BALI INFECTIOUS DISEASE
SYMPOSIUM 11 & BALI TRAVEL
MEDICINE SYMPOSIUM 2
"Fight Infection and Save Your Patients!”
HARRIS HOTELS Jln. H.O.S. Cokroaminoto 23-25 Denpasar-Bali 16 November 2019
Penyakit tropis dan infeksi masih menjadi masalah kesehatan global termasuk di Indonesia. Dalam sau dekade penyelenggaraan Bali Infectious Diseases, terekam pula perkembangan penyakit infeksi; temuan agen penyebab infeksi, perkembangan keilmuan terkait patogenesis dan tatalaksana penyakit Klinisi dipacu untuk mampu mengimplementasikan temuan berbasis bukti ke dalam layanan paripurna.
Perubahan iklim dan cuaca disertai arus mobilisasi yang tinggi mengubah pemetaan penyakit infeksi menjadi masalah global yang dihadapi semua negara di belahan dunia. Eradikasi penyakit infeksi dipersulit dengan munculnya penyakit infeksi baru (emerging disease), kembalinya penyakit menular lama (re-emerging disease), dan penyakit infeksi yang sulit dieradikasi (intractable infectious diseases).
Tantangan besar bagi praktisi kesehatan adalah untuk selalu up to date dan berkualitas. Kebutuhan ini harus didukung oleh sarana edukasi berkelanjutan yang mampu memberikan informasi terkini di bidang penyakit tropic dan infeksi serta travel medicine. Tahun ini genap terhitung 11 tahun sudah penyelenggaraan Bali Infectious Disease Symphosium yang berlangsung setiap tahun, oleh karena itu, divisi Penyakit Tropik dan Infeksi, Bagian Ilmu Penyakit Dalam Fakultas Kedokteran / RSUP Sanglah sekaligus memperingati 11 tahun penyelenggaraan BIDs, akan menyelenggarakan Bali Infectious Disease Symposium 11 (BIDS – 11)/ Bali Travel Medicine Symphosium 2 (BTMS-2).
Kegiatan berupa seminar yang dirancang dengan talk show dan diskusi real case based ini diharapkan mampu menjadi ajang diskusi dan pengayaan keilmuan di bidang penyakit tropik, infeksi, dan travel medicine.
Denpasar, November 2019 Ketua Panitia BIDS-11/BTMS-2
EDITORS
Prof. Dr. dr. K Tuti Parwati Merati, SpPD-KPTI, FINASIM dr. AAA.Yuli Gayatri, SpPD-KPTI, FINASIM Dr. dr. I Ketut Agus Somia, SpPD-KPTI, FINASIM
dr. I Made Susila Utama, SpPD-KPTI, FINASIM dr. Ni Made Dewi Dian Sukmawati, SpPD, FINASIM
Panitia Pengarah : Dekan Fakultas Kedokteran Universitas Udayana
Direktur RSUP Sanglah Denpasar
Kepala Departemen/KSM Penyakit Dalam FK Unud/RSUP Sanglah
Kepala Departemen/KSM Penyakit Dalam FK Unud/RSUP Sanglah
Kepala Divisi Penyakit Tropik dan Infeksi Departemen/KSM Penyakit Dalam FK Unud/RSUP Sanglah
Panitia Pelaksana
Ketua : dr. Made Susila Utama, SpPD-KPTI
Sekretaris : dr. Anak Agung Ayu Yuli Gayatri, SpPD-KPTI
Wakil sekretaris : dr. Dewi Dian Sukmawati, SpPD
Bendahara : Dr.dr. I Ketut Agus Somia, SpPD-KPTI
PIC Residen: dr. IGNG Bayu Prawira Putra
Sie Acara: dr. Karlina Isabella
Sie Perlengkapan, Akomodasi dan transportasi:
dr. Komang Triyanayasa
Sie Ilmiah:
Prof. Dr. dr. Tuti Parwati, SpPD-KPTI Dr. dr. I Ketut Agus Somia, SpPD-KPTI dr. I Made Susila Utama, SpPD-KPTI dr. A.A.Ayu Yuli Gayatri, SpPD-KPTI dr. Dewi Dian Sukmawati, SpPD dr. Cokorda Paramadika
Sie Dana
dr. Saraswati Laksmi Dewi
Sie Registrasi
KATA PENGANTAR KONTRIBUTOR DAFTAR ISI JADWAL ACARA
PREPARING THE TRAVELERS : PRE AND POST TRAVEL CONSULTATION
Prof. Dr. dr. Ketut Tuti Parwati Merati, SpPD-KPTI, FINASIM
1
ROLE OF INFECTION BIOMARKERS IN DIAGNOSTIC AND MANAGEMENT OF PATIENTS
dr. Anak Agung Ayu Yuli Gayatri, SpPD-KPTI, FINASIM
11
CLINICAL APPROACH IN MANAGING FEVER OF UNKNOWN ORIGIN
dr. I Made Susila Utama, SpPD-KPTI, FINASIM
26
HUMAN LEPTOSPIROSIS: CURRENT CONCEPT AND UP-DATE MANAGEMENT
Prof. dr. Hussein Gassem, SpPD-KPTI, PhD
35
MANAGING CLOSTRIDIUM DIFFICILE INFECTION AND THE PREVENTION APPROACH
Dr. dr. I Ketut Agus Somia, SpPD-KPTI, FINASIM
41
COMPREHENSIVE CARE FOR TRAVELERS WITH SPECIFIC CONDITIONS
dr. Ni Made Dewi Dian Sukmawati, SpPD, FINASIM
49
HYPERBARIC THERAPY: BEYOND THE DECOMPRESSION ILLNESS TREATMENT
dr. Anita Devi, M.Kes
11)/ BALI TRAVEL MEDICINE SYMPHOSIUM 2 (BTMS-2) FK UNUD/RSUP SANGLAH, 16 NOVEMBER 2019 Sabtu, 16 November 2019
Tempat : Harris Hotel Jln Cokroaminoto st no.23-25, pemecutan kaja, Denpasar Utara, Kota Denpasar, Bali
WAKTU (WITA) ACARA
08.00 – 08.30 PEMBUKAAN
08.30 – 09.00 Plenary Lecture I
What are the causes of Acute Febrile Illness? Lesson Learned from AFIRE Study
09.00 – 09.30 Plenary Lecture II
Preparing the travelers : Pre And Post Travel Consultation
09.30 – 09.45 COFFEE BREAK
SIMPOSIUM I
09.45 – 10.15 Role of Infection markers in diagnostic and management of patients
10.15 – 11.45 Clinical Approach in managing Fever of Unknown Origin
11.45 – 12.00 DISKUSI
12.00 – 13.00 LUNCH
SIMPOSIUM 2
13.00 – 13.30 Leptospirosis: current concept and management update
13.30 – 14.00 Managing Clostridium Difficile Infection and the prevention approach
14.00 – 14.20 DISKUSI
14.50 – 15.20 Hyperbaric Therapy: beyond the Decompression Illness Treatment
15.20 – 15.40 DISKUSI
PREPARING THE TRAVELERS : PRE AND POST TRAVEL
CONSULTATION
Tuti Parwati Merati Pendahuluan
Kedokteran wisata atau Travel Medicine adalah ilmu kedokteran yang menangani masalah pencegahan dan penanganan penyakit yang berhubungan dengan travel atau perjalanan. Kedokteran wisata merupakan bagian ilmu kedokteran yang unik, karena bersifat multidisiplin yang pada umumnya berusaha mencegah terjadinya risiko perjalanan pada wisatawan, baik risiko infeksi maupun non-infeksi. Bidang ini terutama mempelajari ilmu kedokteran pencegahan, mempelajari epidemiologi berbagai penyakit infeksi di berbagai belahan dunia termasuk penanganannya, dan memberikan tata cara penanganan penyakit oleh yang bersangkutan (self-therapy). Pelayanan kedokteran wisata yang ideal merupakan suatu rangkaian pelayanan yang berkesinambungan, mulai dari pra-wisata (persiapan sebelum wisata), selama didaerah wisata, dan setelah kembali dari wisata (pasca wisata).
Kedokteran wisata menjadi sangat penting sebagai respons terhadap peningkatan arus perjalanan internasional diseluruh dunia. Ilmu ini berkembang menjadi sangat kompleks sebagai akibat perubahan yang dinamis pada epidemiologi penyakit infeksi, resistensi obat dan meningkatnya orang dengan penyakit kronik yang menjadi wisatawan. Kedokteran wisata menjadi semakin penting karena pola epidemilogi penyakit di berbagai Negara tidak sama, dapat berubah setiap saat, munculnya wabah penyakit infeksi baru (new emerging infectious diseases) sehingga dengan adanya globalisasi, risiko mendapat penyakit tersebut semakin meningkat, terutama pada orang yang bepergian atau wisatawan.
