Association
of
disease
activity
and pericardial
effusion
on
systemic lupus
erythematosus
patients
Nurhay
Abdurahman, Idrus
Alwi,
Lukman
Hakim,
DasnanIsmail, Hardjanti Soelistijo*
Abstrak
Efusi perikard merupalan kelainan jantung yang paling sering ditemukan pada pasien lupus eritomatosus sistemik. Adanya efusi perikard sering dikaitkan dengan aktivitas penyakit, hipoalbuminemia dan gagal ginjal kronik. Telah dilakul<nn penelitian prospektif untuk melihat hubungan antara aktivitas penyakit dengan kejadian efusi perikard pada pasien rawat inap dan rawat jalan di Bagian Penyakit Dalam RS.
Dr. Cipto Mangunkusumo mulai bulan Oktober
1995 sampai JuIi 1996. Aktivitas penyakit dinilai dengan Lupus Activity Criteria Count (L'ACC). Dilakukan pemerilcaan ekokardiografi mode-M dan 2-D untuk mendeteksi efusi perikard pada tiga puluh enampasien LES masing-masing 17 pasien LES aktif dan 29 LES tak aktif. Pada penetitian ini efusi perikard lebih sering ditemukansecara bermakna pada LES alatT fu < 0.0 I ) dan merupakan faktor risiko yang independen.
Abstract
Preicardial effusion (PE) is
the most common cardiac abnormality found in SLE. The presence of PE was frequently associatedwith disease activity, hypoalbuminemia and chronic renal failure. A prospective study had been done to observe the coruelation betvveen disease activity, and the presence of PE in patients with SLE admitted at the Departrnent of Internal Medicine Dr. Cipto Mangunkusumo HospitalfromOctober1995 toJune1996. Inthisstudythediseaseactivitywasmeasuredwithlupusactivitycriteriacount(LACC)and M-mode and 2-D echocardiography to detect the presence of pertcardial effusion. Of the 36 patients with SLE, 17 patients were found
with active SLE and 19 with inactive SLE. This study showed thdt the PE was more frequently found in active SLE (P
< 0.01) and
constituted independent risk factors.Keywords : Systemic lupus erythematosus, pericardial eflusion, disease activity
INTRODUCTION
Systemic lupus
erythematosus
(SLE)
is
an
autoim-mune
disease
with highly va{ed
clinical
manifesta-tions
involving
manyorgans.r-r Cardiac abnormalities
constitute
oneof very important SLE
clinical
manifes-tations, becauseof their impact
onmorbidity
andmor-tality.2'4's
Pericarditis
is themost frequentlv
encountered cardiacabnormality in SLE.6-Il oànerty
and Siegel,6in their
review article reported a
prevalence
of
pericarditis
amounting
25,6Voout
of
1194SLE patients,
andfrom
254
autopsy
cases, they found
an
even higher
prevalence
o162,l%o.These
figures
demonstratethat asymptomatic
pericar-dial
involvement
is often found.
Cohen and Li,a
reported
amortalities
dueto
pericarditis
and myocar-diti sin
I 5 Voof
their S LE p atients.With
increasing SLE
patient
life
expectancy
andbetter
imaging
modalities,
cardiac
involvement
in
SLE may
be more
frequently
diagnosed.s'6Uting M-mode
and 2-D
echocàrdiog-raphy,
the prevalence
of
pericardial effusion
in
SLE
patients was reported to rangefrom
20 to 54Vo7.t2-t9 inwhich
most
of
them were
without
clinical
manifesta-tions.8'12'16Lupus pericarditis may
bemanifested
as cardiac tam-ponade case s.20-26 KaÉP7reported cardiac
tamponadein
l3Vo
of
pericarditis
casesand
in
2,5Voof all SLE
cases. Severalfactors
might
contribute
to thedevelop-ment
of
cardiac
tivitv.f2'la'16
duster;id
use3l
an tibody. l s'28'32-:oa relationship between
disease
activity
and
cardiacabnormalitiei in
SLE.l3'37'38Ho*"u"r
the association Division of Cardiology, Department of Internal MedicineUniversity of Indonesia, Faculty of Medicine/Dr. Cipto Mangunkusumo Hospital, J akarta, Indonesia
90 Abdurahman et al.
of
diseaseactivity
andpericardial effusion is still
un-known
due to thefact
that, bias causedby confounding
factorslike hypoalbuminemia
andchronic
renalfailure
were
not considered.
