Health System Research
㻾㼑㼟㼑㼍㼞㼏㼔㻌
㼀㼛㻌㼙㼍㼗㼑㻌㼍
Difference
2006 - 2009
July 2013
Health System Research
Research
To make a
Difference
Perak
Health System Research (HSR) in Perak 2006-2009 Using Research to Make a Diference
© July 2013, Clinical Research Centre Perak, Level 4, Ambulatory Care Centre,
Raja Permaisuri Bainun Hospital, Jalan Hospital, 30990 Ipoh, Perak, Malaysia.
Editorial Committee
Amar-Singh HSS Ooi Qing Xi
Lionel Chia Dick Hua Lim Wei Yin
Lina Hashim
Arvinder Singh Harbaksh Singh
Advisors
Datin Dr Ranjit Kaur Praim Singh
Deputy Director of Perak State Health Department (Public Health)
Sondi Sararaks
Head Health Outcomes Research Division, Institute for Health Systems Research (IHSR)
Dr Asmah Zainal Abidin
Head of Assistant Director of Public Health Division (Non-Communicable Disease Centre, NCDC) Perak State Health Department
Disclaimer
The views, interpretations, implications, conclusions, and recommendations expressed in this book are those of the authors of individual reports and do not necessarily represent the opinions, the views or policy of the Ministry of Health Malaysia.
Acknowledgement
Contents
Home Safety Practices for Prevention of Poisoning in
Young Children
1
Effective Implementation of a Structured
Psychoeducation Programme Among Caregivers of
Schizophrenia Patients in the Community
41
Improving Asthma Care in Ministry of Health Primary
Care Clinics
89
The Involvement of Lay Educators in Diabetic Control
of Type 2 Diabetic Patients
123
Improving Knowledge of Type 2 Diabetes Mellitus
Patients on Oral Hypoglycaemic Agents
163
Health Seeking Behaviour Towards Communicable
Diseases Among Foreign Workers in Industrial &
Agriculture Sectors of Selected Districts in Perak,
Malaysia
205
Improving Blood Pressure Controls in Primary Care
Settings
249
An Intervention Programme Among Overweight
Primary School Children
281
Effectiveness of the Diabetic Foot Care Programme in
a Primary Care Setting
1
Home Safety Practices for Prevention
of Poisoning in Young Children
Health Systems Research 2008/2009
Authors
Shoba Pathmanathan Paediatric Department,
Hospital Raja Permaisuri Bainun Ipoh, Perak
Lina Hashim
Clinical Research Centre Perak
Affendi Yusuf
Manjung District Health Office
Vishanthri Kulasingam Greentown Health Clinic
Hooi-Meng Puah Kinta District Health Office
Amar-Singh HSS
Clinical Research Centre Perak, Department of Paediatrics,
Hospital Raja Permaisuri Bainun Ipoh, Perak
Sondi Sararaks
Institute for Health Systems Research
Ranjit Kaur Praim Singh Perak State Health Department
Asmah Zainal Abidin Perak State Health Department
Clinical Research Centre (CRC) Perak recommends using the following statement to cite this report in our publication entitled “Health System Research (HSR) in Perak 2006-2009: Using Research to Make a Difference”:
Shoba Pathmanathan, Lina Hashim, Affendi Yusuf, Vishanthri Kulasingam, Hooi-Meng Puah, Amar-Singh HSS, Sondi Sararaks, Ranjit Kaur Praim Singh, Asmah Zainal Abidin. ”Home Safety Practices for Prevention of Poisoning in Young Children” in Health System Research (HSR) in Perak 2006-2009: Using Research to Make a Difference. Clinical Research Centre (CRC) Perak, 2013, pp 1. (ISBN: 9789671063422)
ISBN
2 Home Safety Practices for Prevention of Poisoning in Young Children
Contents of Report
page
Abstract 3
1. 0 Introduction 5
1.1 Problem statement
1.2 Problem analysis
2.0 Objective 9
2.1 General objective
2.2 Speciic objectives
3.0 Methodology 9
3.1 Overview of research design
3.2 Intervention package
3.3 Study type
3.4 Ethical considerations
3.5 Variables
3.6 Sampling
3.7 Techniques for data collection & pre-testing
3.8 Plan for Data Analysis and Interpretation (Include Dummy Tables)
4.0 Results 17
4.1 Results of Evaluation of Safety Device
4.2 Socio-demographic data
5.0 Discussion 24
5.1 Statement of principal indings
5.2 Strengths and weaknesses of the study
5.3 Strengths and weaknesses in relation to other studies
5.4 Meaning of the Study (Possible Mechanism and Implication for Clinicians/Policymakers)
5.5 Unanswered questions and future research
6.0 Conclusion & Recommendations 27
References 28
3 Home Safety Practices for Prevention of Poisoning in Young Children
ABSTRACT
Home Safety Practices for Prevention of Poisoning in Young Children
Shoba Pathmanathan¹, Lina Hashim², Affendi Yusuf³, Vishanthri Kulasingam4, Hooi-Meng Puah5, Amar-Singh HSS¹,², Sondi Sararaks6, Ranjit Kaur Praim Singh7, Asmah Zainal Abidin7
1 Paediatric Department, Hospital Raja Permaisuri Bainun Ipoh 2 Clinical Research Centre Perak
3 Manjung District Health Office 4 Greentown Health Clinic 5 Kinta District Health Office
6 Institute for Health Systems Research 7 Perak State Health Department
Introduction and Objectives
Poisoning in young children is defined as unintentional ingestion of medication(s) and common household products or chemicals. Poisoning in young children is a preventable cause of mortality and morbidity. Poisoning accounts for 2% of the accidental deaths in developed countries and for 5% in developing countries. Most poisoning accidents occur in children aged between 1 to 4 years old. The objective of the study was to evaluate and improve home poison safety practices to prevent poisoning in homes with children aged 1-4 years in the Kinta and the Manjung Districts.
Methodology
The study was a non-controlled community trial conducted at urban and semi-urban areas in Perak state to assess home safety practices and effectiveness of an intervention programme in home setting. Initial validation of a safety device involved 100 children and 100 adults (parents/caregivers accompanying the child) who attended Ministry of Health (MOH) health clinics and were recruited to test two home safety devices. In both urban and semi-urban areas, 300 households with children aged 1-4 years were randomly selected. They were audited at baseline. Two post-intervention audits were conducted at 3 and 6 months post-baseline audit using the same tools as in the first audit. The households were divided into two intervention arms. Caregivers in the first arm received Intervention Package 1 which consists of an immediate post-audit feedback, an educational pamphlet and a home safety device while caregivers in the second arm received Intervention Package 2 which consists of an immediate post-audit feedback and an educational pamphlet.
Results
4 Home Safety Practices for Prevention of Poisoning in Young Children knowledge. Good knowledge does not ensure a safe household. At the end of the study there was a statistically significant increase in the percentage of safe households in both districts with Kinta District doing better. Kinta District had an incarese from 48.6% (CI 40.4-56.8) to 93.9% (CI 89.7-98.0) while in the Manjung District, the increase was from 21.3% (CI 14.7-28.0) to 67.7% (CI 59.7-75.6).
Conclusion
The intervention package notably the Home Safety Practices Audit checklist, which was developed by the researchers for the study, significantly improved home poisoning safety practices. 75.7-85.3% of urban and semi-urban households in Perak had a safe home to prevent poisoning in children at the end of the study. Addition of the safety device to the home safety practices audit further improves home poisoning safety practices. Knowledge and perception does not ensure a safe household in prevention of poisoning in young children.
