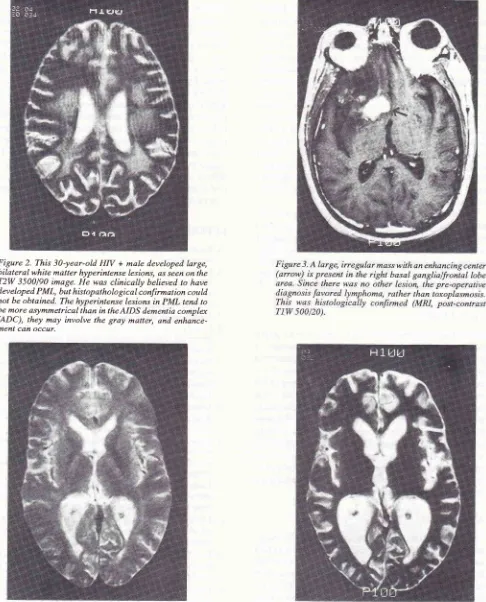
January-March, 1995Figure 2. This 30-year-old
HN
+ male developed large,bilateral white matter hyperintense lesions, as seen on the
T2W 3500/90 image. He was clinically believed to have developed. PML, but histopathological confirmat ion could not be obtained. The hyperintense lesions in PML tend to
be more asymmetrical than in theAIDS dementia complat (ADC), they may involve the gray matter, and enhance-ment can occur.
Neuroitnaging of ÀlDS
4t
Figure 4. This 25-1'ear-old HIV + rnale had an essentialb' nornal M R scan upo7t preseltatio1t (a: T2W 20OO/80). A repeat stutly 2 yearS
[image:5.595.314.546.84.354.2] [image:5.595.56.542.87.689.2]7
42
HardjasudarnnandHardjasudannaIn
theearlier
stagesof
the disease theyield of CT
andMRI
islow. It
is pointless,for
example, toperform
routine
screening
cranial
MRI
in
neurologically
asymptomatic HlV-positive subjectr.la
CT
will
un-doubtedly
detect mostof
the large, andobvious
abnor-malities,
especially
if
done
with
enhancement.
Extensive
areas
of
brain involvement
by
toxoplas-mosis or lymphoma,
for example,
arenot likely
to
be missed.Moderate
to severeatrophy is
alsocommonly
diagnosed,or
at least suspected, onCT. However,
it is
clear that in most instances
MRI
is superior
to
CT.
Enhanced
MRI
is often very helpful in revealing
the extent, or the numberof
lesions,however T2 weighted
imagescan actually
besuperior.ls Wh"n
MRI
is
per-formed,
it
is best to perform short and long
TR
spin-echo
sequences,as well
asa series
of
post-
contrast enhancedTl
weighted
images.A
numberof nuclear medicine
(SPECT, orsingle
proton
emission computed tomography), positron
emission tomography (PET) and
MR
spectroscopy studies have shownpromise
inshowing early
manifes-tations of
the disease, sometimesin
the absenceof CT
or
MRI abnormalities.
They can also used todocument
improvement,
as thepatient improves
clinically.
l'7'16CONCLUSION
The relentless
increase
in
HlV-positive
and AIDS
patients
will
almost
certainly cause
an increase
in
positive imaging studies
of
the CNS. Toxoplasmosis
and lymphoma are the most common
cause
of
in-tracranial
massesin AIDS,
and they share manyof
theimaging characteristics.
Clinical
management often
includes an empirical
trial
of
antitoxoplasmosis
medications.
It
is
important
to
definitively
diagnosetoxoplasmosis
early, since
the infec'tion usually
respondswell to therapy.
SubacuteHIV
encephalitis,
ADC
and PML also share some imaging
charac-teristics, their clinical
course is relentless. Other
en-tities which
are uncommon,
or
arerarely manifested
onimaging
studies, arebriefly
discussed.ADDENDUM
Spin-echo (SE) sequences are
commonly
usedin
mag-netic
resonanceimaging (MRI).
Tl
weighted
(TlW)
and
T2W
sequencesare integral
components
of
SEMRI.
The
TIW
sequenceis characterized
by a
shortrepetition time (TR),
and
ashort echo time (TE), for
example TR |TET 5Ol2O.Both
theTR
and theTE
values are expressedin milliseconds. Long TR and long TE
values
signify
the T2W
sequence,
for
example
3500/90.