In
addition
thecriteria
of disease
activity
used are alsovaried.
This
study
wastherefore
performed to
assess associationof disease
activity
andpericardial
effusion
prevalenceby taking
into
account alsoall
possible confounding factors.
MATERIALS
AND METHODS
A
crosssectional study
was conducted onall
hospital-ized
and
ambulatory SLE
patients
in
the Department
of Internal
Medicine, University
of
IndonesiaMedical
School,
Dr.
Cipto
Mangunkusumo
Hospital,
Jakartafrom
October
1995 toJuly 1996.
The diagnosis ofSLE
was established according
to
the
revised ARA
criteria.3g
Exclusion
criteria
were
as follows
(1)
pericardial effusion as
the
only clinical
manifestation
of
SLE activity,
(2) pulmonary
or
extrapulmonary
tuberculosis, (3)
MCTD
(mixed connective
tissue dis-ease),(4)
acutemyocardial infraction, (5)
congestive
heart
failure,
(6) malignancy,
(7)
acute
rheumatic
fever, (8)
postpericardiectomy,
(9) postirradiation of
the
chest. Disease
activity
was
assessedby
using
LACC
(Lupus
Activity Criteria
Count).40 Based
oncalculation
the
minimal
number
of
sample
was
10patients
for pericardial effusion
(PE)
and nonpericar-dial effusion
(NPE)
groups.For
all
patients,
acomplete
history
andphysical
ex-amination,
standardECG
and chestX
ray
were taken.Laboratory investigatios included: peripheral
blood
and urinalysis,
ureum,
creatinin,
albumin,
anti-dsDNA,
complement
C3
and
C4. M-mode
and
two-dimensional echocardiographic examinations
were
conducted
in all
patients
by
using
aToshiba
echocar-diographic
unit with
mechanical transducer
of
3,5MHZ.
Standard parasternal
long axis,
short
axis and
apical 4
chamberexamination were
done.Recordings
were performed
with
Toshiba ultrasonostrip chart
on paper speedof
50 mm/second.Echocardiographic
datewere read by a cardiologist
who
did
not
know
thepatients
condition
and
the results werc
analyzed
ac-cording
to
the
recommendation
of
the
American
Society
of
Echocardiography.al
RESULTS
In
aperiod
from
Ocrober
1995to July
1996,42 SLE
patients satisfied the
1982ARA
criteria. Four
patientswere
excluded
from
the
study
becausethey did
not
appear
for
echocardiographic examination and two
Med J Indones
other patients
with MCTD
were alsoexcluded, leaving
36eligible
patients.Prevalence
of pericardial effusion
Based on
echocardiographic examination
13 (36.llVo)SLE patients were shown to
havepericardial effusion
and23
(63.89Vo)patients
hadno
pericardial
effusion.
Of
the
13
patients
with
pericardial
effusion,
l0
(76.92Vo) patients had
mild
effusion,
2
(15.38Vo)patiens had moderate
effusion
and
I
(7.697o)patient
had severeeffusion.
Seventeen
patients
(47 .2Vo) hadactive
SLE
according
to
ALCC criteria,
of
whom
11patients
(64.7Vo)had
pericardial effusion. Of
theremaining inactive
patientsonly
2 subjects (10.5Vo) hadpericardial effusion.
