Clinical study of skin cancer 71 VoI 9, No 2, APril - June 2000
A clinical
study
on
skin
cancer
in
Indonesian patients
Mochrar Hamzahr, Masamitsu-Ichihashi2, Herman Ciptor, Evert DC Poetirays, Arman Mukhtai,
Yq"
Til*"ta
il."
il;|\4;r*
ù"a/,
Sanroso comaina, Setyawati Budiningsih5, Joedo Prihartono), Yoshiyuki ohno", Nobuo Munakata'Abstrak
Kelamin
adalahp59,4=l2,2tahun),KSSyangterdaP4t
]3(40,6tara24.85tahun(rata.rata57,8+15'5
I
I kasus
Ilmur mereka berkisar antara 30-80 tanai lokalisa erah
terp
atau tidak, tiidapatkan masing-masing; KSB 88 (96'7 Eù da.ri 9I (37,5 Vo)di
20 (62,5 tidak terpajan. bicntara MM J (27,3 Vo) pada daerah terpajan, 8daerahtida
KSBterh
h83:30=2'8:1'Abstract
I
2.8: I.
Keywords: Basal cell carcinoma, squamous cell carcinoma, skin typing
t
Deltartment of Dermatology, Faculty of Medicine, University of Indonesia, Jakarta 10430, Indonesia2 Department of Dermatology, Kobe University School of
Medicine, Kobe 650-0017, JaPan
t
Department of Surgery, Faculty of Medicine, University of o Indonesia, Jakarta 10430, Indonesia ine,cine,
6
Department of Preventive Medicine, Nagoya UniversitySchool of Medicine, Nagoya 466-8550' Japan
7
Radiobiology Division, National Cancer Center ResearchInstitute, Tolcvo 104-0045, Ja7an
Skin cancer especially non-melanoma
skin
cancer(NMSC) is the most common cancer in Indonesia, as well as in other places in the world.t The Indonesian National Center for Pathology-based Cancer Registry
in
1992 reported that skin cancer ranked the first inmales and the fourth in female.s'
The
markedrise
in
incidenceof
squmous cell carcinoma has been noticed in United Slates3'a and78
Hamzahwas due
to
both the increasing incidence and themortaliry.3'4
Solar ultraviolet exposure has been considered as the
important
factor
]or
tde
developmentof
non-melanoma skin cancer for quite a long time. Such an
effect has been also observed recently although the association might be more complex.
The development
of
squamous cell carcinoma has been implicated in a prospective studyT as well.Higher incidence
of
non-melanomaskin
cancers among white people has been reported to be related to the latitude closer to equator.sIt will
be interesting to study such relationship among Indonesian populationliving
at
and around
theequatorial belt.
A
case-control study was conductedin
1995 in Dr.Cipto
MangunkusumoNational Center
GeneralHospital (RSUPN-CM) Jakarta, as a
joint
research between Indonesia and Japan.The aim of this study is to find characteristics of the
various clinical aspects of each type of skin cancer in
Indonesian patients.
MATERIALS AND METHODS
All
casesof
skin cancer
were obtained from thepoliclinic of the Department of Dermatovenereoiogy
and
the
policlinic
of
Departmentof
Surgery, Oncology subdivision atDr.
Cipto MangunkusumoHospital, Jakarta. The study included parients who
came for consultation at both policlinics since January 1996 until March 1999. Age, sex, nationality, site,
duration of illness, type of tumor, size and localization
were recorded
from
each patient. patients were divided into sex and age group in decades. The sitesof
tumor were groupedinto
sun-exposed area, i.e.neck, hand and forearm and the non sunrexposed area,
i.e. trunk, soles, back and buttock.
RESULTS
In this study, we evaluated 139 skin cancer cases. The
most frequent skin cancer was BCC (91 cases, 65.5
Vo) and SCC was the second (32 cases, 23.0 Vo). We
saw I
I
(7 .9 Vo) cases of malignant melanoma, 2 casesof
lentigo maligna (precursorto
MM),
I
solar keratosis (precursorof
SCC), basosquamous cellMed J Indones
carcinoma and Bowen's disease (precursor
of
SCC),respecLively.
Among the
9l
BCC cases,53 (58.ZEo) were ferrralesand 38 (41.8 Vo) were males. The age ranged from 32 to 87 years old (mean = 59.4 + l2.Z yrs). See Table
l.