Becauseof
thesecharacteristics, many
nor-mal
andpathologic findings
show different
signal
in-Med J Indones
tensities on
TIW
andT2W MRI.
Edema,for example,
shows
up as a hyperintense
("bright")
areaon T2W
images, but is hypointense
("dark") on
TIW
images. Theintravenously administered MRI
contrastmaterial
used was gadopentetate
dimeglumine (Gd-DTPA)
which shortens both
T1
andT2,
thereby
resulting in
areasof
greateror
lessersignal intensity, respectively.
Post-contrast
MR
imaging
is
cnstomarily
done with
TIW
sequences, where enhancement is seen ashyper-intense signal. As with
computed
tomography
(CT),
enhancementwithin
thecentral
nervous system is due to either vascular structures, ordisruption
of theblood-brain barrier which then allows contrast
material to
escapeinto
thebrain parenchyma.
Contrast-enhancedMRI
is more sensitive then
contrast-enhancedCT, in
thatit allows detection of
more lesions, or moreexten-sive pathology,
orboth.
REFERENCES
l.
ReedersfWAL
Diagnostic imagingin AIDS.
Stuttgart: Georg Thieme Verlag, 1992.2.
Hollander
H, Katz MH. HlV-related conditions.
In:Schroeder SA, Tiemey
LM,
McPhee SI, Papadakis MA,Krupp MA, editors. Cunent medical diagnosis & treatment.
Norwalk: Appleton & Lange, 1992;992-lOO8. 3. AIDS sejagad. Berita Epidemiol RI, Juli 1992.
4. Ilyas J. Masalah dan kebijaksanaan pencegahan dan
pem-berantasan acquired immuno deficiency syndrome (AIDS) di Indonesia. Berita Epidemiol
RI,
1992;7-15.5. Ridwan RM. Pengidap
HfV
dan kasus AIDSdi
Indonesia s.d. 30 Juni 1993; L8-22.6. Utomo
B.
Masalah dan implikasi epidemiologiAIDS
di Indonesia. Bul Epidemiol Indon 1992; 4tl-35.
7. Bowen BC, Donovan Post
MI.
Intracranial infection. In:Atlas SW. Magnetic resonance imaging
of
the brain and spine. New York: Raven Press, 1991; 501-38.8. Wheeler
AL, Truwit CL,
Kleinschmidt-DeMasters BK, Byrne WR, Hannon RN. Progressive multifocal leukoen-cephalopathy: contmct enhancement on CT scans and MRimages. Am J Roentgenol 1993; 161: 1049-51.
9.
Mark
AS, Atlas SW.
Progressivemultifocal
leukoen-cephalopathyin
patientswith AIDS:
appearance on MRimages. Radiology 1989; 173: 517-20.
10. Mathews VP, Alo PL, Glass ID, Kumar Atr, McArthur IC.
AlDS-related CNS cryptococcosis: radiologic-pathologic correlation. AJNR 1992; 13: 1477 -86.
11. Rauch RA, Bazan C III, Iinkins RI. Imaging of infections
of
the central nervous system. Curr Opinion Radiol 1992; 4:43- 51.
12. Donovan Post MJ, Tate
LG,
Quencer RM, Hensley GT,Berger IR, Sheremata WA, Maul G. CT, MR, and pathology in HIV encephalitis and meningitis.
AINR
1988; 9t 469-76. 13. Olsen WL, Longo FM, Mills CM, Norman D. White matterdisease in AIDSL: findings at MR imaging. Radiology 1988;
ï
Vol 4, No
l,
January-March, 199514. Donovan Post MI, Berger fR, Duncan R, Quencer RM, Pall
L,
Winfield D.
Asymptomatic
and neurologically
symptomaticHIV-
seropositive subjects: resultsof
long-term MR imaging and clinical follow-up. Radiology 1993;188:727-33.
Neuroinnging of
AIDS
4315. Brant-Zawadski lr,t, Mattox S. Value of Gd-DTPA in brain MRI of Aids patients. MRI Decisions 1991; Jul/Aug: 2-10.
16, Donovan Post ML Neuroimaging in various stages of human immunodeficiency virus infection. Cur Opin Radiol 1990; 2: