70 Ichihashi et al Med J Indones
Clinical
and
epidemiological
study of skin cancer
in
Japan
Masamitsu
lchihashil,
MasatoUedal,
Tooru Naganol, Keishi
Arakil,
Yoshii'uki
Ohno2, Santoso Cornain3Abstrak
Untuk menentukan prevalansi dan insidensi kanker kulit dan lesi prekan.ker (actinic keratcsis) ,7ar! populasi Jepang, l(ami meinulai pemeril<saan kanker kuLit
di
Kota Kasai (340 56' LU) dan Pulau Ie (250I0'
LU), pada tahuni992
-1993. Radiasi sinar mataliari pertahun di Pulau Ie diharapkan yang tertinggidi
Jepang. Pcda makalah ini, kami akan mempresentasikan hasil penelitian kanker kulit baik di Kota Kasai maupun di Pulau Ie, masing-masing sejak 1992 sampai 1997 dan sejak 1993 sampai 1997.Di
Kota Kasai, ditemukan 128 kasus keratosis aktinik (KA), 3 kasus lcarsinoma sel basal (KSB), danI
kasus karsinoma sel skuamosa (KSS), yang diidentifikasi secara klinik dan histopatologik. Sedangkandi
Pulau Ie, ditemuknn 130 kasusKA, 9
kasus KSB dan2
kasus KSS. Prevalansi KA per 10A.000 penduduk pertahundi
Kota Kasai pada tahun 1992-1997 adalah masing-masing413,4, 291,2,
203,7,86,8
123,1 dan 101,8. Walaupun demikian, jumlah KA di Pulau Ie pada tahun 1993-1997 adalah masing-masing 1.159,4, 572,8,l.A14,3,988,9dan6I2,5.Angka-angkadiPulaulesecarabermaknalebihtinggidariangka-angkndiKotaKasai. RasioOddsyang disesuaikan terhadap umur setiap tahun untuk KA adalah masing-masing 2,79, 1,38, 2,45, 2,39 dan 2,01. Nilai rata-rata prevalansi kanker kulit non melanoma (KKNM KSB dan KSS) di Pulau Ie pada periode penelitian adalah 50,0 untuk pria dan wanita. Total knsus KSB dan KSS di Kota Kasai pada tahun 1992-1997 adalah masing-masing
I
dan 3, jumlah yang terlalu kecil untuk dapa! menghitung prevalansi dan insidensi KKNM. penderita dengan keratosis seboroik (KS) diatas6
menunjukkan prevalansi yanglebih
tinggi daripada penderitalain
dengan KS dibawah 5. Hasilini
menindikasikan adanya relasi inversi yanghnt antara prevalansi dan
insidensi prakanker dengangaris
lintang pada nopulasi Jepang. Prevalansi KKNMdi
PulauIe
yang sama tingginya dengan prevaiansi patla orang Jepang yang tinggaldi
Hawai menunjuklcan insidensi KKNM yang lebih tinggidi
bagian Utara Jepang,dimana ladar ozon akan sangat berkurang di masa yang akan datang. Kulit tipe I dan penderita dengan KS ganda diduga sebagai faktor risiko kanker kulit pada populasi Jepang.
Abstract
In order to determine the prevalence and incidence of skin cancer, and pre-cancer lesions (actinic keratcsis) of Japanese we started skin cancer examination
it
Kasai City 640'56' N) and Ie Island Q50rc'
N)in 1992
and 1993, respectively. Annual solar radiation in Ie island is expected to be highest in Japan. Here, we will present the results of skin cancer examination in both Kasai City and Ie Island during 1992 through 1997, andduring
1993 through 1997, respectively. In Kasai City, a totalof
128 aclinic keratosis(AK),
3of
basal cell carcinoma (BCC) and one of squamous cell carcinoma (SCC) were identified clinically and histopathologically. While, a total of 130 AK, 9 of BCC and 2 of SCC were identified in Ie Island. The annual prevalence of AK per 100,000 population in Kasaicirydurtng1992through1997were413.4,291.2,203.7,86.8,
123.1and
l0L8
respectively.However,thoseofAKinIeIslandduring1993throughl99T
were 1,159.4,572.8, 1,014.3,988.9 and612.5 respectively.Thesevaluesweresignificantlyhigherthan those of KasaiCity.