Konsultasi pra-wisata bertujuan untuk mempersiapkan wisatawan sebelum keberangkatannya, konsultasi pasca-wisata
bertujuan mengidentifikasi dan menangani masalah yang dihadapi pasca wisata.
Konsultasi pra-wisata
Konsultasi sebaiknya dilakukan 4 – 8 minggu sebelum keberangkatan, terutama untuk wisata jangka panjang.
Konsultasi pra wisata intinya adalah tiga hal : 1. Melakukan penilaian risiko individual.
2. Memberi informasi dan edukasi tentang risiko perjalanan dan cara mencegahnya.
3. Memberikan vaksinasi dan obat profilaksis. Apa yang dimaksud dengan risiko ?
Risiko yang dimaksud disini adalah kemungkinan terjadinya penyakit, trauma fisik atau mental, kecelakaan, gangguan keamanan atau malah kematian yang dapat terjadi sebagai konsekuensi perjalanan itu sendiri dan bisa terjadi selama perjalanan/wisata atau pasca perjalanan. Menurut Steffen (1994), the art of travel medicine adalah dalam memilih strategi pencegahan yang penting tanpa menimbulkan efek samping yang tidak perlu, termasuk biaya dan ketidak nyamanan wisatawan.
Untuk dapat membuat rekomendasi bagi calon wisatawan, ada empat komponen yang perlu dibahas saat konsultasi pra-wisata, sebagai berikut:
• Destinasi : daerah atau negara tujuan wisata,penyakit-penyakit apa yang terdapat di negara tujuan, bagaimana risiko penyakit itu dan hal-hal lain yang mungkin terdapat didaerah destinasi. Durasi tinggal di daerah destinasi juga mempengaruhi risiko.
• Transportasi : Apakah ada risiko pada wisatawan bila bepergian dengan pesawat udara, perjalanan darat dengan mobil atau kapal laut.
• Akomodasi : Apakah penginapan bagi wisatawan dapat melindungi dari kemungkinan paparan yang mungkin berbahaya
bagi mereka. Apakah tersedia upaya dan prosedur pencegahan terjadinya risiko atau apakah berisiko bagi orang lanjut usia, bayi, anak2 atau orang cacat.
• Aktifitas didaerah tujuan wisata: Wisatawan dengan aktifitas berbeda akan menghadapi risiko berbeda, sebagai contoh, wisatawan yang mengikuti kegiatan didalam ruangan mempunyai risiko berbeda dari wisatawan yang beraktifitas di luar atau di alam terbuka. Kemungkinan terjadi kontak erat dengan penduduk setempat, olah raga atau kendaraan yang berisiko terjadi kecelakaan, minum minuman beralkohol yang mungkin menyebabkan kurang pengendalian diri dan perilaku. Ketersediaan air bersih, kebersihan makanan dan minuman, dan ketersediaan fasilitas kesehatan termasuk vaksinasi didaerah tujuan wisata
Membuat rekomendasi calon wisatawan.
Berdasarkan ilmu kedokteran wisata, seorang dokter akan memberikan rekomendasi yang diperlukan seorang calon wisatawan berdasarkan penilaiannya terhadap kondisi kesehatan individu tersebut dan data dari empat komponen penting tersebut diatas.
Wisatawan yang berisiko tinggi
Seseorang mungkin mempunyai risiko lebih tinggi untuk mendapat penyakit saat wisata dibandingkan orang lain, mungkin lebih berisiko untuk menderita penyakit lebih berat atau mempunyai kontraindikasi untuk beberapa jenis vaksin atau obat-obatan. Kelompok risiko tinggi ini adalah: bayi dan anak-anak, orang lanjut usia, wanita hamil, keadaan defisiensi imun, mengidap penyakit kronis ( DM, penyakit kardiovaskuler dan penyakit paru), wisata jangka panjang dan wisatawan yang mengunjungi teman atau keluarga. Mengapa wisatawan yang mengunjungi teman dan keluarga termasuk berisiko tinggi? Dari riwayatnya diketahui bahwa pada umumnya mereka adalah imigran dari negara berkembang ke negara maju, sehingga bila mereka bepergian untuk pulang ke negaranya, akan berisiko tinggi untuk
menderita penyakit akibat wisata, menderita penyakit yang lebih berat, dan umumnya mereka tidak melakukan persiapan yang cukup sebelum keberangkatannya.
Vaksinasi
Terlebih dahulu perlu diketahui pemberian imunisasi rutin sesuai pedoman nasional, terutama untuk calon wisatawan anak-anak. Informasi diberikan sejelas-jelasnya, tentang jenis vaksinasi ( vaksinasi wajib, rutin atau dianjurkan), tujuan imunisasi, jenis patogen (termasuk strain-nya) yang dapat dicegah, daya proteksi (berapa persen sesuai dengan merek vaksin), berapa lama kekebalan yang tercapai, kapan dilakukan booster, dan yang terpenting, apa efek samping yang mungkin terjadi. Catatan lengkap harus dibuat sehubungan dengan vaksin yang diberikan, termasuk merk dan nomor batch, dan pasien diminta untuk menanda tangani informed consent. Vaksin yang perlu diberikan pada wisatawan ditentukan dari pedoman pemberian vaksin pada wisatawan, namun juga tergantung dari riwayat vaksinasi rutin yang telah dilakukan oleh yang bersangkutan. Karena itu perlu diketahui epidemiologi penyakit2 infeksi yang dapat dicegah dengan vaksin, dana yang tersedia, sehingga rekomendasi kita berdasarkan risiko spesifik. Obat profilaksis
Profilaksis terhadap malaria dibuat berdasarkan tinggi rendahnya risiko terhadap paparan malaria di daerah tujuan wisata , namun secara umum juga disarankan menerapkan personal protection (menghindari gigitan nyamuk, tidur memakai kelambu, memakai krem atau lotion anti nyamuk dan pakaian yang dapat melindungi saat beraktifitas). Perlu dijelaskan bahwa semua obat profilaksis tersebut mempunyai kekurangan dan kelebihan masing-masing termasuk efek samping dan efektifitasnya, Karena itu rekomendasi ditujukan spesifik orang perorang. Untuk wisatawan yang bepergian jangka panjang didaerah endemis dengan risiko tinggi, sebaiknya juga diberikan petunjuk cara-cara mengobati sendiri, seandainya akses pelayanan kesehatan tidak
ada atau jauh. Tentunya hal ini harus dilakukan dengan edukasi yang cukup intensif.
Edukasi kesehatan
Isu kesehatan yang diberikan sebagai edukasi ada yang bersifat sebagai pengetahuan umum yang perlu diketahui oleh semua wisatawan, dan isu kesehatan khusus untuk calon wisatawan tertentu. Karena itu penilaian risiko dapat membantu mengarahkan isu mana yang relevan untuk wisatawan tertentu.Pada saat konsultasi, infomasi dan saran diberikan secara singkat dan sederhana sehingga dapat dimengerti oleh calon wisatawan tersebut, disamping itu perlu diberikan juga informasi tertulis (dalam bentuk brosur) secara rinci untuk mengingatkan informasi yang telah diberikan saat konsultasi.
Isu umum yang perlu didiskusikan antara lain adalah cara makan dan minum yang sehat dan aman, masalah diare dan cara penanganannya, menghindari gigitan serangga atau binatang. Hal lain adalah informasi tentang pentingnya pasca wisata untuk memeriksakan diri ke klinik wisata, terutama bila mengalami gejala penyakit, seperti demam, penyakit saluran nafas, saluran pencernaan atau adanya rash pada kulit.
Isu spesifik, tergantung dari orang-perorang, mungkin meliputi masalah vaksinasi, mabuk perjalanan, thrombosis vena profunda, beberapa penyakit infeksi yang mungkin berisiko termasuk infeksi menular seksual (IMS), perilaku seks aman, dan akses terhadap pelayanan kesehatan didaerah tujuan wisata. Mungkin juga tentang pentingnya asuransi, karena tidak jarang masalah ini akan memberi dampak ekonomi yang tidak terduga.