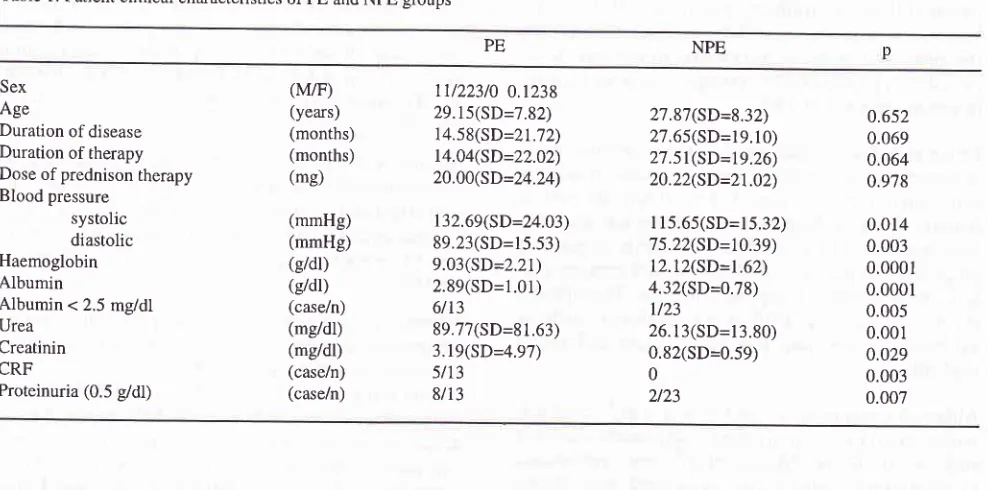
Characteristics of patient
Patient characteristics
of
both
groups
of
patients
arelisted
in Table
1.Association of
disease
activity
and
prevalence
of
pericardial effusion
In
thePE
group 11
patients
(83.3Vo)had active SLE,
whereasin
theNPE group active
SLE
wasfound
in
6patients
(26.09Vo)(X2--9.1 p=0.002, OR
15).
To
as-sess therelationship
of
somerisk
factors
such asdis-ease activity,
chronic renal
failure, severe
hypo-albuminemia
and the presenceof pericardial
effusion,
multivariate
analysis
was
done
with Backward
step-wise method
(LR).
Prevalenceof pericardial effusion
was
mostly related
to
disease
activity
(p=0.002
Cl=2.65-97.56).
DISCUSSION
The
prevalence
ofpericardial effusion in our
seriesof
36patients, was
36. 1 1Vo. This figurewas
similar to
a prevalenceof
2l-54%oreported
in
theliterature. Table
2
shows the prevalence
of
pericardial effusion in
various
reports.The
apparently
slight disparity
in
the
prevalence
of
pericardial
effusion
could
be dueto
differences
in the
level
of
disease activity
at the
time
of
echocar-diographic examination and
in
racial
distribution.
Pericardial
effusion
was
mild in
27.78Vo,
of
the patients moderatein
5.56Vo and severein
2.78Vo. Thesefigures are not so different
from
another study
by
Table 1. Patient clinical characteristics
ofpE
and NpE groupsNPE
PE
Sex
Age
Duration of disease
Duration of therapy
Dose of prednison therapy Blood pressure
systolic diastolic Haemoglobin Albumin
Albumin
<2.5
mgld| UreaCreatinin CRF
Proteinuria (0.5 g/dl)
(M/F) (years) (months) (months) (mg) (mmHg) (mmHg) (e/dl) (e/dl) (case/n) (mg/dl) (mg/dl) (case/n) (case/n)
ll/223/0
0.1238 29.15(SD=7.82) 14.58(SD=21.72) 14.04(SD=22.02) 20.00(SD=24.24) 132.69(SD=24.03) 89.23(SD=15.53) 9.03(SD=2.21) 2.89(SD=1.01) 6/13 89.77(SD=81.63) 3.19(SD=4.97) 5/13 8/13 27.87(SD=8.32) 27.65(SD=19.10) 27.51(SD=19.26) 20.22(SD=21.02)I 15.65(SD=15.32) 75.22(SD=10.39)
12.12(SD=1.62) 4.32(SD=0.78)
l/23
26. r 3(SD=13.80)
0.82(SD=0.59) 0 423 0.652 0.069 0.064 0.978 0.014 0.003 0.0001 0.0001 0.005 0.001 0.029 0.003 0.007
effusion
in 20Vo,
4Vo and 3Vo, ofthe patients
respec-tively. Difference in
the
level of
diseaseactivity
SLE
at the
time of examination could explain
thedissimilar
distribution
of
theseverity pericardial effusion in
somereports. The higher prevalence
of pericardial
effusion
in
active SLE
in
our study
compared
to
that
in
theinactive SLE patients was
in
accordance
with
other
reports by Cervera
et alr2 and
Leung
etal.l6
Association
of
disease
activity
and
prevalence of
pericardial effusion
In this
study
