Behavioural Family Intervention with parents of children
with ASD: What do they find useful in the parenting
program Stepping Stones Triple P?
Koa Whittingham
*, Kate Sofronoff, Jeanie Sheffield, Matthew R. Sanders
The University of Queensland, Queensland, Australia
Autism Spectrum Disorders, including Autism and Asperger syndrome, are defined by three key characteristics; social interaction impairments, communication and imagination impairments and stereotyped interests or behaviours (Gillberg, 2002). The prevalence of emotional and behavioural disturbance within the ASD population is significantly higher than within the intellectually disabled population (Brereton, Tonge, & Einfeld, 2006) where it is 2–3 times higher than the normal population (Einfeld & Tonge, 1996).
A R T I C L E I N F O
Article history:
Received 12 January 2009 Accepted 27 January 2009
Keywords:
Parent training
Behavioural Family Intervention Autism Spectrum Disorders Stepping Stones Triple P
A B S T R A C T
This study was conducted in conjunction with a randomised controlled trial of the parenting program Stepping Stones Triple P for parents of children with Autism Spectrum Disorders. The current study concerned examination of the qualitative data arising from the RCT as well as evaluation of the particular parenting strategies that the parents found helpful. The results showed that parents were satisfied with the program, including the partial group format. Further, the majority of participants found the parenting strategies within Stepping Stones Triple P to be helpful, including timeout, physical guidance and blocking. In addition, many of the parents also used the additional strategies of Comic Strip Conversations and Social Stories and the majority of the parents who attempted these strategies found them to be helpful. The clinical implications of the findings are discussed.
Crown Copyrightß2009 Published by Elsevier Ltd. All rights reserved.
* Corresponding author at: Queensland Cerebral Palsy and Rehabilitation Research Centre, Paediatrics and Child Health, School of Medicine, The University of Queensland, Herston Campus, Brisbane, Queensland 4006, Australia.
Tel.: +61 7 3656 5539; fax: +61 7 3656 5538.
E-mail address:[email protected](K. Whittingham).
Contents lists available atScienceDirect
Research in Autism Spectrum
Disorders
Journal homepage: http://ees.elsevier.com/RASD/default.asp
1750-9467/$ – see front matter . Crown Copyrightß2009 Published by Elsevier Ltd. All rights reserved.
1. Parent training and Autism Spectrum Disorders
The treatment of children with ASD has long incorporated the use of specific training programs, involving the training of parents and others to administer behavioural interventions (Koegel, Schreibman, Britten, Burke, & O’Neill, 1982). These programs have been developed to treat specific problems of children with ASD, aiming to improve social behaviour and increase language, as well as to decrease inappropriate behaviours.Lovaas, Koegel, Simmons, and Long (1973)demonstrated that training parents as co-therapists produced better outcomes for children with autism at follow-up than clinic treatment alone.
These specific programs for ASD make use of operant techniques. In spite of the problems that children with ASD may encounter, the core principles of operant conditioning apply to them, just as they apply to typical children (Howlin & Rutter, 1987). Howlin and Rutter have themselves effectively used operant techniques in treating children with autism, including strategies such as time out, prompting, fading, reinforcement and the pairing of tangible rewards with attention, and note a significant reduction in maladaptive behaviours in children in their program.
Specific parenting programs have also been successful in helping parents of children with Asperger syndrome.Sofronoff, Leslie, and Brown (2004)evaluated a parenting program specifically targeting parents of children with Asperger syndrome. The program included psychoeducation, management of behaviour problems, routines, special interests and anxiety. Results from parent reports showed a significant decrease in the number and intensity of problem behaviours and a significant increase in parental self-efficacy (Sofronoff & Farbotko, 2002).
Although the efficacy of these specific parent training programs in treating children with ASD has been well documented, little research has been conducted on the experiences of children with ASD and their parents in standard parenting programs. The current study was conducted in tandem with a randomised controlled trial of the parenting program Stepping Stones Triple P for the ASD population.
