High plasma levels of
a
- and
b
-carotene are associated with a
lower risk of atherosclerosis
Results from the Bruneck study
Anna D’Odorico
a, Diego Martines
a, Stefan Kiechl
b, Georg Egger
b,
Friedrich Oberhollenzer
c, Piero Bonvicini
d, Giacomo Carlo Sturniolo
a,
Remo Naccarato
a, Johann Willeit
b,*
aDepartment of Surgery and Gastroenterology,Uni6ersity of Padua,Padua,Italy bDepartment of Neurology,Uni6ersity of Innsbruck,Anichstr35,A-6020Innsbruck,Austria
cDi6ision of Internal Medicine,Bruneck,Italy
dDepartment of Clinical Biochemistry,Uni6ersity of Padua,Padua,Italy
Received 13 July 1999; received in revised form 29 November 1999; accepted 7 January 2000
Abstract
Background and purpose: A large number of studies have contributed to the hypothesis that carotenoids, vitamins A and E are protective against atherosclerosis by acting as antioxidants. The aim of this study was to assess the relationship between plasma levels of carotenoids (a- andb- carotene, lutein, lycopene, zeaxanthin,b-cryptoxanthin), vitamins A and E, and atherosclerosis in the carotid and femoral arteries. Methods: This prospective and cross sectional study involved a randomly selected population sample of 392 men and women aged 45 – 65 years. Carotid and femoral artery atherosclerosis was assessed by high-resolution duplex ultrasound.Results:a- andb- carotene plasma levels were inversely associated with the prevalence of atherosclerosis in the carotid and femoral arteries (P=0.004) and with the 5-year incidence of atherosclerotic lesions in the carotid arteries (P=0.04). These findings were obtained after adjustment for other cardiovascular risk factors (sex, age, LDL (low density lipoproteins), ferritin, systolic blood pressure, smoking, categories of alcohol consumption, social status, C-reactive protein). Atherosclerosis risk gradually decreased with increasing plasmaa- and b-carotene concentrations (P=0.004). No associations were found between vitamin A and E plasma levels and atherosclerosis. Conclusions: This study provides further epidemiological evidence of a protective role of higha- andb- carotene in early atherogenesis. © 2000 Elsevier Science Ireland Ltd. All rights reserved.
Keywords:Antioxidants;a-Carotene;b-Carotene; Atherosclerosis; Carotid artery disease
www.elsevier.com/locate/atherosclerosis
1. Introduction
Cardiovascular disease is the leading cause of mor-bidity and mortality in industrialized countries and hyperlipidemia constitutes one of the main underlying risk conditions. A large number of epidemiological and experimental studies have contributed to the hypothesis that oxidative surface modifications of low-density lipo-protein (LDL) are crucial in the initiation of lipid-in-duced atherogenesis [1,2]. Modified LDL is more
readily taken up by macrophages through the scavenger receptor, giving rise to the formation of foam cells and fatty streaks. Antioxidant substances disolved in LDL may be expected to counteract lipid peroxidation and decelerate atherosclerosis progression [3]. Strong sup-port for this concept derives from an animal model in which large amounts of dietary carotenoids protected against the development of atherosclerosis [4].
Furthermore, a variety of epidemiological studies [5 – 13] suggest inhibitory effects of high vitamin E and carotenoids on myocardial infarction, ischemic stroke and progression of coronary heart disease. These stud-ies focused on clinical complications of advanced atherosclerosis, and thus cannot furnish the proof of an * Corresponding author. Tel.: +43-512-5044279; fax: +
43-512-5044260.
E-mail address:[email protected] (J. Willeit).
A.D’Odorico et al./Atherosclerosis153 (2000) 231 – 239 232
antioxidant defense of carotenoids and vitamins [14]. Vitamin E, for example, could prevent progression of cardiovascular disease by potential blood clotting con-trol [15] and platelet adherence modulation properties [16,17]. Epidemiological surveys which directly address the effects of antioxidant levels on early atherosclerosis are needed to verify the key issue, but such evaluations are particularly scarce [18].
The current study was designed to investigate the association between carotenoids (a- and b- carotene, lutein, lycopene, zeaxanthin,b-cryptoxanthin), vitamins A and E, and carotid and femoral artery atherosclerosis in a large random sample of men and women aged 45 – 65 years.
2. Methods
2.1. Study population
Population recruitment was performed as a part of the Bruneck Study [19 – 23]. The survey area is located in northern Italy (province of Bolzano). Agriculture, tourism, commerce, and light industry are the main sources of income. Geographic remoteness determines low population mobility and maintenance of a tradi-tional lifestyle. At the 1990 baseline the study popula-tion was recruited as an age- and sex-stratified random sample of 1000 men and women aged 40 – 79 years (125 in each of the 5 – 8th decades). A total of 93.6% partic-ipated, with data assessment completed in 919 subjects. During the follow-up period between summer 1990 and 1995 a subgroup of 62 individuals died and one moved away and could not be traced. In the remaining popula-tion, follow-up was 96.5% complete (n=826). Plasma antioxidant levels were assessed as part of the 1995 evaluation in all subjects aged 45 – 65 years (n=452). After the exclusion of men and women with missing laboratory data (n=38) and those with temporary vitamin supplements (n=22), in whom a single antioxi-dant measurement may fail to adequately reflect long-term concentrations, 392 subjects were eligible for the current evaluation. All participants gave their informed consent before entering the study.
2.2. Clinical history and examination
The study protocol included neurological and cardio-logical examinations as detailed previously [19,20]. A standardized questionnaire was completed by each par-ticipant on current and past exposure to candidate cardiovascular risk factors, sociodemographic variables, previous diseases, and use of medication. The systolic and diastolic blood pressure was taken in a sitting position after at least 10 min of rest (mean of three independent measurements). Hypertension was defined
by a systolic blood pressure ]160 mmHg or diastolic blood pressure ]95 mmHg. The average number of cigarettes smoked per day was noted for each smoker and ex-smoker. Diabetes mellitus was coded present for subjects on therapy with insulin or oral antidiabetic drugs and/or with fasting glucose plasma levels \7.8 mmol/l (140 mg/dl), or a 2-h value \11.1 mmol/l (200 mg/dl) after oral glucose loading. The body mass index was calculated as weight (kg) divided by height (m2).
Assessment of regular alcohol consumption was per-formed with a standardized questionnaire [23]: Subjects were instructed to indicate their customary drinking frequency (days per week) and the average amount of alcoholic beverages ingested on a typical occasion or during a typical day. Beer (500-ml bottle, equivalent to about 25 g ethyl alcohol), white or red wine (250-ml glass, 25 g ethanol), and spirits and liqueurs (standard drink, 8 – 10 g alcohol each) were included as separate items. Average alcohol consumption was quantified in terms of grams per day (g/day) and classified in four categories: abstainers (0 g/day) and light (1 – 50 g/day), moderate (51 – 99 g/day), and heavy drinkers (]100 g/day). Socioeconomic status was defined with a two-category scale (1=low, 2=high) based on information about the occupational status of the person with the highest income in the household and the educational level of the proband. A high social status was assumed if the subject had ]12 years of education and/or the average monthly income of the subject or his/her spouse was $2000 or greater. Finally, subjects were asked to record frequency and duration of sports activ-ities over a 4 week period. Based on these data, three levels of leisure-time physical activity were differenti-ated: 1) no exercise at all, 2) regular physical activity of up to 2 h on average per week, and 3) regular physical activity of \2 h per week [20].
2.3. Laboratory measurements
chromato-graphic system consisted of a Beckman 114 Mitzi au-tosampler with a Spherisorb S5 ODS 2 reversed phase column 259×4.6 mm (Phase Separation, Clwyd UK), and acetonitrile – water (9:1, v/v) and ethylacetate were used as the mobile phase at a flow rate of 1 ml/min. A diode array detector (Module 168, Beckman) was used. Carotenoids were detected at 450 nm, retinol and retinol acetate at 325 nm and a-tocopherol at 292 nm. Pure forms of each carotenoid were used as reference standards for quantification by ultraviolet or visible spectrophotometry (Uvicon Spectrophotometer 922, Kontron Instruments). Apolipoproteins were measured using a nephelometric fixed-time method (apolipo-protein B and AI, CV=5.7 and 2.4%). Total choles-terol, high-density lipoprotein cholesterol and triglycerides were determined enzymatically (CHOD-PAP and GPO-(CHOD-PAP methods, Merck, Germany; CV=
2.2 – 2.4%). Low-density lipoprotein cholesterol was calculated using the Friedewald formula, except for subjects with triglyceride concentrations \400 mg/dl. Fibrinogen and other parameters were measured by standard laboratory procedures [19].
2.4. Chemicals
Standards of a- and b-carotene, lutein, lycopene, retinol, retinol acetate anda-tocopherol were purchased from Sigma Chemical (St. Louis, MO). The zeaxanthin standard was kindly provided by Hoffman La Roche (Basel, Switzerland). HPLC-grade acetone, absolute ethanol, ethyl acetate, and hexane were purchased from Merck. Acetonitrile was obtained from Carlo Erba (Milan, Italy).
