PRETES 3
dr. Syah Rini Wisdayanti Sp.OG , M.KesKehamilan multifetal meningkat sebanyak 3% pada populasi dunia. Persalinan preterm merupakan masalah utama dari kehamilan multifetal, global survey dari WHO menyatakan 35.2
% kehamilan multifetal berakhir dengan persalinan preterm (Fallis, 2013; Wei, 2016)
PENDAHULUAN
Kehamilan multifetal merupakan hasil dari 2 atau lebih kejadian fertilisasi, fertilisasi tunggal diikuti pembelahan ”erroneous´ dari zigot, atau kombinasi dari keduanya (Cunningham, 2018)
FAKTOR RISIKO
• 3,5% pada wanita kulit hitam, 3 % pada wanita kulit putih. Wanita Hispanik, Asia dan Amerika kemungkinanya lebih rendah daripada wanita kulit putih.
Ras
• Kejadian kembar dizigot meningkat pada usia 15-37 tahun
Usia saat kehamilan
• Kemungkinan meningkat 8x lipat saat paritas ≤4 dan 20x lipat saat paritas ≥5 (Olusanya,2012)
Jumlah paritas
• Riwayat kembar dari ibu lebih berpengaruh daripada riwayat kembar dari ayah
Hereditas
• Beberapa penelitian menunjukkan wanita yang mendapat asam folat memiliki prevalensi yang lebih tinggi. Pada World War II di eropa saat pemenuhan nutrisi bagi wanita hamil lebih sulit tercatat penurunan angka kehamilan kembar
Nutrisi
• Peningkatan kelahiran kembar berkaitan dengan pelepasan FSH hipofisis yang berlebihan sebagai respons terhadap penurunan umpan balik negatif dari kegagalan impending ovarium
Gonadotropin Pituari
• Induksi ovulasi dengan FSH plus human chorionic gonadotropin (hCG) atau klomifen sitrat meningkatkan kemungkinan ovulasi bersamaan.
Terapi Infertilitas
DIZIGOTIK VS MONOZIGOTIK Dizigotik
Lebih sering
Dipengaruhi kadar FSH (geografi, ras,
multipara, usia, kontrasepsi)
Selalu dikorionik
Monozigotik
Jarang (3.5- 4/1000 kelahiran)
Paling dipengaruhi genetik
Korionisitas tergantung kapan
membelah
(Cunningham et al, 2018) (Basiri et al, 2019)
KLASIFIKASI
DIAMNION
DICHORION
7
DIAGNOSIS MULTIFETAL
Evaluasi Klinis Sonograf
• Pengukuran TFU. Memantau pertumbuhan janin & volume cairan amnion. Pada uk 20-30 minggu dapat > 5 cm daripada kehamilan tunggal
• Palpasi. Menentukan bagian janin pada trimester ketiga, penyulit : posisi janin saling tumpang tindih, ibu dengan obesitas dan hidramnion.
• Pemeriksaan DJJ, dengan alat Doppler dapat dibedakan jika letak jantung janin cukup berjauhan
• Tidak disarankan diagnosa multifetal hanya menggunakan 1 kriteria
Gambar 2 A. Sonografi “puncakkembar”/”tandal lambda”
B. Sonografi dengan “tanda T”
Pemeriksaan sonografi pada trimester pertama, sering terjadi deteksi dini kehamilan kembar Sonografi juga dapat digunakan untuk menentukan jumlah janin, perkiraan usia kehamilan, korionisitas, dan amnionisitas. Dengan pemeriksaan yang cermat, jika ada kantung kehamilan yang terpisah, dapat diidentifikasi pada awal kehamilan kembar.
Alat Bantu Diagnostik lainnya:
• Radiografi abdominal sulit saat janin bergerak dan uk <18minggu
• Magnetic Resonannce Imaging patologi kembar yang lebih detail
• Kadar β-hCG dan maternal serum levels of alpha-fetoprotein (MSAFP) meningkat
A B
• Evaluasi USG perkiraan usia kehamilan, menentukan korionisitas dan screening Down’s syndrome
Menentukan usia kehamilan dan korionisitas
• Lebih beresiko anemia rutin evaluasi as folat/zat besi
Diet and Nutrisi
Perawatan spesialistik
• Skrining down syndrome saat CRL : 45 mm - 84 mm (pada usia kehamilan : 11 – 13+6 minggu)
• Screening kombinasi : nuchal translucency, β hCG , pregnancy associated plasma protein A)
• Monitoring untuk IUGR
Komplikasi Janin
SKRINING
Usia kehamilan 16-17, 19-20, dan 21-22 minggu
untuk skrining TTTS dan TAPS serta skrining jantung sebagai bagian dari skrining anatomi lengkap pada minggu ke 18-19 minggu atau pada minggu ke 21-22.