The annual age-adjusted odds ratiosfor
AK was 2.79, 1.38, 2,45,
2.39 and 2.01 respectively. The mean prevalence. of non-melanoma skin cancer (NMSC BCC and SCC) in Ie island during studypeiod was
50.0for
men and women, Thelotal
cases of BCC and SCC in Kasai Ciry during 1992 through 1997 were 3 andI
respectively, too small to calculate prevalence and incidence of NMSC. Subjects with seborrheic keratosis (SK) over 6 showed a higher prevalence of AK than those with sebonheic keratosis wtder 5. These results indicate a sftong inverse relationship benveen prevalence and incidence of pre-cancer and latitude among Japanese. Further, NMSC prevalence in Ie Island is as high as that of Japanese who livein
Hawaii,
suggesting a higher incidence of NMSC of Japanese evenin
the northem part of Japan when ozone severely decreasedin
thefuture.
Skin typeI
and subjects with multiple (SK) were suggested to be riskfactorsfor
skin cancer of Japanese.Keywords: non-melanoma skin cancer, actinic keratosis, epidemiology, ultraviolet light, riskfactor.
A
large body
of
evidence
has been
accumulatedsupporting
arole of
sunlight
to
induce skin
cancerin
I Department of Dermatology, Kobe University Schoot
of
Medicine, Kobe 650-0017, Japan
2 Department of Preventive Medicine, Nagoya Universitl,
Sc hool of M edicine, N agoya 466-85 50, J apan
t
Department of Anatomic Pathology, Faculty of Medicine, University of Indonesia, .lakarta 10430, lndonesiaEpidemiology
of
skin cancer in Japan 71 Vot 9, No 2, APril-
June 2000descriPtive s
including
inCividuals
n-melanoma
skin
cancerto
latitude
in
PoPulationskinned
PeoPIeborn
in
orre
i0 Years
of
age haveSC and melanoma
than.
er
10
Years
of
age
toAustralia
from Europe,
suggesting a role,of
exposure;-ririn;
childhood
in
tÈin
cancer
development'Another important
evidence isthat skin
cancer occursmainly
atsun-expos"J*"ut of
theskin
andin
peoplewho
burrr
eashigher Yield
of
(XP) Patients
develoP
manYcancers
confined
io
sun-exof
the
atmosPheric ozoneof
harmful
UVB flux
ani;";i:i'îhit
-uy i"
tu'n
resultsin
an increasein
skincancers ancl
precancerous
lesions
on
sun-exposed6
SKIN.
Epidemiclogical studies
on
skin
cancer'
however'
were primarily
conducted
to
elucidate
the
incidencerate
in
light-skinneJ
Caucasians'
To
our knowledge'
ttt"r" it
n"od"tuit"d
report aboutskin cancer incidence
or prevalenc"
on
'un-!*posed
areatn
t:lun
including
Japanese,
except
diseâse
rate'
or
incidence
ratecalculated
from
mortality
rate
or
incomplete
ieglst ation, since sunlight was
not
evaluated
as
a*i.jo,
"uut"
of
skin
cancerof
Japanese'rada
and
MikiT ,tn*11,"îT,"îi,1di
;"::",i;
:i
epidemiological
studYsurveYed
bY
a
larseâ".*urofogy
clinics
"of
university
hospitals
in
Japan'Tada
andMiki
showedan apparent increase
in
basalcell
carcinoma
(BCC) in
comparison
with
squamouscell carcinoma
(SCC)'First,
we
conducted
aNMSC
and Precanceroin
JaPanese, bY analYzidermatologY
dePartmen"tn;;;"t"'tn"
àu.1"ttlut
of
the study wasto elucidate
a reliable skin
cancer frequency
in
Japaneseand
to.r"t#y
,i"
ir"na
*
skin cancer
frequency
overthe last
two decades. Next, we
have.conducted
a
screenlngilt tti"
cancer
in
Kasai
Cityro-rr
which
is
located almost at the centerof
Japan at :+0 SO'N'
since 1992'
anci
in Ie
Island, Okinawï
Prefecture'r2
located at 250îô:N,
tin""
1993.We
determined the prevalence rateài
NftrsC
andactinic keratosis
(AK)
of
Japaneseby
healthexamination.Participantsinre€ionalhealth
examinationwereseenbydermatologrsts.Final
;"s;;
il
;as
made hi stop ath olo s"i"^]ll
.l1'l':
:lont'
*"i"
utto interviewed by
meansof
a questtonnalre'MATERIALS
AND METHODS
SurveY
on disease
rate
The
hospital records
of
the patients
with BCC'
SCC;;;
p;":"*cer
lesion,
Ad
were
analyzed
in
2'l
iniu"i*irv
hospitals
in
Japan'The
age and.sex
of
thep"i"".
