Management of
biliary
ascariasis:
report
of
21
cases
L.A.
Lesmana
INTRODUCTION
Ascariasis
is
oneof
themost frequent
helminthic
dis-eases
in humans.l
It
occurs mainly in countries
where the standardofpublic
health
and personalhygiene
arelow.
The adult worm of
ascariscommonly lives
in
theintestinal lumen without any significant
symptoms.2However, when
aggregated
into
worms
masses theymay
cause intestinal obstruction, volvulus, and
per-foration of
thebowel. Ascaris
may also invadeinto
thebiliary
tree
which can cause recurrent
biliary
colic,
acute
cholangitis, cholecystitis, and
pancreatitis.2-aAfter
invasion
into
the
bile
duct, the worms
usually
migrate
into
the duodenum
within
a period
of
two
weeks. Endoscopic retrograde cholangiography
is
anexcellent,
diagno-sticmodality
to delineate
worms in
the biliary
tree.2'5-7Some
investigators have
also described the sonographic featuresof
ascaris in thebile
duct.5'7-9
The majority of patients with
biliary
ascariasis can bemanaged conservatively
with
simptomatic
treatment
andantihelminthic
drugs.2'10Endor.opic
treatment
of
biliary
ascariasis has also beenreported.6'l
I'12The purpose
of this
study was toreport our
experiencein the management
of biliary
ascariasis
with
special referenceto
endoscopic treatment"Abstrak
Studi ini diLakukan untuk menilai penatalaksanaan asknriasis biLier khususnya terapi endoskopik.
Dari I
Januari, 1986 sampai dengan 3I
Desember I 996, pada pemeriksaan endoscopic retrograde cholangio-pancreatography (ERCP) ditemukan sebanyak 2I
kasus askariasis bilier. Tiga dari 2I pasien telnh menjalani sfingterotomi sebelumnya untuk pengeLuaran batu saluran empedu (BSE) dan 4 pasienjuga
mempunyai BSE pada ERCP. Tiga belas dari 21 penderita (62Vo) mengeluh kolik bilier berulang sedangknnI
lainnya (38Vo) mengalami kolangitis akut. Ultrasotnd (US) dengan real time scanner mendeteksi cacingdi
dalam SE pada 7 danl3
(54Vo) penderita yang diperiksa. Tujuh belas pasien (81%) menjalani sfingterotomi kecil diikuti dengan ekstraksi cacing dengan dormia basket. Pengeluaran cacing askaris berhasil padall
(657o)dari
17 penderita sedangkan pada6
lainnya dipasang kateter naso-bilier. Pembersihan saluran empedu didnpatkan pada keenam penderita ini pada kolangiografi melalui kateter. Empat pasien sisanya ( lgVo) yang disertai BSE menjalani operasi tanpa penyulit. Sebagai kesimpulan, US dan ERCP sangat bermanfaat dalam diagnosis askariasisbilier
dan terapi endoskopik perlu dipertimbangkan sebagai pilihan pertama pada pasien dengan obstruksi bilier simptomatik dan kolangitis akut.Abstract
This shrdy was carried out to assess the management of biliary ascariasis with special reference to endoscopic treatment. From January
l,
1986 to December 31, 1996, twenty one casesof
biliary ascariasis were detected at endoscopic retrograde cholangio-pancreatography (ERCP) examination. Thirteen of 21 patients (62Vo) presented with recurrent biliary colic and the remaining 8 patients (387o) developed acute cholangitis. Ultrasound (US) using a real time scanner detected the worm in the CBD in 7 of 13 (54Va) palients examined. Three of 21 patients had prior sphincterotomy for removal of common ble duct (CBD) stones and 4 patients had concurrent CBD stones at ERCP. Seventeen patients (81%) underwent a small sphincterotomy followed by extraction of worm with a dormia basket. Removal of worm was successfulinll
(65%) of these patients, whereas in the other 6 patients a naso-biliary tube was inserted for the administration of pyrantel pamoate directly into the bile duct. Interval duct clearance was obtained in all these 6 patients at subsequent tube cholangiography. The remaining 4 patients(I9%)
with CBD stones underwent uneventful surgery. In conclusion, US and ERCp are very useful in the diagnosis of biliary ascariasis and endoscopic treatment should be considered as the flrst treatment of choice for tbose patients with symptomatic biliary obstruction and acute cholangitis.Keywords : Biliary ascariasis, ultrasound, endoscopic retrograde cholangio-pancreatography
106 Lesmana
PATIENTS AND METHODS
From January
1,
1986
to
December
31, 1996,2046
endoscopic
retrograde cholangio-pancreatography
(ERCP) examinations were performed
for
bilio-pancreatic disorders.) ERCP was performed
using
standard
technique under intravenous sedation
with
Olympus
duodenoscopes typeJb3,
JB4, JFIT-10
or JFIT-20. Twenty
one
caseswith biliary
ascariasis were detected assmooth, long, linear
filling
defects in
thebile duct
(figurel).
