A CASE REPORT
Ashri Yudhistira, Farhat, Rizalina A Asnir, Syamsul
Otorhinolaryngology Head and Neck Department Medical Faculty, University of Sumatera Utara
INTRODUCTION
Juvenile nasopharyngeal angiofibroma is a rare hypervascular, locally aggressive
benign tumour which is exclusively found in the nose and paranasal sinuses of male
adolescents.
Juvenile Nasopharyngeal Angiofibroma usually originates from the region of the
sphenopalatine foramen just posterior to the middle turbinates.
1
Unilateral or bilateral nasal obstruction, recurrent epistaxis, proptosis and facial
asymmetry are its common signs and symptoms. Typically in boys or young men
complaining from recent nasal obstruction and recurrent epistaxis, this diagnosis should be
considered. On nasal endoscopy a soft vascular and submucosal mass in seen beyond the
middle turbinate.
2
The imaging characteristic of Juvenile Nasopharyngeal Angiofibroma are typical and
diagnostic, and recourse to a biopsy or angiography for confirming the diagnosis is not
required in current times. Computed Tomography and MRI offer complimentary
information.
3
Surgery is considered to be the gold standard Juvenile Nasopharyngeal Angiofibroma
treatment. Other treatement options include radiation therapy (external beam), chemotherapy
and hormone therapy antiandrogen (flutamide).
4
We report a case of nasopharyngeal angiofibroma in a boy aged 17 years following
surgery in degloving approach.
5
Case Reports ( MR: 56 74 12 )
YS, 17 years old boy, came to Adam Malik General Hospital Medan on July 16, 2013
with a main complaint of nasal obstruction. Right nasal obstruction since about 8 months ago
and he also complained masif nosebleeds and stopped after the treatment to the hospital the
1. 2. Figure 1 & 2.
Anterior rhinoscopy showed tumor with smooth surface and hypervascularitation in
dextra nasal cavity and posterior rhinoscopy showed tumor in nasopharynx.
Patient had hormonal therapy (microgynon) for 1 month. There was bleeding where
the bleeding can not be controlled,and had therapy propanolol within 3 month.
The patient had angiografi on July 31,2013, and the result: mass hipervaskuler at
nasopharynx area is very possibly a angiofibroma.
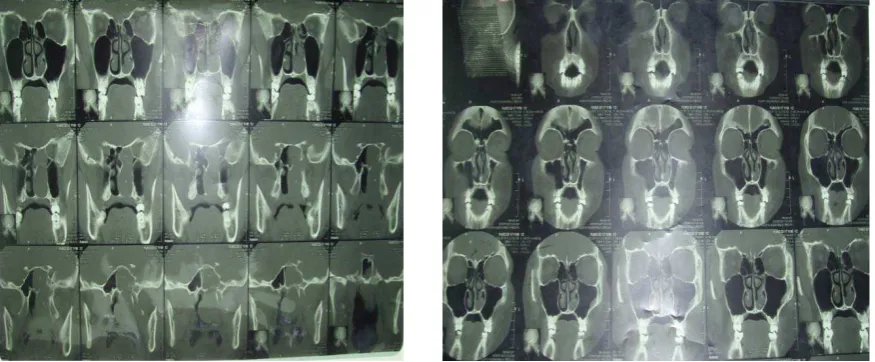
The first CT-Scan (18 th July
2013) that taken before surgery showed a mass soft
tissue in blood density nasopharynx fills all size nasopharynx cavity of 4-5 cm. Surface of
lobulated. Mass extends to choana and nasal cavity especially right side and sinus
sphenoidalis.
Figure 3 & 4. CT Scan Sinus Paranasal
We repeat the CT Scan evaluation on the November 12th 2013 after had therapy
propanolol within 4 months. CT Scan showing a soft tissue mass wide of assertive boundary
with necrotic solid component is very post nasopharynx projection contrast with picture of
obliteration of torus tubarius and fossa bilateral russen. Superior the mass seen extend to
sphenoidalis sinus with suspicion of destruksi base os sphenoidalis. Anterior the mass seen
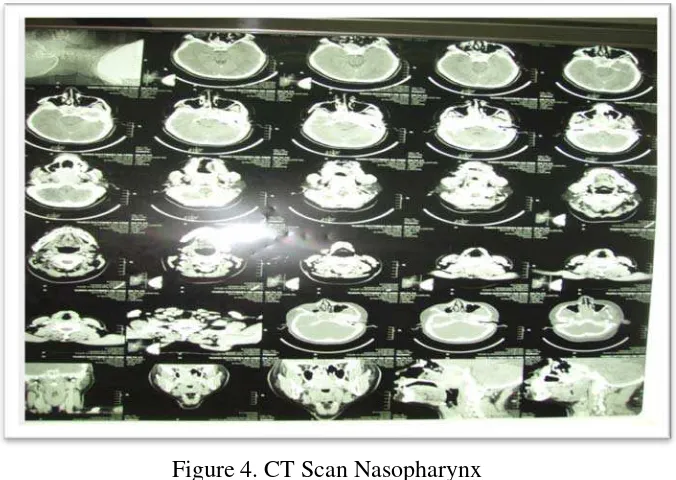
[image:2.595.150.402.69.185.2] [image:2.595.77.515.405.586.2]Figure 4. CT Scan Nasopharynx
Laboratory tests Hb : 12,20 g%, protrombin time 12,50 second, APTT 27,1 second.
