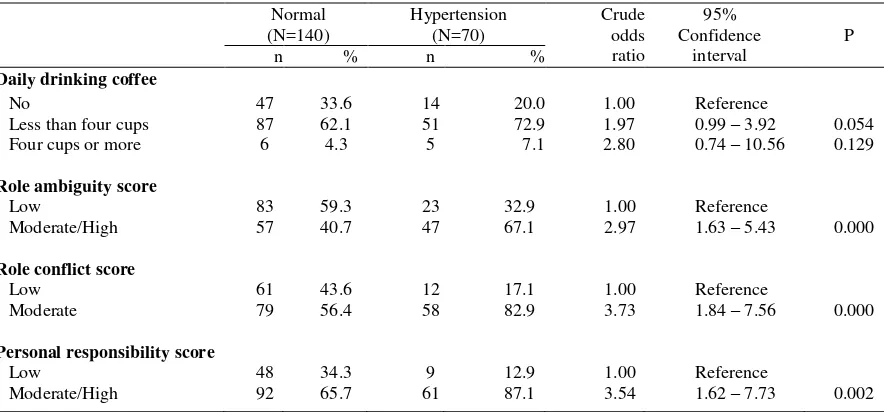
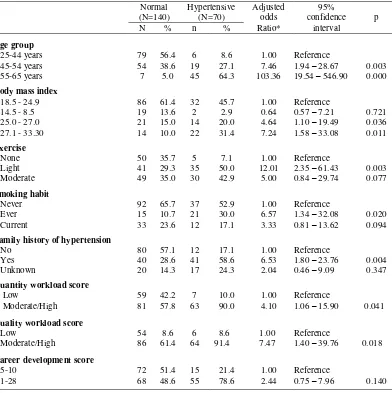
Job stressors and other risk factors related to the risk of hypertension among selected employees in Jakarta
Teks penuh
Gambar
Dokumen terkait
A previously introduced network approach (Peusner, 1970, 1983) is shown to yield known linear transport equations without using Onsager's theory.. Although these equations are
Kerusakan ini dapat merusak pulpa, dengan atau tanpa menyebabkan kerusakan pada mahkota dan atau akar, atau pada kasus yang parah dapat menyebabkan perpindahan
According to available data from 2008 to 2016 and studies on a variety of modeling methods using time series analysis, the modeling is based on polynomial method and
Standar ini merupakan dasar teknik untuk membantu perancangan, pemasangan, pengu- jian, pengoperasian, dan pemeliharaan dari sistem manajemen asap yang baru atau
adalah badan hukum yang merupakan persekutuan modal, didirikan berdasarkan perjanjian, melakukan kegiatan usaha dengan modal dasar yang seluruhnya terbagi dalam saham dan
portofolio pada kelas eksperimen maupun data nilai dari kelas kontrol yang tidak. diberi perlakuan. Tes ini dilakukan sesudah perlakuan tentang metode
Data kesehatan masyarakat diambil menggunakan berbagai macam cara yang umumnya didefinisikan sebagai fakta atau gambaran dari suatu fakta ketika data tersebut
menjadi salah satu daya tarik wisata alam di Kabupaten Gunungkidul. Sejak awal dibukanya pantai ini menjadi destinasi wisata, sudah mulai.. dikunjungi oleh wisatawan, yang