2. Stepping Stones Triple P
Stepping Stones is a new variant of the Triple P positive parenting program that specifically targets families of children with disabilities (Sanders, Mazzucchelli, & Studman, 2003). Triple P is a Behavioural Family Intervention with social learning principles as the theoretical basis (Sanders, 1999). The Triple P approach to parenting focuses on providing children with positive attention and managing children’s behaviour in a constructive way that does not hurt the child (Sanders et al., 2003). To this end, the parents are encouraged to develop knowledge, skills and confidence (Sanders, 1999). Stepping Stones Triple P incorporates standard Triple P strategies and includes additional strategies arising from the disabilities literature, developed especially for this population (Sanders et al., 2003; Sanders, Mazzucchelli, & Studman, 2004).
Triple P has an impressive evidence base and has been shown to produce statistically significant and clinically meaningful decreases in the problem behaviour of children that are maintained over time (Sanders, 1999;Sanders, Markie-Dadds, Tully, & Bor, 2000). Triple P’s treatment effect has been replicated in several studies and has been typically associated with high levels of acceptance and satisfaction on the part of the participating parent (Sanders, 1999). Initial research on Stepping Stones Triple P demonstrated that it too has a meaningful treatment effect (Roberts, Mazzucchelli, Studman, & Sanders, 2006). The first randomised controlled trial of Stepping Stones Triple P was conducted with families of children with disabilities including Down’s syndrome, Cerebral Palsy, other genetic syndromes, disability due to accident or disease and developmental disability of unknown origin. Within this trial Stepping Stones Triple P was associated with significant reductions in child problem behaviours as well as significant improvements in parental styles.
3. The current study
reduced child behaviour problems and dysfunctional parenting styles. The results of the RCT are discussed in detail elsewhere (Whittingham, Sofronoff, Sheffield, & Sanders, in press). The current study involves an interpretation of the qualitative data arising from the RCT and an exploration of which of the Stepping Stones parenting strategies the parents found most useful. Stepping Stones as delivered in the trial included the strategies of Comic Strip Conversation and Social Stories (Gray, 1998) and the usefulness of these strategies for parents will also be considered.
4. Methods
4.1. Design
The treatment group received Stepping Stones Triple P and the wait-list group received Stepping Stones after the treatment group had completed the program.
4.2. Participants
The participants were parents/carers of a child aged between two and nine (at point of recruitment) with an Autism Spectrum Disorder. Fifty-nine families participated in total, 29 in the treatment group and 30 in the wait-list group.
All children included in this study had a primary diagnosis of an Autism Spectrum Disorder from a paediatrician. A semi-structured diagnostic interview based upon DSM-IV criteria for Autism and Pervasive Developmental Disorder Not Otherwise Specified and Gillberg’s criteria (Gillberg, 2002) for Asperger syndrome was used to verify a diagnosis of ASD. Participants were matched for functioning according to diagnosis and reported language and randomly allocated to the treatment and wait-list control groups.
No significant differences in demographics were found at pre-intervention between the treatment and the wait-list groups using Chi-Square tests andt-tests as appropriate. Participant characteristics are detailed in the following table,Table 1.
4.3. Procedure
The therapists conducting the intervention were all postgraduate students enrolled in the clinical psychology programe at the University of Queensland. All of the therapists completed a two-day training workshop in Stepping Stones delivered by an accredited practitioner prior to commencing the intervention. Therapist adherence to the protocols was also targeted through weekly supervision sessions with an accredited practitioner. Ethical approval for the study was gained from the University of Queensland research ethics committee in accordance with the standards required by the National Health and Medical Research Council of Australia.
4.4. Intervention
The intervention was run in a partial group format. Participants were placed into groups of four or five, where the target children were at a similar level of functioning. A summary of session content is found inTable 2.
Group format was used for the sessions that involved teaching parenting strategies and an individual format for sessions involving observation, practice and feedback. During the fortnight of practice sessions (sessions five and six) the parents were given one to three individual sessions, as required to achieve competency (Sanders et al., 2003).