disease
activity
was a
risk
factor for
pericardial effusion
with
an odds
ratio
of
15
times
compared
to
inactive
group. This is
in
agreementwith
Table 2. Prevalence of Pericardial Effusion in SLE
some
studies done abroad. Crozier
et
all4
reported
from their
seriesof
50 SLE
patients
atrend
towardshigher
prevalenceof pericardial effusion
in
activeSLE
as
determined
by LACC criteria. A
possible
explana-tion
is
the
presence
of
confounding factors
such
ashypoalbuminemia, chronic renal
failure,
difference
in
the
level
of
diseaseactivity.
Cervera
et
alrz reported
pericardial effusion only in
active SLE patient.
Activity
criteria were
if
there is
symptom
or
the
following
signs: specific
dermatitis
(malar rash),
arthritis,
serositis, centralnervous
systemdisorder
(recently
occured chorea,
convulsion,
psychosis,
organic brain
syndromenot
causedby drug
or
metabolic
disorder, cerebrovascular disturbance dueResearchers Year Number
of patient EffusionModalities Pericardial %
Authors Ito et allg
Chia et al (quoted from 6)
Badui et allB
Klinkoff et allT Dohertv et al8 L"ung
"t
all6Nihoyannopoulos I 5 Crozier et all4 Ong et all3 Ceweral2 M-mode,2-D M-mode M-mode M-mode M-mode,2-D M-mode,2-D M-mode,2-D M-mode,2-D M-mode,2-D M-mode,2-D M-mode,2-D t996 1979 1981 r985 1985 1988 1990 t990 1990 1992 r992 36 48 21 100 47 50 75 93 50 40 70 13 22 5 39
l0
2l
2t t9 27 t9l9
[image:3.595.42.536.88.333.2]92 Abdurahman et al.
to
embolism, thrombocytopenia
(<
100.000/1),
haemolytic
anaemia, vasculitis (biopsy), or nephritis
(recently
occured haematuria> l0 erythrocyte/field, or
cylinder,
orproteinuria
(> 500mgl24 hour)
or increasein
serumcreatinin
of
25Vo.Leung et all6
alsoobserved pericardial
effusion
morecommonly
in
active
SLE patients. Criteria of activity
were when there is
atleast
3of
thefollowing clinical
features :
fever, without
evi dence ofinfection,
serositi s,new skin lesion or exacerbation,
recently occured or
progressive alopecia, oral ulcers, central nervous
sys-tem involvement,
lymphadenopathy, leucopenia,
thrombocytopenia, ESR
>
55
mm/hour without
evidence
of
infection,
low
complement and
activenephritis.
Although
Cervera er
al2r andLeung et al,l6
useddif-ferent
criteria
for
activitv their
comDonentswere not
still very much alike.
Maéedo etal,a2iound
prevalenceof
pericardial effusion was
associated
with
higher
SLEDAI
score diseaseactivity. SLEDAI
scoreinclude
components
which
arevery similar
toLACC, but
eachcomponent is
measuredfor its
score.Based
on
abovementioned
studies, onemay conclude
that pericardial effusion occurs more frequently in
active SLE patients.