Keywords
5 Home Safety Practices for Prevention of Poisoning in Young Children
1.0 INTRODUCTION
Poisoning in young children is defined as unintentional ingestion of medication and common household products (J. Nixon et al. 2004).
Poisoning in young children is a preventable cause of mortality and morbidity (Laffoy M., 1997). Poisonings account for 2% of the accidental deaths in developed countries and for 5% in developing countries (Nadarajah P., 2004).
Most poisoning accidents occur in children aged between 1 to 4 years (48.5% in the study by Sibel E. and Sukran S. (2006) and 60.3% according to FDA’s Poisoning Surveillance and Epidemiology Branch 1981.
Around 80-85% poisoning accidents occur in the home (B. Jacobson et al. 1989).
Children under the age of 5 are in a stage of development where they constantly explore their home environment. This is a normal characteristic and should not be restricted. Unfortunately they usually put whatever they see or reach in their mouth (A. W. Craft, 1990).
Most of the poisoning accidents (49.5%) stemmed from storing of drugs within the reach of children. Out of these accidents, 49.5% were due to drugs, 17.5% due to cleaning agents and 16.5% due to insecticides/pesticides (Sibel E. et al. 2006).
In a study on home safety in the United States, although most families reported locked storage of medications, 77% had unlocked storage of medication documented during home observation (Kimberly E. et al. 2007).
Medications involved in suspected poisoning were most frequently packed in containers without Child Resistant Containers (CRC) (63%) or transparent blisters (20%). However safe packaging cannot compensate for unsafe storage. Bathroom and kitchen cabinets and drawers are the safest place to store medication (H. M. Wiseman et al. 1987).
The concept of CRC is widely supported by parents as an important mechanism for protecting children from toxic products. However the support for CRCs was often based on the notion that they were childproof rather than child resistant. As a result some parents were more likely to store products unsafely if they were in CRCs (L. Gibbs et al. 2005).
6 Home Safety Practices for Prevention of Poisoning in Young Children paraffin poisoning in the study community compared to the control community (Krug
et al. 1994).
Safe storage of toxic products should be in a locked cabinet or cupboard out of reach if possible in the kitchen or bathroom (L. Gibbs et al. 2005). Safe disposal according to the National Drug Control Policy Federal Guidelines Washington DC for unneeded or expired prescription drug should be taken out of their original container and thrown into the trash, returned to a community pharmaceutical take back program or flush down the toilet if the label instructs so.
Other implementation measure, besides safe storage and disposal practices and CRC, is parental education and improved supervision by parents. In rendering the child’s environment safe, the family’s education especially that of the mother is vital (Stewart J., 2001). 67% of the children involved in a poisoning accident were under the supervision of their mothers at the time of the accident (Sibel E. et al. 2006). 69% of mothers claimed to have taken measures to prevent future poisoning accidents in their homes however there was no mention at all of basic precautions such as storage in locked cupboards which are out of reach of children. This proves the necessity for educational measures in the families (Sibel E. et al. 2006).
In summary, a combination and not a single home poison safety strategy is needed to reduce accidental poisoning in young children. The strategies are:
1. Safe storage practices.
2. Efficacious CRC and Child Safety Devices. 3. Safe disposal practices.
4. Parent education.
5. Responsible supervision of children by caregiver at all times.
1.1 Problem Statement
The number of cases of accidental poisoning admitted to government hospital is static with no reduction over the years. There are no available local studies assessing the knowledge of caregivers or home poison safety practices. There is also no CRC or Child Safety Device in regular use in our local setting.
Based on international data, only 20% of homes are safe in terms of preventing an accidental poisoning and we assume this is the case in our setting as well.
7 Home Safety Practices for Prevention of Poisoning in Young Children
Table 1. Number of deaths in government hospital due to poisoning by drugs, medicaments
and biological substances.
Age (years) 1999 2000 2001 2002
<1 0 0 0 1
1-4 1 3 0 2
5-11 1 0 0 1
Table 2. Number of admissions in government hospital in Malaysia due to poisoning by
drugs, medicaments and biological substances.
Age (years) 1999 2000 2001 2002
<1 101 96 104 67
1-4 446 481 466 459
5-11 132 137 163 130
The above local statistics are comparable with international data such that the common age group involved in accidental poisoning is 1-4 years old. The local statistics available are only from those cases of accidental poisoning admitted to hospital and we are unable to capture data on children who seek treatment from health clinics and private clinic and hospital. So the actual number of cases of accidental poisoning is most likely to be 100 times the numbers projected in the table above.
Table 3. Number of admissions in government hospitals in Perak due to poisoning by
drugs, medicaments and biological substances for those in the 1-4 years old age group.
Year Number of poisoning cases
2003 66
2004 72
2005 nil
2006 37
2007 65
Based on the 1-4 years old population size in Perak of 171 853, the incidence of accidental poisoning in this age group in Perak is about 3% in keeping with international data for developing countries (5%).
1.2 Problem Analysis
8 Home Safety Practices for Prevention of Poisoning in Young Children 1. Educational program for parents
2. No audit of home poison safety practices to determine number of safe households
3. No CRCs or child home safety device in use regularly.
Figure 1: Bubble chart of problem analysis
9 Home Safety Practices for Prevention of Poisoning in Young Children
2.0 OBJECTIVES
2.1 General Objective
To evaluate and improve home poison safety practices to prevent poisoning in homes with children aged 1-4 years in the Kinta and Manjung districts.
2.2 Specific Objectives
1. To assess the home safety practices for poisons in homes with young children with respect to:
a. Knowledge of caregivers on safe practices.
b. Safe storage of medications and household products. c. Safe disposal of poisons.
2. To develop an intervention programme to improve poison safety measures at home by:
a. Immediate audit feedback and recommendations to caregivers. b. Education of caregivers.
c. A home safety device for safe medication and household product storage.
3. To evaluate the effectiveness of the intervention programme for poison safety in:
a. Improving knowledge of caregivers on safe practices.
b. Improving safe storage of medications and household products. c. Improving safe disposal of medications and household products. d. The value of a home safety device for safe medication and household
product storage.
4. To make recommendation on the use of the intervention package to improve home poison safety practices for poisons in homes with young children in Malaysian communities.
3.0 METHODOLOGY
3.1 Overview of Research Design
10 Home Safety Practices for Prevention of Poisoning in Young Children Phase 0: Validation of Home Safety Device
In order to ensure that the home safety device used in this study works effectively, the researchers performed a sub-study to test the efficacy of two different children home safety devices prior to its implementation in the study. The most efficacious device was then chosen.
In this sub-study, 100 children and 100 adult parents/caregivers accompanying the child to attend the MOH health clinics were recruited to test the home safety devices. Parents/caregivers accompanying a child aged between 12 to 60 months to a MOH clinic were approached about the study and a written consent was obtained if he or she agreed to be involved. 100 children and 100 of their parents/caregivers were asked to test on Device A and Device B.
The inclusion criteria for the children recruited for the study were: i) Seeking treatment at MOH health clinic.
ii) Aged 12-60 months.
The exclusion criteria for the children recruited for the study was: i) Suffering from any physical or mental disabilities.
The inclusion criteria for the adults recruited for the study were: i) Parent/caregiver for the child recruited for the study. ii) Ability to communicate in English or Malay.
The exclusion criteria for the adults recruited for the study were: i) Suffering from any physical or mental disabilities.