Medikal kit
Medikal kit penting bagi wisatawan, dan isinya disesuaikan dengan kebutuhan wisatawan tersebut. Kebutuhan dasar adalah obat-obat dasar dan pertolongan pertama pada kecelakaan (P3K), seperti pembersih luka, plester, verband, antiseptic, obat tetes mata, repellent, nasal decongestant, oralit, analgesic dan thermometer. Disamping itu
tergantung destinasi wisata, diperlukan obat antidiare, anti malaria, obat penenang, kondom, dan item pribadi yang sering dipakai. Bagi wisatawan yang memerlukan obat-obat yang diminum secara rutin misalnya obat asthma, diabetes, dan sebagainya sebaiknya juga membawa resep dari dokter untuk menunjukkan bahwa obat tersebut diperlukan secara pribadi oleh yang bersangkutan.
Wisatawan dengan kebutuhan khusus
Seperti diketahui, risiko sakit pada wisatawan berkaitan dengan wisatanya akan berbeda-beda. Sekelompok orang yang disebut kelompok risiko tinggi, seperti anak-anak, orang lanjut usia, wanita hamil, orang dengan penyakit kronis, dan orang cacat tubuh akan lebih berisiko dibanding yang lain. Risiko juga berbeda tergantung tujuan dan aktifitas wisata. Kelompok ini semuanya memerlukan informasi dan saran yang khusus meliputi keberadaan pelayanan kesehatan di daerah tujuan wisatanya.
Kehamilan
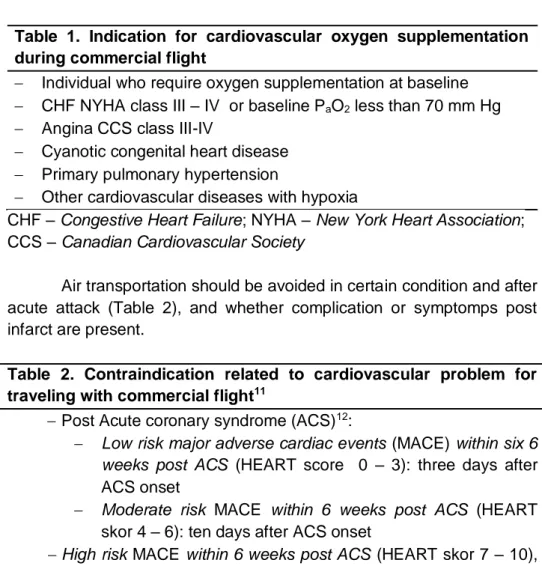
Bagi wanita hamil bepergian secara umum tidak merupakan kontra indikasi, namun ada restriksi sejauh kehamilannya adalah normal, tidak ada komplikasi dan kondisi kesehatannya baik. Maskapai penerbangan memberlakukan pembatasan untuk kehamilan trimester ketiga dan neonatus.
Vaksinasi saat kehamilan juga ada beberapa keterbatasan, disamping itu sangat terbatas ketersediaan jenis obat anti malaria pada kehamilan. Wanita hamil yang terinfeksi malaria berisiko untuk mengalami komplikasi berat, karena itu disarankan bagi wanita hamil untuk tidak melakukan wisata ke daerah endemik semasa hamilnya. Namun jika tidak dapat dihindari, pemberian obat profilaksis dapat dipertimbangkan, dan diberikan sesuai dengan pedoman (lihat pedoman profilaksis malaria pada wisatawan). Pada wanita hamil setiap obat yang diminum harus berdasarkan rekomendasi dokter. Wisata kedaerah pegunungan yang tinggi juga tidak disarankan selama kehamilan.
Cacat tubuh
Cacat tubuh umumnya tidak merupakan kontraindikasi untuk wisata asal keadaan kesehatannya baik. Maskapai penerbangan mempunyai peraturan bagi orang dengan cacat tubuh yang memerlukan bantuan orang lain, informasi bisa didapat sebelumnya dari maskapai penerbangan yang bersangkutan.
Wisatawan yang mengidap penyakit kronik.
Calon wisatawan yang termasuk kelompok ini harus melakukan pemeriksaan dan meminta saran yang berkaitan dengan kedokteran wisata sebelum merencanakan suatu wisata. Beberapa penyakit kronis yang meningkatkan risiko penyakit saat wisata adalah : penyakit epilepsy, penyakit kardiovaskuler, hepatitis, diabetes mellitus, penyakit ginjal kronis yang memerlukan dialysis, penyakit paru kronis, imuno supresi/defisiensi imun, riwayat penyakit tromboembolik, anemia berat, gangguan mental berat dan penyakit kronis yang memerlukan intervensi medis.
Mereka harus membawa obat-obatan yang diperlukan dan biasa diminum selama ini, termasuk membawa resep dengan menggunakan nama generik obat tersebut.
Karena itu untuk setiap penyakit, penilaiannya juga meliputi ketersediaan obat profilaksis, kemungkinan efek samping yang akan terjadi, dan perhatian dari calon wisatawan terhadap masalah tersebut bila berhubungan dengan kesehatan masyarakat, misalnya risiko penularan yang mungkin terjadi.
Pengumpulan informasi yang diperlukan ini dilakukan dengan menanyakan pada calon wisatawan secara terperinci. Oleh karena itu diperlukan check lists yang sangat berguna untuk menjamin bahwa semua informasi yang relevan sudah didapat dan dicatat.
Perlu diberikan kartu pribadi catatan vaksinasi pada wisatawan karena vaksinasi bisa saja diberikan diklinik yang berbeda dan kartu ini disimpan dan dibawa oleh yang bersangkutan. Contoh berikut adalah model check list yang dapat diperbanyak untuk pemakaian pribadi.
Check list konsultasi pra-wisata
Destinasi : risiko yang berkaitan, tipe akomodasi, lama tinggal, ketinggian, keamanan didaerah tersebut dan ketersediaan pelayanan kesehatan local.
Pencegahan: vaksinasi, sebelum keberangkatan, informasi risiko malaria, obat profilaksis, mencegah gigitan nyamuk, serangga atau binatang lain, lotion atau krem anti nyamuk, kelambu, baju lengan panjang, dan sebagainya.
Makanan: kebersihan makanan, makanlah makanan yang sudah dimasak dan bersih, buah-buahan yang ada kulitnya; minumlah minuman yang masih tertutup rapat, kalau ragu-ragu sebaiknya direbus dulu atau minum air dalam botol.
Kecelakaan: Bisa berupa kecelakaan lalu lintas, terjatuh, gigitan binatang (ular atau anjing gila) terbakar matahari, allergi, dll
Pemeriksaan kesehatan sebelum berangkat, pemeriksaan gigi, mata, ginekologi, dsbnya.
Medical kit yang sesuai dengan kebutuhan.
Asuransi wisata : asuransi yang berlaku internasional, baik untuk kecelakaan, sakit, atau medical repatriation
Pasca wisata hendaknya memeriksakan diri ke klinik wisata, terutama bila mengalami gangguan kesehatan
Konsultasi pasca-wisata
Kejadian penyakit infeksi pasca wisata ternyata cukup sering, bervariasi antara 22% - 64%, umumnya terjadi satu bulan setelah kembali dari wisata, walaupun beberapa infeksi dengan masa inkubasi yang panjang mungkin juga terjadi. Sindroma penyakit pasca wisata pada umumnya adalah demam sistemik, keluhan saluran pencernaan seperti diare, keluhan saluran pernafasan, dan rash pada kulit. Demam pada orang yang baru kembali dari perjalanan harus dicari penyebab demamnya, termasuk pemeriksaan hapusan darah untuk kemungkinan malaria. Pertimbangan dalam mencari penyebab demam harus
mengacu pada penyakit-penyakit infeksi setempat, dimana diperkirakan wisatawan tersebut tertular.
Kesimpulan
Konsultasi pra dan pasca-wisata merupakan bagian penting dari Kedokteran Wisata dimana dilakukan konsultasi, edukasi dan pencegahan risiko penyakit yang bertujuan untuk mempersiapkan wisatawan sebelum keberangkatannya, sehingga calon wisatawan dapat mengadakan perjalanan dalam keadaan sehat, mencapai tujuan perjalanannya dan kembali dalam keadaan sehat dan selamat. Dalam konsultasi pra-wisata dilakukan penilaian kondisi kesehatan dan risiko perjalanan, vaksinasi, pemberian profilaksis anti-malaria dan masalah medis lain yang diperlukan. Disamping itu calon wisatawan harus mendapat edukasi karena edukasi adalah unsur terpenting dari proteksi diri. Edukasi diberikan dalam waktu yang cukup, dibantu dengan pemberian materi tertulis dari sumber-sumber informasi seperti brosur, buku-buku, pelayanan telepon, komputer dan bahan edukasi lainnya. Dalam konsultasi pra wisata diberikan juga informasi pentingnya memeriksakan diri pasca-wisata, terutama untuk wisatawan dengan penyakit kronik dan wisatawan dengan durasi wisata cukup lama apabila ada gangguan kesehatan.