This
is
in
line
with
the
pathogenesis
of
pericardial
effusion
in
SLE that
isassumed
to be
due
to
immune
complex
deposit
originating
from antigen
andantibody reaction.
In
ac-tive
SLE the increasing formation
of
antibody
will
elevate
circulating immune complex which
inturn
will
facilitate
tissuedeposit.
Ong
et
all3
however
did not
find
any relationship
between
LACC
disease
activity
and cardiac
abnor-malities
in
SLE including: valvuvar deformity, left
ventricular disorder, pericardial
abnormalities
(pericardial effusion and pericardial thickening)
andright
cardiac disorder.
In this study, however, the
as-sociation
betweenpericardial
effusion
and diseaseac-tivity
wasnot specifically
evaluated.In.SLE, pericardial effusion may also
be
causedby
hypoalbuminemia
andchronic
renalfailure.
In
areport
by Ong
etal"
of hypoalbuminemia
(serumalbumin <
3,5
g/dl)
wasfound in76Vo
ofpatients with pericardial
effusion, and
all of
them had moderate
and
secerepericardial effusion.
Nevertheless they
failed to
con-sider hypoalbumemia as
a
contributing factor of
pericardial effusion.
In
our study hypoalbunemia
(al-bumin
< 3,5g/dl)
was detectedin
10(76.92Vo)patients
with pericardial effusion. In the PE group normal
al-Med J Indones
bumin level (albumin
> 4g/dl)
wasfound in
onepatient
with
pericardial
effusion and one patient
with
mild
pericardial effusion.
Oneotherpatient
with
analbumin
concentration of
3,5g/dl
hadmild pericardial effusion.
In NPE group albumin level
wasnormal in
most cases(9L3Vo).
The occurence
of
generalized edema was associatedto
severe
hypoalbunemia
(< 2,5 g/dl) including
pericar-dial effusion.
Based on absolute Fisher teststhis
severehypoalbunemia
was significantly
more
prevalent
in
th;
PE group
compaied
to
NPE gtoup
(X2=6.79
p=0.005).
Chronic renal failure
in
another potential
cause
of
pericardi al
effusion (uremic
pericarditis), especially in
overload condition.
In
the PE group, chronic
renal
failure
wasfound in
5 outof
13 patients (38.467o)with
pericardial effusion, while
in
the NPE group chronic
renal failure
wasnot observed. Of
thesefive
patients,one
patient
sufferedfrom pericardial
effusion
andfour
cases had
mild pericardial effusion. On
absoluteFisher
tests,
chronic renal
failure
was found significantly
more common
in the PE group compared to
theNPE
group (X2=7.309
p=Q.QQ3;.At
multivariate
analysis,
of
various
risk factors:
dis-ease
activity, hypoalbunemia
andchronic
renalfailure,
disease
activity was found to be
anindependent
risk
factor (p-0.002). The
assocation
of
hypoalbunemia
and
chronic
renalfailure with
pericardial
effusion
wasnot significant.
REFERENCES
l.
Boumpas DT, AustinIII
GA, Fessler BJ, et al. Systemiclupus erythematosus: emerging concepts. Part
I:
renal,neurophychiatric,
cardiovascular,
pulmonary,
andhematologic disease. Ann Intern Med 1995;122:940-50.
2. Quismorio Jr FP. Cardiac abnormalities
in
systemic lupuserythematosus.
In:
Wallace DJ, HahnBH,
eds. Dubois'Lupus Erythematosus. 4th ed. Philadelphia: Lea
&
Febiger1993:332-42.
3. Stevens
NM.
Systemic lupus erythematosus and thecar-diovascular system: the heart. In: Lahita RG (ed). Systemic
Lupus
Erythematosus.2th
ed.New
York: Churchill
Livingstone; I 992:7 O7 - 17 .
4.
Cohen
MG,
Lie EK. Mortality
in
systemic
lupuserythematosus: active disease is the most important factor.
Aust NZ J med 1992;22:5-8.