There were three activities in the study:
i) The first activity involved the child operating Device A or Device B without guidance. The child was given 5 minutes to operate the device. The method used by the children to successfully operate the device was documented. ii) The second activity phase involved the child operating Device A or Device B
without guidance, following a demonstration by a researcher. The child was given 5 minutes to operate the device. The method used by the children to successfully operate the device was documented.
iii) The third activity involved the accompanying parent/caregiver operating Device A or Device B without guidance, following a demonstration by a researcher. The adult were given 5 minutes to operate the device.
11 Home Safety Practices for Prevention of Poisoning in Young Children
Table 4. Criteria for efficacy of home safety device
Activity Criteria for Efficacy
Activity 1
Child operates device without guidance
At least 85% of the children must fail to operate the device within 5 minutes of attempting
Activity 2
Child operates device without guidance, following a demonstration by a
researcher
At least 80% of the children must fail to operate the device within 5 minutes of attempting
Activity 3
Adult operates device without guidance, following a demonstration by a
researcher
At least 85% of adults must be able to successfully operate the device within 5 minutes of attempting
Phase 1: Identification, Baseline Audit and Intervention
Phase 1 involved the identification of households with children aged 1-4 years, a baseline audit of the households and the implementation of an intervention package which include an immediate post audit feedback, an educational pamphlet and a home safety device.
The samples were randomly chosen from the Birth Registration Book from Year 2004 till Year 2007. The homes identified were sampled into two intervention arms. Caregivers in Group 1 received intervention package which consists of an immediate post audit feedback, an educational pamphlet and a home safety device while caregivers in Group 2 received intervention package which consists of an immediate post audit feedback and an educational pamphlet.
Public health nurses from district health clinics were identified as research assistants as they are well versed with the demographics of the study areas. They were trained to administer a knowledge questionnaire (refer to Appendix A), to conduct a home safety audit using a checklist (refer to Appendix B), to give immediate feedback, recommendations to caregivers after the audit, to explain an educational material (refer to Appendix D) and to explain the use of a home safety device to caregivers based on an instruction leaflet (refer to Appendix E).
12 Home Safety Practices for Prevention of Poisoning in Young Children
Figure 2: Flow chart of study design Inclusion criteria:
1. All households with children aged 1-4 2. Respondents consented
to participate 3. Respondents able to
converse in English or Malay
Exclusion criteria:
1. Households where only the maid and children are present during the visit
Identification of households with children age 1 -4 (n = 300)
Group 2 (Manjung) (n=150)
Households to receive intervention package 2
1. Immediate post audit feedback & Education
Group 1 (Kinta) (n=150)
Households to receive
Training of public health
Audit 1
Nurses administered questionnaire, carried out 1st audit and implemented intervention package 1.
Audit 1
Nurses administered questionnaire, carried out 1st audit and
implemented intervention package
Evaluation of the effectiveness of intervention package in terms of
1. Safe storage 2. Home safety device 3. New changes by parents eg
use child resistant device
Evaluation of the effectiveness of intervention package in terms of
1. Safe storage
2. New changes by parents eg use child resistant device Nurses administered questionnaire
Evaluation of the effectiveness of intervention package in terms of
1. Safe storage
2. New changes by parents Evaluation of the effectiveness of the intervention
package in terms of 1. Safe storage
2. New changes by parents 3. Home safety device
Phase 0: Sub-study to validate the home safety device
Two home safety devices will be tested on children and adults. The most cost-efficient and effective device was chosen based on the following criteria:
i) At least 85% of children fail to operate the device after 5 minutes without guidance
ii) At least 80% of children fail to operate the device after 5 minutes without guidance, following demonstration by the researcher
iii) At least 85% of adults successfully operate the device after 5 minutes without guidance, following demonstration by the researcher
The most cost-efficient and effective home safety device was chosen and used for the study
Phase 1: Identification of households, baseline audit and intervention implementation
Nurses administered questionnaire
Phase 2: 3 months post intervention audit
Phase 3: 6 months post intervention
13 Home Safety Practices for Prevention of Poisoning in Young Children
to the respondent. An educational material were provided to both intervention groups but the home safety device with instruction leaflet and demonstration of the device by the nurse were provided only to homes in Group 1.
Phase 2
The second audit was conducted after 3 months from the first audit. The same tools as in the first audit were used. Improvements in home poison safety practices were evaluated in both intervention arms. Additional changes made by parents to improve home poison safety practices were assessed in both intervention arms.
Phase 3
The third audit was conducted after 6 months from the first audit. The same tools as in the first audit were used. Improvements in home poison safety practices were evaluated in both intervention arms. Additional changes made by parents to improve home poison safety practices were also assessed in both intervention arms.
Fidelity testing was also done for the audit to monitor the quality of the intervention implementation. This was carried out by telephone calls to the audited respondents based on a Fidelity Test Form (Appendix C). In both intervention arms of each audit, 30 different samples were chosen for fidelity testing each time.
3.2 Intervention Package
1. Immediate post audit feedback and recommendations:
a. Store medication and household products in locked cabinet. b. Keep medication and household products out of reach of children. c. Keep medication in CRCs.
d. The safe places to store medication and household products are the kitchen, bathroom and the storeroom.
e. Safe disposal of medication by removing from the original container and throwing in the trash bin, flush down the toilet if the labels says so and return medication to the pharmacy.
f. Store household products in their original containers.
2. An educational material will be prepared in three languages (Malay language, Mandarin and Tamil) to educate caregivers about safe storage and disposal of medication and household products and home safety practices to avoid poisoning in young children.
14 Home Safety Practices for Prevention of Poisoning in Young Children 3.3 Study Type
This study is an interventional study (non-controlled community trial) conducted in 2 districts with similar demographic distribution in Perak. There was no control group as the researchers feel that it is unethical not to intervene as most children in a household are at risk of poisoning.
3.4 Ethical Considerations
The researchers had obtained approval from the national ethics committee prior to implementing the study. All the information from the questionnaire and audit checklist was kept confidential. No identification data were captured. Verbal consent was obtained and documented before the respondent’s participation in the study. Caregivers were allowed to refuse consent to participate in the study.
3.5 Variables
Table 5. Variables definition
No Variables Operational Definitions Scale of Measurement
1 children at home as obtained by a direct question to the respondent
2 Age of the caregiver
Age in complete years is obtained from respondent to a direct question to the respondent to a direct question to the respondent
1. Malay 2. Chinese 3. India 4. Others
4 Education level of caregiver
Highest education level achieved by respondent as obtained by direct questioning to respondent aged 1-4 obtained from direct question to the respondent
15 Home Safety Practices for Prevention of Poisoning in Young Children
No Variables Operational Definitions Scale of Measurement
6
Number of adult persons who stay in the house available obtained by direct observation by research from direct question to the respondent
storage obtained from direct question to the respondent
Reported practice of disposal of medication obtained from direct question to the respondent
Correct Incorrect
(Based on criteria#)
12 young children posed to the respondent
Percentage of
16 Home Safety Practices for Prevention of Poisoning in Young Children
No Variables Operational Definitions Scale of Measurement
13
Possible rate of poisoning in household of young child
Specific question on prior experience of poisoning in the past year in young children in the family
Rate per 1000 children per year
Specific question on any experience of poisoning in the past year in young children in the family or relatives
Specific question on young child behaviour toward medication/household chemicals to young children posed to the respondent knowledge on safe storage of medication poisoning/ household chemicals to young children posed to the respondent
Open ended
3.6 Sampling
The sample size for the study was calculated using the Epicalc 2000 software. A similar study carried out shows that about 20% of homes have good home poison safety measures in place (Kimberly E, et al Home Safety in Inner Cities: Prevalence and Feasibility of Home Safety Product Use in Inner City Housing Pediatrics 2007). Setting the significance level at 0.05 with a study power of 90% and assuming an improvement in home poison safety practices level from 20% to 40%, the calculated sample size was 108 for each intervention arm. After considering an estimated 30% attrition rate, the sample size was set at 150 for each intervention arm.