âna
,it"
of
tf'"
tu*ot
were collected
in each
disease
for the
1976-80
and
1980-90
intervals'
For
comparaiive "uutuution
of
disease ratein two
periods'
age:
and
sex-standardized
disease ratcs
werecalculated
for each
ï;;il"t-"i
by.di'""'
method'
!
"ti"î-itt"
smndardsfor
poputatlons
1976-80 and
in
for
1979
1986-90' respectively'
and
1989
as
theThe
analysesw"re aslotlows:
the disease ratein
each,ni"".tity
hospitals
basedon the total number
of
out-pu,i"n,,'during
each period:
the
disease
rate
per 100,000population
ualot'"0
for
age-and
sex
during
"""t
p"t.O,
and
the iate
of
BCC'
SCC
and
AK
in
northËrn and southern parts of Japan'
Skin
cancer examination
at
Kasai
City
and
Ie
Island
ions
iii
and
rf the aged. Residents
agedV0
and over were registered
undei
the
Health
Science'sLaw for
the
Agedl [uestionnaires
asking information
on
name,
ug",
'"*,iddress'
telephone
number'
skintype,
useof
cosmetics and sunscreenon sun-exposed
skin,
occupationai-sun exposure
(oltdoor
or
indoor)'
acute
sunbu-t
'à;;;g
ihildhood'
smoking
habit'
location
of
uny-
'tii
tumors'
past history
andfor
cutaneousdisorders'
Skin
types
were-d from
I
to
III'
based
on the criteria of
72
lchihashi et alParticipants were examined
for skin cancers and
pre-cancer lesions
(AK) on the
face, neck, extensor
surfaceof the
forearms
andback
of the hands, and for
benign
tumor
(seborrheic keratosis:
SK)
on the
face.Age- and sex-standardized
prevalence and
incidencerates
for
AK
weie
calculated
by
the direct
method,using
theJapar,eselopulation
in 1990
as the standard.The
incidence
of
AK
wascalculated
for
people who
had participated
in
the
screening
consecutively for
two years
in
K.asaiCity from 1992 through
1997,
andin Ie
Island
from
1993
through 1997, respectively.
Sex-and age-specific p\evalence and incidences
werecalculated
with
SAS cbmputer program
(PC-SAS,
1987).
The
differences
in
AK
prevalence
and incidence
among people having different
skirr types,
occupational
exposure, cosmeticor
sunscreen use, andsevere acute
sunburn
atchildhood
andbeing
a smokeror
non-smoker, were
estimatedby
the chi-square
test.Numbers
of
SK on the face
were
counted
andclassified
into
two
groups:
subjectshaving
6 or more
SK
or subjects
having
5
or
less.
The
statistical
significance
of
SK
in
relevance
to
AK
was also
analyzedby
the chi-square-test.RF,ST]LTS
Disease
rate of
SCC,
BCC
and
AK
The disease rates
of SCC,
BCC and
AK
in
university
hospitals
of
Japan showed
an
increasing
trend with
'decreasing latitude, except
in
Sapporo
and were
higher
in 1986-90 than in 1976-80.
The
ratesot BCC
and AK were
significantly
(<0.001) higher
in 1986-90
than in
1976-80,
whereas
there was
no
significant
difference
of
SCC rate
between
two
terms.
No
significant differences
v/ere
seenfor
skin tumors of
unexposed
body
sites.When
thehospitals
weredivided into
those inlocation
more
than
and less than
350N, the
rates
of all three
types
of
skin tumors
were
higher
in
hospitals
in
thesouth than
in
the
north of
35oN. Significantly
higher
rates
of
BCC
and
AK
were
again
found
in
1986-90than
in
1976-80
in both
locations,
while
that
of SCC
was not significantly lower
in
the later period.