2.5. E6aluation of 6ascular status
At the 1990 baseline sonographic assessment was performed using a duplex ultrasound system (ATL8, Advanced Technology Laboratories) with a 10-MHz scanning frequency in B-mode and a 5-MHz scanning frequency in pulsed Doppler mode. All subjects were examined in a supine position. The scanning protocol included imaging of the right and left common (proxi-mal and distal segments) and internal carotid arteries (bulbous and distal segments) [19 – 22] and of the femoral arteries 40 mm proximal and 10 mm distal to the bifurcation into the superficial and deep branches. Pulsed Doppler was used to provide information on blood flow velocity and to identify the different arteries. Atherosclerotic lesions were defined by two ultrasound criteria: [1] wall surface (protrusion into the lumen or roughness of the arterial boundary) and (2) wall texture (echogenicity). The maximum axial diameter of the plaque was measured as the distance from the leading edge of the lumen-intima interface to the leading edge of the media-adventitia interface. As detailed previously
[20], an atherosclerosis score was calculated by adding the diameters of plaques (in millimeters) at each imag-ing site in the carotid arteries. Rescannimag-ing was per-formed in 1995 using the same ultrasound protocol. Incident carotid atherosclerosis was defined by the oc-curence of new plaque in previously normal segments. All the ultrasound methods applied were highly repro-ducible (for details see references [21,22]).
2.6. Statistical analysis
The association of carotenoid plasma concentrations with demographic characteristics and potential vascular risk factors was analyzed by means of Pearson’s corre-lation coefficients and analysis of variance. The associa-tion between carotenoid levels and ultrasonographic outcome measures (prevalent carotid and/or femoral artery atherosclerosis, incident carotid atherosclerosis) was examined by logistic regression analysis, with the hypothesis test based on likelihood ratio statistics. a+ b-carotene (sum of alphacarotene and betacarotene) concentrations were modeled either as a continuous variable or as a set of indicator variables. Multivariate logistic regression models were constructed with a for-ward stepwise selection procedure using standard inclu-sion and excluinclu-sion criteria (P1 B0.05;PE\0.10).
3. Results
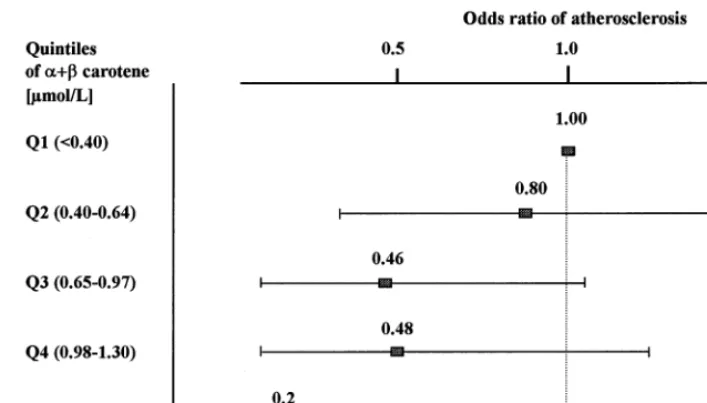
Proportions and mean values of selected demo-graphic parameters, vascular risk factors and carotenoid plasma concentrations are given in Tables 1 and 2; Fig. 1. Levels of a-carotene, b-carotene and cryptoxanthin were significantly higher in women. An-tioxidant concentrations did not show clear age trends (P\0.05, each). Notably,a- andb-carotene levels were reduced by half in heavy smokers and drinkers (Table 3). Two-factorial analysis of variance demonstrated that effects of smoking and alcohol consumption were at least in part independent of each other (P=0.005 and 0.034). Relationships with other vascular risk fac-tors are summarized in Table 4.
A.D’Odorico et al./Atherosclerosis153 (2000) 231 – 239 234
atherosclerosis according to quintiles ofa+b-carotene. This graph shows a gradual decrease in atherosclerosis risk with increasing carotene levels (P value for linear trend, 0.0049). Split analyses in genders, in smokers and non-smokers, and in abstainers and regular alcohol consumers all yielded consistent relations between atherosclerosis anda+b-carotene levels (data not pre-sented). Thus, alcohol consumption and cigarette smok-ing neither confounded nor modified the association obtained. Other carotenoids did not significantly pre-dict the risk of atherosclerosis. This finding applied to all subfractions (cryptoxanthin, etc.) and to their sum (‘other carotenoids’). Likewise, retinol and a -tocopherol were unrelated to atherosclerosis in our population (Table 5) as was the a-tocopherol/ choles-terol ratio.