Random quota sampling of households which fulfil the inclusion and exclusion criteria was carried out.
The following are the inclusion criteria for houses selected for the study: 1. Households with children aged 1 to 4 years
17 Home Safety Practices for Prevention of Poisoning in Young Children
3. The respondents are able to converse in either English or Malay
The following are the exclusion criteria for houses selected for the study: 1. Households where only the maid/babysitter is present during the visit
The samples were randomly chosen from the Birth Registration Book from Year 2004 till Year 2007. The homes identified were sampled into two intervention arms. Caregivers in Group 1 received intervention package which consists of an immediate post audit feedback, an educational pamphlet and a home safety device while caregivers in Group 2 received intervention package which consists of an immediate post audit feedback and an educational pamphlet.
3.7 Techniques for Data Collection & Pre-Testing
Baseline data collection and data collection during each of the subsequent audits were carried out by trained public health nurses using a questionnaire (refer Appendix A) and an audit checklist (refer Appendix B). The questionnaire is used to determine the level of knowledge of caregivers on home poison safety practices including safe storage and safe disposal to prevent accidental poisoning in young children.
3.8 Plan for Data Analysis and Interpretation (Include Dummy Tables)
SPSS version 15.0 and Epicalc 2000 were used to analyse the results of the study.
4.0 RESULTS
4.1 Results of Evaluation of Safety Device
A total of 133 children and their accompanying caregivers were involved in a sub-study to decide which safety device was more efficacious to be used in the intervention package of the main study. Safety Device 1 is the Patrull Drawer/Cabinet Lock and Safety Device 2 is the Patrull Multilock.
Some of child-caregiver teams were tested on Safety Device 1 only (66), some on Safety Device 2 (104) and some were tested on both devices.
This sub-study, to validate the home safety device, showed only Safety Device 2 (Patrull Multilock) to be efficacious which was then used in the intervention package for Kinta District in the main study. A total of 100 (96.2%) out of 104 children failed to open Safety Device 2 on their first try and 89 (89.0%) out of 100 children failed to open Safety Device 2 on their second try. All 104 (100%) accompanying caregivers/ adults successfully opened Safety Device 2 (Table 6).
18 Home Safety Practices for Prevention of Poisoning in Young Children failed to open Safety Device 1 on their second try. For the device to be considered efficacious, 85% of children tested should fail to open the Safety Device within the 5 minutes allocated on their first try and 80% of children should fail on their second try after the investigator demonstrates how to open the lock. We did not continue our study on Safety Device 1 after we found out that Safety Device 1 was no longer available for purchase in this country. Hence only 66 instead of the planned 100 children were tested on Safety Device 1 (Table 6).
The mean age of the participating children was 39.24 months (SD 9.42). The minimum age was 18 months and the maximum 68 months. A total of 61 (45.9%) children were male and 72 (54.1%) were female. Their accompanying caregiver was mainly mothers (75.9%), followed by fathers (14.3%), grandmothers (6.8%), grandfathers (1.5%) and others (1.5%). The accompanying caregivers’ mean age was 34.77 years (SD ± 9.09 years). The accompanying caregivers’ minimum age was 21 years old and the maximum 62 years old. Most of the caregivers (69.9%) of them had up to secondary level education.
Out of the 4 children who could open safety Device 1 on their first try, 3 were males. On their second try eleven out of 18 children who successfully opened Safety Device 1 were males. The same trend was seen with Safety Device 2 whereby 3 out of 4 children who were successful on their first try were males and 8 out of 11 children successful on their second try were males.
4.2 Socio-demographic Data
For the first audit, 146 households were evaluated from the Kinta District and 150 from the Manjung District. 8 (6.1%) households dropped out in the Kinta District for the second audit and 12 (8.0%) from Manjung. For the third audit another 8 households dropped out in Kinta District and another two (1.4%) households dropped out from Manjung (Table 7).
Socio-demographic data comparing both the districts at baseline is shown in Table 8. There was no significant difference in terms of relationships of the caregivers to the child, age, ethnicity and education level of the caregivers.
19 Home Safety Practices for Prevention of Poisoning in Young Children
Only 30 (20.4%) households in Kinta District (Group 1) compared to 79 (52.7%) households in Manjung District (Group 2) had good knowledge (Table 9).
Most caregivers in Kinta District (Group 1) perceived their children to be safe from poisoning at home with 113 (77.4%) households safe from medication poisoning and 120 (81.6%) from chemical poisoning. The same results were seen in Manjung (Group 2) with 122 (81.3%) households perceiving their children to be safe from medication poisoning and 121 (80.7%) households safe from chemical poisoning (Table 9).
Good knowledge and high perception did not ensure a safe home in prevention of poisoning in children as the data from Manjung (Group 2) revealed that although they had better scores in knowledge and perception, only 21.3% of households were safe when audited as compared to 48.6% in Kinta District (Audit 1) as shown in Figure 3 and Figure 4.
Number of poisoning in children in the past year was 4 (0.91%) in the Kinta District and 6 (1.26%) in the Manjung District. (The incidence of accidental poisoning in this age group in Perak is about 3% and international data for developing countries is 5%.) The incidence of poisoning per 1000 children per year in the Kinta District was 9.11 compared to 12.55 in the Manjung District. (p-value 0.85).
Table 7. Number of respondents for each audit visit by district
Audit Kinta District Manjung District
1st Audit 146 150
2nd Audit 138 138
3rd Audit 130 136
Table 6. Validity of safety device by ability of child and caregiver to open a drawer/cabinet
Safety Device 1 (Patrull Drawer/ Cabinet Lock) n = 66
Safety Device 2 (Patrull Multilock)
n = 104
Child Attempt 1 (Inability of child to
open the drawer with safety device) 62 (93.9%) 100 (96.2%)
Child Attempt 2 (Inability of child to
open the drawer with safety device after a demonstration)
45 (72.6%) 89 (89.0%)
Parent Attempt (Ability of parent to
open the drawer with safety device after a demonstration)
20 Home Safety Practices for Prevention of Poisoning in Young Children
Table 8. Socio-demographic characteristics comparing both the districts at baseline
Socio-demographic
Relationship to the child
Father 4 7
Number of children in households
Total number 439 478
-Mean number (SD) 2.99 (1.49) 3.19 (1.82)
-Ethnicity
Lower education 29 33 0.67 comparing
lower and higher education level
21 Home Safety Practices for Prevention of Poisoning in Young Children
Table 9. Knowledge on safe medication, chemical storage, disposal, poisoning numbers
& rates and perception of caregivers
Pre-intervention (Audit 1)
Group 1 (n=147)
Group 2
(n=150) p-value
Knowledge on safe medication & chemical storage & disposal
Number of poisoning in household in past year 4 (2.8%)
6
(4.0%) –
Number of poisoning in children in past year 4 (0.91%)
6
(1.26%) –
Rate per 1000 children per year 9.11 12.55 0.85
Possible poisoning in young child of household or relative in the past (excluding above)
6 (4.1%)
4
(2.8%) –
Perception of Caregivers
No access of young child to medication in household
113 (77.4%)
122
(81.3%) 0.40
No access of young child to chemical in household
120 (81.6%)
121
(80.7%) 0.83
Table 10: Safety of household for pre and post intervention audits by district
Safety of household
Pre-intervention Post-intervention
Audit1 Audit 2 Audit 3
22 Home Safety Practices for Prevention of Poisoning in Young Children
Figure 3. Pre-intervention knowledge assessment compared with households’ safety
practices (Audit 1) by district
Figure 4. Knowledge and perception compared with households’ safety practices (Audit
23 Home Safety Practices for Prevention of Poisoning in Young Children
Figure 5. Overall household safety for pre- and post-intervention audits by district
showing 95% CI
Figure 6. Household safety for Medication pre- and post-intervention audits by district
24 Home Safety Practices for Prevention of Poisoning in Young Children Table 10 above and Figure 5 below show the key outcomes of the three audits by district. The initial overall safe households were higher in Kinta (Group 1) than in Manjung (Group 2). It can be clearly seen that there was a statistical significant increase in the percentage of safe households in both districts. Kinta (Group 1) had an increase from 48.6% to 93.9%, while in Manjung (Group 2) the increase was from 21.3 to 67.7% over 7 months. The significant increase of safe households continued in Kinta from audit 2 and 3, however in Manjung the increase plateaued after audit 2.