The
rates of all
three
typesof
skin tumors were
five times
higher
in
the Kyushu area (Kurume, Nagasaki
andMiyazaki)
in
the
southern
part of Japan
than
in
thenorthem Tohoku area
(Hirosaki, Sendai
andFukushima).
Med J Indones
Prevalence
and Incidence of
AK
in Kasai City and
in Ie Island
The number
of
participants were approximately 4,500
in Kasai City and
about
1,000on
Ie
Island every
yearthroughout
the studyperiod.
Ages
of the
participants
ranged between 20 and
97
years olci inKasai
City and
between20
and
101 yearsold
on
Ie
Island.
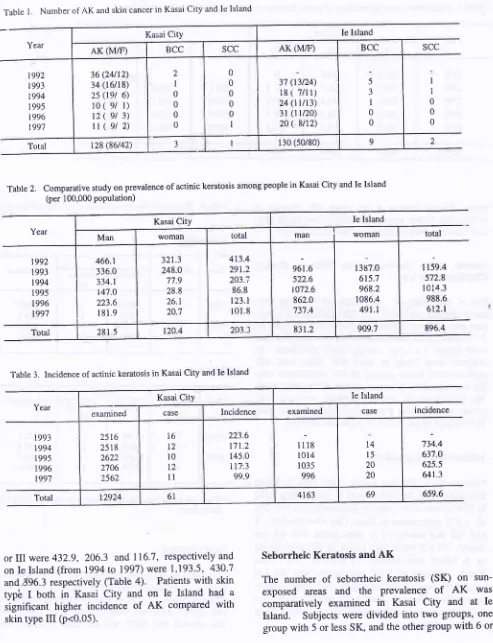
A
total of
128 casesof
AK
(86
males,
42
females),
3 BCC (all
male) and
I
SCC
(a
male) were
identified
histo-pathologically in
Kasai
City during
the
6
year period
from
1992
through
1997
(Table
l).
On Ie Island,
atotal
of
130
cases ofAK
(50
males,
80 females),
9BCC
and
2 SCC
were diagnosed histopathologicaliy
from
1993
through
1997
(Iable
l).
No melanomas
were detected
in both locations
during the study.
The
total number
of AK fcr each
year
in bcth
locations
is alsolisted in Table
l.
The prevalenceof AK in Kasai
City
19928
was found
to
be
413.4
per
100,000population, the highest
..'alue
obtained during
thestudy so far, and decreased to
86.8 (the
lowest
value)
in 1995.
The
prevalenceof AK for
men
in
Kasai
City
was
significantly higher than
in
women each
yearihroughoui the sturiy period.
Whereas,
on
Ie
Island
there
was
no
significant difference between
theprevalence
of
AK
in
rnen and
in
women, The mean
prevalence
of AK
per 100,000
population,
calculated
from
thetotal number
of AK in
Kasai
City
from
1992to
1997
and
on [e lsland
from
1993
to
1997
were
203.33 (281.55
for
malcs, 120.5
for
females)
and841.8 (831.2
for
males,
909.7
for
female)
respectively (Table
2).
The mean
AK
prevalence
onIe
Islând was
about4
times higher than that
of Kasai
city
(Table
2). The meanincidence of
AK per 100,000
Japanese residents
was
148,2 inKasai
City and 659.6
on IeIsland, respectively (Table
3).Comparison
of
AK
prevalence
between
Kasai City
and Ie
Island
To
estimate the a,ssociation between theprevalence
of
AK
in
Kasai City
and
that of
on Ie Island, the
age-adjust odds ratio
(ORs)
during
the study
period (1993
-
1997) werecalculated.
ORs
in
1993,
1994,
1995,
1996,
and
1997were2.79, 1.38,
2.45, 2.39
and2.01, respectively.
Skin
type
and
AK in Kasai City
and
Ie Island
Year
Kasai City Ie Island
AK (M/F) BCC SCC AK (MÆ) BCC SCC
1992 1993
t994
1995 1996
199'7
36 (24n2) 34 (16/18) 2s
(t9t
6)lo
( 9/
r)t2(
91 3)|(9t2)
2 I 0 0 0 0
0 0 0 0 0 I
3't (t3124)
l8
(
7/l r)24
(tvt3)
31(tU20)
20( 8tr2)
5 3 I
0 0
I I 0 0 0
Total t28 (86142) 3 I 130 (so/80) 9 2
VoI9, No 2,
APril-
June 2000Table
l.