Untuk petugas kesehatan yang bergerak dibidang kedokteran wisata pengetahuan yang penting dikuasai adalah medical geography, distribusi dan epidemiologi penyakit infeksi, vaksinasi, pemberian profilaksis; serta kondisi-kondisi tertentu dalam perjalanan, seperti problem ketinggian (high altitude), jet lag, mabuk perjalanan, temperatur tinggi dan sebagainya.
Daftar Pustaka
The Pretravel Consultation – Chapter 2-2018 Yellow Book/Travellers’ Health/CDC http://wwwnc.cdc.gov/travel/yellowbook/2018/the-pre-travel-consultation/the-pre -travel consultation
Jessica K. Fairley.General approach to the returned traveller- Chapter 5-2018 Yellow Book/Travellers’ Health/CDC… .
http://wwwnc.cdc.gov/travel/yellowbook/2018/post-travel- evaluation/general -approach-to-the-returned-traveller
DuPont HL. Steffen R. Travel medicine as a unique medical specialty. In: DuPont HL. Steffen R. Textbook of travel medicine and health. 2nd ed. Hamilton: BC Decker Inc, 2001 : 1-2
ROLE OF INFECTION BIOMARKERS IN DIAGNOSTIC AND
MANAGEMENT OF PATIENTS
Anak Agung Ayu Yuli Gayatri Tropical and Infectious Disease Division
Internal Medicine Department, Faculty of Medicine, Udayana University/ Sanglah Hospital
Introduction
Infectious diseases are categorized as illnesses caused by pathogenic microorganisms such as viruses, bacteria, parasites, or fungi. With more than half of the world population at risk of such fatal illnesses, infectious diseases are classified among the most dangerous threats to the society. Compared with other diseases, infectious diseases can be exponentially transmitted among populations in a relatively short period of time thus threatening the general public health and potentially the economy. It is estimated that over half of the world population are at risk for infectious diseases, making them one of the most dangerous threats to humanity. Therefore, different diagnostic and prognostic tools are needed to help make the most accurate decisions at each moment of patient´s care with suspected infection. Sensitive, specific and rapid diagnostic testing not only paves the way toward effective treatment but also plays a critical role in preventing the transmission of infectious diseases. Timely and accurate diagnosis and antimicrobial treatment is mandatory to improve survival in infectious diseases. However microorganisms can be detected in 30% of blood cultures and it usually takes 48 to 72 hours. While central clinical laboratories offer sensitive and specific assays, such as high-throughput immunoassays and polymerase chain reaction (PCR), they are often time and labor intensive, costly, and dependent on sophisticated instruments and well trained operators. Fortunately, biomarker have significant role in detection of such infections in the early stages is estimated to significantly reduce the mortality rate.1 During the past decades, the development of universal and reliable methods to detect
biomarkers for diagnostics and prognostics of the infectious diseases and the search for highly specific and sensitive biomarkers have been the most important challenges.
Definition
Biological markers (biomarkers) have been defined by Hulka and colleagues1as “cellular, biochemical or molecular alterations that are measurable in biological media such as human tissues, cells, or fluids”. 2 More recently, the definition has been broadened to include biological characteristics that can be objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacological responses to a therapeutic intervention. In practice, biomarkers include tools and technologies that can aid in understanding the prediction, cause, diagnosis, progression, regression, or outcome of treatment of disease
Biomarkers of infection are proteins or components of the immune system that participate in the body's acute response to infection. No tests are currently able to provide perfect diagnostic accuracy for infections. This could lead to over- as well as under-diagnosis. Some tests have been developed that assess the presence of infections by looking for certain of these biomarkers.
Almost all the molecules or cells involved in the infection process of infectious diseases can be used as biomarkers, such as proteins, nucleic acids and antibodies. Unfortunately, no biomarker in infection has proven to have 100% sensitivity and specificity at the same time to establish the diagnosis of an infectious cause in those who suffer some organic failure or indicate when antibiotic treatment should be started or stopped, but their use help to make these decisions with a smaller margin of error. Thus, the main utility of a biomarker is given by its likeli-hood ratios (LR). The LR (+) = Sensitivity / (1 - specificity) and the LR (-) = (1 - sensitivity) / Specificity. For example, when a sepsis is suspected, a useful biomarker will have a high LR (+), which increases the post-test probability supporting the clinical diagnosis.3
Biomarkers can be classified based on their clinical application. In the management of infection, biomarkers have been used or are currently being developed as diagnostic, prognostic, monitoring, surrogate and stratification biomarkers . Diagnostic biomarkers, which can also include screening biomarkers, are used to determine health or disease. Prognostic biomarkers provide information on the likely outcome in an untreated individual and help in establishing the intensity of treatment. Monitoring biomarkers serve to evaluate the disease process and are especially informative of the effectiveness of response to the therapeutic intervention, allowing the clinician to titrate or change the management protocol. A surrogate biomarker is usually an end-point that can be used as an outcome in clinical trials to evaluate safety and effectiveness of therapies instead of measurement of the true outcome of interest. The underlying principle is that changes in the surrogate biomarker follow closely with changes in the outcome of interest. Surrogate biomarkers have the advantage that they may be obtained in a more timely and inexpensive manner than primary end-points such as serious complications and mortality, which require large clinical trials for evaluation. Stratification biomarkers are used to identify a group of patients with shared homogenous biological characteristics and help to select the optimal management for the patients and achieve the best possible outcome in terms of disease category. In the context of management of sepsis, which is a complex and heterogeneous pathologic disease, the use of stratification criteria may also help in effectively characterizing risk groups for inclusion into specific treatments or into clinical trials of new interventions. In the context of infection and sepsis, biomarkers can potentially provide the following additional information:
- Screening & diagnosis - Stratification of severity
Biomarker in screening and diagnostic test
The use of biomarkers for identification of individuals destined to become affected or who are in the “preclinical” stages of the illness. Biomarkers depicting prodromal signs enable earlier diagnosis or allow for the outcome of interest to be determined at a more primitive stage of disease. Blood, urine, and cerebrospinal fluid provide the necessary biological information for the diagnosis. In these conditions, biomarkers are used as an indicator of a biological factor that represents either a subclinical manifestation, stage of the disorder, or a surrogate manifestation of the disease. Biomarkers used for screening or diagnosis also often represent surrogate manifestations of the disease. 4
In clinical practice the use of biomarkers has increased substantially specially because enthusiasts claim that biomarkers may improve the early diagnosis of infections and be available as a point-of-care tool. Both single as well as serial measurements of biomarkers have been evaluated in diagnosis, in a variety of infections as well as in clinical settings, namely emergency departments (ED), medical and surgical wards and intensive care units (ICUs).
Biomarker in the stratification of severity
The early identification of infection is particularly important in those who are critically ill because the rapid establishment of resuscitation measures and administration of the appropriate antimicrobial reduce mortality. Procalcitonin (PCT) values, particularly in low ranges (0.5-2 ng/mL), are not very useful in identifying the most severe patients because of its little power of discrimination. However, very high values (> 10 ng/mL) suggest a significantly increased risk of sepsis and/or septic shock and low values (< 0.2 ng/mL) practically rule out bacteraemia with a negative predictive value (NPV) > 98% 5 and consequently its determination will also help to make decisions in some cases. So a patient suffering from shock, very low levels of PCT (<0.2 ng/mL) confirmed 12 hours later, make a bacterial infection unlikely and require alternative diagnoses (viral infections, autoimmune conditions or other types of shock).
Biomarker in antibiotic stewardship and monitoring response to the therapy
In case of suspected infection, undelayed and appropriate antibiotic treatment should be considered. Any start of such therapy should wait until after the draw following analysis of a blood sample for microbiological blood cultures to identify the presence of any blood-borne microorganisms. Because blood culture results may take several days to be available and is associated with limited diagnostic accuracy for infection, PCT levels can aid the clinician in the early antibiotic management of patients with suspected infection.