4. Discussion
Oxidative modifications of LDL are widely accepted to represent a key event in lipid-induced atherogenesis. The efficacy of lipid peroxidation depends on LDL composition, residence time of LDL in the sub-en-dothelial space and, most important, the balance of pro-oxidants involving ferrous iron [19] and antioxi-dants. Carotenoids, a group of lipid-soluble pro-vita-mins contained in LDL particles, are experimentally well-founded to protect against lipid peroxidation [24 – 26]. b-carotene represents 25 – 50% of total carotenoids and may be the fraction with the most pronounced antioxidant effects [27].
The current population study is the first to demon-strate a strong inverse association between a+b -carotene plasma levels and the prevalence of atherosclerosis in carotid and femoral arteries. This association was internally consistent in genders and across the whole age range (45 – 65 years) and emerged as independent of other vascular risk factors. It was particularly relevant to cigarette smokers and heavy drinkers, whose a+b-carotene levels were markedly reduced (Table 3). As for other carotenoids, we ob-served a tendency towards lower atherosclerosis risk in subjects with high plasma levels, though statistical sig-nificance was not achieved.
To the best of our knowledge, there is only one previous epidemiological study addressing the potential protective effects of carotenoids on atherogenesis. This study attempted to quantify nutritional carotene intake and revealed an inverse association of this variable with early stages of carotid atherosclerosis in men [28]. A protective role of carotene in atherogenesis is further substantiated by an animal model [4] and various stud-ies on symptomatic coronary artery disease: With a few exceptions [10,13] low plasma b or total carotene pre-dicted an increased cardiovascular risk [9,11,12,29]. In-tervention trials, however, exhibited effects of a regular intake of 20 – 50 mg of synthetic b-carotene on cardio-vascular risk and mortality that were at times beneficial [30,31], at others non-existent [32] or even unfavorable [33,34]. Several clues to explain this discrepancy may be inferred from the inconsistencies observed between and within observational and interventional studies. i) Plasma antioxidant concentrations are the result of long-term dietary habits. In clinical intervention trials the period of antioxidant supplementation may be too short for lipid-soluble antioxidants to accumulate in the lipid core of plaques [14]. ii) Commercial supplements of b-carotene were higher in the trans- than in the cis-isomer, whereas natural b-carotene showed an op-posite ratio. Recently, the nine-cis form of b-carotene was shown to have a higher antioxidant capacity in vitro [35] and in vivo [36]. Furthermore, the ability of these isomers to accumulate in the lipid core of Table 1
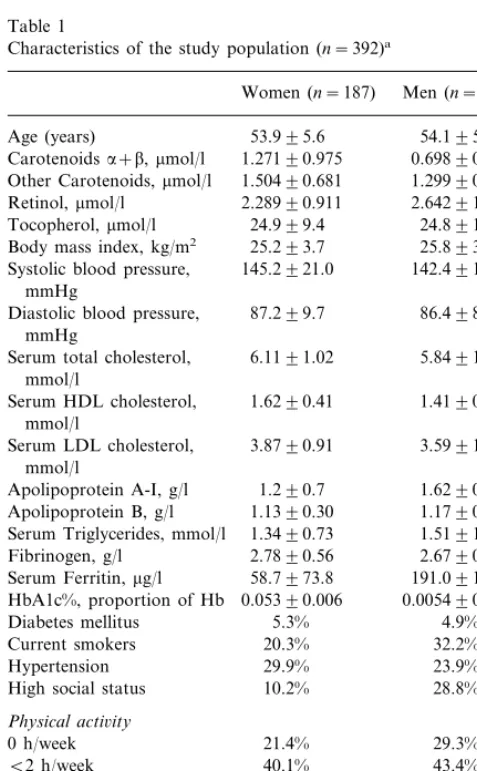
Characteristics of the study population (n=392)a
Women (n=187) Men (n=205)
Other Carotenoids,mmol/l 1.50490.681 1.29990.492 Retinol,mmol/l 2.28990.911 2.64291.039 Systolic blood pressure, 145.2921.0
mmHg
87.299.7
Diastolic blood pressure, 86.498.3 mmHg
5.8491.02 Serum total cholesterol, 6.1191.02
mmol/l
Serum HDL cholesterol, 1.6290.41 1.4190.40 mmol/l
3.5991.07 Serum LDL cholesterol, 3.8790.91
mmol/l
1.6290.27 1.290.7
Apolipoprotein A-I, g/l
1.1790.32 Apolipoprotein B, g/l 1.1390.30
1.3490.73
Serum Triglycerides, mmol/l 1.5191.04 2.6790.59 Fibrinogen, g/l 2.7890.56
Serum Ferritin,mg/l 58.7973.8 191.09176.1 0.05390.006 0.005490.007 HbA1c%, proportion of Hb
5.3%
Diabetes mellitus 4.9%
20.3%
Current smokers 32.2%
Hypertension 29.9% 23.9%
High social status 10.2% 28.8%
Physical acti6ity
0 h/week 21.4% 29.3%
D
’
Odorico
et
al
.