Number of AK and skin cancer in Kasai City and lc IslandTable
2.
Comparative study on prevalence of actinic keratosis among people in Kasai City and Ie Island (per 100,000 PoPulation)Table
3.
Incidence of actinic keratosis in Kasai City and Ie Islandor III
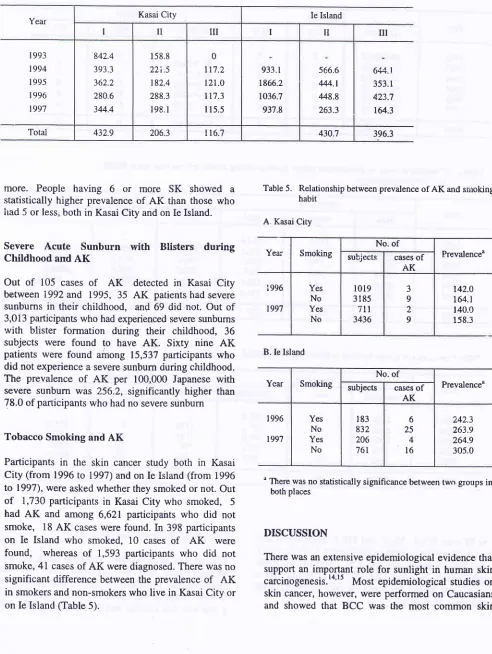
were 432.9, 206.3 and I
l6'7,
respectively
andon Ie
Island (from
1994to
1997)were
1,193.5,
430.7and696.3 respectively (Table
4).
Patientswith
skin
typê
I
both
in
Kasai
City
and
on
Ie
Island had
asignificant higher incidence
of AK
compared with
skin
typeIII
(p<0.05).
Epidemiology of skin cancer in Japan '13
Seborrheic
Keratosis
and
AK
The
number
of
seborrheic keratosis
(SK)
on
sun-exposed areas
and the
prevalence
of
AK
wascomparatively examined
in
Kasai
City
and
at
IeIsland.
Subjects were
divided into two
groups,
one groupwith
5or
lessSK,
and the othergroup with
6 orYear
Kasai City Ie lsland
Man woman total man woman total
t992
I 993 1994 1995
I 996 1997
466.r 336.0 334.1 r47.0 223.6
l8l
,9321.3 248.0 77.9 28.8 26.1 20.7
4t3.4 291.2
203.i
86.8 t23.1 101.8
96t.6 522.6 t072.6
862.0 737.4
l3 E7.0 615;1 968.2 1086.4 491.i
1159.4 572.8 1014.3
988.6 612.1
Total 281 5 120.4 203.3 83t.2 909.7 896.4
Year
Kasai City Ie Island
examined case Incidence examined case incidence
I 993
t994
I 995
1996 1997
25t6
25 l8 2622 2'106 256216
l2
l0
t21l
223.6
L7 r.2
145.0 tt7'.3 99.9
lllS
l0l4
1035 996t4
l5
20 20734.4 637.O 625.5 641.3
[image:4.554.33.526.56.699.2]Year Kasai City Ie Island
I II
III
I TilI
1993 1994
I 995
I 996 1997
842.4 393.3 362.2 280.6 344.4
158.8
22i.5 182.4 288.3 198, I
0 117.2 t2L.O
tt?.3
l15.5
933.1 1866.2 1036.7 937.8
566.6 444.1 ,148.8 263.3
644.t 353.1 423.7 t64.3
Total 432.9 206.3 116.7 430.7 396.3
74 Ichihashi et aI
Table
4.
Comparative study on incidence of actinic keratosis and skin type in Kasai City and Ie Islandmore.
People
having
6
or
more
SK
showed
astatistically
higher prevalence
of
AK
than those who
itad
5or
less,both
in
KasaiCity
and on IeIsland.
Severe
Acute Sunburn
with
Blisters
during
Childhood
and
AK
Out
of
105
cases
of AK
detected
in
Kasai
City
between
1992and 1995,
35
AK
patients had severesunburns
in
their
childhood,
and
69 did not. Out
of
3,013 pafticipants
who
had experienced severe sunbumswith
blister
formation
during
their
childhood,
36subjects
were
found
to
have
AK.