Antibiotic treatment is common in respiratory tract infections (RTIs) despite the fact that the vast majority are caused by viruses, against which antibiotics are ineffective and unnecessary. The concern is that antibiotics may cause side effects and are directly associated with antibiotic resistance in common bacteria, causing treatment failure and complications, including death. Antibiotics have a modest, if any, effect against the majority of respiratory tract infections. Their use in therapeutic monitoring is taking several forms including predicting response, monitoring for side effects, and as surrogate endpoints. The decision to start and stop antibiotics is probably one of the most frequent and difficult decisions at the bedside. Whereas clinical information is usually sufficient to initiate empiric therapy, they lack accuracy to tailor subsequent therapy and decide on its duration. Physicians’ decisions would be strengthened if they could get help from results of accurate biomarkers reflecting the diagnosis or evolution of the infectious processes. Several studies have shown the importance of early ad-ministration of an adequate antibiotic treatment on the reduction of mortality, particularly in critically ill patients. In this regard, if the patient is in septic shock, current biomarkers do not allow us waiting to start antibiotics until they rise up to a certain threshold level because, for instance PCT can take up to 6 hours to reach abnormal plasma levels, which would unjustifiably delay the start of treatment. However, in COPD patients with respiratory exacerbation or in cases of respiratory infection in primary care, the measurement of PCT avoids the overuse of
antibiotics in a significant and safe way, compared to making decisions without knowing their value.1
On the other hand, administering unnecessary or very prolonged antibiotics courses over time might be harmful to the patient, so limiting them for such period as is strictly necessary is mandatory. Some studies have shown that shorten duration treatments can be as effective and safe as longer ones 1,6 , but the fear that keeping them only for a few days decreases curation rates or increases recurrences, leads to unjustifiably prolonged treatments. For more severe infections (i.e., pneumonia, sepsis), antibiotic stewardship by monitoring PCT kinetics resulted in shorter antibiotic treatment duration by early cessation of therapy. These strategies appear to be safe without increasing the risk for mortality, recurrent infections, or treatment failure. PCT kinetics have also proved to have prognostic value, correlating with disease severity (i.e., pancreatitis, abdominal infection) and resolution of illness (i.e., sepsis). In this context, the PCT has proved useful because it becomes a tool that reduces the level of physician´s uncertainty when deciding to stop antibiotics.
Monitoring PCT levels allows shorten antibiotics in a significantly and safely way, particularly in cases of respiratory infection, an average of 2.5 days, even in critical patients.1,6 However, it is also important to take into account the limitations of PCT to make an adequate use of it. PCT is released to blood when monocytic cells adhere and interact with parenchymal cells as expression of systemic response to infection that might not occur in localized infections such as abscesses so PCT is not useful in those cases. The onset or duration of antibiotics in other serious infections such as endocarditis cannot be guided by PCT or other biomarker because it aims to “sterilize” the affected endocardial structure and that may require a long period of antibiotic treatment even though the PCT is normalized. Apart from that, the studies that have analyzed the role of PCT in guiding antibiotic duration have not included cases of endocarditis.
CRP
CRP is a well-established biomarker of infection and inflammation. CRP is an acute-phase reactant produced only by hepatocytes in response to inflammation or tissue injury. CRP hepatic synthesis starts rapidly after a stimulus with rise noted by about 6 hours with peak around 48 hours and a plasma half-life of approximately 19 hours. The half-life is constant under all conditions, so hepatic synthesis determines the serum concentration. Because the levels of CRP rise much more significantly during acute inflammation than the levels of the other acute phase reactants, the CRP test has been used for decades to indicate the presence of systemic inflammation, infection, or sepsis. Studies have found that CRP changes were not influenced by neutropenia in septic patients, but CRP was not a good predictor of infection in neutropenic patients. 7 Elevated CRP levels in sepsis have been correlated with increased risk of death and organ failure, but in part due to the persistence of elevated levels, were unable to predict survival when evaluating CRP trends. There is currently no set standard for CRP blood levels, and guidelines vary. However, as a general rule, the following classifications apply to CRP:
- -Levels between 3 mg/L and 10 mg/L are mildly elevated and usually result from chronic conditions such as diabetes, hypertension, or lifestyle factors including tobacco smoking and being sedentary.
- Levels between 10 mg/L and 100 mg/L are moderately elevated and are usually due to more significant inflammation from an infectious or non-infectious cause.
- Levels above 100 mg/L are severely elevated and almost always a sign of severe bacterial infection.
A huge range of conditions can raise CRP levels slightly, and, as there is no standard reference range set for CRP, there is usually no way to draw any conclusions by looking at CRP levels alone. The following factors can also make it challenging to interpret CRP levels:
Medications: Medications that reduce inflammation in the body, such as some cholesterol-reducing medicines (statins) and
specific nonsteroidal anti-inflammatory drugs (NSAIDs), may lower CRP levels.
Minor injuries or infection: These conditions may temporarily raise CRP levels and conceal other potential conditions such as diabetes or IBS.
Chronic conditions: Conditions that cause persistent inflammation, including autoimmune diseases, may mask other possible causes of elevated CRP such as minor infection.
Estrogen levels: Estrogen-based medications such as birth control pills and hormone replacement medications may raise CRP levels.
Pregnancy: Pregnancy can elevate CRP levels, especially during the later stages.
CRP in combination with a procalcitonin (PCT) test can effectively distinguish systemic inflammation from sepsis. Sepsis is the result of an uncontrolled immune-response to infection and has a mortality rate close to 30 %.
Procalcitonin
Procalcitonin, a 116 amino acid polypeptide prohormone of calcitonin, has emerged as a highly sensitive biomarker to aid diagnosis of bacterial sepsis. Synthesised primarily by the C-cells of the thyroid gland, and to a lesser extent in the neuroendocrine tissue of other organs such as the lungs and intestines, normal procalcitonin levels in the blood are very low. However, production can be stimulated in almost every organ by inflammatory cytokines and especially bacterial endotoxins, causing high amounts of procalcitonin to be released in the blood. This allows procalcitonin levels to be used as a biomarker of severe inflammation, infection and sepsis. The higher the level of PCT, the greater the likelihood of systemic infection and sepsis. Procalcitonin levels in blood increase following bacterial infection and decline following adequate treatment with antibiotics. 8 Procalcitonin increases more extensively during bacterial than in viral RTIs and has a more
responsive kinetic profile, potentially reflecting the bacterial disease progression compared to CRP. Procalcitonin has been studied as an intervention biomarker in RCTs, where procalcitonin levels in blood determined the initiation and discontinuation of antibiotic treatment. Procalcitonin-guided antibiotic treatment protocols were associated with a decrease of 19% in the antibiotic prescription rate (p <0.0001) and 30% in overall exposure days to antibiotics (p <0.0001) in a recent systematic review and meta-analysis involving patients with acute respiratory infections. 1 Similar rates of treatment failure and length of ICU or hospital stay were found between the procalcitonin and the control groups. Interestingly, a lower 30-day morality rate (p <0.05) and antibiotic side effects (p <0.0001) were observed within the procalcitonin group. A meta-analysis based on two RCTs of 655 upper RTI patients showed that procalcitonin was associated with a decrease in the antibiotic prescription rate from 51% in the control group to 18% in the procalcitonin group.9 No significant differences in clinical outcomes such as treatment failure, mortality or days with restricted activity were found between the procalcitonin and the control groups. Current challenges that limit application of PCT include the etermination of optimal diagnostic cut off values to diagnose bacterial RTIs, and the impact of various patient conditions on these values, which should be studied in stratified randomized clinical studies. Another recent paper by Sager et al. offers recommendations PCT diagnosis and antibiotic stewardship of patients in emergency department (ED) and ICU with suspected infection or sepsis, based on PCT levels. See figures 1, 2, 3 below. 10
Furthermore, the 2016 guidelines of the Surviving Sepsis Campaign (SSC) recommend the use of PCT as a tool to steer and optimise antibiotic treatment.
New biomarkers
Several biomarkers are currently used in clinical practice, but only a few of them have the characteristics of the ideal laboratory test. Recently, there has been a growing interest in identifying novel biomarkers, such as proadrenomedullin, s TREM-1 and pentraxin -3. The identification of these new candidates has been followed by a thorough operational evaluation to validate its application in the clinical setting.
Proadrenomedullin (Pro-ADM)
Proadrenomedullin serves as a biomarker for indirect quantification of adrenomedullin (ADM). ADM plays a vital role in immune-modulation, and its serum level increases during bacterial and viral infections. Recently, the role of ProADM in emergency depart-ments and critically ill patients has been studied as a marker of severity since it is more stable and its determinations more reproducible than adrenomedullin (ADM), a peptide hormone of the calcitonin family,
produced by different tissues in response to physiological and pathological stress (including sepsis). A study that compared the utility of proadrenomedullin to predict bacterial community-acquired pneumonia (CAP) vs. non-bacterial RTIs did not show the predictive relevance of proadrenomedullin.11 However, the evidence of proadrenomedullin to support the diagnosis of bacterial respiratory tract infections is inconsistent. The prospective studies with a larger and more uniform patient population can support establishing the relevance of proadrenomedullin in identifying bacterial infections.
sTREM-1 (Soluble triggering receptor expressed on myeloid cells-1) sTREM-1 levels rise in biofluids after an increase of TREM-1 expression on neutrophils, granulocytes, monocytes and alveolar macrophages in normal lung tissue. TREM-1 regulates inflammatory responses associated with monocytes and neutrophils . Microbial products increase TREM-1 expression with a subsequent increase of sTREM-1 levels in the biofluids .
