Vol 9, No 2, April
-
June 2000ln
the developed
country
such as the United
States,skin
cancers showed increased incidence.l-3
Thet
Department of,Surgery, Faculty of Medicine, Universityof
Indonesia, Jakarta I 043 0, Indonesia2 Department of Dermatology, Kobe University Schaol
of
Medicine, Kobe 650-0017, Japan
t
Deparmert of Dermatology, Faculty of Medicine, University of Indonesia, Jakarta 10430, Indonesia a Department of Anatomic Pathology, Facuby of Medicine,_ University of Indonesia, Jalcarta 10430, Indonesia
5 Department of Community Medicine, Faculty of Medicine, University of Indonesia, Jakarta 10320, Indonesia 6 Department of Preventive Medicine, Nagoya University _ School of Medicine, Nagoya 466-8550, Japan
'
Radiobiology Division, National Cancer Center ResearchInstitute, Tolcyo 104-0045, Japan
Surgical procedures in skin
cancer
8 1problems of its morbidity
remain important
in
spiteof
lower
mortility
for
non-melanoma
skin
cancers.
In
terms
of
the detection
of
skin
cancer, usually
thepatients themselves
could recognize
the tumors
andvisited
thephysician
relatively eiuly,
so thatthey
were treatedat
anearly
stageof malignancy.
In
Indonesiahowever, patients with skin cancer
seedoctors at
thelate
stageof
the
disease,mainly
due to ignorance
of
the patients
andtheir
family or the delay
in
seekingfor medical
helpfrom
thephysician.
In
1992, the relative frequency
femalesis 6.35
Vo, ranked the4ft
and thefirst in
males (11.2I
Vo).4that solar
ultraviolet
exposure caused increasedrisk
of
skin cancer
in
variouscbunries, including
Japan.l-3' 5' 6Surgical procedures implemented
in
Japan-Indonesia collaborative study
of
skin cancer
mitsu
lchihashi2,Mochtar
Hamzah3,Masato
Uedt,
SonarPanigoror,
1i artaa, Joedo Prihartonos, Seryawati B udiningsihs, Yo shiyuki -Ohno6,Abstrak
Kanker kulit kelihatan menjadi suatu masalah keganasan yang penting
di
Indonesia dan Jepang. Berdasarlcan suatu kepentingan bersamadari
masalahini,
maka dibentuk suatu studi gabungan antara Indonesia dan Jepang, mengenaitiga
aspek tentangepidemiologi,
Hinik
dan histopatologi, yang ditangani oleh2
buahtim
multidisiplin,dai
Jepang dan Indonesin. Kami al<anmembahas hasil penelitian penyakit l<anker kulit
di
Rumah Sakit Umum Pusat NasionalDr.
Cipto Mangunkusumo, mulai Agustus 1996 sampai 29Maret
1999, dimana terkumpul 139 l<asus, dengan jumlah terbanyak pada golongan usia diatas 60 tahun yaitu 78 kasus (56.1 Vo). Bergantung pada diagnosis dan meluasnya kcganasan, prosedur bedahyang diterapkan adalah amputasi dengan atautanpa pengangkatan kelenjar getah bening, hemimalcsilektomi dan el<sisi lebar dengan atau tanpa penganglcatan kelenjar getah
bening. Eksisi lebar dilakukan pada sebagian besar kasus (77,3 Eù, yaitu pada 87,9 Vo karsinoma sel basal, 66,7 Vo lcarsinoma sel skuamosa dan 66,7 Vo melanoma maligna. Selama penelusuran 2 tahun, tidak ditemulan kelcambuhan.
Abstract
Skin cancer appeared to be an important cancer problem in Indonesian and Japan. Based on common interest of the problem, a
joint
study between Japan and Indonesia
on
Skin Cancer has been established. Three foW-study, namely epidemiological,clinical
and histopathological aspects building oJ Multidisciplinary teams,for
both the Japanese and the Indonesian sides. Here, we present theresults
of
skin cancer examination in Dr. Cipto Mangunkusumo National Center General Hospital from August 1996mtil
March 29, 1999, with a total of 139 cases, with the peak at 6-decade age Broup, i.e. 78 cases (56.1 Vo). Depending on the diagnosis and theextent of the malignancy, the surgical procedures applied were amputation with or without lymph node dissection, hemimaxillectomy and wide excigion with or without lymph node dissection. Wide excision was performed in the majortty (77.3 Eù of cases, i.e. in 87.9 Vo of basal cell carcinoma, 66.7 Vo of squamous cell carcinorna and 66.7 Vo of malignant melanoma, During 2 years
follow
up, norecurrence of the malignant lesion was observed.