/
Atherosclerosis
153
(2000)
231
–
239
235
Mean values9SD of serum Retinol,a-tocopherol and carotenoids in men and women aged 45–64 years
Lutein (mmol/l) Zeaxanthin
Retinol a-Tocopherol Cryptoxanthin
Age (years) Lycopene a-carotene b-carotene
(mmol/l) (mmol/l)
(mmol/l)
(mmol/l) (mmol/l) (mmol/l) (mmol/l)
Men
0.3190.13 0.0990.03 0.2190.14 0.6690.35 0.1290.13 0.5990.47
2.8790.92 24.0910.4 45–49
0.2990.22 0.5890.28 0.1390.13 0.6490.36
0.1090.06
50–54 2.5090.93 20.698.80 0.3390.15
0.1090.05
55–59 2.5890.93 22.099.57 0.3690.20 0.2290.15 0.6790.38 0.1190.11 0.5890.40
0.2390.17
60–64 2.5191.22 19.8914.6 0.3590.19 0.1090.05 0.5390.34 0.0990.06 0.5490.30
Women
0.3190.21 0.7690.49 0.2490.36
2.1490.81 1.1590.91
45–49 20.698.70 0.3790.21 0.0990.06
0.3690.15 0.1090.05 0.3690.19 0.7190.29 0.1990.17 1.1190.67
2.3690.95 21.899.08 50–54
0.3690.21 0.6690.33 0.1990.32 1.1190.81
55–59 2.3590.91 23.498.98 0.3890.20 0.1090.08
0.3790.27 0.6290.42 0.1390.09 0.9590.68
0.1090.05 0.3990.17
60–64 2.3291.00 24.1911.4
0.772
Pvalue for sex B0.001 0.704 0.070 B0.001 0.038 B0.001 B0.001
A.D’Odorico et al./Atherosclerosis153 (2000) 231 – 239 236
Fig. 1. Risk of carotid and femoral artery atherosclerosis according to quintiles ofa- andb-carotene (n=392) Odds ratios of carotid and femoral atherosclerosis decreased with increasing plasmaa+b-carotene concentrations. The horizontal bars represent 95% confidence intervals.
Table 3
Mean plasma values of antioxidant according to various categories of cigarette smoking and alcohol consumption (n=392)a
Cigarette smoking (number of cigarettes/day)
Antioxidant 0 1–10 11–20 \20 Pvalueb
2.3990.96
Retinol (mmol/l) 2.8790.83 2.4290.91 2.8791.24 0.230
30.1910.0 23.798.05
24.290.37 27.0910.7
a-Tocopherol (mmol/l) 0.015
1.4691.70 0.7090.43 0.6890.86
a+bCarotene (mmol/l) 1.0190.70 0.022
1.5490.60 1.2990.54 1.2290.56
1.4290.67 0.287
Other carotenoids (mmol/l)
Alcohol consumption (g/day)
1–10
Antioxidant 0 11–20 \20 Pvaluea
2.4890.95
Retinol (mmol/l) 2.2490.90 2.9391.12 2.9190.17 0.011
24.799.73 27.3913.2
23.998.73 26.9914.5
a-Tocopherol (mmol/l) 0.086
1.0690.81 0.6090.42 0.4090.03
a+bCarotene (mmol/l)1.0890.88 1.0890.88 0.013
1.4590.70 1.2590.55 1.2090.61
1.4190.59 0.341
Other carotenoids (mmol/l)
aValues are mean9SD.
bPvalues for differences of antioxidant levels across smoking or alcohol categories after adjustment for age and sex.
Table 4
Correlation of plasma antioxidants levels with vascular risk factors
Variables Retinol a-Tocopherol Carotenoidsa+b Other Carotenoids
Women Men Women Men Women Men
Men Women
0.08 −0.02 0.13
Age −0.11 −0.09 −0.13 −0.04 −0.03
Total cholesterol 0.15 0.10 0.32* 0.24* 0.01 −0.07 0.19 0.01
−0.26* 0.33* 0.23*
Triglycerides 0.17 −0.24* −0.20 −0.09 −0.07
0.17 0.14 0.08 −0.28*
0.16 −0.21
Serum ferritin −0.12 −0.13
−0.2
Systolic BP −0.03 0.09 −0.01 −0.09 −0.10 −0.03 −0.13
−0.02 0.02 0.03 −0.19 −0.11 0.01 −0.08
C-reactive protein −0.02
0.00 −0.03 0.06 −0.16
−0.07 −0.17
Fibrinogen −0.10 −0.13
−0.11 0.13 −0.06 −0.17
Body mass index 0.03 −0.23* −0.02 −0.24*
0.17 0.08 0.11 −0.32*
0.17 0.04
Alcohol g/day −0.14 0.15
Physical activity −0.03 −0.04 −0.05 0.01 0.11 0.09 0.02 0.09
0.04 −0.05 0.09 −0.10
−0.12 −0.21
HbA1c −0.15 −0.07
atherosclerotic plaque may differ and awaits future clarification.