A meta-analysis of nine studies showed that bronchoalveolar lavage fluid (BALF) sTREM-1 could identify bacterial RTIs with high accuracy BALF sTREM-1 was higher only in pneumonia patients with positive BALF cultures (100% specificity) and could accurately differentiate them from pneumonia patients with negative BALF cultures.12
Pentraxin-3
Pentraxin-3 is an acute inflammatory marker and a vital component of innate immunity. Pathogens stimulate pentraxin-3 production in different cells including epithelial, endothelial, myeloid dendritic cells, neutrophils and macrophages . Pentraxin-3 promotes the recruitment of neutrophils. Studies suggest the potential diagnostic value of pentraxin- 3 in RTIs. Sputum pentraxin-3 levels were higher in chronic inflammatory pulmonary disease (COPD) patients with bacterial exacerbations compared to those with viral and non-infectious exacerbations 13 BALF pentraxin-3 was associated with good
performance and >90% sensitivity to discriminate patients with culture positive bacterial, viral or fungal and culture negative pneumonia at a cut-off of <1 ng/mL.14 At a cut-off of >7 ng/mL, BALF pentraxin-3 performed similarly and identified the subgroup of patients with proven bacterial pneumonia. The non-homogenous patient population involving CAP, hospital-acquired pneumonia, health-care associated pneumonia and ventilator-associated pneumonia patients may have affected the sensitivity and specificity of BALF pentraxin-3.
Conclusion
Biomarker, when used in conjunction with an optimal clinical assessment can improve the diagnostic and prognostic assessment of infection. Both strengths and weaknesses of biomarkers must be considered for a rational and safe implementation in a routine clinical setting. Importantly, biomarkers can also improve the prognostic assessment of infection to predict failure compared with other routinely used laboratory parameters or compared with a clinical assessment
alone. A combination of biomarkers may be more functional in the case
of clinical application, but this may require further investigation in various aspects as a reliable diagnostic tool, guided antibiotic stewardship and its prognosis.
References
1. Schuetz P, Wirz Y, Sager R, Christ-Crain M, Stolz D, Tamm M, et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: a patient level meta-analysis. Lancet Infect Dis. 2018;18(1):95-107. doi: 10.1016/S1473- 3099(17)30592-3.
2. Hulka BS. Overview of biological markers. In: Biological markersin epidemiology (Hulka BS, Griffith JD, Wilcosky TC, eds), pp3–15. New York: Oxford University Press, 1990.
3. Byrnes SA, Weigl BH. Selecting analytical biomarkers for diagnostic applications: a first principles approach. Expert review of Molecular
diagnostics, 2018;18: (1) 19-26, DOI: 10.1080/14737159.2018.1412258
4. Salluh JIF, Souza-Dantas VC, Po’voa P. The current status of biomarkers for the diagnosis of nosocomial pneumonias. Curr Opin Crit Care 2017, 23:391–397 DOI:10.1097/MCC.0000000000000442 5. Martínez-Sagasti F, Busto-González B, Requesens-Solera M,
Sánchez-Cesteros C, Blesa Malpica A, Pérez-Cecilia Carrera E, et al. [Usefulness of procalcitonin to rule out bacteraemia in critically ill patients with fever: guide in the clinical decision making process] Med Intensiva 2015;39(Supp):1-209.
6. Sawyer RG, Claridge JA, Nathens AB, Rotstein OD, Duane TM, Evans HL, et al. Trial of short-course antimicrobial therapy for intraabdominal infection. N Engl J Med. 2015;372(21):1996-2005. doi: 10.1056/NEJMoa1411162.
7. P. P´ovoa, V. C. Souza-Dantas, M. Soares, and J. I. F. Salluh, “C-reactive protein in critically ill cancer patients with sepsis: influence of neutropenia,” Critical Care, vol. 15, no. 3, article R129, 2011. 8. Bartoletti M, Antonelli M, Arturo F, Blasi B, Casagranda I, Chieregato
A, et al. Procalcitonin-guided antibiotic therapy: an expert consensus. Clin Chem Lab Med 2018;56:1223–9.
9. Odermatt J, Friedli N, Kutz A, Briel M, Bucher HC, Christ-Crain M, et al. Effects of procalcitonin testing on antibiotic use and clinical outcomes in patients with upper respiratory tract infections. An individual patient data meta-analysis. Clin Chem Lab Med 2017;56:170–7.
10. Sager R, Kutz A, Mueller B, Schuetz1 P. Procalcitonin-guided diagnosis and antibiotic stewardship revisited. BMC Medicine 2017; 15:15 DOI 10.1186/s12916-017-0795-7
11. Esposito S, Di Gangi M, Cardinale F, Baraldi E, Corsini I, Da Dalt L, et al. Sensitivity and specificity of soluble triggering receptor expressed on myeloid cells-1, midregional proatrial natriuretic peptide and midregional proadrenomedullin for distinguishing etiology and to assess severity in community-acquired pneumonia. PLoS One 2016;11:1–14.
12. Shi JX, Li JS, Hu R, Li CH, Wen Y, Zheng H, et al. Diagnostic value of sTREM-1 in bronchoalveolar lavage fluid in ICU patients with bacterial lung infections: a bivariate meta-analysis. PLoS One 2013;8:e65436.
13. Thulborn SJ, Dilpazir M, Haldar K, Mistry V, Brightling CE, Barer MR, et al. Investigating the role of pentraxin 3 as a biomarker for bacterial infection in subjects with COPD. Int J COPD 2017;12:1199–205. 14. Mauri T, Coppadoro A, Bombino M, Bellani G, Zambelli V, Fornari C,
et al. Alveolar pentraxin 3 as an early marker of microbiologically confirmed pneumonia: a threshold-finding prospective observational study. Crit Care 2014;18:562
PENDEKATAN KLINIS FEVER OF UNKNOWN ORIGIN
I Made Susila Utama
Divisi Penyakit Tropik Dan Infeksi, Departemen/KSM Penyakit Dalam, Fakultas Kedokteran Universitas Udayana/Rumah Sakit Sanglah,
Denpasar, Bali PENDAHULUAN
Keluhan demam sering kita dapatkan dalam praktik klinis namun penyebab demam juga tidak selalu mudah bisa didapatkan sehingga menyulitkan para klinisi dalam memberikan penanganan. Pada kasus demam dengan suhu diatas 38,30C lebih dari 3 minggu dalam perawatan belum terdiagnosis walaupun sudah dilakukan penelusuran selama 1 minggu dengan pemeriksaan penunjang diagnostik sesuai standar digolongkan sebagai fever of unknown origin (FUO). Prevalensi FUO pada pasien dewasa yang dirawat di rumah sakit sekitar 2,9%. Diagnosis banding penyebab FUO mencapai 200 lebih kelainan atau penyakit yang digolongkan menjadi infeksi, neoplasma, autoimun dan penyebab lainnya. Penggolongan FUO terakhir untuk mempermudah investigasi penyebab meliputi FUO klasik, nosokomial, neutropenia (defisiensi imun) dan Human immunodeficiency virus associated FUO. Tidak ada standar diagnostik dalam pendekatan klinis FUO, diperlukan anamnesis yang cermat, pemeriksaan fisik yang teliti dan pemilihan pemeriksaan penunjang yang selektif. Walaupun sudah dilakukan prosedur diagnostik yang lengkap namun 30% kasus FUO tetap tidak diketahui penyebabnya.1,2,3
Penyebab FUO secara umum dibedakan menjadi infeksi dan non infeksi. Pada dugaan etiologi infeksi perhatian difokuskan pada penggunaan peralatan medis atau prothese seperti catheter-related infection, infeksi saluran kencing pada penggunaan kateter urine, sinusitis pada penggunaaan naso gastric tube, ventilator associated pneumonia, juga komplikasi post operasi seperti surgical site infection, hematom, abses, infected foreign body dan kemungkinan adanya infeksi nosokomial seperti infeksi Clostridium difficile. Pada pasien neutropeni