4.5. Measures
4.5.1. Family Background Questionnaire
The Family Background Questionnaire consists of demographic data, information on the child’s disability and contact details (Sanders et al., 2003).
4.5.2. Client Satisfaction Questionnaire
This is an adaptation of the Therapy Attitude Inventory developed by Eyberg (1993, as cited in Sanders et al., 2003). It measures the quality of service provided, congruency between the program and the parent’s needs, increased parental skills and decreases in the child’s disruptive behaviours, as well as whether the parent would recommend the program to others. The measure uses 7-point Likert scales and a composite score of program satisfaction can be derived (a maximum score of 91 and a minimum score of 13 are possible). Parents are also asked to provide written comments or suggestions if they wish.
4.5.3. Strategies Questionnaire
The strategies questionnaire was designed for the study. It consists of a list of the strategies that were taught in the intervention including Comic Strip Conversations and Social Stories. The participants were required to indicate whether or not they used each strategy and if they did, whether Table 1
Sample characteristics.
Variables Treatment (N= 29) Control (N= 30) Combined (N= 59) Age of target child 5.62 (SD = 1.74) 6.20 (SD = 2.04) 5.91 (SD = 1.90) Sex of the child
Male 24 23 47
Female 5 7 12
Specific diagnosis on the ASD spectrum (reported)
ASD 11 11 22
Autism 4 4 8
Asperger syndrome 12 15 27
ASD-NOS 2 0 2
Current language abilities (for age)
No language 1 4 5
Little language 6 7 13
Verbal 22 19 41
Professional help sought for child emotional or behavioural problems
Not sought 17 17 34
Sought 12 13 25
Current martial status of parents
Married 21 26 47
Defacto 2 2 4
Divorced 2 1 3
Separated 3 1 4
Never married/defacto 1 0 1
Type of family in which child is currently living
Original 22 27 49
Step-family 1 1 2
Sole parent 5 2 7
Extended 1 0 1
Both parents 15 20 35
Relationship of primary participating parent to the child
Mother 29 25 54
Father 0 4 4
or not they found it helpful. There was also a series of statements about satisfaction with the group format, to which participants responded on a 5-point Likert scale. The Strategies Questionnaire was completed at post-intervention and at follow-up six months later.
5. Results
5.1. Parenting strategies used during program delivery
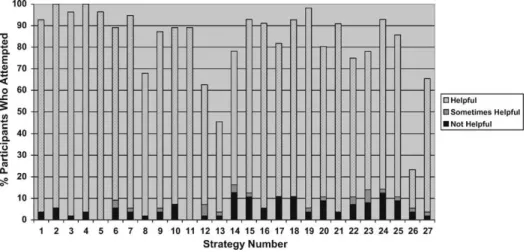
On the Strategies Questionnaire, participants were asked whether they attempted to use each parenting strategy throughout the program, and if they did attempt the strategy whether it was helpful. Fig. 1 illustrates usage for the treatment group and the wait-list group (after receiving treatment) combined. Three participants in the wait-list group elected not to receive Stepping Stones Triple P and therefore are not included in the analyses (N= 56). From the figure it can be observed that for each strategy, including the additional strategies of Comic Strip Conversations and Social Stories, the majority of participants who used a strategy reported that it was helpful.