Similar
data has been obtainedin
our Japan-IndonesiaCollaborative
Study.TIf
the ozonedepletion
continues at theAntarctic
and also extendto
the equatorial
areain
the
future,
the
increasing number
of
cancer
in
Indonesia may become a social concem
to
be
solved.Therefore,
our ongoing epidemiological
case-control study was also accompaniedby direct
measurementof
the
solarultraviolet-B
using
biological
method
(sporedosimetry)
in
various
partsof
thecountry,
i.e. Jakarta, Padang,Yogyakarta
and Denpasar. Sofar,
the
resultsindicated
that the uv-B strength
in
Jakarta
andDenpasar
was about three
to five
times
ashigh
asin
Tokyo.s
The
findings
arenow being
analyzedfurther
in
order to
make better
assessmentof
the ultraviolet
risk
for
the
development
of skin
cancer
relative
togeographical
(tatitude) and ethnical difference
(skin
type).In
the present study,
we
aimed
to clarify
the
clinical
characteristicsof
skin
cancer treatedin
Department
of
Surgery,
applying specific
surgical
procedures adjustedfor
individual
caseaccording
to
the
stageof
thetumor
at the admissionto
thehospital. The
present paperis to discuss
the
efficacy of
the most common
treatment
applied to
the Indonesian
skin
cancer patients and someproblems
encountered.MATERIALS
AND METHODS
Clinicopathological characterization of skin
cancer
cases
for
determining surgical treatment
Skin
cancer patients
enrolled
to
the
Japan-IndonesiaJoint
Study
onEtiology
andClinicopathology
of
Skin
Cancer were patients
who visited the
Department
of
Dermatology
and
Department
of
Surgery
of
theFaculty
of Medicine,
University of
Indonesia,
from
August
1996to March
29,1999.
They
were examinedby
well-trained
dermatologists
and
surgeons during
our
study
period,
and
diagnosedclinically
at the
first
visit. Histopathological confirmation
was
establishedfrom
thebiopsy
specimens sentto
the Department
of
Pathology. Periodic evaluation
was madeboth
during
the
pilot
study started from 1995 and during
thedefinitive
studyfrom
1997 onfor
3 years.Skin
cancerpatients
with
1cm or
larger
in
diameter were
treatedby
surgery.In
orderto
characterize theclinical
aspectsand
to
evaluate
the efficacy
of the
treatments,
thepatients
were
categorized according
to
age, sex
andsite
of
the skin
cancer.
The
stageof
the
disease andthe
extent
of
the
surgical procedure
were
taken into
account
for
overall
evaluation
of
the
treatments.Depending
on
such
considerations,
the type
of
surgical
procedures
were applied accordingly.
Theguidelines applied
wasmodified from
the
one usedin
thepreliminary
study.eSurgical
procedures of
skin
cancer
Surgical
treatment
of
both
non-melanoma
andmelanoma
skin
cancerincludes
methods such aslocal
excision,
curettageand
electrodessication, cryosurgery andMohs micrographic
surgery.The
methodsapplied
were both standard and
modified
surgical managementsdocumented
elsewhere.l0-''
On"
centimeter
margin of
excision was determined
for basal cell
carcinoma
(BCC)
on
the face,
while
1.5
-
2
cm
margin
wasapplied
to
the BCC on the
back.
The margin
of
theexcised tissue was
examined
by
the pathologist for
detecting
anyremaining tumor cells, starting
from
theclosest
margin
near
the tumor border
to
the
edge
of
clinically/
macroscopically
normal skin.
If
theextreme end
of
the tissue was
free from tumor
cells,reconstruction
of
the mutilated
area
was
performed.When there were tumor cells in
or adjacent
to
theborder
of
the
tissue,
re-excision was done
until
thepathological report was negative
from tumor cells. If
the
surgery
might
causemutilation,
radiotherapy
wasapplied.
