158
Abdoerrachman Med J IndonesPerceptual
and
Acoustical
Assessments
on Spasmodic
Dysphonia: Pre
and
Post
-
Botulinum
Toxin
Injection
Hartono Abdoerrachman
Abstract
Adductor spasmod.ic dysphonia is a vocal disorder of uncertain etiology with no satisfactory long-term treatment-result. Recently injecrton of Botulinum toxin (BOTOX) into the thyroarytenoid muscle has been used as an effective temporary treatment.
In
this experiment, 9 partents with adductor spasmodic dysphonia (SPD) were studicd and injected percutaneously the Bonlinum toxin with dose of injection ranges from 1.25 to 5 units totally. Post teatment results were monitored acousticallyfor
objective voice analysis and auditorilyfor
perceptual judgment. Temporary satisfactory results were obtained after the average of 2 months post-iniection, and lastedfor
at least 5 months of average. The test ofvocal controllability derived from several acoustic parameters exftaction, e.g. the pitch pernrbation quotient (PPQ), amptinde perturbation quotient (APQ), the Fo overallvariability (FoV), energy of slow andfast Fo perturbation (FoS and FoF), showed improvement on post-BOTOX injection, and illustrate thefficacy
of the analysis system used.Abstrak
Disfonia addulctor spasmodik adalah kelainan suara yang etiologinya belwn jelas, dengan hasil terapi jangla panjang yang tidak memuaskan. Dewasa ini injetcsi toksin Botulinwn (BOTOX) læ muskulus tiroaritenoi.d banyak diteraplcan. Pada pmelitian ini dilalatkan sndi pada 9 kasus disfonia ad.duktor spasmodik dengan menyuntikkan 1.25 sampai 5 unit BOTOX melalui kulit ke dalam otot I'aring. Hasil terapi dimonitor secara akustik untuk menganalisis suara secara objektif dan perseptual. Keberhasilan semmtara didapatkan setelah kurang lcbih 2 bulan pasca terapi, dan berlanjut sampai kurang-lebih 5 bulan. Tes kontrol suorayang dihimpun dari hasil beberapa parameter yang
dihiung
yaitu: pitch perturbation quotient (PPQ), amplinde perturbation quotient (APQ),Fo
overall variability(loV), energy of slow andTastperturbation(FoS andFoF) menunjukkanperbaikanyangbermaknapada gruppasca-BOTOX. Hal ini juga menggambarlcan kinerja yang berdaya-guna dari sistem analisis suara yang dipakai.Keyw or ds : sp as tic dy s phonia, v o ice analy sis, v o cal c ontro llab ility.
Spasmodic dysphonia (SPD)
is
acentral nervous
sys-tem phenomenon
of
unknown etiology characteized
by
c€tremor
with
erratic
patternsof
lar
The
uncertainty
of the SPD
etiology
arose researchers toconduct experiments
andoptions in
the treatmentof
SPD patients
to
try
to eliminate the disruptive
voice
resection
of
aPortion
on one side,2Côz
laser 3anterior
laryngoplas-ty,
voice
therapy, pharmacotherapy, and the
most
promising
oneis
Botulinum toxin injection.
Eventhough most
of
opinions
declared
that adductor
SPD was
a vocal disorder with nosatisfactory
long-term treatment-result, many experiments had been
Department
of Otorhinolarytgology,
Facuhyof
Medicine, Llniversity of Indonesia/Dr. Cipn Mangunkusumo Hospital, Jakarta, Indonesiaconducted.
Woodson
et
al4
reported a study on the
effects
of
Botulinum
toxin
therapy
in
patients with
adductor SPD in
term
of
acoustic, aerodynamic
andvideoendoscopy
findings, and
concluded
a successful result on post-therapycondition.
Adams etal'reported
a
study
concerning
unilateral
versus
bilateral
Botulinum toxin injections
in
SPD
for acoustic
andperceptual
results
and concluded
that
unilateral
BOTOX
injections
may provide
both
superior
andlonger lasting begefits than bilateral BOTOX
injec-tions.