Our study failed to obtain a significant relation be-tween plasma concentrations of vitamin E and atherosclerosis. In the EVA study, in contrast, erythro-cyte vitamin E was negatively associated with common carotid artery intima-media thickness in elderly volun-teers (59 – 71 years) [18]. In addition, there is limited epidemiological evidence from the ARIC study to show that high nutritional intake of a-tocopherol protects against carotid atherosclerosis [28]. Studies of the asso-ciation between vitamin E intake/levels and onset of cardiovascular disease yielded contradictory results [5,6,8,10,12,13,37 – 39].
There are several potential reasons for the inconsisten-cies in the results of the above studies: 1) The method of vitamin E determination was highly variable. The EVA study measured erythrocyte vitamin E, which reflects long-term dietary intake better than do plasma concentrations. Other surveys attempted to quantify vitamin E content in nutrition as a surrogate of the actually important plasma levels. 2) Levels of vitamin E in various populations are highly variable based upon differences in diet. Likewise, distinct proportions of subjects have plasma levels low or high enough to be protective or deleterious. In the urban population of India [10], in whom low vitamin E significantly predicted an increased risk of cardiovascular disease, meana
-toco-pherol was 40% lower than in Bruneck. The Basel study in turn accorded with our survey in that the plasma concentration of vitamin E were usually high and a protective role of a-tocopherol could not be demon-strated [9]. Lack of significant associations in this and in our survey may be due to the low variation in vitamin E concentration and does not rule out the possibility of consistently high vitamin E levels contributing to a generally low rate of atherosclerosis in these populations. 3) Recently, vitamin E has been reported to exert antioxidant, neutral or even prooxidant (‘tocopherol-me-diated peroxidation’) activities, depending on the pres-ence of compounds which have not yet been fully characterized [40]. This finding may contribute to the inconsistencies in the results of previous surveys.
The merits of the current study include its randomized recruitment strategy encompassing men and women and the measurement of atherosclerosis in various vascular territories. All plasma sampling was performed within a limited time, between July and early October. Concentrations of antioxidants obtained are thus not subject to seasonal variations. Because samples were immediately processed and stored at −70°C for 3 months, variable storage conditions are unlikely to confound the results. The main weakness of the current analysis is the simultaneous assessment of antioxidant levels and atherosclerosis in the carotid and femoral arteries. However, plasma levels of carotenoids reflect
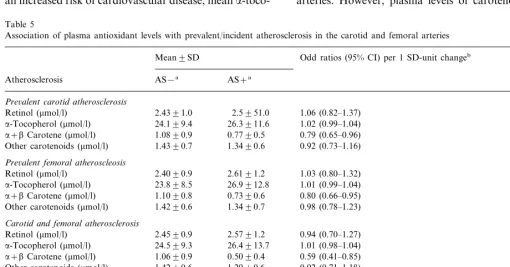
Table 5
Association of plasma antioxidant levels with prevalent/incident atherosclerosis in the carotid and femoral arteries
Pvalue Odd ratios (95% CI) per 1 SD-unit changeb
Mean9SD
AS−a
Atherosclerosis AS+a
Pre6alent carotid atherosclerosis
2.4391.0
Other carotenoids (mmol/l)
Pre6alent femoral atheroscleosis
2.4090.9 2.6191.2 0.81
Carotid and femoral atherosclerosis
0.94 (0.70–1.27)
Other carotenoids (mmol/l) 0.92 (0.71–1.18) 0.48
Incident carotid atherosclerosis
Other carotenoids (mmol/l) 0.30
aAS−, no prevalent or incident atherosclerosis; AS+prevalent or incident atherosclerosis.
bOdds ratio were derived from logistic regression analysis of prevalent/incident atherosclerosis on antioxidants and covariates (age, sex, LDL
A.D’Odorico et al./Atherosclerosis153 (2000) 231 – 239 238
long-term dietary habits that proved consistent in the Bruneck population over a longer period. When 1995 plasma levels were used as a surrogate for the 1990 levels and the analysis was repeated with a prospective design, the results were virtually unchanged (Table 5). In this context it is important to note that the inherent assessment variability of this ‘prospective’ approach may tend to bias results towards a null association but does not create spurious association. Theoretically, an artificial relation could emerge when atherosclerosis per se affects carotene levels. At this time, however, there are no data to support such a conjecture. As a further limit of our study (and of all previous epidemiological surveys in this field) it can not be ruled out that high carotene concentration acts as a marker of other ingre-dients of fruits and vegetables or of a healthy life style, rather than being protective in itself.