5.2. Parenting strategies used after completion of program
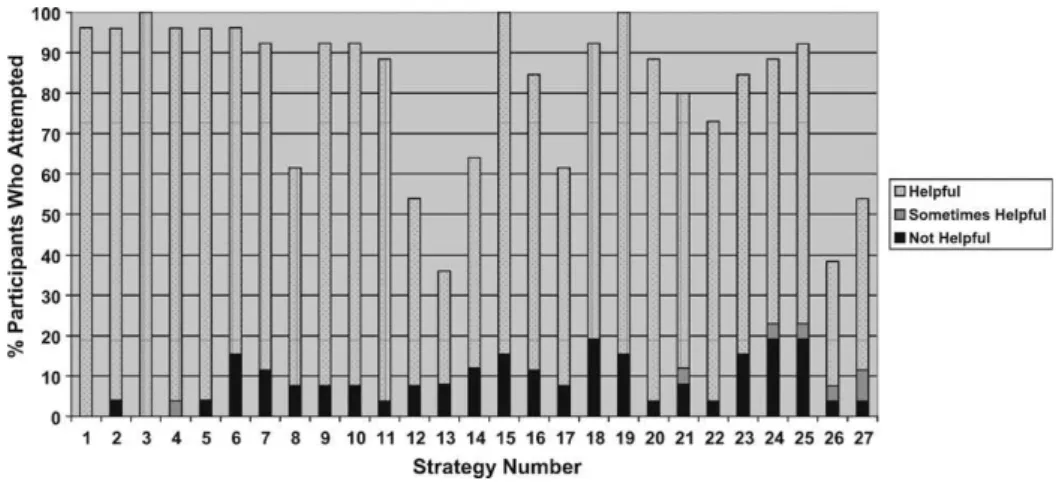
At follow-up participants were asked which strategies they had used in the six months since completing the program. If they did use a strategy during that six-month period they were also asked if they found the strategy helpful.Fig. 2 illustrates those frequencies for the treatment group only excluding the three participants who did not complete the follow-up (N= 26). For each of the strategies the majority of participants who attempted the strategy reported that it was helpful.
5.3. Satisfaction ratings
The ratings of Client Satisfaction as measured by the Client Satisfaction Questionnaire (min = 13, max = 91) were high with a mean rating of 74.25 (SD = 9.98) for the treatment group alone, and a mean of 73.50 (SD = 10.15) collapsed across the treatment and the wait-list groups (after treatment Table 2
Stepping Stones Triple P content.
Week Format Topic
Week one: Introduction Group The basic principles of positive parenting are introduced and the parents are taught to monitor their child’s behaviour Week two: Observation and feedback Individual An observation of a parent-child interaction is performed
and there is feedback of assessment findings including the observation, questionnaires and monitoring Week three: Promoting children’s
development
Group The parenting strategies that focus on developing positive relationships and encouraging desirable behaviour are taught Week four: Managing misbehaviour Group The parenting strategies that relate to the management of
misbehaviour are taught
Week five: Practise Individual The parents are able to set goals and practise specific parenting strategies in session. Feedback is given. Implementation of the strategies at home is discussed Week six: Practise Individual The parents are able to set goals and practise specific parenting
strategies in session. Feedback is given. Implementation of the strategies at home is discussed
Week seven: Planned activities training Group The ability to plan for high-risk situations is taught. In addition, parents are introduced to the strategies of Comic Strip Conversations and Social Stories. These strategies are not currently in Stepping Stones Triple P
Week eight: Implementing planned activities training
Individual Planned activities skills are practised with a visit to the clinic being the high-risk situation. Feedback is given. Implementation of the strategies at home is discussed
Table 3
Strategies included in the Stepping Stones Triple P parenting program.