We planned for surgery under general anasthesia on November 26th
We diagnose the patient is Juvenile Nasopharyngeal Angiofibroma and we performed
surgical technique used for removal of the mass with Degloving approach in general
anasthesia to removed the mass. Desinfection and pehacain infiltration to the incission site,
the incission made in the sublabial, bilaterally start from maxilla tuberosity from the right to
the left to the periosteum. The soft tissue then detached, the septum cartilage was cut from the
nasal spina up to the nasofrontal suture.
2013. Thorax x-ray and
ECG was normal.
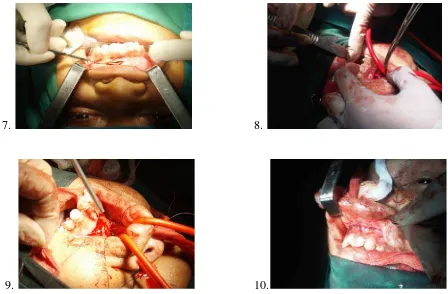
7. 8.
[image:4.595.70.518.69.363.2]9. 10.
Figure 5-10. Procedure of degloving to remove the mass from nasopharynx
Evaluate nasopharynx, with finger and respactorium mass was detached and extracted
from its surrounding tissue. Nasopharynx was evaluated endoscopically to find any residual
tumor. We used posterior tamponade (belloque) and followed by anterior tamponade to
prevent bleeding.
Figure 11. Mass of the nasopharynx
The mass consisted of several lobules with approximate size of the lobules were about
[image:4.595.181.406.509.659.2]On follow-up the overall result was satisfying and patient was discharged on the 4th day after
operation. The histopathology examination showed nasopharingeal angiofibroma.
Discussion
Juvenile nasopharyngeal angiofibroma is uncommon tumor originating primarily in
the nasopharynx with extension to surrounding structures such as nasal cavity, sphenoid
sinus, sella, pterygomaxillary fossa, infratemporal space, inferior orbital fissure, and
intracranial region.6
Extranasopharyngealangiofibroma are vascular fibrous nodules occuring outside the
naspharynx and are rare, benign neoplasms characterized by a different biological history and
clinical features with respect to nasopharyngeal tumours, and for these reasons, should be
regarded as a separate clinical entity.
In this case report the tumor extend to dextra nasal cavity and
sphenoidalis sinus with suspicion of destruksi base os sphenoidalis.
Surgical excision is the treatment of choice. Various treatment modalities like
surgery, radiotherapy, embolization, chemotherapy and hormonal therapy are used and each
has its own limitations.
7
8
A hormonal influence in sinonasal angiofibromas has long been
suggested by the manifestation of this tumor in adolescent males.9
.Various systems of classification exist for angiofibroma. The Radkowski’s
classification is currently popular and increasing stages have been correlated with
incremental rise in tumor reccurences. In this case report by this staging this patient was as
stage II A.
In this case report, patient
had treatment hormonal therapy, propanolol therapy, angiografi and surgey with degloving
[image:5.595.90.525.571.749.2]References
Sinha NK. (2011). Juvenile Nasopharyngeal Angiofibroma Excision Through Lateral
Rhinotomy and Sublabial Approach. J Dhaka Med Coll. 2011; 20(1) : 78-81
Tyagi,I. (2007). Recurrent and residual juvenille angiofibromas. Sarjay Gandhi Post Graduate
Institute of Medical Sciences :pp. 460-461
Ardehali, MM. (2011). Juvenile Nasopharyngeal Angiofibroma, New Aspects in
Management. Iranian Journal of Otorhinolaryngology No.3, Vol.23, Serial No.64,
Summer-2011
Thakar, A. (2013). Nasopharyngeal Angiofibroma. Department of Otolaryngology and Oral
and Head-Neck Surgery,All India Institute of Medical Sciences 2013;6 (1) :pp :25-34
Singh, AC. (2013). Anaesthetic management of endoscopic resection of juvenile
nasopharyngeal angiofibroma: our experience and a review of the literature. Department of
Otolaryngology and Oral and Head-Neck Surgery, All India Institute of Medical Sciences
2013;19 (6) : pp 314-316
Park CK et all. (2006). Reccurent Juvenile Nasopharyngeal angiofibroma treated with
Gamma Knife Surgery. J Korean Med Sci 2006; 21: 773-7
Karthikeyan P. (2014). Extra Nasopharyngeal Angiofibroma of the Sphenoid Sinus: A rare
Case Report. Int J Cur Res Rev, June 2014/Vol 06 (11) p: 8
Junuki, MG. (2007). Nasopharyngeal angiofibroma treated with radiotherapy. Department of
ENT and Head-Neck Surgery, India vol.2; pp 100-101
Montag, AG (2006). Steroid Hormone Receptor Expression in Nasopharyngeal
Angiofibromas. Am J Clin Pathol 2006;125:832-837
Quin, MS. (2012). Juvenile nasopharyngeal angiofibroma : Evaluation and Treatement.