Green et al6reported his method
of point-touch
technique
of
Botulinum
toxin injection
for
the
treat-ment
of
SPD
by means
of
flexible
nasopharyngeal endoscopy guidance.Kobayasi
et al/ alsoreported his
successful methodfor
percutaneusinsertion technique
of
the needlefor
injecting the Botulinum toxin into the
thyroarytenoid muscle
of SPD patients.
ofacetyl-VoI 6, No 3, July - September 1997
choline
at the neuromuscular
junction. This
action
isclinically
usedto
alleviate muscle
spasmby injecting
thetoxin directly into
theoveractive
muscle.Despite
somany experiments
and researches has beendone concerning
SPD,
there are
still
many
un-answered questions,
and the
field for
investigations
and researches
in
SPDremains
widely
open.In
this
study,experiment
was conducted uponadductor
SPD patients, and
injection
of
Botulinum toxin
wasperformed using
percutaneustechnique
of
needle
in-sertion
into
the
thyroarytenoid
muscle.
Auditory
per-ceptual were done subjectively
by
the
patients
themselves
and objectively
by
the doctor.
Besides,acoustical analysis were
also
performed before
andafter
treatment,
to monitor
the results
as afollow
up mean.MATERIALS
AND
METHOD
This
study
wasconducted
in
the ResearchInstitute
of
Logopedics and Phoniatrics (RILP), Tokyo
Univer-sity,
from
1995
through
1996.
The
subjecrsfor
this
experiment
were 9 patientsof
adductor SPD, consistedof
2 males and 7 femaleswith
ages rangedfrom
20to
71 years,who
had beensuffering from
the diseasefor
more than six months. Thecontrol
group voice sampleswere obtained
from
15normal
speakersaged26 to
67 years. ThenormaVhealthy
voices were the modalvoice
samples
produced
atmost comfortable
level
andpitch
by
healthy
speakers,without
anyhistory of
pathology
affecting phonation.
BOTOX injection
were performed using
percutaneusprocedure, and
the
technique
is
identical
to
electromyography
of
the vocal folds.
A
23-gauge
hypodermic needle, coated
with Teflon
except
for
its
tip,
was usedboth
as amonopolar electrode
to
locate thevocal
folds
and as aninjection
channel. The needlewas inserted percutaneusly
through the crycothyroid
membrane,
andcorrect
positioning
of
the needle wasconfirmed
by
EMG
display
or
audiomonitoring
onphonation.
Voice
samplescollection
wereperformed
byrecording
sustained
vowel /a/
produced
by
subjects
aslong
asthey were
ableto,
attheir
most comfortable
level
andpitch.
SPD
voice
sampleswere obtained before
(pre-BOTOX)
and about
2
months
after (post-BOTOX)
BOTOX injection.
Recordings
were madeusing
DAT
tape-recorder,with
a constant distance
of
15 cm, betweenmicrophone
andVocal Assessmmt on
SPD
159mouth,
following
repeated
patient's
practice,
andrecordings
were madein
sound attenuated room.Voice
samplesof
sustained
vowel
lal
were
then digitalized
through
a16-bit
A/D
converter
at asampling
rateof
40kHz
and storedon
adisk controlled
by
computer. The
acoustic
feature
of
avoice
sample was analyzedusing
the
"SONG"
computer
aidedprogram.
Using waveform
matching
andpeak
picking
method,
the method proposed
by
Imaizumi
et al,8'elocal
maxi-mum points which could
correspond
to vocal
excita-tion
epochswere detected successively
andthen
two
time
seriesof
Fo(i)
andA(i),
thefundamental
frequen-cy
andthe
maximum
amplitude
of i-th
glottal
period
were
determined.
Cycle-by-cycle
perturbation
quotient were
calculated,
pitch perturbation
quotient
(PPO
andamplitude perturbation quotient
(APQ)
andseveral
voice properties were extracted such
as
theoverall
variability
of Fo(FoV),
theadditive
noiselevel
(Noise Level),
and
the energy
of
slow and fast
Fo
perturbations (FoS
andFoF).
Two
kinds
of
scoring were applied to
assess thevoice
condition
auditorily:
appraisement
by
the
patients
themselves depending on
their
feeling,
called
as"sub-jective scaling".
The
scores rangedbetween
0(for
nocomplaints
on phonation,
no difficulty,
smooth,
thevoice
seemedregular
andnot disruptive), up to
3
[for
difficult
feeling
onphonation, straining,
and no changecompared
to before injection (pre-BOTOX)1.
In
be-tween there were better
conditions
of
voices, score
1(much better
thanbefore
injection)
and2 (better
thanbefore).
The
"perceptual
objective
scaling" was a
scoring
method performed
by
thedoctor using 25
morae.The
score
dependsupon how many
morae
could
be
well
pronounced by the patients. Scaling ranged between25
for
bad
condition with no mora
pronounced
clearly,
smoothly, regularly
andwithout voice
stops,
up to
0for
normal condition, the whole
25
morae
were
pronounced smoothly, effortless and
without
voice
stops.