In conclusion, our study is among the first to docu-ment an inverse association between plasma levels ofa -and b-carotene and the risk of atherosclerosis in vari-ous vascular territories. It provides further support for the hypothesis that antioxidants protect against atherosclerosis and arterial disease and intends to stim-ulate further research efforts in this field.
Acknowledgements
We are grateful to Milena Minotto, Daniela Pizzuti and Carla Pasini Venturi for technical assistance and support. The study was supported by a grant from the Italian National Research Council (CNR), Progetto finalizzato FATMA.
References
[1] Steinberg D, Parathasarathy S, Carew TE, Khoo JC, Witztum JL. Beyond cholesterol: modifications of low-density lipoprotein that increase its atherogenicity. N Engl J Med 1989;320:915 – 24. [2] Ross R. The pathogenesis of atherosclerosis: a perspective for
the 1990s. Nature 1993;362:801 – 9.
[3] Witztum JL. The oxidation hypothesis of atherosclerosis. Lancet 1994;344:793 – 5.
[4] Shaish A, Daugherty A, O’Sullivan F, Shonfeld G, Heinecke JW. Beta-carotene inhibits atherosclerosis in hypercholes-terolemic rabbits. J Clin Invest 1995;96:2075 – 82.
[5] Bellizzi MC, Franklin MF, Duthie GG, James WP. Vitamin E and coronary heart disease: the European paradox. Eur J Clin Nutr 1994;48:822 – 31.
[6] Knekt P, Reunanen A, Jarvinen R, Seppanen R, Heliovaara M, Aromaa A. Antioxidant vitamin intake and coronary mortality in a longitudinal population study. Am J Epidemiol 1994;139:1180 – 9.
[7] Pandey DK, Shekelle R, Selwyn BJ, Tangney C, Stamler J. Dietary vitamin C and beta-carotene and risk of death in middle-aged men: the Western Electric Study. Am J Epidemiol 1995;142:1269 – 78.
[8] Kushi LH, Folsom AR, Prineas RJ, Mink PJ, Wu Y, Bostick RM. Dietary antioxidant vitamins and death from coronary heart disease in postmenopausal women. New Engl J Med 1996;334:1156 – 62.
[9] Gey KF, Stahelin HB, Eichholzer M. Poor plasma status of carotene and vitamin C is associated with higher mortality from ischemic heart disease and stroke: Basel Prospective Study. Clin Investig 1993;71:3 – 6.
[10] Singh RB, Ghosh S, Niaz MA, Singh R, Beegum R, Chibo H, Shoumin Z, Postiglione A. Dietary intake, plasma levels of antioxidant vitamins, and oxidative stress in relation to coronary artery disease in elderly subjects. Am J Cardiol 1995;76:1233 – 8. [11] Morris DL, Kritchevsky SB, Davis CE. Serum carotenoids and coronary heart disease: the Lipid Research Clinics Coronary Primary Prevention Trial and Follow-up Study. J Am Med Assoc 1994;272:1439 – 41.
[12] Street DA, Comstock GW, Salkeld RM, Schuep W, Klag MJ. Serum antioxidants and myocardial infarction. Are low levels of carotenoids and alpha-tocopherol risk factors for myocardial infarction? Circulation 1994;90:1154 – 61.
[13] Riemersma RA, Wood DA, Macintyre CC, Elton RA, Gey KF, Oliver MF. Risk of angina pectoris and plasma concentrations of vitamin A, C, and E and carotene. Lancet 1991;337:1 – 5. [14] Steinberg D. Clinical trials of antioxidants in atherosclerosis: are
we doing the right thing? Lancet 1995;346:36 – 8.
[15] Dowd P, Zheng ZB. On the mechanism of the anticlotting action of vitamin E quinone. Proc Natl Acad Sci 1995;92:8171 – 5. [16] Calzada C, Bruckdorfer KR, Rice-Evans CA. The influence of
antioxidant nutrients on platelet function in healthy volunteers. Atherosclerosis 1997;128:97 – 105.