The
most
frequentsite
affectedwas the
face,especialiy the cheek and the nose. The total number of
SCC was 32 cases, consisting
of
l3
females (40.6 Vo)and 19 rnales (59.4 Vo).The age ranged between 24 -85 years old (mean = 57.8 + 15.5 yrs).
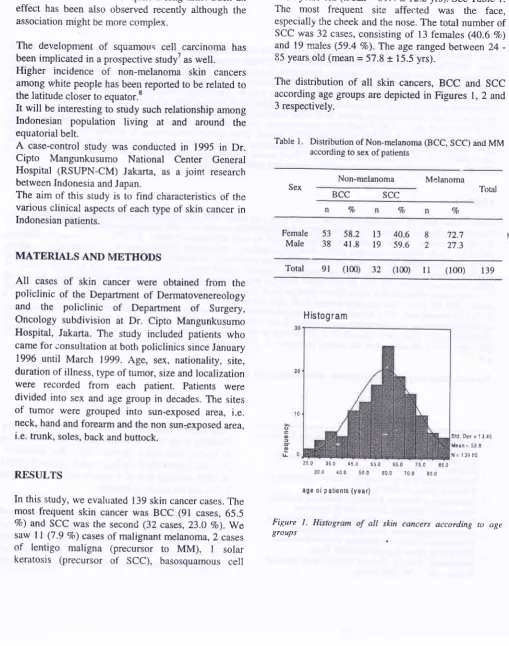
The distribution
of
all skin
cancers, BCC and SCCaccording age groups are depicted in Figures 1,2 and
3 respectively.
Table
l.
Distribution of Non-melanoma (BCC, SCC) and MM according to sex of patientsNon-melanoma Melanoma
Sex Total
BCC scc
%
Vo %
Female
Male 40.659.6
I
72.7
2
27.353
58.2
1338
41.8
19Total
9t
(100)32
(100) I I (lo0) t39Sli DEy=1345 Mear,, 55 6
,,1: 138 Ci
250 350 45C
3ro 100 50n
55C ê50 75C
6C0 7c0 Eôû 050
age oi p atienrs (year)
Figure
l.
Hisbgram of alt skin cancers according ro age SrouPs [image:2.595.57.567.157.803.2]H istogram
VoI9, No 2' APril - June 2000
300 {00
3s.c 45 t
Clinical study of skin cancer
c a t
u
[image:3.595.68.301.63.585.2]age ol patients (Y€ar)
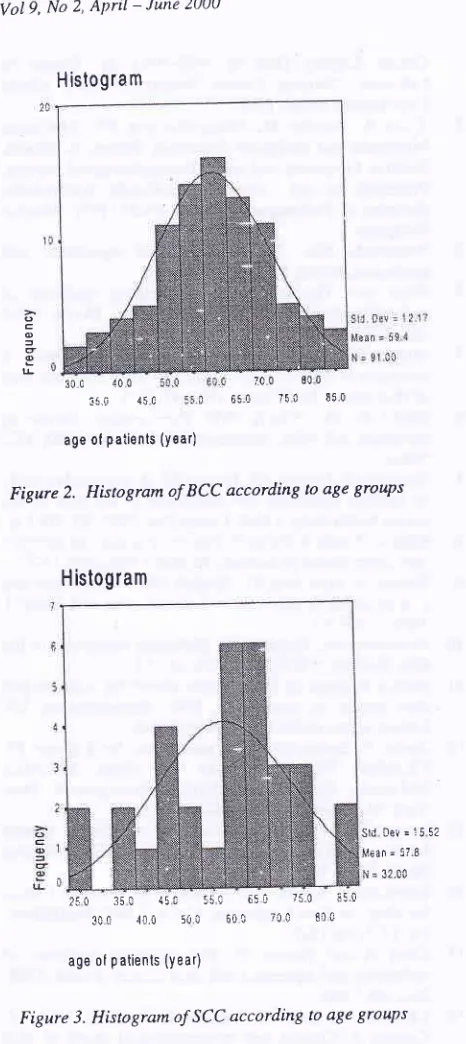
Figure 2. Histogram ofBCC according ro age SrouPs
BCC 0.5 cm - 10 cm (mean
-
7.0 cm) for SCC 5 ci-n -10 cm (mean = 7.5 cm) while for MM the lesion wasI
om- 5 cm (mean-
3 cm).The most frequent site of BCC was cheek (29'7 7o),
followed by nose (26.4 Vo) and forehead (8.8 7o)' For
SCC the most frequent site affected was
foot
(21'97o).
