1
Capillar y Haemangioma of Nasal Septum
Bestari J Budiman, Ricki Octiza
Otorhinolaryngology Head and Neck surger y depar tment Medical faculty of Andalas Univer sity/ Dr .M.Djamil Hospital
Abstr act
Capillar y haemangioma is a benign, rapidly gr owing lesion of the skin and mucous membr anes. It may r ar ely pr esent as a mass of considerable size and thus entirely fill the nasal cavity. Its etiology remains obscur e. Capillar y haemangioma usually involves the gingiva, lips, tongue, and buccal mucosa. However, the nasal cavity is a r are location for this lesion. The most common symptoms are unilateral epistaxis and nasal obstr uction. The tr eatment of choice is surger y to r emove the tumour even for lar ge lesion. A case of capillar y haemangioma at anter ior nasal septal in 6 year s old gir l had been treated with extir pation.
Keys w ord : Capillar y haemangioma, nasal septum, epistaxis, diagnosis, tr eatment
Abstrak
Haemangioma kapiler mer upakan suat u lesi jinak pada kulit dan mukosa dengan per t umbuhan yang cepat. Meskipun jar ang ber ukur an besar , namun dapat memenuhi selur uh kavum nasi. Et iologinya sampai sekar ang masih belum jelas. Haemangioma kapiler ser ing t er dapat pada ginggiva, bibir , lidah dan mukosa bukal. Kavum nasi mer upakan lokasi yang jar ang t er dapat nya haemangioma kapiler . Gejala yang paling ser ing adalah unilat er al epist aksis dan sumbat an hidung. Pembedahan unt uk mengangkat t umor ini mer upakan t er api pilihan meskipun ber ukur an besar . Suat u kasus haemangioma kapiler sept um ant er ior pada anak per empuan ber umur 6 t ahun t elah dilakukan ekst ir pasi sebagai t er api.
Kat a kunci : haemangioma kapiler , sept um nasi, epist aksis, diagnosis, penat alaksanaan
Korespondensi: Ricki Octiza: r [email protected]
Introduction
Haemangioma is a benign neoplasm of vascular phenotype.1 Usually, congenital lesions are located on the
skin or oral mucosa while the nasal cavity and paranasal sinuses are uncommon sites for haemangiomas. Nasal cavity haemangioma is extraor dinar ily rar e in children.2
Mucosal haemangiomas of the nasal cavity, paranasal sinuses and nasophar ynx account for 10% of all head and neck haemangiomas and appr oximately 25% of all non-epithelial neoplasms of this anatomical region. The haemangiomas occur in all ages, although there is a peak in childr en and adolescent males, females in the r epr oductive year s, and then an equal distr ibution beyond 40 year s of age. Patients w ith caver nous haemangiomas tend to be men in the 5th decade.1,2
Haemangioma of nasal cavity also know n as lobular capillary haemangioma, pyogenic granuloma, capillar y haemangioma, caver nous haemangioma, epulis gravidar um. This various name of this tumor show that the exact pathogenesis is still continued debated.Some theories say that capillar y haemangioma has an association with injur y and hormonal factor s.1,2,3,4
In the nasal cavity, anterior septum is the most frequently affected followed by tur binate but have also been described arising from the maxillar y sinus, r oof of the nasal cavity, and floor of the nasal vestibule. This disease usually pr esented as unilateral epistaxis and nasal obstr uction.1,3
Histologically, these masses ar e character ized by var ying sized capillaries in lobular arr angements and anastomosing netw orks of capillaries, thus suppor ting
the name lobular capillar y haemangioma. Sur r ounding these lobules is a loose spindle cell pr oliferation of pericytic cells. Surgical excision is the treatment of lobular capillar y haemangiomas. Intraoperative fr ozen sections may be necessar y to confirm the diagnosis.3
Case r epor t
A six year s old gir l came into emergency room’s
Dr .M.Djamil hospital Padang on November 14th 2010 (MR
716907), with chief complain bleeding fr om left nostr il since 2 hour s before admission. The blood came when the patient w as sleeping w ith amount appr oximately 5 teaspoon. No sign of tr auma. History of nasal bleeding one week ago, appr oximately a half of glasses, spontaneously stop by it self. Since 1 week ago patient complaint about a mass w as gr ow n in her left nostr il and obstruction her nose. Then her parents took her to otor hinolaringologyst and recommended for operation. No histor y of tr auma to the nose. Left nostr il w as obstruction. No history of smelly discharge fr om the nose. No histor y of aller gy.