Sixty nine
AK
patients
were found among
15,537participants who
did not
experience a severe sunburnduring childhood.
The
prevalence
of AK
per
100,000
Japanesewith
severe
sunbum was
256.2,
significantly higher
than78.0 of participants who
had no severe sunburnTobacco Smoking
and
AK
Participants
in
the skin
cancer
study both
in
KasaiCity (from
1996to
1997) and on[e Island
(from
1996to
1997), were asked whether they smoked ornot. Out
of
1,730 participants
in
Kasai
City who smoked,
5had
AK
and among 6,621
participants
who
did
not
smoke,
18AK
cases werefound.
In
398 participants
on
Ie
lsland
who
smoked, 10
casesof AK
werefound,
whereas
of
1,593
participants who
did
not
smoke,
4l
casesof
AK
were diagnosed.There
was nosignificant
difference
betweenthe prevalence
of
AK
in
smokers and non-smokerswho
live in
KasaiCity or
on Ie
Island (Table
5).Med J Indones
Table
5.
Relationship between prevalence ofAK
and smoking habitA. Kasai City
B. Ie Island
n There was
no statistically significance between two groups in both places
DISCUSSION
There was an extensive
epidemiological evidence
that supportan
important role
for
sunlight
in
human skin
carcinogenesis.'*'tt Most epidemiological
studies
onskin
cancer,however, were performed
on
Caucasiansand
showed
that BCC was the most common
skin
Yea; Smoking subjectsNo.
of
casesof
Prevalence"AK
i996
t997
Yes No Yes No
l0l9
3185itt
3436
3 9 2 9
t42.0
t64.t
140.0 158.3
Ycar Smoking subjectsNo.
of
casesof
PrevalenceuAK
1996
1997
Yes No Yes No
183
832 206 761
6 25 4
l6
[image:5.566.58.550.91.745.2]Vol 9, No 2, APriI
-
June2N0
cancer
in
light-skinned
peopl'e.There
wasalso
strong evidencefor
therole
of
sunlight
in
SCC genesis'There was
little
information about the incidence of
NMSC
in
Japanese,since
Japanese,who
generally
haddarker skin
than Caucasians,were believed not to
develop skin
cancers on sull-exposed areas,but rather
to
devâlop skin
cancers
on
legs and other
coveredareas due to
burn
andX-ray radiation.
The
inciden'ceof
skin
cancer however, was
expectedto
have increased among Japanese, since the meanlife
Japanese
life-styles,
such asexposing
theskin
moreto
runtight
to
get
tanning
alsocontributed to
an increaseof
skin
cancer.To
determinewhether skin
cancers and pre-cancerousthan
in
1976-1980, andalso that
ratesof
BCC,
SCCancl
AK in
southem
parts-of
Japanwere
about
five
times
higher
than
in
northern
Japan. Similar
studiegtv
rtiiv"Ïiï?"iliqlo
to
1960 unouv
Tada andMikiT
fiom
1971
to
1975 provided additional information
about skin
cancer characteristics
in
Japan,but
thosestudies
did not report the
prevalence
or
incidence
of
skin
cancers
in
Japanese.
IARC
reports gave
anestimated
skin
cancer incidence
of
1'5-5'0
per
100,000
Japanesein
Saga,
Hiroshima, Osaka
andMiyagi,
bui
there
was
no
report showing a
reliable
registry
for
skin
cancerin
those areas.We tterefore initiated this
study
on
the incidence
of
skin
cancers and pre-cancerous lesionsin
Japanesein
Kasai
City
(populated
about
50,000 residents)
since1992,
anàon
tè
tsland
(located
in
the
far
south of
Japan) since 1993. The prevalence
of
AK
per
100,000 Japanesein Kasai
City
had decreased every year,from
+l+.1tn
1992to
86.8
in
1995.
The incidence
of
AK
Epidemiology of skin cancer in
Japan
75prevalence
or
incidence
of
skin
cancer
in
Kasai
City,
iince
the
number
of
skin
cancer patients \t/as
too
small.
Occupational exposure
to
the
sun
wassuggested
to
be
a causativefactor
of
AK
according
to
the prevalence andincidence
of
AK
in
Kasai
City,
which
showed
a
higher
ratio
in
people working
outdoors, compared
to
people
working
indoors'
However,
there
was
no
signtficant difference
in
theprevalence
of AK in
people
working
outdoors in
kasai
City
from
1995
to
1997 and
on Ie
Island
throughout the studY Period.