MM
occurred mostly on the plantar pedis (27'3 7o) and foot (18.2 ?o).lt
appeated thatin
BCC thenumber
oi
tumorsin
sun exposed area compared tothe non-sun exposed area was 88 versus
3
(96'7 Vo)while
in
SCC was 12 versus 20 and inMM
was 3versus S,respectively. The ratio of BCC to SCC
=2'8:I'
DISCUSSION
Due to the location of Indonesia near the equatorial belt the people will have an extensive sunlight all over
the year. Therefore, sun rays
will
play an importantrole
in
producingthe skin
cancer although the Indonesian hasdark
skin
(mostlyskin
type
V)compared to Caucasian. The majority
of
Indonesian*orÈ
in
agriculturalfield
and fisherywith
much exposure of the skin to sunlight.Basal cell carcinoma (BCC) is the commonest skin
cancer
in this study. From 139
non-melanoma skincancer, 91 cases (65.5 Vo) were BCC, while SCC was
only 32 cases (23,0 Vo)..'pte data was similar to the
ones found by others.e'
r0
From the 91 BCC casesthere were 53 (58.2 7o) females and 38 (41'8 7o)
males. This finding was in contrast to other reports'"
showing that the highest incidence was
in
males cumparedto
females because males were usuallyoutdoor workers.
The
controversial findings needsclarifying
byconsidering other factors involved
in the
occurrenceof BCC. As a matter of fact, most of the Indonesian female patients were farmers. The highest tumor
incidence was found in the age group between 51-70
years in BCC and between 60-70 years in SCC.
Regarding
the
distributionof
BCC, SCC
and rnelanoma according to tumor sites,it
appeared thatBCC were mostly located on the sun-exposed area,
i.e. head (97 .8 Vo) suggesting the role of sun exposure' Such relationship has been reported elsewhere'''
"
The locationof
SCC were mostly on the non sun-exposed area namely 20 (62.5 7o) or non-sun exposed part and 12 (37.5 Vo) on sun-exposed area' This was àlso the case with melanoma which had 8 (72'7 Vo) on 7C C 8',J 0Ê5t 7[c 8t0
Srd oer=:552
l4€an = 5? Ê
fi = 32.0C 250 :5 I {5r -q5ç 650 7:0 ,!50
3CC .10.,i 50û 6Ût t(]l 8tt
age of p atients (year)
Figure 3. Histogram ofSCC according to age Sroups
The duration of the tumor ranged from 6 months to 20
years for BCC (mean
=
4.40 yrs), whereas for SCCand
MM
fromI
month to 6 years (mean=
1.72 yrs)and from
4
months'to4
years (mean=
1.37 yrs)respectively. The local symptoms found in BCC were
change
in
color, small ulcer, sonetimes itching orbleeding, while
in
SCC the ones were the appearanceof
ulcer, bleeding tendency and
weightloss
inadvanced cases.
In MM
the local symptoms werechange in color, i.e. darkening, rapid growth, itching and bleeding. The size of the ulcer or lesion was for
80 Hamzah
non-sun exposed area, especially on the sole and 3
cases (27.3 7o) on sun exposed area of the body. This
suggested that other factors should
be taken
intoaccount, environmental factor such as trauma or bum.
We found only 11 cases of
MM
(j.9
Vo) which was very low in.^comp_arison with figures foundin
otherpopulatioirs.lo' l2' t6' l?
Similarly, we founC only
I case
of actinic
keratosis(AK)
which was _verylow
in
comparison with the Japanese findings.rT Such difference might depend onthe skin type, i.e. the Indonesian people have mostly
skin type V while the Japanese have skin type
III
and mostly skin type II. In addition, melanin pigmentationin
human has been considered as the most importantbiologic protection against ultraviolet radiationr8-le for preventing both melanoma and non melanoma skin
cancer.
Conceming the long duration
of
the existing turncrand
the big
sizeof
the
lesion,at
thê
time
of consultation, it was evident that most of the cases came to the hospital at a very late stage which was accompaniedwith poor response to the available heatment.
In
orderto
prevent this,we
haveto
organize acornprehensive and intensive educational program to
reduce the mortality rate of skin cancer by identifying
ihe cases at earlier stages.