General examination, condition w as good,
composmentis, temperatur e 37,30C, pulse rate
2
bleeding and no ulceration. Inferior and medial turbinate cannot be evaluated.
Labor ator y finding, Hb: 11,1 gr / dl, leukocyte: 9500/ mm3, hematocrit: 30%, tr ombocyte: 407.000/ mm3,
PT: 10.9 second, APTT: 39.5 second.
Patient was diagnosed w ith post epistaxis caused by suspected haemangioma septum, differential diagnosed with granuloma septum. Patient w as treated w ith amoxicillin clavulanate 3x250 mg, tranexamic acid injection 3x250 mg, vitamin K 3x5 mg and vitamin C injection 3x30 mg. Patient was planned for extir pation under general anesthesia.
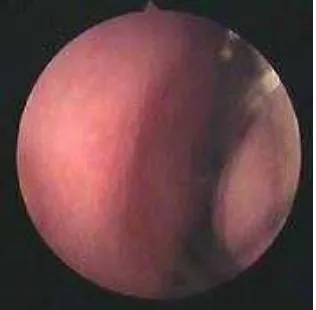
Figur e 1. Haemangioma ar ising from left anter ior septum
Tw o days after the patient was consulted to oncology subdepar tment, with diagnosed suspected haemangioma septum, differential diagnosed with nasal septal granuloma. Transamin, vitamin K and vitamin C injection were stopped and antibiotic ther apy w as continued. Paranasal sinus CT Scan w as planned. Patient w as planned to go on extir pation under gener al anesthesia.
On November 19th 2010, CT Scan (C.2353) w as
perfor med w ith result “there w as a mass in left nasal cavity w hich is push nasal septal to the right, isodense in density, clear edge, regular , no sign of car tilage destr uction. Par anasal sinuses w as clear, no mass at nasopharynx, no enlar gement of lymph node. Conclusion : left nasal cavity tumor ”.
Figur e 2. CT Scan axial and coronal showing mass at left nasal cavity
On November 22th, 2010 extir pation w as
perfomed under gener al anesthesia. Operating repor t :
- Patient lying dow n on operating table under gener al
anesthesia
- Septic/ antiseptic pr ocedur e
- Applied or al packing
- Applied adr enaline : lidocaine tamponade 1:4 in the both nasal cavity.
- Evaluation, there was a reddish mass at anterior
septum, easy to bleed, smooth surface. The later al w all is free fr om lession.
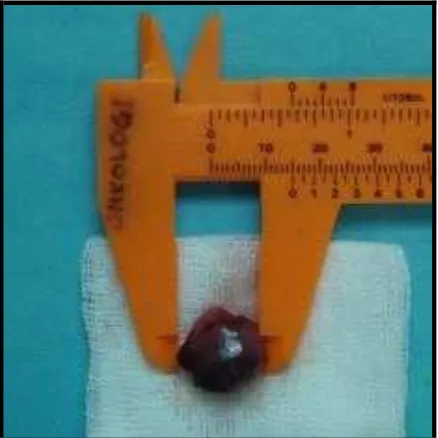
- Mass w as dissected fr om septum w ith respator ium, it
sized was 1x1x0.5 cm. Bleeding was coming fr om lession bed and treated w ith applied tamponade. - Rest of mass at lession bed was cleaned and cutted
w ith curr etage and cutting for sep.
- AgNO3 w as applied on lession bed to stop bleeding.
- Evaluation : no sign of car tilage destruction. - Then nasal packing was set up in left nasal cavity.
- Oral packing was released and operation had been
finished.
3
After oper ation the patient w as given cefixime 2x50 mg and ibupr ofen 3x200 mg or ally.
Thr ee days later the nasal packing w as removed and no active bleeding at left nasal cavity, clotting at extir pation site, infer ior and medial tur binate eutr ophy, no sinechia, no septal perforation. Wor king diagnosis w as post extir pation suspected haemangioma nasal septum and patient w as dischar ge with therapy cefixime 2x50 post extir pation suspected haemangioma nasal septum and give therapy cefixime 2x50 mg.