Strategy Description Applications Developing positive relationships
Spending quality time with children Spending frequent, brief amounts of time (as little as 1 or 2 min) involved in child-preferred activities
Opportunities for parents to become associated with rewarding activities and events, and also for children to share experiences and practice conversational skills Communicating with your children Having brief conversations or interactions
with children about an activity or interest of the child
Promoting vocabulary, conversational and social skills
Showing affection Providing physical affection (e.g., hugging, touching, cuddling, tickling, patting)
Opportunities for children to become comfortable with intimacy and physical affection Encouraging desirable behaviour
Using descriptive praise Providing encouragement and approval by describing the behaviour that is appreciated
Encouraging appropriate behaviour (e.g., speaking in a pleasant voice, playing cooperatively, sharing, drawing pictures, reading, compliance) Giving attention Providing positive non-verbal attention
(e.g., smile, wink, stroke on the cheek, pat on the back, watching)
As above
Providing other rewards Providing tangibles desired by the child (e.g., a toy, mirror, torch, article of clothing, food) with praise and attention
As above – particularly for children who do not respond to praise and attention Providing engaging activities Arranging the child’s physical and
social environment to provide interesting and engaging activities, materials, and age-appropriate toys (e.g., board games,
paints, tapes, books, construction toys)
Encouraging independent play, promoting appropriate behaviour when in the community (e.g., shopping, travelling)
Setting up activity schedules Arranging a series of pictures or words representing activities that children can engage in
Prompting participation in the daily routine of activities
Teaching new skills and behaviours
Setting a good example Demonstrating desirable behaviour through parental modeling
Showing children how to behave appropriately (e.g., speak calmly, wash hands, tidy up, solve problems)
Using physical guidance Providing just enough pressure to gently move a child’s arms or legs through the motions of a task
Teaching self-care skills (e.g., brushing teeth, making bed) and other new skills (e.g., playing with toys appropriately). Also, ensuring compliance with an instruction (e.g., ‘‘put your hands down’’) Using incidental teaching Using a series of questions and prompts
to respond to child-initiated interactions and promote learning
Promoting language, problem solving, cognitive ability, independent play Using ask, say, do Using verbal, gestural, and manual
prompts to teach new skills
Teaching self-care skills (e.g., brushing teeth, making bed) and other new skills (e.g., tidying up)
Teaching backwards Using verbal, gestural, and manual prompts to teach new skills beginning with the last steps of the task
Table 3 (Continued)
Strategy Description Applications Using behaviour charts Setting up a chart and providing social
attention and back-up rewards contingent on the absence of a problem behaviour or the presence of an appropriate behaviour
Encouraging children for appropriate behaviour (e.g., playing cooperatively, asking nicely) and for the absence of problem behaviour
(e.g., tantrums, swearing, hitting) Managing misbehaviour
Using diversion to another activity Using instructions, questions, and prompts to divert a child who may soon misbehave
Establishing ground rules Negotiating in advance a set of fair, specific and enforceable rules
Clarifying expectations (e.g., for watching TV, shopping trips, visiting relatives, going out in the car)
Using directed discussion for rule breaking
The identification and rehearsal of the correct behaviour following rule breaking
Correcting occasional rule breaking (e.g., leaving school bag on floor in kitchen, running through the house)
Using planned ignoring for minor problem behaviour
The withdrawal of attention whilst the problem behaviour continues
Ignoring attention seeking behaviour (e.g., answering back, protesting after a consequence, whining, pulling faces) Giving clear calm instructions Giving a specific instruction to start a
new task, or to stop a problem behaviour and start a correct alternative behaviour
Initiating an activity (e.g., getting ready to go out, coming to the dinner table), or terminating a problem behaviour (e.g., fighting over toys, pulling hair) and saying what to do instead (e.g., share, keep your hands to yourself) Teaching children to communicate
what they want
Teaching a functionally equivalent way of making needs known or met
Dealing with noncompliance, temper outbursts, self-injurious behaviour, pica
Backing up instructions with logical consequences
The provision of a specific consequence which involves the removal of an activity or privilege from the child or the child from an activity for a set time
Dealing with noncompliance, mild problem behaviours that do not occur often (e.g., not taking turns)
Blocking Catching or blocking hands, legs to prevent the completion of a behaviour
Dealing with dangerous behaviour (e.g., reaching for an iron, running out onto the road, attempting to hit themselves) or terminating a problem behaviour (e.g., hitting another person) Using brief interruption Having a child sit quietly were a problem
has occurred for a set time
Dealing with self-injurious behaviour, repetitive behaviour, or struggling during physical guidance Using quiet time for misbehaviour Removing a child from an activity in
which a problem has occurred and having them sit on the edge of the activity for a set time
The removal of a child to an area away from others for a set time
Dealing with children not sitting quietly in quiet time, temper outbursts, serious misbehaviour (e.g., hurting others)
Planned activities Providing engaging activities in specific high-risk situations
received). Additionally, the ratings of satisfaction with the partial group format as measured by the Strategies Questionnaire (min = 5, max = 25) were high with a mean rating of 19.52 (SD = 3.58) for the treatment group alone and a mean of 19.13 (SD = 3.41) collapsed across the treatment and wait-list groups.