Acknowledgement
We
wouldlike
to
thank the International CancerResearch Grant system, Monbusho, Japan and the
Dean, Faculty of Medicine, University of Indonesia,
Jakartr for
his approval
of
the Japan-Indonesia collaborative study. This work has been supported bythe grant no. 09042004, under Ministry of Educarion,
Science, Sport and Culture, Govemment of Japan and
was
partly
supportedby
the
Indonesian CancerFoundation,
the
Jakarta
International
Cancer Conference Fund andthe Terry Fox
Forrndation,Canada. The collaborative study was initiated with
Dean's
approvalno.
845|PTOZ.H4.FWE/97. Wewould
also appreciatethe
Directorof
Dr.
CiptoMangunkusumo National Central General Hospital
for his technical suppori to finish this work.
R.EFERBNCES
1.
Cornain S, Mangunkusumo R, Nasar IM, prihartcno J.Ten Most Frequent Cancer in Indonesia. pathology based
Med J Indones
Cancer Registry Data
of
1988-1992.In:
Cancer in Indonesia. National Cancer Registry Center, JakartaCoordinating Board, I 997.
ljarta A, Kanoko
M,
Mangunkusumo RR. Malignant Melanoma and Malignant Epidermal Tumors in Jakarta.Relative Frequency and some Histopathological aspects,
Presented on 2nd Congress Asia-Pacihc Associations Societies of Pathologist, February 20-23, 1991, Manila-Philippine.
Weinstock
MA.
The epidemicof
squamous cellcarcinoma. JAMA 1989; 262: 2138-40.
Glass AG. Hoover RN. The emerging epidenic of
melanoma and squamous cell carcinoma. JAMA 1989;
262:2097-lOQ.
Magnus K. The l.lordic profile of skin cancer incidence. A comparative epidemiological study of the three main type of skin cancer. Int J Cancer I99l; 4'7 : l2-9.
Marks R, Mc. Charty WH. Skin cancer: increasing
incidence and public awareness. Med J Aust 1990; 153:
Grodstein F, Speizer FE, Hunter DJ. A prospective study of incident squamous cell carcinoma of the skin in the nurses health study. J Natl. Cancer Inst. 1995; 87: 106l-6. Giles G, Marks R, Foley P. Incidence of non-melanocytic
skin cancer treated in Australia. Br Med J 1988 296: l3-7. Kricker A, Armstrong BK, Engtish DR. Sun exposure and
non-melanocytic skin cancer. Cancer Cases and Control,
1994; 5: 367-92.
Armstrong BK, Holman CD. Malignant melanoma of the
skin. Bulletin of WHO 1974;45:245-52.
Koliias N, Baqer A. Solar middle ultraviolet radiation and
skin cancer
in
Kuwaitin
BFS. Environmental UV Radiation and Health Effect 1995: 203-9.Autier P. Epidemiology of melanoma. In: I-ejeune FJ,
Chaudhuri
PK,
Das GuptaTK
(Edg.
Malignant Melanoma. Medical and Surgical -Management. New York: Mc Graw-Hill Inc., 1994: I -7Intemational Agency for Research on Cancer. Cancer Incidence in Five Continents. Vol III. IARC publication No.15. Lyon 1976
International Agency for Research on Cancer. Cancer Incidence in Five Continents. Vol V. IARC publications No. 88. Lyon 1987.
Glass
A
and Hoover R. The emerging epidemic ofmelanoma and squamous cell skin cancer. JAMA 1989;
262:2097-100.
Ichihashi M, Ueda M, Nagano T, Araki K, Ohno y, Cornain S. Clinical and epidemiological study of skin
cancer in Japan. Med J Indones 20Cf',9:70-6. - ^ Suzuki T, Ueda M, Naruse K, Nagano T,'Harada S,
Imazumi
K,
et al. Incidenceof
actinic keratosis of Japanese in Kasai City, Hyogo. J Dermatol Sci 1997; 16:74-8.
Ortonne J-P: Biology and photobiology of the melanin pigmentary system. In: Leujeune FJ, Chaudhuri PK, Das
Gupta
TK
(Eds). Malignant Melanoma. Medical andSurgical Management. New York: Mc Graw- Hill Inc., 1994:81-9.
Tyrell RM. Ultraviolet protection.
In:
t ejeune FJ,Chaudhuri
PK,
Das GuptaTK
(Eds). Malignanr Melanoma. Medical and Surgical Management. New York: Mc Graw- Hill Inc., 1994: 9l-5.