On December 14th 2010, histopatological
Figur e 4. Histological appear ance shows er itrocyte in little cavity layer ed by endotel
After 4 months, there w as no sign of r ecur rence muscles and glands. It gr ow th rapidly, r egress slow ly and never recur . In the biologic classification pr oposed by Mulliken & Glowacki in 1982, haemangiomas are defined as vascular tumour s that enlar ged by r apid cellular pr oliferation. They ar e classified as capillar y, cavernous, and mixed lesions. Ther e are 3 stages in the life cycle of a haemangioma : (1) the pr oliferating phase (0-1 year of age), (2) the involuting phase (1-5 year s of age) and (3) the involuted phase (> 5 year s of age). Usually, congenital lesions are located on the skin or or al mucosa w hile the nasal cavity and paranasal sinuses are uncommon sites for haemangiomas. Nasal cavity haemangioma is extraor dinar ily rar e in children. Only nine cases have been r epor ted in the English literature between 1985 and 2005.2,3,4,6,8
Haemangiomas account for about 20% of all benign neoplasms of the nasal cavity. Haemangioma of the nasal cavity occur s most commonly on the septum (65%), later al w all (18%), and vestibule (16%).4,5,7,9
No mechanism for the development of capillar y haemangioma has so far been defined. How ever , trauma,
hormonal influences, viral oncogenes, under lying
micr oscopic arteriovenous malfor mations, and the pr oduction of angiogenic gr owth factor s have been suspected to act in the pathogenesis. Puxeddu et al found that predispossing factor s such as nasal trauma w ere identified in 15% fr om 40 patients and pregnancy were identified in 2 patients (5%). Meanw hile Nair also hypothesized that micr otrauma or chr onic iritation in nasal cavity as aetiology of haemangiomas, but in this patient, none of these potential etiological factor s w as determined.7,8,10
Epistaxis in childhood are generally repeated, shor t-lasting and self-limiting. However, they are a cause of significant distr ess to childr en and their par ents and r esult in significant mor bidity and hospital refer ral. Several etiology have been found that cause epistaxis in childhood such as tr auma, inflamation, haematological, neoplastic and vascular abnormalities.11
This patient have symptom recurr ent unilater al epistaxis and left nasal obstruction. Puxeddu et al founded that in 40 haemangiomas patients, the pr esenting symptoms, w hich had been present for a period var ying fr om 1 w eek to 5 year s, w ere unilater al epistaxis (95%), nasal obstr uction (35%), rhinor rhea (10%), facial pain (7.5%), headache (4%), and hyposmia (4%) alone or in different associations.7,8,9
4
Haemangiomas should be distinguished fr om
granulation tissue, telangiectasia, vascular
malfor mations, vascular polyps, papillar y endothelial hyper plasia, angiofibr oma, angiolymphoid hyper plasia w ith eosinophilia, glomus tumour , lymphangioma, Kaposi sarcoma, and angiosarcoma. Haemangioma can be distinguished fr om granulation tissue by the lobular arr angement of the capillaries in the former and the more parallel arr angement of vessels in the latter . The distinction between a haemangioma and telangiectasia may be difficult but is facilitated in a patient with a know n family histor y of hereditar y haemorr hagic telangiectasia (Osler -Weber-Rendu syndr ome).1,4,7,8,10,12
Ahmad and Nor ie pr ove that nasal cavity vascular ’s tumour can be mistaken w ith juvenile nasopharyngeal angiofibr oma but after angiography they didn’t find any significant feeding vessel supplying the tumour. Meanw hile Puxeddu also state that differential diagnosis may pose challenging pr oblems in lar ge lessions w here it can be misdiagnosed as angiofibr oma and low grade angiosarcoma. Because of that infor mation obtained with imaging techniques, along with the age and gender of the patient, help to make a correct diagnosis of angiofibr oma and differ entiation of haemangioma fr om other hypervascular ized lesions.1,4,8,10,13
Based on histopathology this tumor can be divided into capillary and caver nous types based on the size of the blood vessels. Haemangiomatosis is a more diffuse lesion often involving contiguous structures. Caver nous haemangiomas ar e fr equently intr aosseous or involve the tur binates or lateral nasal w all. They are composed of multiple, large thin-walled, dilated blood vessels separ ated by scant fibr ous str oma.1,2,4,8
The management of haemangiomas continues to be an ar ea of consider able contr over sy. The tr eatment of
congenital vascular anomalies is based on an