5. Ward MM, Pyun E, Studensky S. Cuases of death in systemic
lupus erythematosus. Arthri ti s Rheum 199 5 ;38 : I 492-9 .
6. Doherty NE, Siegel RJ. Cardiovascular manifestations
of
systemic lupus erythematosus. Am Heart J;1985:1257-65.
7. Mandell BF. Cardiovascular involvement in systemic lupus
8. Doherty NE, Feldman G, Maurer G, Siegel RJ.
Echocar-diographic findings in systemic tupus erythematosus. Am J
Cardiol 1988;61- 1144.
9. Ansari A, Larson PH, Bates HD. Cardiovascular
manifesta-tions of systemic tupus erythematosus. Prog Cardiovasc Dis
1985;274:21-34.
10. Jouhikainen
T,
Pohjola SS, StephanssonE.
Lupusan-ticoagulant and cardiac manifestations
in
systemic lupuserytlrematosus. Lupus 199 4;13 (3): I 67 -7 .
11. Maniscolco BS, Felnes
JM,
McCansJL,
Chiopella JA.Echocardiographic abnormalities
in
systemic lupuserythematosus. Circulation 1975;15:Suppl II-21 1.
12. Cervera R, Font J, Pare C, et al. Cardiac disease in systemic
lupus erythematosus: prospective study of 70 patients. Ann
Rheum Dis 1992;51: 156-9.
13. Ong ML, Veerapen K, Chambers JB, Lim MN, Mainsavagar
M,
WangF.
Cardiac abnormalitiesin
systemic lupuserythematosus: prevalence and relationship to disease
ac-tivity. Int J Cardiol 1992;34:69- 74.
14. Crozier IG, Li E, Milne MH, Nicholls MG. Cardiac
involve-ment in systemic tupus erythematosus detected by
echocar-diogcaphy. Am J Cardiol 1990;65:1 145-8.
15. Nihoyannopoulos P, Gomez PM, Joshi J, Loizou S, Walport
MJ, Oakley
CM.
Cardiac abnormalitisin
systemic lupuserythematosus. Circulation 1990;81 :369-75.
16. Leung
WH,
WongKL,
Lau CP, WongCK,
Cheng CH.Cardiac abnormalities
in
systemic lupus erythematosus: aprocpective M- mode, cross sectional and Doppler
echocar-diographic study. Int J Cardiol 1990;27:267-75.
17.
Klinkhoff AV,
Thompson CR, Reid GD, Tomlinson CW.M-mode and
two
dimensional echocardiographicabnor-malities
in
systernic
lupus erythematosus. JAMA
1985;253:3273-7.
18. Badui E, Garcia-Rubi D, Robles E. Cardiovascular
manifes-tations in systemic lupus crythematosus. Prospective study
of 100 patients. Prog Cardiovasc Dis 1985;27:421-34.
19. Ito M, Kagiyama Y, Omura I, et al. Cardiovascular
manifes-tations
in
systemic lupus erythematosus. JapanCirc
J 1979;143:985-94.20. Gulati S, Kumar L. Crdiac tamponade as an initial
manifes-tation of systemic tupus erythematosus
in
early childhood.Ann Rheum Dis;5 1 :279-80.
21. Ehrenfeld
M,
AsmanA,
SphilbergO,
SamraY.
Cardiactamponade as the presenting manifestation of systemic lupus
erythematosus. Am J Med 1989;86:626-7.
22. Leung WH, Lau CP, Wong CK, Leung CY. Fatal cardiac
tamponade
in
systemic lupus erythematosus-
a hazardof
anticoagulation. Aih Heart J 1990;119:422-3.
23. Reiner JS,
Fuirie RA.
Cardiac tamponade as aninitial
manifestation of systemic tupus erythematosus. J Rheumatol
1989;16:1127-9.
24. Zasbin SJ, Lipsky PE. Pericardial tamponande complicating
systemic lupus erythematosus. J Rheumatol 1989;16:374-7.