5.4. Qualitative findings
The Client Satisfaction Questionnaire and the follow-up Questionnaire offered opportunities for qualitative feedback and this was analysed from the combined group (N= 56). The majority of the Table 3 (Continued)
Strategy Description Applications
Additional strategies
Social stories Facilitation of social understanding through the creation of a short story about a particular situation
Facilitation of social understanding
Comic strip conversations Using simple drawings as visual supports to aid conversation
Promoting conversational and social skills
Fig. 1.The number of participants who attempted each of the strategies during the program, grouped according to those who found the strategy helpful, sometimes helpful and not helpful. Key to strategies utilised:
Number Strategy Number Strategy
1 Quality time 15 Diversion
2 Communicating with children 16 Establishing clear ground rules 3 Showing affection 17 Directed discussion
4 Praise 18 Planned ignoring
5 Giving attention 19 Giving clear, calm instructions 6 Other rewards 20 Teaching to communicate 7 Providing engaging activities 21 Logical consequences 8 Activity schedules 22 Blocking
9 Setting a good example 23 Brief interruption 10 Physical guidance 24 Quiet time 11 Incidental teaching 25 Time out
12 Ask, say, do 26 Comic strip conversations 13 Teaching backwards 27 Social stories
feedback was of a positive nature (66.07%). The positive feedback fell into four key themes. Participants felt that the program was sound, participants reported noticing an improvement in their child’s behaviour, participants reported improvements in their own parenting skills and confidence and, finally, participants felt they had established rapport with their therapists. Areas where participants offered suggestions for improvement included the program having more specific information about ASD, the program containing more information about promoting emotional regulation in their children and changes to the format of the program (particularly longer breaks in between sessions and longer group sessions).
The Client Satisfaction Questionnaire offered participants the opportunity to report other problems with their child that they felt might be related to the original difficulty. The majority of the participants (73.21%) answered ‘no’ or left this question blank. The responses were found to contain three themes: Autistic traits (8.93%), emotional management (7.14%) and continued behaviour management difficulties (12.5%).
The Strategies Questionnaire offered the participants the opportunity to comment on the partial group format. The majority of the feedback was positive (87.1%). The positive feedback contained four key themes. Participants reported desiring more group time, finding the groups supportive, participants appreciated the opportunity to share ideas with other parents and, finally, participants reported that they felt understood and that the experience normalised their own difficulties. The only negative feedback came from a small percentage (6.78%) of parents who were uncomfortable in their group or with working in groups generally.
6. Discussion
6.1. Strategies used
Participants reported attempting the majority of the strategies during the course of the program and for each strategy the majority of the parents who attempted a strategy found it to be helpful.
From clinical experience parents of children with ASD frequently report concern about using the parenting strategy ‘timeout’ with their children. It is thus noteworthy that 75% of parents reported that they had tried timeout during the program and found it to be helpful. In addition, 68.2% of parents reported that they had used timeout in the six months following the program and found it to be helpful. This indicates that the majority of parents of children with ASD can expect to experience success with the strategy timeout if it is applied correctly and for appropriate behaviours.
physical guidance and blocking (Whittingham et al., 2006). However, 81.8% of the parents involved in this study indicated that they had used physical guidance through out the program and found it to be helpful and 84.5% reported that they had used physical guidance and found it to be helpful by follow-up. In addition, 64.3% of parents reported that they had used blocking through out the program and found it to be helpful and 69.2% reported that they had used blocking and found it to be helpful by follow-up. These results show that, for the majority of parents, concerns about the physical contact involved in these strategies are unfounded.