In
Dr.
Cipto Mangunkusumo
Hospital,
Jakarta,skin
cancerswith
a diameterof
I
cm or larger
were treated
in
the Department
of
Surgery
and thosewith
diameter less
than
1 cm
were treated
in
theDepartment of Dermatology.
For
the
management
of
squamous
cell
carcinoma
(SCC)
andmalignant melanoma
(MM)
patients, wide
excision
with 3
cm
margin
was
acommon
procedurein
Indonesia.For preventing
further growth of primary
skin
cancer,surgical
dissection
was applied
to
the
first regional
lymph
nodes,
if
any palpable
enlarged
lymph
nodewas
pathologically containing
tumor cells.
Suchlymph node was
removed
surgically
(therapeuticlymph
node dissection).Another application
of
surgical removal
wasto
excisea
single,
slow growing
metastatic
lesion
and also
toprepare
circulation
system
for isolated
regional
perfusion
of
anti
cancer agents,
after
excising
amelanoma
lesion of
theextremity.
The schemes
for biopsy procedures
are given
in
Vol 9, No 2, April
-
June 2000 [image:3.569.178.523.81.517.2]Figure
l.
Biopsy scheme depending on rhe size and the depth of skin cancer (in vertical orientation)Figure
2-
Bioltstl schcne dcpending on theizt
and the widthol
skin æncer lin horizoualoriawtiut)
RF^SULTS
A
total
of
139 casesof
skin
cancer were collected in
the Departments
of
Surgery and Dermatology during
study period
of
January
1996to
March
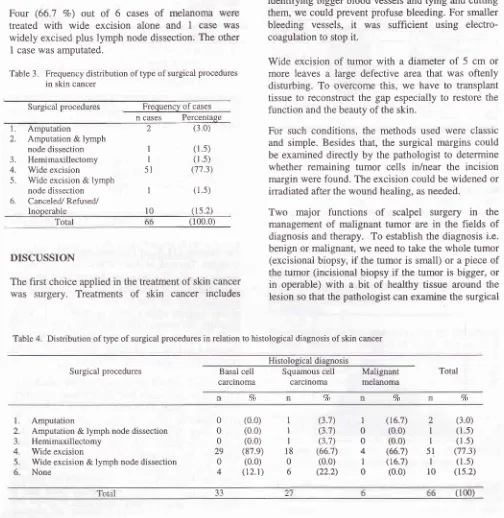
1999.The
agedistribution
of
139
cases
is
given
in
Table
l.
The
frequency distribution according
to
age
was
alsodepicted
in
Figure
3,
showing normal
distribution
with
mean ageof
58.8t
13.5 years.F t e q
U
e n
v
Sld Cor=1345 M*sn. 5g 8
NE1!SD( ?5C
3ùû 4a0 !c0 60a ?0t 6t0 age of patients (year)
Figure 3. Age distibution of
all
skin cancer cases collected in :\rc Departmerûs of Dennatology and Surgery,from
January1996 to March 1999.
SurgicaL procedures in skin cancer
Table 1. Age
distribution
ofall
skin cancers (n=
139)collected at Departments
of
Dermatology and surgery from 1996 to 1999Age group Frequency of cases
n
(Vo)83
20
-29
30-39
40-49
50-59
60-69
70-2 10
l9
30 45 33
(1.4) (7.2)
(t3.7)
(2r.6) (32.4)
(23;t)
Total (100.0)
"lable
2.
Age distribution of skin cancers treated at Department of Surgery from 1996 to 1999Age group Frequency of cases
(vo)
139
20-29
30-39
40-49
50-59
60-69
70-I
2
11 t4 24 t4
(1.5) (3.0) (r6.7)
(2t.2)
(36.4) (21.2)
Total (100.0)
The
majority (77
Vo)of
the
cases aged50
-
70'years
or
higher.
The peakof
skin
cancer cases wasin
the 6th decade,i.e.
45
(32.4
Vo) cases.Among
them 66
caseswere
treated atthe Department
of
Surgery.