Skin type
I
subjectsof both Kasai City
and
Ie
Island
had
a
itatistically higher mean
prevalence
of
AK
during
the
study
period
compared
with
skin type
m
skin tumors (sebonheic keratosis
SK)
asearly
as oneyear
of
ageon
sun-exptlsed
sites,
such as
the
face, itre Uactsof
the hands and the extensor surfacesof
theforearms.
These observation onXP
patientsprompted
,
us
to
examine the relationship between
SK
anciAK'
îless SK.
Urback
et
alrs
forrnd
strong
associations
betweenBCC and
SCC
and
sunburn. Hunter
et
alte
also showedthat
risk
of
BCC
increasedwith a history of
sunburn.Further, Marks
et al20 showed thatchildhood
exposure
to
sunlight plays
a
significant
role
in
the developmentof
AK'
In
our
questionnaires,
we
askedwhether
the number
of AK in
Japanese correlatedwith
severe acute sunburns
during
childhood'
A
higher prevalence
of
AK
was observed among peoplewho had
severe
acute sunburns
during
childhood
compared
with
thosewithout
such severe sunburns'[n
out
lP
(type
A)
siblings, first
diagnosed at
4
and2
years
of age,
theelder
sister had herfirst
skin
cancerigCq
at13
yearsof
age, whereasthe younger
sister had herfirst
skin
cancer. (BCC)
at 23 yearsof
age'-'
rtant
role
lbr
sun-exPosurecarcinogenesis,
PossiblY bYof
skin
cancer develoPment76
lchihashi et alOur
results
thus indicate that people
who
worked
outdoors,
hadskin
type
I
andhave
6 or
more SKs
onsun-exposed areas,
were
at
high
risk
for
AK
andpossibly
for
NMSC. Further, protection
of
the
skin
from solar
UV
radiation since
childhood might
significantly
reduced the
risk
of
SK,
AK,
BCC
andSCC.
We
believe
that
these datamight contribute
tobetter
understandingof
therisk
andpreventive factors
of
sk-in cancersin
Indonesia.Acknowledgement
Parts
of
this work were
supportedby a Grant-in-Aid
from
the
Ministry of
Education,
Science,Culture
andSports
ofJapan, by the research fund
for
the effectsof
Ultraviolet Ray Influence
of
Human
Heaith from
theGlobal
Environmentai
Research,
Environmental
Agency,
and
by
a
grand
from Shinryokukai,
Kobe
University School
of
Medicine,
Japan.
Further,
this
work
is supported
in
part by a granttiom
the JapaneseCommittee
for
sunlight Protection,
Kycto,
Japan.We
are verygrateful
to Ms
Emiko
Miki
in
ts'asaiCity
and
Ms
Masako Namisato on
Ie
Island
for their
greathelp
in
the health
examinations
and
to
ivls Mariko
Hibi for editorial
assistance.REFERENCES
i.
UrbackF.
Man
and ultraviolet radiation.In:
PasschierWF,
BosnjakovicBFM,
editors. Human Exposure toUltraviolet Radiation Risk and Regulation. Amsterdam, New York, Oxford: Except Medical,1987: 3-16.
2.
RobbinsYH,
KraemerKH,
Lutzner MSA, Festoff BW, Coon HG. Xeroderma pigmentosum: An inherited diseasewith
sun sensitivity, multiple cutaneous neoplasms andabnormal DNA repair. Ann Inter Med, 1974; 8O:221-48.
3.
IchihashiM,
FujiwaraY.
Clinical
and photobiologicalcharacteristics
of
Japanese xeroderma pigmentosumvariant.
Br J Dermatol, 1981; 105: l-12.4.
YamamuraK,
IchihashiM, Hiramoto
T,
Ogoshi M,Nishioka
K,
FujiwaraY.
Clinical and photobiological characteristic of xeroderma pigmentosum complementation -group F: a review of cases from Japan. Br J Dermatol,1989;
l2l:471-80.
5.
DahlbackA,
HenriksenT,
LarsenSMH,
Stamnes K.Biological UV-doses and the effect
of
an ozone layerdepletion. Phctochem Photobiol, 1989; 49:. 621 -5.