Comic Strip Conversations and Social Stories (Gray, 1998) were added to the Stepping Stones Triple P program as part of Planned Activities Training on the basis of the focus group research (Whittingham et al., 2006). The majority of parents reported attempting Social Stories in the course of the program (65.4%) and over half of the parents were using Social Stories at follow-up six months later (53.8%). Additionally, of the parents who used Social Stories the majority found it to be helpful. Comic Strip Conversations was attempted by 23.3% of parents during the course of the program and this rose to 38.4% of parents at follow-up six months later. Again, the majority of parents who used Comic Strip Conversations found it to be helpful. Thus, there appears to be a significant number of parents of children with ASD who appreciate the opportunity to learn Comic Strip Conversations and Social Stories and find such strategies useful when implemented. Further use of Comic Strip Conversations and Social Stories with the ASD population may address the desire of some parents for ASD specific strategies.
6.2. Parent satisfaction
Overall, the level of participant satisfaction was high and this was demonstrated in the qualitative feedback. Participants felt that the program was sound, they reported noticing an improvement in their child’s behaviour, reported that they were now more skilled and confident as parents and finally, participants wrote notes of thanks and appreciation to their own therapists.
The areas that the parents believed could be improved fell into three areas. Firstly, parents would like to have a program that was specialised for ASD. Some were concerned that it focussed too much upon ‘‘normal tendencies’’ of children and expressed a desire to spend more time in session on comic strip conversations and social stories. One implication of this feedback is that it emphasises the importance of psychoeducation to enable the parents to understand the relevance of behavioural management techniques to the ASD child.
Another area raised by parents was their continued concern about the emotional regulation skills of their child, particularly the role that their child’s anxiety and anger plays in their behaviour. Many of the Stepping Stones Triple P strategies can be used to foster emotional regulation skills in children (e.g., rewards for ‘brave’ behaviour). However, this concern demonstrates that some parents may need particular assistance to understand how the Stepping Stones strategies may be used to improve emotional regulation skills. It also suggests that some parents may benefit from specific information about how to foster emotional regulation skills in their child as part of the parenting program. Further investigation is necessary but Acceptance and Commitment Therapy may provide a promising adjunct to parenting interventions if this is the case. Lastly, some parents made suggestions for changing the format of the program. Mostly, this consisted of requesting longer group sessions and/or longer time in between sessions. It may be that some parents from this population need longer to process the information and make the parenting changes. Of course, in a normal clinical context this adaptation could have been made more easily than was possible in a controlled trial. It is also possible that a better outcome may be achieved by spending more time addressing general parent concerns prior to commencing the parenting program. This could be achieved by training parents in mindfulness based strategies via an Acceptance and Commitment Therapy workshop.
6.3. Group format
difficulties. However, a minority of parents reported a negative experience of the partial group format. This negative experience consisted of either discomfort in group situations or a dislike of the particular group in which they were placed. Participants who reported disliking their group commented that their group found it difficult to ‘‘remain focussed in their discussions’’ and one participant simply commented, ‘‘a strange group’’. Thus, whilst we can conclude that a partial group format is beneficial to many parents of children with ASD, there is a caveat that practitioners ensure that the group remains focussed during the session.
Additionally, it may be the case that the presence of autistic traits in some of the parents also contributed to these less positive experiences. Practitioners working with parents of children with ASD should be aware that some parents may have autistic traits themselves. This may contribute to feelings of discomfort or other difficulties in a group situation.
6.4. Limitations and future directions
The parents within this study were highly satisfied with the partial group format. In addition, many parents used the additional strategies of Comic Strip Conversations and Social Stories and of those that did use these strategies the majority found them to be helpful. However, it remains to be tested whether the partial group format and the additional strategies of Comic Strip Conversations and Social Stories added anything above and beyond the effect of standard Stepping Stones Triple P. Some parents also desired specific information about how to foster emotional regulation skills in their child. Future research could explore this further with an Acceptance and Commitment Therapy adjunct to parent training being one potential way to address this.