under standing of the clinical behaviour and natur al histor y of individual lesions, the localization and size of the neoplasm. Some treatment had been intr oduced such as injection of scler osing solution, intr alesional injection of ster oid, interfer on application, laser therapy, cr yosur ger y, cytostatic, embolization and surgical treatment.4,8,14,15,16
Haemangiomas are gener ally easy to remove, although lar ger tumour s may be complicated by excessive bleeding. They should be r emoved in all ages, especially in childr en since aplasia of the nasal car tilages may cause eventual disfigurement. If the tumour is pr egnancy- related, regression w ill often occur after parturition. Multiple r ecur rences are more common in children if the lesional bed is not completely eradicated.4,8,10
Total excision of the lesion by either classical or endoscopic sur ger y techniques has been recommended. The endoscopic surger y pr ovides better visualization of the mass and sur r ounding anatomy, thus allow ing the sur geon to r emove the mass completely without an exter nal incision. In the ver y recent literature, all patients w ith a lar ge lesion have been managed without pr eoper ative embolization and none has experienced blood loss r equiring tr ansfusion.12,13,15
The application of endonasal endoscopic sur ger y is constantly evolving. One of the advantages of this technique is that it does not involving any facial skin incision and is better tolerated by the patient. This sur gical appr oach involves a shorter hospitalization. This
technique w as once considered to have limitation on the vascular tumor because endoscopic removal of such tumor could be difficult due to uncontr olled bleeding
w hich could hamper visualization and mar gin
assessment. Kelley TF state that w ith car eful pr eoper ative planning and conser vative surgical technique, these highly vascular tumor s can be safely and effectively r emoved w ith an endoscopic appr oach.7,8,12,13,15
The application of AgNO3 to stop bleeding w as
succesfull w hile oper ation. Many treatment can apply to treat bleeding such as cauter ization, using of laser or embolization. But in r ecent year s many clinicians found that this tumour can be managed without pr eoper ative embolization and none has experienced blood loss r equiring tr anfusion.7,15,16
After 4 months follow up ther e is no r ecurrent
of haemangioma. Some studies and cases of
haemangioma reported that recurrences are uncommon if there is no residual at lesion bed.4,6,7,8,15
Liter atur es
1. J.C.Fanbur g-Smith, L.D.R. Thompson. Benign soft
tissue tumour s. In: Bar nes L, Eveson JW, eds. Wor ld Health Organization Classification of tumour s, pathology and genetics head and neck tumour s. Lyon, 2005
2. Valencia MP, Castillo M. Congenital and acquired
lesions of the nasal septum: A pr actical guided for differential diagnosis. Radiogr aphics 2008;28:205-33
3. Duvvuri U, Carrau RL, Kassam AB. Vascular tumour s
of the head and neck. In: Byr on BJ, Jonas JT, Shaw n ND, eds. Head and neck surger y-otolar yngology, 4th edition. Pittsbur gh. Lippincott Williams & Wilkins, 2006; p: 1812-25
4. Nedev P. Lobular capillar y haemangioma of the
nasal cavity in children - Literature sur vey and case r epor t. Tr akia Jour nal of Sciences 2008;6(1): 63-7.
5. Zarr inneshan A, Zapanta P, Wall SJ. Nasal pyogenic
granuloma. Otolar yngology–Head and Neck Surger y 2007; 136: 130-1
6. Mar ler JJ, Mulliken JB. Current management of
hemangiomas and vascular malformations. Clin plastic surg 2005;32:99-116
7. Takeda K, Takenaka Y, Hashimoto M. Intraosseous
haemangioma of the infer ior turbinate. Case repor t in medicine, 2010.
8. Puxeddu P, Ber lucci M, et al. Lobular capillar y haemangioma of the nasal cavity: A retr ospective study on 40 patients. Am J Rhinol 2006; 20: 480–4 9. Genc S, Kur kcuoglu S et al. Giant lobular capillar y Pediatr ics ENT. Springer 2007; p. 285-9
12. Archontaki M, Stamou, et al. Cavernous
haemangioma of the left nasal cavity. Acta otor hinolar yngologica italica 2008;28:309-11
13. Ahmad R, Nor ie A. Endonasal endoscopic resection
of intranasal haemangioma. Med J Malaysia 2006;
5
14. Ber lien HP. Principles of Therapy of Infantile
Hemangiomas and Other Congenital Vascular Tumor s of the Newbor ns and Infants. In: Matassi R, Loose DA, Vaghi M, eds. Hemangiomas and vascular malfor mations-an atlas of diagnosis and treatment. Springer ver lag Italia, 2009. p: 49-84
15. Kelley TF. Endoscopic management of an intranasal
haemangioma: A case repor t and literatur e review . Otolar yngol Head Neck Sur g 2003;128:595-7.
16. Andronikou, S, Mandelstam S, Fasulakis, S. MRI and