All
thesepatients
presentedwith
recurrent biliary colic
and acutecholangitis.
Routine hemogram,
liver
function tests, and
serum amylasedeterminations were carried out according to
[image:2.595.51.548.331.770.2]standard
methods-'
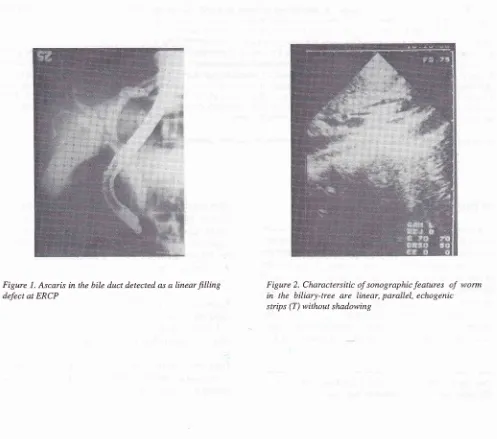
Figure
I.
Ascaris in the bile duct detected as a linearfilling
defect at ERCPMed J Indones
Thirteen
of
2l patients
had undergone ultrasound (US)3examination
prior to ERCP
in
several other
hospitals using arealtime
scanner. Sonographic features ofworm
in
thebiliary
tree weredefined
aslong, linear, parallel
echogenic strips
without
shadowing(figure
2).All
patients were
initially
treated
with
intravenous
fluids
and analgesic. Thosewith
acutecholangitis
alsoreceived antibiotics.
In
17patients with biliary
ascariasiswithout
common
bile
duct stones a smallsphincterotomy
was carriedout
to facilitate insertion of dormia
basketsfor worm
ex-traction.
The remaining
four
patients which were
associatedwith
ratherbiq
commonbile
duct(CBD)
stonesunder-went surgery.'
All
patients
received anthelminthic
(pyrantel
pamo-ate)therapy
in
single
dose of 10mglkg
body weight.
RESULTS
Of
the 21 patientsproven
biliary
ascariasiswith ERCP
therewere
l3
females
and 8 maleswith
an average ageof
45 years (range26-55
years).Biliary
ascariasis was detectedwith
US
in
sevenof
13patients examined
(5480) and
biliary
dilatation
wasreported
in
theremaining
6patients.
In
all patients
nopart
of
the
worm was protruding
from
the
papilla.
Thirteen
(6280)
patients
presented
recurrent
biliary
colic
and
the remainin9 8
(38Vo)patients
developedTable
l.
Clinical presentation of2l
patients with biliary ascariasisRecurrent biliary colic Acute cholangitis
tract
via
the tube.Three
dayslater duct
clearance wasobtained
in
all
these
6
patients at tube
cholangiog-raphy.
Three
of the
2l
patients
hadprior
sphincterotomy
for
removal
of CBD
stones andfour
patients
had concur-rentrelative big CBD
stones at ERCP(figure
5). Thosefour
patients
associatedwith CBD
stonesunderwent
uneventful surgery
(figure
6).