Households within Manjung (Group 2) had lower rates of safe homes for both medication and chemicals when compared to Kinta (Group 1) households. The increase in safe households in both districts was similar for medication and chemicals as shown in Figure 4 and Figure 5.
5.0 DISCUSSION
5.1 Statement of Principal Finding
At baseline (Audit 1) between 29.3-40.3% of urban and semi-urban households in Perak have safe home safety practices to prevent poisoning in young children.
Figure 7. Household safety for Chemical pre- and post-intervention audits by district
25 Home Safety Practices for Prevention of Poisoning in Young Children
At baseline (Audit 1), 40.4-56.8% of households in the Kinta District were found to be safe in prevention of poisoning compared to 14.7-28.0% in the Manjung District. In Kinta, more households (66.8-81.2%) were safe for prevention of household chemicals poisoning compared to medication poisoning (43.9-60.3%). In Manjung, the rates for safety from household chemicals poisoning and medication poisoning did not differ much at 28.2-43.8% and 33.4-49.3%, respectively.
However only 30 (20.4%) households in the Kinta District compared to 79 (52.7%) households in the Manjung District had good knowledge when assessed at audit 1. Households in Kinta and Manjung had similar high rates in perceiving their children to have no access to medication and household chemicals, 77.4% and 81.6% respectively in Kinta and 81.3% and 80.7% in Manjung.
The percentage of safe households in the Kinta District improved significantly to between 60.2-76.0% after Audit 2 and further to between 89.7-98.0% after Audit 3. Manjung also showed significant improvement to between 52.6 – 69.1% after Audit 2 but plateaued at 59.7-75.6% at Audit 3. The sustained improvement in Kinta District may be attributed to the Safety Device.
Knowledge does not affect practice as demonstrated by the findings from the Manjung District.
Number of poisoning in children in the past year was 4 (0.91%) in the Kinta District and 6 (1.26%) in the Manjung District. The incidence of poisoning per 1000 children per year in the Kinta District was 9.11 compared to 12.55 in the Manjung District.
In Audit 2, 88.4% households were satisfied with the device and this was sustained in Audit 3. However, satisfaction or dissatisfaction with the device did not affect safety practices in the household.
5.2 Strengths and Weaknesses of the Study
This study did not assess post intervention knowledge at Audit 2 and Audit 3 as it was considered that the audit conducted with carers was superior to conventional health education using leaflets.
There was no control group as it will be unethical not to intervene in those households at risk. The Manjung district was used as a “partial control” as no safety device was provided in the intervention package.
26 Home Safety Practices for Prevention of Poisoning in Young Children This study did not evaluate the use of the safety device. Instead, the study focused on evaluating the satisfaction of caregiver with the device. The majority of caregiver involved in the study was female and this may have contributed to the success of the intervention.
5.3 Strengths and Weakness in Relation to Other Studies
Rate of Unsafe Households
This study shows 60-71% of urban and semi-urban households in Perak have unsafe homes. The figure is comparable to a study done in urban lower income households in the USA where 77% of homes were not safe in preventing poisoning in children (Kimberly E. et al. 2007).
Improvement Rate of Safe Household
In this study, good knowledge and high perception did not affect practice. This is similar to finding in other studies. A study in Turkey shows that 69% of mothers claimed to have taken preventive measures after their child had a poisoning accident at home but they did not even mention at all basic precautions such as storage of poisonous agents on different shelves and storage of medication and household chemicals in locked cabinets (Sibel E. et al. 2006). 76.1% of mothers only mentioned keeping the medication out of the reach of children.
The study in the USA also shows that caregiver reports of poison safety/storage (71%) were falsely higher than if evaluated by a home safety checklist/audit (17%) (Kimberly E. et al. 2007). This strongly suggests that home audit rather than conventional education or questionnaire alone is a more powerful tool to identify unsafe home as well as to make significant changes in practices. The audit not only gathers information but also educates the respondents and ensures that correct practices are adhered to.
The use of the safety device may have contributed to further improvement but this needs to be studied further.
Community-based prevention educational programmes are an important component in preventing poisonings and have been shown to change parental poison storage habits (Maiesl G. et al. 1967 as quoted by John T. Arokiasamy in an editorial Accidental Poisoning: Selected Aspects of its Epidemiology and Prevention Med. J. Malaysia June 1994).
27 Home Safety Practices for Prevention of Poisoning in Young Children
lower in this study as the denominator includes all children in the household aged 0-12 years of age.
5.4 Meaning of the Study (Possible Mechanism and Implication for Clinicians/ Policymakers)
The high rate of unsafe households i.e. between 60-71% of urban and semi-urban households calls for some intervention to improve the situation. The single most powerful means of change is the Home Safety Audit Tool.
5.5 Unanswered Questions and Future Research
One concern is whether parents will sustain good home poison safety practices after this study is over. The fact that caregiver were aware that health personnel were returning for an audit may have contributed to them maintaining safe home practices. This could be answered by an unannounced audit one year after the 3rd Audit.
It was uncertain from the study what impacts the use of a safety device had in changing the household behaviour to prevent poisoning. Finally, the rate of unsafe household in rural communities is not known and needs to be investigated.
6.0 CONCLUSION & RECOMMENDATIONS
This study shows between 60-71% of urban and semi-urban households in Perak have unsafe home safety practices to prevent poisoning in young children.
The intervention package, mainly the Home Safety Practices Audit developed by the researchers for this study, significantly improved home poisoning safety practices. 75.7-85.3% of urban and semi-urban households in Perak had a safe home to prevent poisoning in children at the end of the study.
Addition of the safety device with the Home Safety Practices Audit further improves home poisoning safety practices.
Knowledge and perception does not ensure a safe household in preventing poisoning in young children.
Recommendation:
1. There is a need to support parents to make their home poison safe.
28 Home Safety Practices for Prevention of Poisoning in Young Children
REFERENCES
1. K Chatsantiprapa, J Chokkanapitak N Pinpradit Host and environment factors for exposure to poisons: a case-control study of preschool children in Thailand. Injury Prevention 2001;7, 214-217.
2. E Towner, T Dowswell, S Jarvis. Updating the evidence. A systematic review of what works in preventing childhood unintentional injuries; Part 1. Injury Prevention 2001;7:161-164.
3. E Towner, T Dowswell and S Jarvis.Updating the evidence. A systematic review of what works in preventing childhood unintentional injuries; Part 2. Injury Prevention 2001;7:249-253.
4. L T Lam. Childhood and adolescence poisoning in NSW, Australia: an analysis of age,sex,geographic, ad poison types. Injury Prevention 2003;9:338-342.