Thirty
six
were males and 30
were
females.The
agedistribution
of
the
surgical treated
cases
is
given
in
Table
2.Similarly,
the
majority
(78.8
Vo)of
the
cases aged 50-
70
years or
higher.
Histologically,
they
were diagnosed asBCC
in
33
(50.0
Vo) cases,SCC
in
27 (40.9 7o) casesMM in
6 (9.1 7o) cases.The type
of
surgical procedures
applied varied from
amputation, amputation
plus
lymph
node
dissection,hemimaxillectomy,
wide
excision,
wide excision
andlymph
node dissection.The
majority,
i.e.
5l
(77.3
Vo)cases
were
treated
by
wide
excision
only
andcombination
with
lymph node dissection
in
1
case,while the
reÉtwas treated
by
amputation
in
2
cases,amputation
plus
lymph node dissection
in
1
case,hemimaxillectomy
in
1 case.The
details
aregiven
in
Table
3.
Ten
cases
were
not
treated either due
tocancellation, refusal
orinoperable
status.Twenty nine (87.9
Vo)out
of
33
cases ofBCC
werewidely
excised,
with
only
I-2
cm margin
in
most
of
the cases,
while
in
5
cases,the excision
wasfollowed
by
reconstruction
dueto the wide
lossof
normal
skin.Four
cases
(12.1
Vo)
were
not
treated
by
surgery.Wide
excision
was also applied
to
the majority of
SCC, i.e.
in
18(66.7
7o) oatof
27
cases.Three
caseswere
treated
by
amputation, amputation
plus
lymph
node
dissection and
hemimaxillectomy,
respectively.
Six
cases(22.2
Vo) were untreatedsurgically.
Four
(66.7 Vo)
out
of 6
cases
of
melanoma
weretreated
with
wide
excision alone
and
1
case
waswidely
excisedplus
lymph
node
dissection.The
other 1 case was amputated.Table
3.
Frequency distribution of type of surgical proceduresin skin cancer
Surgical procedures Frequency of cases n
cases
Percentagemethods
such asscalpel surgery/
local
excision,
lasersurgery,
cryosurgery,
curettage,
electrosurgery
(electrodessication)
andchemosurgery method (Mohs
micrographic surgery),
with
its advantages
and disadvantages.The goal
of
thesurgical
procedure wasto
provide
the
patients
with the
safest, most
costeffeitive
andcuràtive
treatment.r3As for
scalpel surgery, bleeding was
the
common
disadvantage,
but
by
carefully
dissecting
the
tissue,identifying
bigger blood
vessels andtying
andcutting
them,
we could prevent profuse bleeding.
For
smaller
bleeding vessels,
it
was
sufficient using
electro-coagulation to
stopit.
Wide excision
of
tumor
with
a
diameter
of
5
cm
or
more
leaves
a large defective
area
that was oftenly
disturbing.
To
overcome
this,
we
have
to
transplant tissueto
reconstruct
the
gap especially
to
restore
thefunction
and the beautyof
the skin.For
such
conditions, the
methods used
were
classicand simple. Besides
that, the
surgical margins could
be examined
directly
by
the pathologist
to
determinewhether remaining tumor cells in/near the
incision
margin
werefound. The excision could
bewidened or
irradiated
after thewound healing,
as needed.Two major
functions
of
scalpel surgery
in the
managementof
malignant
tumor
are
in
the fields of
diagnosis andtherapy. To
establishthe diagnosis
i.e.benign or malignant,
we needto
take thewhole tumor
(excisional biopsy,
if
thetumor
is
small)
or
apiece
of
thetumor (incisional biopsy
if
the
tumor
is
bigger,
or
in
operable)
with
a
bit of
healthy tissue
around
thelesion
so that thepathologist
can examinethe surgical
2
I
I 51I
l0
l.
z. 3. 4. 5. 6, AmputationAmputation & lymph
node dissection Hemimaxillectomy Wide excision
Wide excision & lymph
node dissection
Canceled./ Refused/ Inoperable
(3.0)
(l.s)
(l.s)
(77.3)( 1.5)
(rs.2)
Total (100.0)
DISCUSSION
The
first
choice
appliedin
the treatmentof
skin
cancerwas
surgery. Treatments
of
skin
cancer
includesTable
4.