rentan terhadap infeksi bakteri dan jamur seperti candida dan aspergillus. Penyebab non infeksi seperti deep vein thrombosis (DVT), drug fever dan beberapa penyebab lainnya.4 Penyebab FUO dari berbagai studi mendapatkan hasil berbeda. Pada studi evaluasi penyebab FUO didapatkan penyebab terbanyak adalah inflamasi non infeksi terutama pada usia tua sedangkan pada FUO pediatri didominasi penyebab infeksi5,6. Pada sebuah studi kohort dengan jumlah kasus FUO sampai 215 kasus, penyakit infeksi masih mendominasi sampai 42,3% terutama tuberkulosis diikuti connective tissue disease (32,1%).7 Studi lainnya mendapatkan kasus penyakit inflamasi non infeksi (30,6%) sebagai penyebab terbanyak diikuti kasus infeksi (23,1%) dan neoplasma (10,7%).8
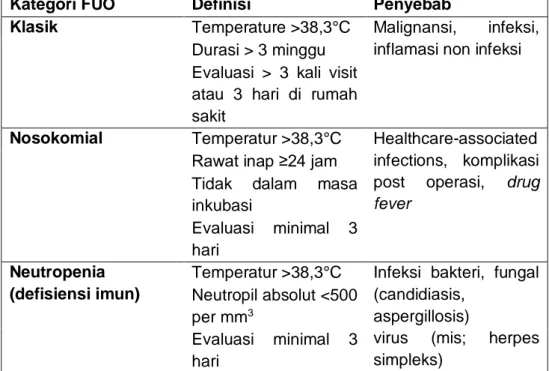
Tabel 1. Kategori FUO3
Kategori FUO Definisi Penyebab
Klasik Temperature >38,3°C Malignansi, infeksi, inflamasi non infeksi Durasi > 3 minggu
Evaluasi > 3 kali visit atau 3 hari di rumah sakit
Nosokomial Temperatur >38,3°C Healthcare-associated infections, komplikasi post operasi, drug fever
Rawat inap ≥24 jam Tidak dalam masa inkubasi
Evaluasi minimal 3 hari
Neutropenia (defisiensi imun)
Temperatur >38,3°C Infeksi bakteri, fungal (candidiasis,
aspergillosis)
virus (mis; herpes simpleks)
Neutropil absolut <500 per mm3
Evaluasi minimal 3 hari
HIV associated Temperatur >38,3°C Infeksi primer HIV, mycobacterium (typical, atypical), cytomegalovirus, lymphoma, toxoplasma, cryptococcus, IRIS Durasi > 4minggu (rawat jalan)
Durasi >3 hari (rawat inap)
Terkonfirmasi infeksi HIV
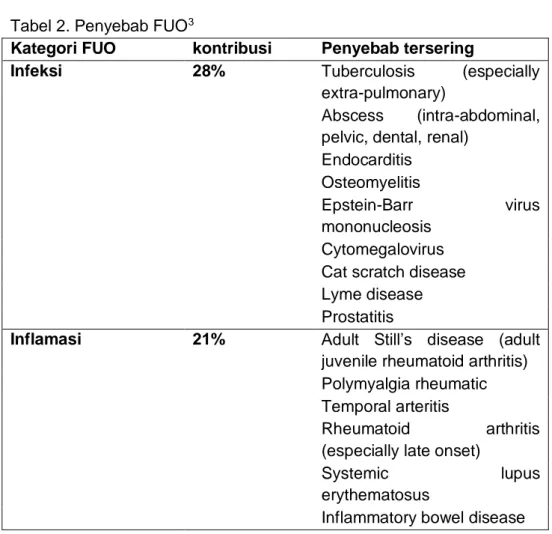
Tabel 2. Penyebab FUO3
Kategori FUO kontribusi Penyebab tersering
Infeksi 28% Tuberculosis (especially
extra-pulmonary)
Abscess (intra-abdominal, pelvic, dental, renal)
Endocarditis Osteomyelitis
Epstein-Barr virus mononucleosis
Cytomegalovirus Cat scratch disease Lyme disease Prostatitis
Inflamasi 21% Adult Still’s disease (adult
juvenile rheumatoid arthritis) Polymyalgia rheumatic Temporal arteritis
Rheumatoid arthritis (especially late onset)
Systemic lupus
erythematosus
Malignansi 17% Leukemia and lymphoma Metastatic cancers Renal cell carcinoma Colon carcinoma Hepatoma
Myelodysplastic syndromes Pancreatic carcinoma Sarcomas
Penyebab lain 15% Drug-induced fever
Complications from cirrhosis Factitious fever
Hepatitis (alcoholic, granulomatous, or lupoid) Deep venous thrombosis Sarcoidosis
Mediterranean familial fever Hyperthyroidism
Tidak terdiagnosis 19% PENDEKATAN KLINIS
Dalam pendekatan klinis kasus demam kronik terlebih dahulu dipastikan apakah sudah sesuai dengan definisi FUO. Langkah awal adalah dengan anamnesis cermat dan pemeriksaan fisik yang komprehensif. Pada anamnesis difokuskan pada karakter demam untuk lebih mengarahkan dugaan penyebab. Setiap penyebab FUO sebenarnya punya kekhususan sendiri seperti pada neoplasma atau malignansi maka gejala yang dominan adalah anoreksia lebih awal disertai penurunan berat badan yang signifikan, pada penyebab infeksi sering didapatkan gejala menggigil, pada penyebab inflamasi/rheumatik ada synovitis1. Manifestasi klinis penyebab FUO sering tidak spesifik, diperlukan data onset munculnya gejala demam, gejala penyerta demam dan derajat berat ringannya keluhan. Penurunan berat badan yang drastis menandakan kemungkinan neoplasma walaupun juga bisa
disebabkan oleh penyakit infeksi seperti tuberkulosis atau bruselosis. Keringat malam sering didapatkan pada keganasan hematologi dan tuberkulosis. Nyeri sendi pada pagi hari mengarahkan pada artritis inflamasi. Riwayat nyeri kepala terutama di retro orbita unilateral dengan kaku pada rahang terutama pada usia tua merupakan tanda giant cell arthritis (arteritis temporal). Riwayat kontak dengan penyakit menular, riwayat bepergian dan juga riwayat pengobatan sangat diperlukan4. Riwayat penyakit sebelumnya dan juga riwayat penyakit dalam keluarga sangat penting bila menduga kemungkinan penyebab autoimun. Riwayat pengobatan juga diperlukan terkait adanya drug fever, jenis obat terkait drug fever antara lain antibiotika terutama antibiotika golongan beta laktam, anti konvulsan termasuk karbamazepine dan penitoin, anti inflamasi non steroid seperti ibuprofen dan naproxen, obat pengganti hormon tiroid dan anti hipertensi diltiazem dan methyl dopa. Pada pemeriksaan fisik diperhatikan adanya lesi kulit, orofaring, gigi (abses), pembesaran kelenjar limfe, pembesaran liver dan lien, massa di abdomen, pelvis dan suara jantung tambahan.9,10,11
Pendekatan diagnostik FUO dengan pemeriksaan penunjang bersifat individual sesuai kasus artinya tidak ada pemeriksaan standar, beberapa pendekatan klinis bisa diikuti. Pemeriksaan laboratorium tidak spesifik dalam pendekatan diagnosis awal diperlukan untuk identifikasi seperti darah lengkap, urinalisis, C-reaktif protein (CRP), laju endap darah (LED), kreatinin serum, fungsi liver, elektrolit, faktor rematoid, elektroforesis protein dan kultur darah. Pemeriksaan lini kedua yang lebih spesifik bila sudah mengarah ke dugaan penyebab seperti serologi HIV, serum feritin, fungsi tiroid, Lacatate Dehydrogenase (LDH), serologi untuk penyebab spesifik, ekokardiografi dan pemeriksaan lainnya. Pada pemeriksaan radiologi di awal disarankan pemeriksaan kurang spesifik seperti x-ray dan ultrasonografi. Bila pemeriksaan awal belum mendapatkan kesimpulan barulah diikuti pemeriksaan CT (Computerized Tomography), MRI (Magnetic Resinance Imaging) dan terakhir dikembangkan pemeriksaan PET-CT (Positron emission Tomography) namun masih terbatas karena kendala biaya. Prosedur endoskopi diperlukan pada dugaan kasus IBD (inflammatory bowel
disease) dan sarkoidosis.9,10 kriteria Duke mempunyai spesifisitas yang sangat tinggi (99%) dalam mendiagnosis dugaan endokarditis infektif demikian juga CT scan abdomen dalam dugaan penyebab intra abdominal sedangkan kultur sumsum tulang nilai diagnostiknya sangat rendah.12
TATA LAKSANA
Secara umum terapi empirik pada FUO tidak direkomendasikan karena bisa memberikan efek masking, memperlambat diagnosis etiologi spesifik dan tata laksana. Pada beberapa kondisi bisa diberikan terapi empirik seperti pemberian antibiotika pada kasus endokarditis infektif dengan kultur negatif, obat anti tuberkulosis pada dugaan tuberkulosis aktif terutama pada usia tua, kortikosteroid dosis rendah pada kasus arteritis temporalis dengan risiko kehilangan penglihatan dan penggunaan tes naproxen. Tes naproxen membedakan penyebab FUO antara infeksi dan neoplasma. Pada etiologi infeksi maka naproxen tidak respon sedangkan pada neoplasma terjadi respon penurunan demam dalam 24 jam. Tes naproxen masih menjadi perdebatan karena penelitian lain membuktikan rendahnya sensitifitas dan spesifisitas dalam membedakan penyebab demam antara neoplasma dan infeksi.13 Penggunaan glukokortikoid pada FUO disarankan hanya pada kasus yang sangat selektif. Antipiretik diberikan pada pasien FUO yang tidak toleran terhadap demam dan pemberian anti piretik secara rutin akan menghilang gambaran demam sebenarnya yang diperlukan dalam penelusuran etiologi.1,9
PROGNOSIS
Prognosis FUO tergantung etiologi, mortalitas FUO berkisar 12-35%. Sebagian besar kasus FUO bersifat self-limited illness dengan prognosis yang baik.12,14 Prognosis makin memburuk bila diagnosis etiologi makin terlambat ditegakkan.15
DAFTAR RUJUKAN
1. Cunha BA, Lortholary O, Cunha CB. Fever of Unknown Origin: a Clinical Approach. The American Journal of Medicine (2015) 128, 1138.e1-1138.e15
2. Harrison's Fever of unknown origin. In: Longo D, Fauci A, Kasper D (Eds). Principles of Internal Medicine, 18th edition. Mc Graw Hill; 2012. pp.158-64.