5. Audrey T Hingley. Preventing Childhood Poisoning. FDA Consumer magazine March 1996.
6. Sibel Erkal, Sukran Safak. An evalution of the poisoning accidents encountered in children age 0-6 years in Kirikkale. The Turkish Journal of Pediatrics 2006;48:294-300 7. C Chien, JL Marriott, K Ashby, J Ozanne-Smith. Unintentional ingestion of over
the counter medications in children less than 5 years old. J Puediatr Child Health 2003, 39, 264-269.
8. Accident Poisoning in Children. http://www.alegent.com
9. H M Wiseman, K Guest, V S Murray, G N Volans. Accident poisoning in childhood: a multicentre survey. 2. The role of packaging in accidents involving medications. Hum Toxicol. 1987 Jul; 6, 4, 303-14 3623576, P, S, E, B, Cited:1.
10. National Poison Prevention Week. www.poisonprevention.org.
11. T Schroeder, M S, C Irish, other staf member. Nonfatal, Unintentional Medication Exposures Among Young Children-United States, 2001-2003. JAMA. 2006;295 (8): 882-884
12. How To Manage Your Medications. Bahagian Perkhidmatan Farmasi Kementrian Kesihatan Malaysia, Gabungan Persatuan-Persatuan Pengguna-Pengguna Malaysia. 13. K Chatsantiprapa, J Chokkanapitak, N Pinpradit. Host and environment factors for
exposure to poisons: a case-control study of preschool children in Thailand. Injury Prevention 2001;7:214-217.
14. F Cheraghali, M Taymori. Epidemiological Study Of Drug Intoxication In Children. Acta Medica Iranica, 44 1:37-40;2006.
15. L Gibbs, E Waters, J Sherrard, J Ozanne-Smith, J Robinson, S Young, A Hutchinson. Understanding parental motivators and barriers to uptake of child poison safety strategies: a qualitative study. Inj Prev 2005;11;373-377.
29 Home Safety Practices for Prevention of Poisoning in Young Children
17. Odd RW, Laing G, Thompson M, Logan S, Jacobs M, Williams JM. Child resistant packaging should be legal requirement. BMJ Volume 316; 9 May 1998:1461. 18. Minerva, Jacson R H. Poisoning and child resistant containers. BMJ VOLUME 305;
29 August 1992:522.
19. Sharon Conroy, Jacqueline Collier, Nicola Birchley, Karen Neil, Sarab Rodgers, John Mc Intyre, Imti Choonara, Anthony Avery. An examination of the risk management issues in the handling at home of over-counter medicines purchased for children. The Pharmaceutical Journal, Vol 271;16 August 2003:209-213.
20. Morang MacKay, Dana C Reid, David Mother, Terry Klassen. Systematic Review of the Relationship Between Childhood Injury and Socio-economic Status.
21. Deborah C Girasek. Public beliefs about the preventability of unintentional injury deaths. Accident analysis and Preventio 33;2001, 455-465.
22. RC Nelson, DJ Brancato, GD Armstrong. Poisoning among Young Children – United States. CDC, MMWR, Weekly March 16, 1984/33 10;129-31.
23. Proper Disposal of Prescription Drugs. Oice of National Drug Control Policy; February 2007.
24. L Gibbs, E Water, J Sherrard, J Ozanne-Smith, J Robinson, S Young, A Hutchinson. Understanding parental motivators and barriers to uptake of child poison safety strategies: a qualitative study. Inj Prev 2005;11;373-377.
25. Mohd Zain Z, Fathelrahman A I, Ab Rahman A F. Characteristics and outcome of paracetamol poisoning cases at a general hospital in Northern Malaysia. Singapore Med J 2006;47;2:134-136.
26. Child Resistant Packaging Saves Lives. The U S Consumer Product Safety Commission, Washington, D C 20207
27. Andrew L Dannenberg, Carolyn J Fowler. Evaluation of interventions to prevent injuries: an overview. Inj Prev 1998’4’141-147.
28. Julie L hoy, Lesley M Day, James Tibballs, Joan Ozanne-Smith. Unintentional poisoning hospitalisations among young children in Victoria. Inj Prev 1999;5;31-35. 29. L T Lam. Childhood and adolescence poison in NSW, Australia: an analysis of age,
sex, geographic, and poison tapes. Inj Prev 2003; 9; 338-342.
30. E Towner, T Dowswell, S Jarvis. Updating the evidence. A systematicreview of what works in preventing childhood unintentional injuries: Part 1. Inj Prev 2001;7;161-164.
31. E Towner, T Dowswell, S Jarvis. Updating the evidence. A systematicreview of what works in preventing childhood unintentional injuries: Part 2. Inj Prev 2001;7;249-253.
32. Nonfatal, Unintentional Medication Exposures Among Young Children-United States, 2001-2003. JAMA 2006;295 8;882-884.
30 Home Safety Practices for Prevention of Poisoning in Young Children 34. Protect Your Child from Poisons in your home. http://www.fda.gov.
35. Home Safety Checklist. http://www.chop.edu.
36. Poisoning Fact Sheet. Visit American Association of Poison Control Centers website www.aapcc.org.
37. Medicine and Children. www.knowyourmedicine.com.my, www.pharmacy.gov.my. 38. The Children’s Hospital of Philadelphia. A pediatric healthcare network. http://
www.chop.edu.
39. Poison prevention. http://www.cincinnatichildrens.org.
40. Lynn Calman, Emily Finch, Beverley Powis, John Strang. Only half of patients store methadone in safe place. BMJ Volume 313;7 December 1996:1481.
41. Gregory B Rodgers. The Safety Effects of Child-Resistant Packaging for Oral Prescription Drugs. JAMA, June 5, 1996-Vol 275, No 21:1661-1665
42. Betty R Kirkwood, Jonathan A C Sterne. Essential Medical Statistics. Published by Blackwell.
43. RJ Flanagan, C Rooney, C Griiths. Fatal Poisoning In Childhood, England And Wales 1968-2000. http://www.sciencedirect.com.
44. Roger N Bloor, Rosanna McAuley, Norman Smalldridge. Safe storage of methadone in the home – an audit of the efectiveness of safety information giving. Harm Reduction Journal 2005, 2; 9.
45. Kimberly E Stone, Emmanuella M Eastman, Andrea C Gielen, Barbara Squires, Dana Kaplin, Janet R Serwint. Home Safety in Inner Cities: Prevalence and Feasibility of Home Safety-Product Use in Inner-City Housing. Pediatrics 2007; 120; e346-e353. 46. J Nixon, A Spinks, C Turner, R McClure. Community based programs to prevent
poisoning in children 0-15 years. Inj Prev 2004;10;43-46.