Distribution of type of surgical procedures in relation to histological diagnosis of skin cancerHistological diagnosis
Surgical procedures Basal cell carclnoma
Squamous cell carclnoma Malignant melanoma Total 2
I
I
5l
I
t0
1 1 I 18 0 6 0 0 0 29 0 4l.
2. J. 4. 5. 6. AmputationAmputation & lymph node dissection Hemimaxillectomy
Wide excision
Wide excision & lymph node dissection None (0.0) (0.0) (0.0) (87.e) (0.0) (12.1) (3.7) (3.7) (3.7) (66.7) (0.0) (22.2) (16.7) (0.0) (0.0) (66.7) (r6.7) (0.0) (3.0)
(l.s)
(1.5) (77.3) [image:4.579.43.547.209.727.2]Vol 9, No 2, April
-
June 2000margins,
the
pattern
of
infiltration,
as
well
as
theetiology
of
the lesion.The form
of the excised tissue should
be in
the
form
of
a dice, to makeit
easy tomark
the margins.In
caseof
BCC
of
small
lesions
lessthan
10
mm in
diameter, excisional
biopsy or total
excision
with
a 5mm
margin
from
the
border
the
tumor
wereperformed
for
the treatment. Beside thisfresh
samplesfrom
thetumor,
thenormal
skin peripheralto
thetumor
and also
from
normal skin
apart
from
the
tumor(s)
were taken
for
themolecular epidemiological
study.For
a
BCC
with diameter
of
10mm or
over,
tumorslocated
on
the face and other locations were
wide-excised
with
amargin of
15-20mm, respectively. The
excised
tissueswere examined histopathologically by
pathologists,
for
evaluating marginal
tissue.
We did
not
find
any
lymph
node metastasisin
BCC.
In
Japan,BCC both on the
face and
any
other
body
sites
wasremoved
by 5
mm margin, but
in
case
of
morpheatype
of
BCC, the margin
of
excision was 10
mm,since morphea
type BCC
was known
to invade
efficiently during a
rather short
period.
In
caseof
alarge
facial skin
cancer serial
excision
performed in
the setting
of
Mohs micrographic
surgery has
beenintroduced
and resulted
in
excellent
cosmesis
andfunction.ra
This kind of
techniquemight
bebeneficial
in
case
of
the
presentation
of
the skin
cancers
arealready
in
later
stage
and relatively Qig size
asfrequently encountered
in
our
study,r5
with
themajority
of
BCC
located on theface
(97.6
Vo).In
the
flture,
marginal
areas
may
become smaller
andsmaller, since
longitudinal
analysis of
operated caseshave
been
extensively done and the data show
nodifTèrence
between
5
cm and
3
cm margin
even
in
MM
treatment.For
SCC, wide
excision
of
the primary
lesionscomprises
2 cm
of healthy
skin in all
directions,
with
reconstruction using prefèrably
with split
thicknessskin graft,
except
if
dissection
of
the
tissue
disturbsthe
tunction
of
the area.For MM,
wide
excision
depends
upon
thepathological staging
of
the tumor. For the
low
risk
tumors
measuring less than
0.76 mm, wide
excisionwith
more
than
I
cm free
margins proved
to be
suitable.
While fbr
the moderate
risk
group
of tumor
thickness between
0.76
-
1.50mm, the
safety marginsrequired
are2 -
3cm
fiom
the tumor
borders.But for
the high
risk
group
of
more than
1.50mm, we
exciseSurgicaL procedures in skin cancer 85
with
a
3 - 5
cm
safety margins
from
the
tumor
borders.
For
enlarged
lymph
nodes,
we
perform
only
dissection
if
the
pathology
proved
it
to
contain
metastatic
tumor cells. Appropriate
management
of
local
recurrence,
satellites
and transit
metastasesmight need isolation perfusion.l2 So
far,
malignant
melanoma has become great concern
for
surgical
treatment
due
to
its
aggressive
behavior
and
thepropensity
to
metastasizethrough the lymphatic
andblood
routes. Patients
at
high
risk for
metastasesshould
be evaluatedby
meansof x-ray
and computedtomography
(CT)
scans.A modified
technique namelyresection using
CT
or ultrasound guidedwire
localizationhas been applied to non-palpable metastatic melanoma,
which
offers
several advantages,i.e.
minimal
surgical
dissection, shorter
operatedtimes and
decreased postoperative
morbidity.'6
Acknowledgement
We
appreciate
the
Intemational Cancer
ResearchGrant
system, Monbusho, Japan
and
the
Dean,Faculty
of Medicine, University
of Indonesia,
Jakartafor
his approval
of the Japan-Indonesia
collaborative
study, which was initiated
by
Dean's approval
No.