25. Omdal R, Dickstein K, Brandis CV. Cardiac tamponade in
systemic lupus
erythematosus. ScandJ
RheumatolI 988; I 7:55-7.
26. Averbuch
M,
Bojko A, Levo Y. Cardiac tamponade in theearly postparurn period as the presenting and predominant
manifestation of systemic lupus erythematosus. J Rheumatol
1986;13:44.
27. KahlLE. The spectrum of pericardial tamponade in systemic
lupus erythematosus. Report of ten patients. Arthritis Rheum 1992;35:1343-9.
28. Gaive E, Candei-Riera S, Pigrau C, et al. Prevalence,
mor-phologic types, and evolution of cardiac valvular <Jisease in
systemic lupus erythematosus. N Engl J Med
1988;319:817-23.
29. Bahl VK, Vasan RS, Aradhye, Malavia AN. Prevalence
of
cardiac abnormalities early
in
the course of systemic lupuserythematosus. Am J Cardiol 1991;68:1540-1.
30. Enomoto K, Kaji Y, Mayumi, et al. Frequency of valvular
regurgitation
by
color Doppler echocardiographyin
sys-temic lupus erythematosus. Am J Cardiol
199l;67:209-ll.
31.
Bulkley BR,
RobertsWC.
The heartin
systemic lupuserythematosus and the changes induced
by
corticosteroidtherapy. Am J Med 1975;158:243-64.
32. Roldan CA, Shively BK, Lau CC, Gurule FT, Smith EA,
Crawford MH. Systemic lupus erythematosus valve disease
by
transesophageal echocardiography and the roleof
an-tiphospholi pid antibodies. J Am Coll Car diol 1992'.20 : l l2'7
-34.
33. Gleason
CB,
StoddardMF,
Wagner SG, Longaker RA,Pierangeli, Harris EN.
A
comparisonof
cardiac valvularinvolvement in the primary antiphospholipid syndrome
ver-sus anticardiolipin negative systemic erythematover-sus. Am
Heart J 1993;1 25:1123-9.
34. Khamashta MA, Cervera R, Asherson RA, et al. Association
of antibodies against phospholipid with heart valve disease
in systemic lupus erythematosu s. Lancet l99O;33 5:l 5 4l -4.
35. Leung WH, Wong
KL,
Lau CP, Wong CK,Liu
BW.As-sociation between antiphospholipid antibodies and cardiac
abnormalities in patients with systemic lupus erythematosus.
Am J Med 1990;89:411-9.
36. Chartash EK, Lans DM, Paget SA, QamarT, Lockshin MD.
Aortic
insufficiency and mitral regurgitationin
systemic lupus erythematosus and the antiphospholipid syndrome.Am J Med 1989;86:407-12.
37. Lolli C, Foscoli M, Giofre R, Tarquinii M, Pasquali S, Toschi
GP. Cardiac anomalie in systemic lupus erythematosus: their
prevalence and relation to duration, disease activity and the
presence
of
antiphospholipid antibodies.G Ital
Cardiol1993;23:1125-34.
38. Cujec B, Sibley J, Haga M. Cardiac abnormaliries in patients
with
systemic
lupus
erytematosus. Can
J Cardiol
1991;7:343-9.
39. Tan EM, Cohen AS, Fries JF, et al. The 1982 revised criteria
for
the classificationof
systemic lupus erythematosus.Arthritis Rheum 1982;25:127 1 -7 .
40. Urowitz MB, Gladman DD, Tozman ECS, Goldsmirh CH.
The lupus
activity
criteria count(LACC). J
Rheumatol 1984;11:783-7.41. Shan DJ, Demaria A, Kissio J, Weyman A. The committee
on
M-mode standardizationof
the American Society ofEchocardiography. Recommendation regarding quantitation
M-mode echocardiography: result
of
a survey ofechocar-diography measurements. Circulation 1978;58:1072-83.
42. Macedo TB, Margaredo MS, Rassi C, et al. Cardiac
abnor-malities in SLE. Abstracts. Lupus Avis Intem J Jerusalem,