[17] Keaney JF, Simon DI, Freedman JE. Vitamin E and vascular homeostasis: implications for atherosclerosis. FASEB J 1999;13:965 – 76.
[18] Bonithon-Kopp C, Coudray C, Berr C, Touboul PJ, Fe`ve JM, Favier A, Ducimetie`re P. Combined effects of lipid peroxidation and antioxidant status on carotid atherosclerosis in a population aged 59 – 71 years: the EVA study. Am J Clin Nutr 1997;65:121 – 7.
[19] Kiechl S, Willeit J, Egger G, Poewe W, Oberhollenzer F. Body iron stores and the risk of carotid atherosclerosis: prospective results from the Bruneck study. Circulation 1997;96:3300 – 7. [20] Willeit J, Kiechl S. Prevalence and risk factors of asymptomatic
extracranial carotid artery atherosclerosis: a population-based study. Arterioscler Thromb 1993;13:661 – 8.
[21] Kiechl S, Willeit J. The natural history of atherosclerosis. Part I: Incidence and progression. Arterioscler Thromb Vasc Biol 1999;19:1484 – 90.
[22] Kiechl S, Willeit J. The natural history of atherosclerosis. Part II: vascular remodeling. Arterioscler Thromb Vasc Biol 1999;19:1491 – 8.
[23] Kiechl S, Willeit J, Egger Oberhollenzer M, Aichner F. Alcohol consumption and carotid atherosclerosis: evidence of dose-de-pendent atherogenic and antiatherogenic effects: results from the Bruneck study. Stroke 1994;25:1593 – 8.
[24] Lowe GM, Bilton RF, Young AJ, Graham JM, Ford TC, Billington D. Carotenoid profiles of human plasma lipoproteins. Biochem Soc Trans 1996;24:171S.
[25] Abbey M, Nestel PJ, Baghurst PA. Antioxidant vitamins and low-density lipoprotein oxidation. Am J Clin Nutr 1993;58:525 – 32.
[26] Jialal I, Norkus EP, Cristol L, Grundy SM. Beta-carotene inhibits the oxidative modification of low-density lipoprotein. Biochim Biophys Acta 1991;1086:134 – 8.
[27] Parker RS. Carotenoids in human blood and tissues. J Nutr 1989;119:101 – 4.
[29] Kardinaal AF, Kok FJ, Ringstad J, et al. Antioxidants in adipose tissue and risk of myocardial infarction: the EURAMIC study. Lancet 1993;342:1379 – 84.
[30] Blot WJ, Li JY, Taylor PR, et al. Nutrition intervention trials in Linxian, China: supplementation with specific vitamin/mineral combinations, cancer incidence, and disease-specific mortality in the general population. J Natl Cancer Inst 1993;85:1483 – 92. [31] Gaziano JM, Hennekens CH. Antioxidant vitamins in the
pre-vention of coronary artery disease. Cont Int Med 1995;7:9 – 14.
[32] Hennekens CH, Buring JE, Manson JE, et al. Lack of effect of long-term supplementation with beta carotene on the incidence of malignant neoplasms and cardiovascular disease. New Engl J Med 1996;334:1145 – 9.
[33] Alpha-Tocopherol, Beta carotene Cancer Prevention Study Group. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. New Engl J Med 1994;330:1029 – 35.
[34] Omenn GS, Goodman GE, Thornquist MD, et al. Effects of a
combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N Engl J Med 1996;334:1150 – 5. [35] Levin G, Mokady S. Antioxidant activity of 9-cis compared to
all-trans beta-carotene in vitro. Free Radic Biol Med 1994;17:77 – 82.
[36] Ben-Amotz A, Levy Y. Bioavailability of a natural isomer mixture compared with synthetic all-trans beta-carotene in hu-man serum. Am J Clin Nutr 1996;63:729 – 34.
[37] Stampfer MJ, Hennekens CH, Manson JE, Colditz GA, Rosner B, Willett WC. Vitamin E consumption and the risk of coronary disease in women. N Engl J Med 1993;328:1444 – 9.
[38] Rimm EB, Stampfer MJ, Ascherio A, Giovannucci E, Colditz GA, Willett MC. Vitamin E consumption and the risk of coro-nary heart disease in men. N Engl J Med 1993;328:1450 – 6. [39] Spencer AP, Carson DS, Crouch MA. Vitamin E and coronary
artery disease. Arch Intern Med 1999;159:1313 – 9.
[40] Upston JM, Terentis AC, Stocker R. Tocopherol-mediated per-oxidation of lipoproteins: implications for vitamin E as a poten-tial antiatherogenic supplement. FASEB J 1999;13:977 – 94.