DISCUSSION
The
present
study
supports
previous reports that in
endemic area
biliary
ascariasis should beincluded
into
differ
isin
patients
with biliary colic
andacute
8
Ou,
data also show that
evenpatients
who
have undergone sphincterotomy
candevelop
biliary
ascaripsiswhich
is
in
agreementwith
a
formèr
"ur"
i.port.l3
"
US examination could
only
achieve
sensitivity
rateof
54Vo
for detecting
which
is
lower
compared
to
This
dis-crepancy may
partl
riation in
experience
of
the
sonologists since the
procedureswere performed
in
several
hospitals.
A
recent study
shown thatsensitivity of
UScould
reach 100%without
any false positive
diagnosis
in l9
surgically
proven
biliary
ascariasis
cases.'
The most
prevalent
sonographic
findings
were
linear,
echogenic
non-shadowing
tubes
in 15 patients
(79Vo)
and varying
degree ofbiliary
dilatation
in9 (47Vo).
ERCP has been proved to be the most
reliable
modality
in
thedetection
of
ascarisin
thebiliary-system.
How-ever,
this
delicate endoscopic technique
is not
avail-able
in
most medical
centresin
Indonesia. Therefore,
Vo r00
2l
TotaI T3 8 62 38acute
cholangitis (table
1).Laboratory findings in all
patients were comparable
with biliary
obstruction./
Endoscopic
treatment was performed
in l7
patients(8IVo); extraction
of
theworm from
thebile
duct
was successfulin
1 1 patients (65Vo)(figure
3 andfigure
4).In
six
patients
with
worm-extraction
failure
anasobiliary tube was then inserted
and pyrantel
[image:3.595.177.424.537.711.2]pamoate
(10
cc) was
instilled directly into
thebiliary
108 Lesmana
US
as arapid, non-invasive examination
should be theprimary oi choice
in diagnosing
biliary
ascariasis.eEndoscopic extraction of
ascarisfrom
the commonbile
duct
is
relatively
easy
if
some part
of
the worm
isprotruding
from the
papilla.12'13-Our success rate of
endoscopic treatment
of
the worm
of
65Vois
lower
compared
to
the
previous-report using
a
balloon
catheteror
adormia basket.o In our experience, there
was no specialtrick to catch the
*or-10
with
adormia
basket sothat the successful
removal might
be relatedto the
position
and location
of
the ascaris
in
the bile
duct. The
useof
occlusion
balloon catheter might
bean alternative method
to extract the
worms.Ô Thead-vantage of endoscopic treatment was the rapid
relief of
biliary symptoms
in all patients.
Med J Indones
In six patients
receiving
anasobiliary tube
anthelmin-thic was also administered into
the common bileduct
via the tube hoping the direct effect
of
drug
on the
worm
aspreviously reported.lo
However, this approach
isnot generally
accepted since a dead wormoften
fails to move
out the biliary tract
into
the duodenum and furthermore pyrantel pamoatehas no enterohepatic
circulation.
I aTherefore, the
disappearanceof
ascarisin
all these
6patients obtained at subsequent tube
cholangiography
was
probably due to the
spontaneousmoving
of
theworm into the duodenum
via
arelative big orifice of
the papilla after sphincterotomy. The insertion
of
anasobiliary tube
might be
useful
to
monitor
duct
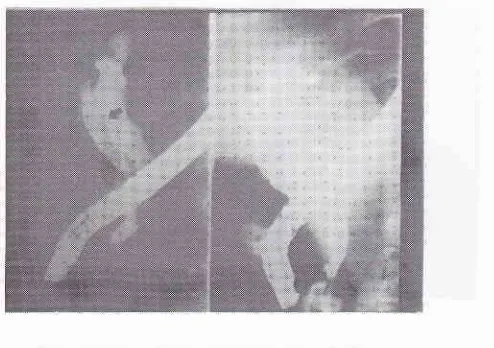
Figure4.Endoscopicfindingsshow:papillaofVaterafter small sphincterotomy (upper left),awotm
is extractedoutofthe
[image:4.595.170.408.516.696.2]papillawithadormiabasket(upper right andlowerleft),the live
worm afierremovalfromtheduodenoscopeFigure 5. A worm in the common bile duct at ERCP after extractionfailure (left) and a naso-biliary tube is insertedfor
Figure 6. ERCP reveals a worm (upper arrow) associated with a reLative big stone (lower arrow) in the common bile duct
7
110 Lesmana
clearance
after oral anthelminthic
treatment although
this
can be donewith
US by experienced sonologist.