6.
UrbackF,
Epstein JH, Forbes PD. Uliravioletcarcino-genesis:
experimental, global and genetic aspects. In: PathakMI,
Harber LC, SeijiM
et al,editors.
Sunlight and Man. Tokyo: Tokyo Univ. Press, 1974: 259-83.7.
Tada
M, Miki Y:
Malignant
skin
tumors
amongdeniratology patients
in
university hospitalsof
Japan.A
Med J Indones
statistical survey
l97l-1975.
J Dermatol, 1984; I 1: 313-21.8.
MiyajiT.
Skin cancersin Japan:
a nationwide 5-yearsurvey, 1956-1960. In:
NCI,
Conference on Biology of Coetaneous Cancer. National Cancer Institute Monograph,No.l0,
1963:55-70.9.
Suzuki T, UedaM,
OgataK, Horikoshi T, Munakata
N and ichihashiM
Dosesof
solar ultraviolet radiation correlate with skin cancer rates in Japan. Kobe J Med Sci,1996;42:375-88.
10.
NaruseK, Ueda
M, Nagano
T,
Suzuki T, Harada S,Imaizumi
K,
WatanabeS,
IchihashiM.
Prevalenceof
actinic keratosis in Japan. J Dermatol Sci, 1997; l5:183-7.I
l.
Suzuki T, UedaM,
NaruseK,
NaganoT,
Harada S,Imaizumi
K,
WatanabeS, Ichihashi M.
Prevalence ofactinic keratosis in Japan. J Dermatol Sci, 1997; 16:74-8.
12.
Nagano T, UedaM,
Suzuki T, NaruseK,
Nakamura T, Taguchi M, Araki K, Na-kagawaK,
NagaiH,
Hayashi K, WatanabeS,
IchihashiM.
Skin cancer screening in Okinawa, Japan. J. Derrnatol Sci, 1999;l9:
161--5.13.
SatohY,
KawadaA.
Action
spectrumfor melanin
pigmentation
to
ultraviolet
light,
and
Japanese skintyping.
In:
FitzpatrickTB, Wick MM,
TadaK
(eds).Brown Melanoderma: Biology and Disease of Epidermal Pigmentation. Tokyo: Tokyo Univ. Press, 1986: 87-95.
14.
Hunter DJ, Colditz GA, Stampfer MJ, Rosner B, WillettWC, Speizer
FE. Risk factors for basal cell carcirroma ina prospective cohort of women. Ann Epidemiol, 1990;
l:
t3-2?.15.
Elwood
JM,
GallagherRP,
Hill
GB,
Pearson JC.Cutaneous melanoma
in
relation
to
intermittent andconstant sun exposure-the Western Canada Melanoma Study. IntJ Cancer, 1985;35:.427.
16.
Siaper H, Velders GJM, Daniel IS, de Gruijl FR, van derLæun
IC.
Estimatesof
ozone depletion and skin cancer incidence to examine the Vienna Convsntion achievements.Nature, 1996; 384: 256-8.
17.
Kraemer KH, Lee MM, Scott J. Xeroderma pigmentosum: coetaneous, ocular and neurologic abnormalitiesin
830 published cases. Arch Dermatol, 1987; 123:- 241-50.18.
Urbach
F,
Rose
DB,
Bonnem
M.
Genetic
andenvironmental interactions
in
skin
carcinogenesis. In:Proceedings of the 24th Annual Symposium on Fundamental Cancer Research. Environmental Cancer. Baltimore,
MD(US):
Williams&
Wilkinsfor
University of Texas,Houston, 1972:355-7 1.
19.
-
Hunter DJ, Colditz GA, Stampfer MJ, Rosner B, WillettWC, Spiezer FE. Risk factors for basal cell carcinoma in a
prospective cohort
of
women. Ann Epidemiol, 1991;l:
t3-23.20.
Marks R, Jolley Dm, læctsas S and FoleyP.
The role ofchildhood exposure
to
sunlightin
the development ofsolar keratoses and non-melanocytic skin
cancer.
Med JAustralia, l99O; 152: 62-6.
21.
Kondoh M, UedaM,
NakagawaK,
Ichihashi M. Siblingswith xeroderma pigmentosum complemcntation group A
with different skin cancer development: importance cf sun