845|PTO2.H4.FWE|97.
This work
has been supportedby
the
grant
no.
09042004,
under
Ministry
of
Education, Science, Sports and
Culture,
Government
of
Japan andwas
partly
supportedby the
[ndonesianCancer Foundation,
the
Jakarta
International
CancerConference
Fund and the
Teny
Fox
Foundation,Canada. We
would also thank the Director
of
Dr.
Cipto
Mangunkusumo
National Central
GeneralHospital
for
technical
assistance.REFERENCES
L
GlassAG,
Hoover
RN. The
emerging epidemicof
melanoma and squamous cell skin cancer.
JAMA
1989; 262:209'1-1O0.2.
Kricker A, Amstrong BK, English DR. Sun exposure and nonmelanocytic skin cancer. Cancer Causes and Control 7994:5:369-92.3.
English
DR,
AmstrongBK, Kricker
A,
Fleming C. Sunlight and cancer. Cancer Causes and Control 1997;8: 271-83.4.
Cornain S, MangunkusumoR,
NasarIM,
Prihartono J. Ten most frequent cancers in Indonesia: Pathology based5.
6.
Groclstein F, Speizer FE, Hunter DJ.
A
prospective studyof
incident tqrumous cell carcinomaof
the skinin
the nurses' health study. J Natl Cancer Inst 1995; 87: 1061-6' Suzuki T, UedaM,
OgataK,
HorikoshiT,
Munakata N, IchihashiM.
Doses of solar-ultraviolet radiation correlate with skin cancer rates in Japan. Kobe J Med Sci 1996; 42: 375-88.Prihartono
J,
BudiningsihS,
Ohno
Y,
Hamzah M,Ichihashi M, Poetiray E, et al. Risk factors of skin cancer among Indonesian population. Med
J
Indones 2000' 9: 100-5.Munakata
N.
Comain
S'
Mulyadi
K,
IchihashiM'
Prihartono J, Ohno
Y,
et al. Biologically effective dosesof ambient solar-uv radiatign in Indonesia and Japan Med
J Indones 2000; 9:123-8'
Evert Poetiray. Surgical Procedures Implemented
in
Skin Cancep Study. Presentedin
OneDay
Symposium on Multicènter Study of Epidemiology and Clinicopathologyof
Skin Cancer (Japan-Indonesia Collaborative Study onEtiology and Clinicopathology
of
Skin Cancer) July 30' 1997.Malignant Melanoma. Medical and Surgical Management' New York: Mc. Graw-Hill, 1994 205-14.
Storm FK, Mahvi DM. Treatment of primary melanoma'
In:
tæjeuneFJ,
ChaudhuriPK,
Das GuptaTK
(Eds)' Malignant Melanoma. Medical and Surgical Management' New York: Mc. Graw-Hill ,1994.193-203.KooPs H'
Kroon
BBR,
Lejeune
FJ't
of
local
recurrence, satellites and transitof the limbs
with
isolation perfusion' In:Lejeune
FJ,
ChaudhuriPK,
Das
Gupta
TK
(Eds)'Malignant Melanoma. Medical and Surgical Management' New York: Mc. Graw-Hill ,1994:.221-31.
Anthony
ML.
Surgical treatmentof
nonmelanoma skin. cancer. AORN J 2000; 71:.552-4.Schanbacker C, Randle
HW.
Serial excisionof
a large facial skin cancer. Dermatol Surg 2000; 26: 381-3' HamzahM,
IchihashiM,
CiptoM,
PoetirayE,
MukhtarA,
KanokoM,
et al,A
clinical studyof
skin cancer in l1t2
8
l3
t4
l5
l6
9