For
statistical calculation,
an
analysis
of
variance
(ANOVA) with
onefactor,
thegroup,
wasperformed
to determined significance.
REST]LTS
The
acousticfeature
of
avoice
sample analyzedusing
160 Abdoetachman Med J Indones
a)
b)
[image:3.595.64.549.87.471.2]c)
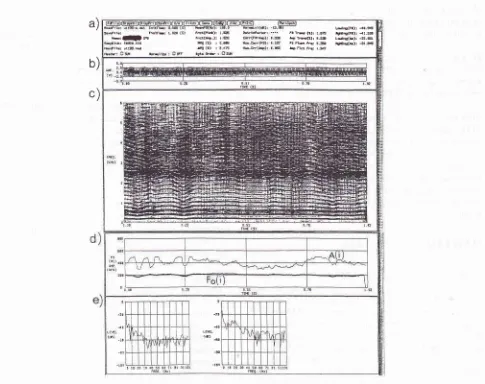
Figure 1. The acoustic feature of avoice sample analyzedby "SONG" computer-aided program. a) display of analysis condirtons
and results, b) the voice waveform, c) the sound spectogram, d) Fo and amplinàe fime series calculated using the acoustic analysis, e) the power spectrum of Fo (i) and A (i).
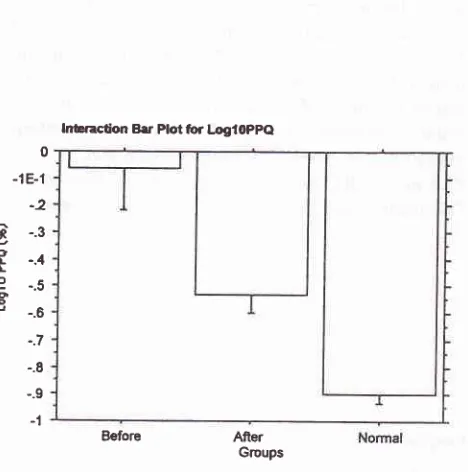
The bar
plot of
theLog10 pitch
perturbation quotient
(PPO
for
the
whole
groups was showed
in figure
2.The
mean
value
of
PPQ before
injection
was
-0.061(SD 0.713).
This
meanvalue
was decreasedto
-0.533(SD. 0.331) after injection,
but
the normal
control
group
hadthe lowest
meanvalue (-0.897, SD
0.246).Statistical
analysis showed thatpost-BOTOX
injection
the PPQ was
decreasedsignificantly
(P<0.0001),
but
still
higher
comparedto normal
voices.The bar
plot
of
Log10
amplitude perturbation quotient
(APQ), for
the
whole
groups was
showedin figure
3.After injection,
theAPQ
(mean value 0.379, SD0.379)
was
unsignificantly
decreased(P>0.005)
comparedto
before
injection
(meanvalue 0.401, SD 0.374).
How-ever, compared to the
normal control
(mean 0.142, SD0.246)
thedifference
is significant
(P<0.0001).
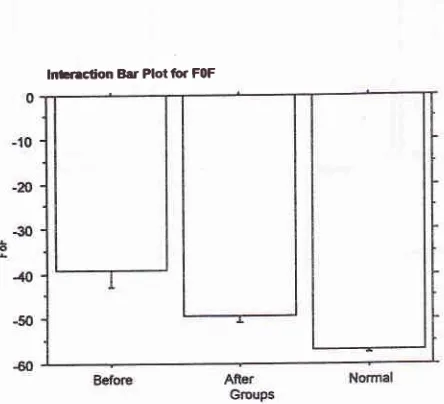
Figure 4
showedthe
barplot
of
theoverall
variability
of
Fo(FoV),
indicating
that after
injection of BOTOX
the
FoV
(meanvalue 2.839, SD 5.685)
was decreasedsignificantly (P<0.0001)
compared tobefore
injection
(mean
valuel9.870,
SD 25.878),
but
still
larger
com-pared to
normal voices
(mean0.830,
SD0.467).