Despite
successful clearance
of
the biliary
system,anthelminthic
therapy
isindicated for
the treatmentof
the gut
infestation
andto
prevent another
worm from
migrating
upto
thebiliary-tract.
In
endemic
area, some have recommended
2
month
antihelmintic therapy
to
avoid recurrent
of
the
dis-
ease.-The
remaining
four
patients
with concurrent
common
bile duct
slones underwent
uneventful
surgery.
With
the current
availability
of accesories
for endoscopic
treatment such as mechanical
or
electro-hydraulic
lithotrypter,
surgery
might
not
belonger
necessaryin
almost
all
hepatobiliary
ascariasis cases
associatedwith
relative
big CBD
stones.In
conclusion,
US
and
ERCP
are
very useful
in the
diagnosis
of biliary
ascariasis and endoscopic
treat-ment should be
considered as
the
first
treatment
of
choice
for
those patients
with
symptomatic
biliary
obstruction
and acutecholangitis.
REFERENCES
l.
Louw JH. Abdominal complications of Ascaris lubricoides infestation in childhood. Br J. Surg 1966;53:510-21.Med J Indones
2. Khuroo MS, Zargar SA. Biliary ascariasis: a common cause
of biliary
and pancreatic diseasein
an endemic area.Gastroenterology 1985; 88: 418-23.
3. Yang SCH, Laube PJ. Biliary ascariasis-report
of
19 cases. Am Surg 1946; 123: 299-303.4. Wright RM, Dorrough RL, Ditmore HB. Ascariasis of the
biliary system. Arch Surg 1963;86: 402-5.
5. Khuroo MS, Zargar SA, Mahajou
R,
BhatRL,
Javid G.Sonographic
appearances
in biliary
ascariasis.
Gastroenterolo gy 1987 ; 93: 267 -'12.
6. Leung JW, Chung SCS. Endoscopic management of biliary
ascariasis. Gastrointestinal Endoscopy 1988; 34: 318-20. 7. Aslam M, Dore SP, Verbank JJ, De Soete CJ, Ghillebert GG.
Ultrasonographic Diagnosis of Hepatobiliary Ascari asis. J Ultrasound Med. 1993; 12:573-6.
8. Khuroo
MS,
MahajanR,
ZargarSA,
JavidG,
Japru S.Prevalence of biliary tract disease
in
India: a sonographic study in adult population in Kashmir. Gut 1989; 30:201-5. 9.Ali
M, Khan AN. Sonography of Hepatobiliary Ascariasis.J Clin Ultrasound 1996; 24:235-41.
10. Kamath PS, Joseph DC, Chandron R, Rao SR, Sri Prakash
ML, D'Cruz AJ. Biliary ascariasis: ultrasonography,
endo-scopic retrograde cholangiography, and
biliary
drainage. Gastroenterology 1986;9l:
730-2.1 1. ChenYS, Den BX, HuongBL,Xu LZ. Endoscopic diagnosis
and management of ascaris induced acute pancreatitis. En-doscopy 1986; 18: 127-8.
12. Moniliawi MS, Khattar WY, Helmy
MM,
Bucharth F.En-doscopic diagnosis and extraction of biliary ascariasis. En-doscopy 1986; 18: 204-5.
13. Van Severen M. Lengele B, Durevil J, Shapiro M, Dove Ch. Hepatic ascariasis. Endoscopy 1987 ; 19: 140-2.
14. Zarfar JA, Khuroo MS. Treatment of biliary ascariasis and