6.5. General conclusions
Overall, participants reported a high level of satisfaction with the Stepping Stones Triple P program and for each strategy the majority of parents who attempted it found it to be helpful, including timeout and strategies involving physical contact. In addition, it is suggested that some parents may benefit from learning Comic Strip Conversations and Social Stories. The partial group format was popular, contributing to feelings of support and normalisation as well as the sharing of ideas, however, it should be noted that a minority of the parents did not feel comfortable in groups. In addition, parents of children with ASD may require particular direction about the use of the parenting strategies in fostering emotional regulation skills in their children.
Acknowledgements
The study was supported by a small grant from the School of Psychology, The University of Queensland. We would like to acknowledge the participation of the parents who took part in the study and the clinical interns who helped to conduct the program.
References
Brereton, A., Tonge, B. J., & Einfeld, S. L. (2006). Psychopathology in children and adolescents with Autism compared to young people with intellectual disability.Journal of Autism and Developmental Disorders, 36, 863–870.
Einfeld, S. L., & Tonge, B. J. (1996). Population prevalence of psychopathology in children and adolescents with intellectual disability: II epidemiological findings.Journal of Intellectual Disability Research, 40, 99–109.
Gillberg, C. (2002).A guide to Asperger syndrome. Cambridge: Cambridge University Press.
Gray, C. A. (1998). Social stories and comic strip conversations with students with Asperger syndrome and high-functioning autism. In E. Schopler, G. B. Mesibov, & L. J. Kunce (Eds.),Asperger syndrome or high-functioning autism? Current issues in autism. New York, NY, US: Plenum Press. pp. 167–198.
Howlin, P., & Rutter, M. (1987).Treatment of autistic children. Essex: Anchor Brendon Ltd.
Koegel, R. L., Schreibman, L., Britten, K. R., Burke, J. C., & O’Neill, R. E. (1982). A comparison of parent training to direct child treatment. In R. L. Koegel, A. Rincover, & A. L. Egel (Eds.),Educating the understanding autistic children. California: College Hall Press. pp. 260– 279.
Roberts, C., Mazzucchelli, T., Studman, L., & Sanders, M. R. (2006). Behavioural family intervention for children with developmental disabilities and behavioural problems.Journal of Clinical Child and Adolescent Psychology, 35, 180–193.
Sanders, M. R. (1999). Triple P- positive parenting program: Towards an empirically validated multilevel parenting and family support strategy for the prevention of behaviour and emotional problems in children.Clinical Child and Family Psychology Review, 2, 71–90.
Sanders, M. R., Markie-Dadds, C., Tully, L. A., & Bor, W. (2000). The Triple P positive parenting program: A comparison of enhanced, standard and self-directed behavioural family intervention for parents of children with early onset conduct problems.Journal of Consulting and Clinical Psychology, 68, 624–640.
Sanders, M. R., Mazzucchelli, T. G., & Studman, L. J. (2003).Practitioner’s manual for standard Stepping Stones Triple P. Brisbane: Triple P International Pty Ltd.
Sanders, M. R., Mazzucchelli, T. G., & Studman, L. J. (2004). Stepping Stones Triple P: The theoretical basis and development of an evidence-based positive parenting program for families with a child who has a disability.Journal of Intellectual and Developmental Disability, 29, 265–283.
Sofronoff, K., & Farbotko, M. (2002). The effectiveness of parent management training to increase self-efficacy in parents of children with Asperger Syndrome.Autism, 6, 271–286.
Sofronoff, K., Leslie, T., & Brown, W. (2004). Parent management training and Asperger syndrome.Autism, 8, 301–317. Whittingham, K., Sofronoff, K., & Sheffield, J. K. (2006). Stepping Stones Triple P: A pilot study to evaluate the acceptability of the
program by parents of a child diagnosed with a Autism Spectrum Disorder.Research in Developmental Disabilities, 27, 364–380. Whittingham, K., Sofronoff, K., Sheffield, J., & Sanders, M. R. (in press). Stepping Stones Triple P: An RCT of a parenting program with