Figure
5 showedthe
barplot of
the energyof
slow
Foperturbation
(F6S),revealing
the significant
decrease(P<0.0001)
in
the
strength
of
FoS
on post-BOTOX
injection
(mean
vahte
-42.560;
SD
8.772)
comparedto
pre-BOTOX injection (mean
valte
-32.200,
SD 16.775),but
still
stronger compared
to normal
group
(mean
-46.503,
SD4.393).
tr.rb: r.D2r (s) fd(tb): L.s
u.l!o Éd(h-): r s
.ld: 3!@0 ole Q G) : | 6c
q(F.): rr.s Filtu (t: I fi EECo): {t.st! h rdc): r.s r4-r: -È.Gr rr frd Fn: t.s É(Lr: -tl æ rr.: utre h.d 4 G) : 2:E
-2û
n ct c
L
o o
o
Vol 6, No 3, JuIy - September 1997
0 -1E-1
-2
-.3 -.4 -.5 -.6 -.7 -.8 -.9
-l
Before
AfierGroups
30
25
20
srs
o10
5
[image:4.595.52.532.75.761.2]0
Figure 4. The bar plot of the overall variability of Fo
for
the whole groups.Vocal Assessment on SPD 161
Before
AfrerGroups
[image:4.595.300.532.78.672.2]Figure 3. The bar plot of Log
l0
APQfor the whole groups. Figure 2. The bar plot oflng
10 pitch perturbarton quotient(PPQ)for the whole groups.
0
-5
-10 -15
-20 -25
U'o
^
-30 -3510
-45
-50
(FoV)
Before
AfierGroups
Figure 5. The bar plot of the energy
of
Slow Fo perturbarton(FoS)
for
the whole groups.lnÈraclion B.r Plotfior LogloPpQ lnEraclion Bar Plot for LogloAFA
lnEraction Bar Plot tor FOV lrbnrclion Bar Plot for FltS
[image:4.595.38.272.93.329.2] [image:4.595.303.533.94.341.2]162
AbdoenaclvnanFigure
6
showedthe
bar plot
of
theenergy of fast
Foperturbations (FqF).The mean FoF
value
of
pre-BOTOX injection
was-39.140
(SD
17.674).This
was-49.171(SD
7.062)
in post-BOTOX,
and-56.689 (SD
4.667)
in
normal control indicating
the
significant
decrease(P<0.0001)
in
the strengthofenergy
onpost-BOTOX injection, but were still
stronger comparedto
normal group.
Figure
7 and 8 showed theauditory perceptual
assess-ments
performed by
the patients themselves (termed asFigure 6. The bar plot of the energy offast Fç perturbation (F"F)
for
the whole groups.Figure 7. The bar plot ofperceptual "Subjective scaling"
of
voice condition performed by male andfemalz SPD patientsthernselves, before and after BOTOX injection.
Med J Indones
the "subjective perceptual scaling")
andby
thedoctor
(termed
as " objecti veperceptual
s c alin g ").
Statistical-ly,
the
scores
on
post-BOTOX injection were
sig-nificantly
decreased
(P<0.0001) compared
to
the scoreson pre-BOTOX injection. Moreover, the
cor-relation between
"subjective"
and"objective scaling"
using Pearson's
95Voconfident interval
was9IVo,
in-dicating
that there was a strongcorrelation
between the"subjective"
andthe "objective" perceptual scaling.
Figure 8. The bar plot ofperceptual "Objective scaling"
of
voice condirton performed by the doctor on male andfemaleSPD patients, before and after BOTOX injection.
DISCUSSION
Injection of Botulinum Toxin (BOTOX)
is directed to
make a temporary
paralysis or paresis
of
the
thyro-arytenoid muscle. The paralysis
will
decrease
themuscular
spasm
that
causes uncontrolled
muscular
contraction
onphonation,
andresulted in better
condi-tion
for vibration. The situation
wasclearly
seenin
thecompared
results
of
analyzed
voice samples
of
pre-BOTOX
versuspost-BOTOX injections,
by
assessingthe voice conditions acoustically and
perceptually.
Temporary satisfactory results
wereobtained after
the averageof
2months,
and lastedfor
at least 5months.
E
e.f*
û
nnoE
sdo*E
,cûoVol 6, No 3, July - September 1997
From
the results obtained,
it
can
be
seenthat
all
theparameters
of
voice
perturbations extracted
e.g.:
thepitch perturbation quotient,
theamplitude perturbation
quotient,
t
riability of
Fo,slow
pertu
and the energybation
of
a
decrease
in
voices,
indicating
that post-BOTOX
patients hadbetter
Fo control
compared
to
Pre-Botox
patients, and
thevoices were
lessfluctuating
andmore
stable.In
other
words,
post-BOTOX
patients had better vocalcontrol-lability
thanpre-BOTOX.