ACKNOWLEDGEMENT
31 Home Safety Practices for Prevention of Poisoning in Young Children
41
ISBN
Efective Implementation of a
Structured Psychoeducation
Programme among Caregivers
of Schizophrenia Patients in the
Community
Health Systems Research 2008/2009
Authors
Paranthaman Vengadasalam Jelapang Health Clinic
Satnam Kaur Harbhajan Singh Bahagia Ulu Kinta Hospital
Jean-Li Lim
Slim River Health Clinic
Amar-Singh HSS
Clinical Research Centre Perak, Department of Paediatrics,
Hospital Raja Permaisuri Bainun Ipoh, Perak
Sondi Sararaks
Institute of Health Systems Research
Nafiza Mat Nasir Tanjung Malim Health Clinic
Ranjit Kaur Praim Singh Perak State Health Department
Asmah Zainal Abidin Perak State Health Department
Clinical Research Centre (CRC) Perak recommends using the following statement to cite this report in our publication entitled “Health System Research (HSR) in Perak 2006-2009: Using Research to Make a Difference”:
42 Efective Implementation of a Structured Psychoeducation Programme among Caregivers of Schizophrenia Patients in the Community
Contents of Report
page
Abstract 43
1.0 Introduction 48
2.0 Objectives 48
2.1 General objective
2.2 Specific objectives
3.0 Methodology 49
3.1 Overview of research design
3.2 Study type
3.3 Ethical considerations
3.4 Variables
3.5 Sample size and sampling method
3.6 Data collection tools and techniques 3.7 Data analysis and interpretation
4.0 Results 55
4.1 Socio-demography of caregivers
4.2 Socio-demography of patients
4.3 Knowledge of caregivers on schizophrenia 4.4 Outcomes of patients with schizophrenia 4.5 FBIS/SF score of caregivers
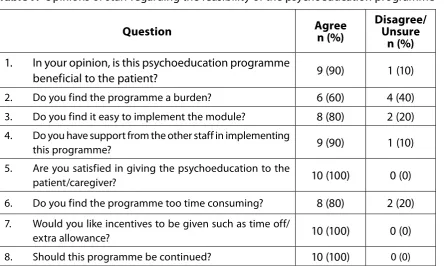
4.6 Feasibility of the psychoeducation programme
5.0 Discussion 64
5.1 Key findings
5.2 Comparison with other studies
5.3 Limitations of the study
6.0 Conclusion & Recommendations 67
Acknowledgement 68
References 68
43 Efective Implementation of a Structured Psychoeducation Programme among Caregivers
of Schizophrenia Patients in the Community
ABSTRACT
Effective Implementation of a Structured Psychoeducation Programme among Caregivers of Schizophrenia Patients in the Community
Paranthaman Vengadasalam1, Satnam Kaur Harbhajan Singh2, Jean-Li Lim3, Amar-Singh HSS4,7,Sondi Sararaks5, Nafizah Mat Nasir6, Ranjit Kaur Praim Singh8, Asmah Zainal Abidin8
1 Jelapang Health Clinic, Perak. 2 Bahagia Ulu Kinta Hospital, Perak. 3 Slim River Health Clinic, Perak. 4 Clinical Research Centre Perak. 5 Institute of Health Systems Research. 6 Tanjung Malim Health Clinic, Perak.
7 Department of Paediatrics, Hospital Raja Permaisuri Bainun Ipoh, Perak 8 Perak State Health Department.
Introduction & Objectives
Psychoeducation has shown promising benefits in managing patients with schizophrenia. In Malaysia, the use of psychoeducation is rather limited and its impact indeterminate. This study was to assess the effectiveness of a structured psychoeducation programme for the community in improving caregiver knowledge, decreasing caregivers’ burden, reducing patients’ readmission and defaulter follow-up rates.
Methodology
This was a controlled interventional study involving caregivers of adults with schizophrenia. Subjects for the interventional and control group were selected from seven separate community clinics. All respondents identified were given the demographic survey, pre-test questionnaire and The Family Burden Interview Schedule - Short Form (FBIS/SF) prior to intervention. The respondents in the interventional group went through a structured psychoeducational program followed by an immediate post-test questionnaire after the completion of the modules. Caregivers were assessed at baseline, 3 and 6 months post-intervention for knowledge and burden using the knowledge questionnaire and FBIS/SF. Patients were monitored for relapse and defaulting treatment. The staff was also required to complete a survey form regarding their opinion of the whole psychoeducation program 3 months into the programme.
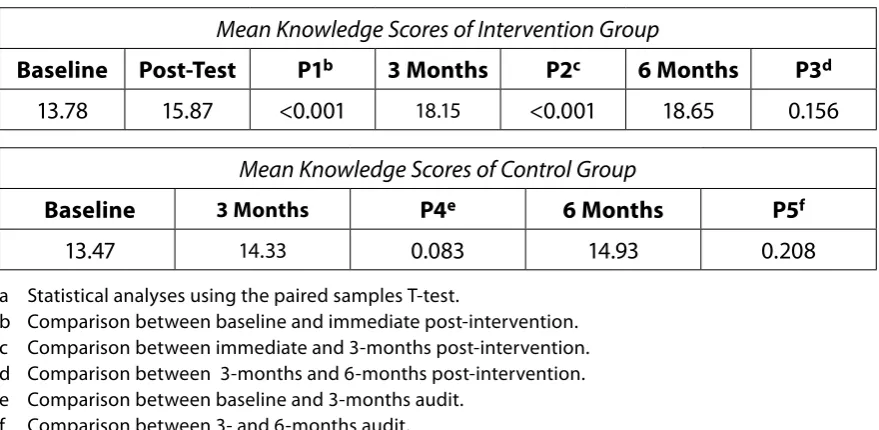
Results
44 Efective Implementation of a Structured Psychoeducation Programme among Caregivers of Schizophrenia Patients in the Community vs. 18.2%, p=0.047), and mean duration of illness was shorter in the intervention group (below 10 years: 48.1 vs. 28.8%, p=0.04). Caregivers in the intervention group showed significant improvement in knowledge scores (18.65 vs. 14.93, p<0.001), reduction in burden of assistance in daily living (severity, p<0.001) and reduced patient defaulter rate. All staffs involved in the psychoeducation program were satisfied in giving the program and 90% agreed that the program had been beneficial to the patient.
Conclusion
The findings support the use of a structured psychoeducation program among caregivers of patient with schizophrenia in the community.
Keywords
45 Efective Implementation of a Structured Psychoeducation Programme among Caregivers
of Schizophrenia Patients in the Community
1.0 INTRODUCTION
1.1 Background
Worldwide, mental health problems present as the fifth most common cause of disability and are associated with a significant burden of morbidity. In Malaysia, schizophrenia presents as the main mental health problem. The burden of this disease has increased over the years. The National Mental Health Registry in Schizophrenia showed a 8.07% increase in registered cases in the year 2004 with 2436 cases to the 2254 cases in 2003 (Aziz SA, 2006).
1.2 Benefits of psychoeducation
Aside from the usual pharmacological treatment, psychoeducation has shown great promise in the management of schizophrenia. Psychoeducational approaches have been developed to increase patients’ and their carers’ knowledge of, and insight into, their illness and treatment. A review of more than 30 randomised clinical trials have shown that family psychoeducation reduces the rate of relapses, encourages recovery of patients as well as improves family dynamics among participants (McFarlane WR et al., 2003). A recent study showed a significant reduction in patient rehospitalisation rates and improved compliance over a period of 2 years after patients and their families attended a psychoeducational programme consisting of 8 sessions (Pitschel-Walz G et al., 2006). In the Asian setting, similar results were observed among Chinese patients in Hong Kong (Chien WT et al., 2007).
Family psychoeducation is a method of working in partnership with families to impart current information about mental illness and to help them develop coping skills for managing problems posed by mental illness in their family. This approach respects and incorporates the individual, family, as well as cultural realities and perspectives. It almost always fosters hope in place of desperation and demoralisation.
Increasingly, mental health facilities are pressured to meet the demands of service and productivity. Mental health program leaders find they need to direct services that will satisfy these demands without sacrificing the quality of care being offered. At the same time, program leaders are concerned about practitioners’ level of satisfaction. The American Psychiatric Association and the Agency for Health Care Policy and Research cite family psychoeducation as one of the most effective ways to manage schizophrenia (APA, 2004). Research has shown that there is a significant reduction in relapse rates (by at least 50% of previous rates) when family intervention, multi-family groups, and medications are used concurrently.