3. Fergus T. Fever of Unknown origin: A Clinical Approach. UBCMJ | FEBRUARY 2013 4(2) | www.ubcmj.com
4. Hayakawa K, Ramasamy B, Chandrasekar PH. Fever of Unknown Origin: An Evidence-Based Review. Am J Med Sci 2012; 344(4): 307–316
5. Zenone T. Fever of unknown origin in adults: Evaluation of 144 cases in a non-university hospital. Scandinavian Journal of Infectious Diseases, 2006; 38: 632-638
6. Chien YL, Huang FL, Huang CM, Chen PY. Clinical Approach to Fever of Unknown Origin in Children. Journal of Microbiology, Immunology and Infection 2017; 50: 893-898
7. Zhai Y,Chen X, Liu X, Zhang Z, Xiao H, Liu G. Clinical analysis of 215 consecutive cases with fever of unknown origin: a cohort study. Medicine (2018) 97:24
8. Naito T, Mizooka M, Mitsumoto F, et al. Diagnostic workup for fever of unknown origin: a multicenter collaborative retrospective study. BMJ Open 2013;3:e003971.
9. Santana LF, Rodrigues M, Silva MP, Brito R, Nicacio JM, Duarte RM, Gomes OV, Fever of unknown origin: a literatur review. REV ASSOC MED BRAS 2019; 65(8):1109-1115
10. Roth AR, Basello GM. Approach to Adult Patients with Fever of Unknown Origin. Am Fam Physician 2003; 68: 2223-8.
11. Beresford RW, Gosbell IB. Pyrexia of Unknown Origin:Cause, Investigation and management. Royal Australasian College of Physicians 2016. doi:10.1111/imj.13180
12. Mourad O, Palda P, Detsky A. A Comprehensive Evidence Based Approach to Fever of Unknown Origin. Arch Intern Med 2003; 163: 545-551
13. Vanderschueren S, et al. Lack of value of the naproxen test in The differential diagnosis of prolonged febrile illnesses. Am J Med. 2003;115(7):572–5.
14. Tan Y, Liu X, Shi X. Clinical features and outcomes of patients with fever of unknown origin: a retrospective study. BMC Infectious Diseases (2019); 19:198
15. Ungur M, Karanikas G, Kerschbaumer A, Winkler S, Aletaha D. Fever of Unknown Origin (FUO) Revised. Wien Klin Wochenschr (2016) 128:796–801
HUMAN LEPTOSPIROSIS
CURRENT CONCEPT AND UP-DATE MANAGEMENT
Muhammad Hussein Gasem
Leptospirosis is a widespread zoonosis caused by pathogenic Leptospira spp, i.e. Leptospira interrogans (1). The disease is endemic in Indonesia with increasing number of outbreaks reported in Java island. It is a complex and dynamic bacterial disease with multiple modes of transmission, and numerous hosts. The broad-range of clinical manifestations cause difficulty to diagnosis on clinical ground alone especially the mild, atypical, non-specific Leptospirosis that accounted for 90% of two clinical syndromes. Leptospirosis is one of the leading causes of hospitalisation and mortality among adults in hospitals of many part of the world especially in endemic areas (2).
Epidemiology
Leptospirosis is not a new emerging disease in Indonesia. This disease has long existed in Indonesia since a century ago as reflected by the old-fashioned names and places in Java as well as Sumatra for naming the serovars or serogroups of Leptospira sp. The actual incidence of leptospirosis is not well documented, most data are based on hospital reports. Based on the on-going surveillance studies in Central Java, confirmed and probable leptospirosis cases are increasingly reported by primary health care in 3 districts i.e. Semarang municipal, Demak and Banyumas regencies (unpublished data). During the last decade, leptospirosis is emerging with major outbreaks were reported in Indonesia i.e. in Jakarta (2002) with the massive flood as a possible main risk factor. In Yogyakarta, during outbreak (2011) most people getting infected were rice field farmers, while in Sampang, Madura (2013), over-flooding of river was the important risk factor. In Central Java, the incidence of leptospirosis has been increasing due to existing risk factors but also caused by more intensive active surveillance that has been done by district and provincial health offices
since the last decade. The leptospirosis outbreaks and the increasing number of cases and mortality reported from districts might stimulate a better attention and concern of the Indonesian Ministry of Health against this disease. The high case fatality rate ranging from 10 to 40%, even may reach 70% in case with pulmonary hemorrhage (3). Improved awareness and surveillance of leptospirosis in some province especially in Central and East Java has proven to result in marked increase of the annual number of notified cases. A hospital-based study at 9 hospitals located in 7 big cities, has shown that leptospirosis as one of the top big five of etiologies of hospitalized acute febrile illness (Gasem MH 2019 et al. submitted)
Clinical Manifestation and Case Definition
In South East Asia, leptospirosis is frequently misdiagnosed as a result of its wide-spectrum clinical manifestation, from non-specific febrile illness to severe or fatal case. (4). The most common clinical syndrome of leptospirosis is mild, anicteric, non-specific, mimicking other prevalent infectious diseases in the region like dengue fever, hantavirus infection, rickettsiosis, and typhoid fever (5) Leptospirosis is still an under-estimated, under-reported disease due to misdiagnosis and less awareness of clinicians to this disease.
Several clinical criteria or case definitions have been developed and used by clinicians worldwide. The Faine and modified Faine criteria have being practiced since last decade (6). Other case definitions made by many institutions from US CDC, Australian Health Department, Indian guidelines and other countries` health authorities are also available to be accessed on-line.
W.H.O South East Regional Office (SEARO) developed the case definition on 2009 and this is the guideline have been widely applied in Indonesia and listed in the formal book of Indonesia Ministry of Health (7).
Case definition of Leptospirosis WHO SEARO 2009 Suspect case:
Acute febrile illness (>= 38.5 C ) and/or severe headache with Myalgia
Prostration AND/OR
Conjunctival suffusion, AND
History of exposure to leptospira- contaminated environment Probable case (At primary health care level)
Suspect case with any two of the following: Calf tenderness
Cough with or without hemoptysis Jaundice
Haemorrhagic manifestations Meningeal irritation
Anuria/ oliguria and/ or proteinuria Breathlessness
Cardiac arrhythmias Skin rashes
Probable case (At secondary and tertiary health care levels)
Based on availability of laboratory facilities a probable case of Leptospirosis is a suspect case with a positive rapid IgM test
AND/ OR
Supportive serologic findings: MAT (Microagglutination Test) titre equal to 200 in a single sample)
AND/ OR Any three of the following:
Urinary findings: proteinuria, pus cells, blood Relative neutrophilia (>80%) with lymphopenia Platelets < 100,000 / cu mm
Elevated serum bilirubin > 2 mg% ; liver enzymes moderately raised ( Serum Alkaline Phosphatase, S amylase, CPK)