Theresults
werein
accord-ance to other
experts' reports
e.g.Zwimer
et a1.,10 andWoodson
et
al.+ They found similar
tendencies
onpost-BOTOX condirion,
although
they did not
com-pare
with Normal
speakers.The APQ was
not
significantly
decreasedon
post-BOTOX,
this
phenomenon was
probably
due to
several reasons:
the SPD
subjects
were mostly
con-sisted
of
female patients (7 out
of
9 speakers), and thefemale patients have a
tendency
to
produce
higher
frequency
andintensity
on sustainedvowel phonation.
This condition
will
be
resulting
in
reducedperturba-tions.
Although
Post-BOTOX
patients regainedtheir
voices,but
compared
to
normal
speakers,their
voices
havelarger perturbations.
Subjective
feeling
andperceptual
assessmentsof
SpD
voices
which
were performed both
by
the
patients themselves as"subjective scaling"
and by the doctor as"objective scaling",
showed that on
post-BOTOX
thevoice conditions
werebetter
and the scaling decreasedsignificantly. Correlation calculation
(pearson,s)
be-tween those
2
scalings showed strong correlation
(=0.906),
suggestedthat those
two
assessments wereparallel.
CONCLUSION
1.
Post-BOTOX voice
samples showed a decreasein
Fo
perturbations, suggested that post-BOTOX
group
hadbetter vocal
controllability
comparedto
pre-BOTOX
group.2.
Although
post-BOTOX group
regained their
voices,
their perturbations
werehigher
thannormal
voices,
indicating
that
compared tonormal
voicesthe
vocal
controllability
is lower.
3.
The "subjective
scale" and
"objective
scale', weredecreased
significantly
on
post-BOTOX
group,
VocalAssessment on
SPD
163and the
two
scoring scales werestrongly correlated.
This
suggestedthat
not only acoustically
the
postBOTOX
group
wasimproved,
but perceptually
aswell.
Acknowledgment
This
study was conducted
in
cooperation
with
theResearch
Institute
ofLogopedics
andphoniatrics,
Fac.of
Medicine,
University
ofTokyo andthe
authorwould
like
to
expresshis gratitude
andthanks
for
the
super-vision
given by Prof.
S. Niimi,Asc.
prof. S.Imaizumi
and
M.
Kumada
MD.
RET'ERENCES
l.
Broniatowski
M,
DaviesCR,
JacobsGB,
Grundfest-Broniatowski S, Nose Y, Tucker HM. Electronic control
of
laryngeal spsm. Blockage of orthodromically induced action potentials in intact canine reccurent laryngeal newe. Laryn-goscope 1990; 100(8):892-5.2. Netterville JL, Stone RE, Rainey C,Zæ,alear DL, Ossoff RH. Reccurent laryngeal nerve awlsion for treatment of spastic dysphonia. Ann Otol Rhinol Laryngol
l99l;100(l):104.
3.
Woo
P.
Carbondioxide
laser-assisted thyroarytenoidmyomectomy. Lasers in Surgery
&
Medicine 1990;10(5): 438-43.4. Woodson GE. Effects of botulinum toxin therapy in patients with adductor spasmodic dysphonia: acoustic, aerodynamic, and videoendoscopic findings. Laryngoscop e 1992;lO2(4): 400-6.
5. Adams SG, Flunt
EI, Charles
DA,
LangAE.
Unilateral versus bilateral botulinumtoxin
injectionsin spasmodic
dysphonia: acoustic and perceptual results. J Otolaryngol 1993;22(3):17l-5.6. Green DC, Berke GS, Ward pH, Genatt BR. point-touch technique of botulinum toxin injection for the treatment
of
spasmodic dysphonia.Ann Otol
RhinolLaryngol
1992;l0l(l
l):883-7.7. Kobayashi
T, Niimi
S, KumadaM,
KosakiH,
Hirose H. dysphonia. Acta8. Imaizumi S, Gauffin J. Acoustical perceptual characteristics of Pathological Voices: rough, creak, fry, and diplophonia. Ann Bull RILP t99l;25:109-19.
9. Imaizumi S, Abdoenachman H,
Niimi
S, Shimuray,
Saida H. Evaluation ofvocal controllability by an object_orientedacoustic analysis system.
J
Acoust
Soc
Jpn
(E)
1994;15(2):l13-16.