46 Efective Implementation of a Structured Psychoeducation Programme among Caregivers of Schizophrenia Patients in the Community 1. Promote improved clinical outcomes, satisfaction, and higher rates of recovery
amongst their clients
2. Feel more supported in their efforts to manage the effects of illness 3. Build relationships with families
4. Experience improved cost-benefit ratios
For consumers, the practice of family psychoeducation: 1. Helps build a support network for recovery 2. Provides hope
3. Reduces relapse and hospitalisation 4. Improves symptom management 5. Reduces medication dosages
6. Improves social skills and community participation 7. Increases employment, earnings, and career options 8. Strengthens family ties
9. Reduces family conflicts
1.3 Rationale of study
However, the application of family psychoeducation in Malaysia has been rather limited and very recent. In June 2004, the Bahagia Ulu Kinta Hospital Psychoeducation Team (HBUK-PET) was initiated to conduct courses to train facilitators who will provide education to clients and their caregivers.
The HBUK-PET programme consists of 5 modules as below: 1. Understanding your illness
2. Understanding your treatment 3. Helping yourself prevent relapses 4. Avoiding and handling crisis
5. Healthy lifestyle – diet and exercise
Following the initiation of this programme, there was encouraging results from both the client as well as their caregivers. Notably, there was an increase in the quality of life in both the client as well as their caregivers. Relapse rates were also lower as they were able to recognise the early warning signs of possible relapse (Ghaus Z, 2006).
47 Efective Implementation of a Structured Psychoeducation Programme among Caregivers
of Schizophrenia Patients in the Community
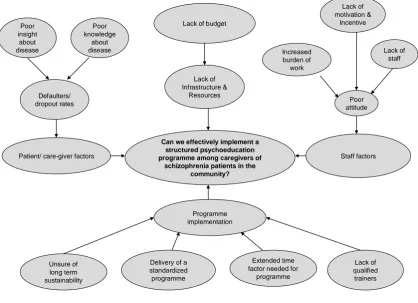
1.4 Problem analysis
The main aim of this study is to assess if a structured psychoeducation programme can be effectively implemented among schizophrenia patients in the community (please refer to Figure 1). However, the researchers foresee some possible problems with implementation of this study.
Similar programmes have been implemented in many psychiatric institutions in Malaysia. The HBUK-PET programme has been shown to be successful in the short term, but the long term sustainability has yet to be studied locally. There is a need to ensure that the delivery of the psychoeducation programme is standardised and less operator dependent. To ensure success of the programme, adequate trainers must be available to impart the knowledge needed. With this, the issue of time, budget, and suitable infrastructure and resources is crucial.
Issues with staff are inseparable from the success of the programme. Adequate staff is needed for the programme to be carried out so that the existing staff is not over-burdened, considering the ever-widening scope of the primary healthcare. Staffs need to have the correct attitude to run the programme. Incentives (allowance, promotional prospects) should be considered to motivate and drive the staff.
Can we effectively implement a structured psychoeducation programme among caregivers of
schizophrenia patients in the community?
48 Efective Implementation of a Structured Psychoeducation Programme among Caregivers of Schizophrenia Patients in the Community Finally, the final outcome of the programme will depend largely on patient and caregiver factors. Defaulter and drop-out rates will largely depend on the patients’ insight and existing knowledge and understanding about the illness. Thus, this programme aims to increase both the insight and knowledge of disease through a structured psychoeducation programme.
With all these issues in mind, our study will perhaps shed some light on improving system of care for schizophrenia patients and ultimately improve the health outcome for these patients and their families.
1.5 Potential utilisation of research
This study hopes to describe the effectiveness of family psychoeducation in terms of increasing the knowledge of schizophrenia among caregivers and its sustainability. The study will also describe the feasibility of the programme in the community setting. Since many studies showed that the psychoeducation programme has impact on patient care, therefore with this study it may change our care of patient with schizophrenia especially in community setting. Ultimately it is hoped that the study will help to improve the current health status and outcome of psychiatric patients currently on follow up in the community.
2.0 OBJECTIVES
2.1 General objective
To compare the effectiveness of a structured versus non-structured psychoeducation programme among caregivers of patients with schizophrenia in the community of an administrative region.
2.2 Specific objectives
1. To determine if the use of a structured psychoeducation programme will significantly:
a. improve the knowledge about schizophrenia among caregivers b. decrease patient readmission rates
c. improve compliance to follow up d. decrease the burden of caregivers
2. To determine the feasibility of the structured psychoeducation programme among the staff implementing it.
49 Efective Implementation of a Structured Psychoeducation Programme among Caregivers
of Schizophrenia Patients in the Community
3.0 METHODOLOGY
3.1 Overview of research design
An interventional study was conducted among caregivers of schizophrenic patients in the community of Perak. This study involved 7 health clinics in the state, of which 3 and 4 were allocated into the intervention and control groups respectively. The intervention used was the introduction of a structured psychoeducation programme. Specific health staffs in the interventional group were trained in the structured psychoeducation module, after which gave structured psychoeducation to the caregivers. The control group included caregivers of patients who followed the standard treatment without any structured intervention. The study was conducted in 3 phases. Please see Figure 2 for the diagrammatic description of the study.
Phase 1
Health clinics and patients/caregivers were identified for inclusion into the study and allocated to the intervention and control groups respectively, according to the researchers’ convenience of access to these clinics.
Phase 2
Specifically identified health staffs in the intervention group from the respective clinics were trained in the use of the Structured Psychoeducation Programme Module (Appendix A). Following this, a baseline audit was conducted. All respondents identified in both groups were given the demographic survey, the knowledge questionnaire form, and The Family Burden Interview Schedule-Short Form (FBIS/ SF) prior to the intervention.
Phase 3 (psychoeducation module)
50 Efective Implementation of a Structured Psychoeducation Programme among Caregivers of Schizophrenia Patients in the Community
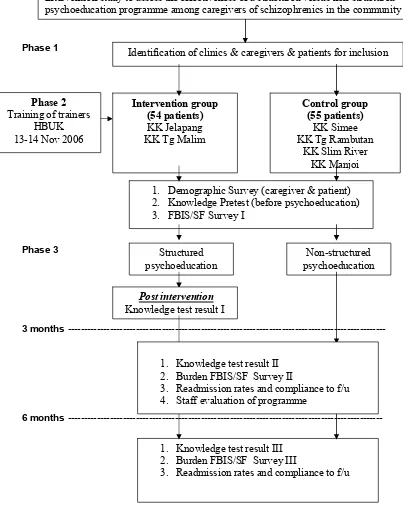
Figure 2. Methodology flow chart
Effective implementation of a structured psychoeducation programme among caregivers of schizophrenia patients in the community
Intervention study to assess the effectiveness of a structured versus non-structured psychoeducation programme among caregivers of schizophrenics in the community
Phase 2
Training of trainers HBUK 13-14 Nov 2006
Identification of clinics & caregivers & patients for inclusion
Control group
1. Demographic Survey (caregiver & patient) 2. Knowledge Pretest (before psychoeducation) 3. FBIS/SF Survey I
Non-structured psychoeducation Structured
psychoeducation
1. Knowledge test result III 2. Burden FBIS/SF Survey III
3. Readmission rates and compliance to f/u
Post intervention
Knowledge test result I
1. Knowledge test result II 2. Burden FBIS/SF Survey II




![Buku BSE SMA KIMIA [KTSP] Kelas X - File guru Kita Bab 8 Bioteknologi](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)