USG pada usia kehamilan 11+0 minggu hingga 13+6 minggu (CRL 45-84 mm)
berfungsi untuk menilai viabilitas janin, usia kehamilan dan korionisitas, serta melihat adanya
malformasi kongenital mayor
Jika tidak terdapat kelainan dilanjutkan pemeriksaan pertumbuhan pada minggu ke
24, 28, 32 dan 34
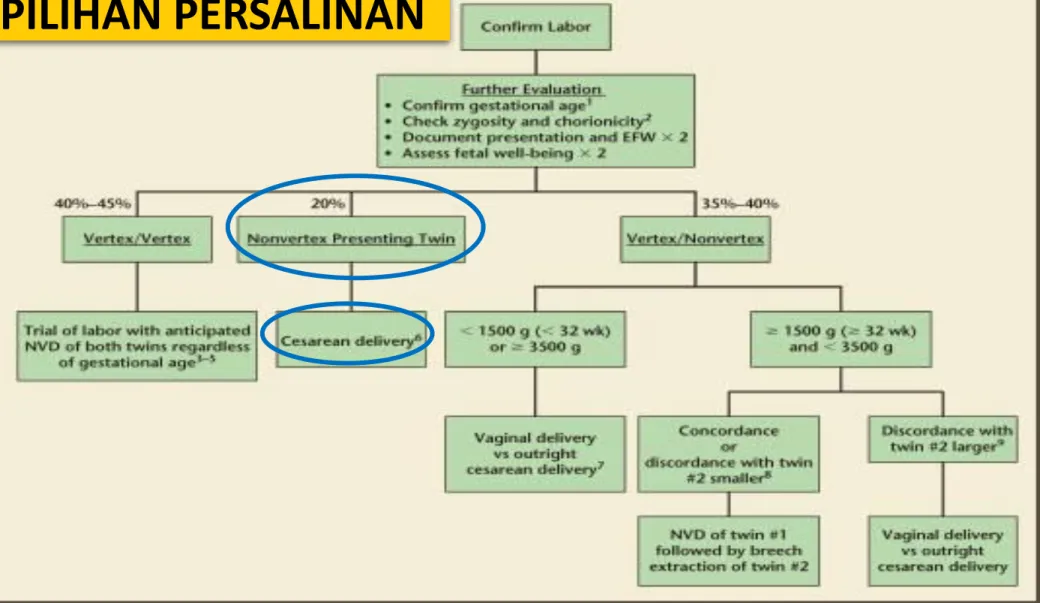
PILIHAN PERSALINAN
Direncanakan sejak UK 24 - 28 minggu (tempat, waktu, metode, dan resiko persalinan)
- Tanpa komplikasi uncomplicated triplet pregnancies elektif UK 35 minggu (setelah + kortikosteroid)
Persiapan standar untuk pelaksanaan persalinan + pertimbangan khusus untuk wanita dengan kehamilan multifetal
Posisi dan presentasi janin paling baik dikonfirmasi secara sonografi
Gambar 3. Macam-macam presentasi janin pada kehamilan kembar Sumber: https://obgynkey.com/multiple-pregnancy-and-other-antenatal-complications/
2016 Royal College of Obstetricians and Gynaecologists
Christopher D, Robinson BK, Peaceman AM. An evidence-based approach to determining route of delivery for twin gestations.
Rev Obstet Gynecol. 2011;4(3-4):109-116.
Gambar 4. Alur pemilihan persalinan pada kehamilan kembar (Christoper, 2011)
PILIHAN PERSALINAN
MATERNAL
Persalinan preterm (35.2%)
( Jun Wei, 2016)
Hipertensi dalam kehamilan 2.5 -2.8 kali
(Devine and Malone, 2004)
Diabetes dalam kehamilan
2.2 kali (Rauh-Hain et al.,
2009).
AFLP
7.1% hingga 28.6%
(Minakami et al., 2014).
Anemia
(multifetal triplet, 70%) (Devine and Malone,
2004).
Cholelitiasis 0.4% - 5.5%
(Rissanen et al., 2019)
KOMPLIKASI
(ACOG, 2016)
KOMPLIKASI
Preterm Delivery
Deteksi
• Pada pasien asimptomatik tidak dianjurkan melakukan tindakan intervensi yang bertujuan untuk skrining risiko preterm
• Pada pasien simtomatik dapat dilakukan pengukuran panjang serviks dan skrining fetal fibronectin sebagai bantuan untuk prediksi risiko kelahiran preterm. Panjang serviks 25mm adalah cut-off paling sering digunakan pada trimester kedua
Pencegahan • Belum ada Tindakan intervensi yang direkomendasikan untuk memprolong masa kehamilan
Manajemen
• Tokolitik dapat diberikan untuk memperpanjang masa kehamilan jangka pendek
• Pemberian kortikosteroid antenatal untuk wanita hamil usia 24-34 minggu mengurangi insiden kematian neonatal karena distres pernapasan
• Pemberian magnesium sulfat prenatal dapat dilakukan untuk mengurangi terjadinya cerebral palsy
FETAL
Gambar 2. Overview insidensi komplikasi kehamilan ganda (Cunningham, 2014)
KOMPLIKASI
Dichorion Diamnion Monochorion Diamnion
Monochorion Monoamnion
TTTS Rare 15% 2-6%
TAPS - Up to 5 % -
TRAP - 1% 1%
sIUGR 11.6% 12% -
Tabel 1. Insidensi komplikasi fetal pada kehamilan Multifetal (Rauh-Hain et al., 2009; Anca et al., 2015; Buyukkaya, Tekbas and Buyukkaya, 2015; Johnson, 2015; K.Behavkova, 2016; Lanna et al., 2019; Antonakopoulos et al., 2020; Gleeson et al., 2020)
KOMPLIKASI
Twin to Twin Trnasfussion syndrome
Mempengaruhi 15% dari kehamilan multifetal monochorionic.
FETAL
Treament of choice adalah ablasi laser
pada quintero stage II (Rekomendasi: A)
Konservatif management dilakukan pada quintero stage I (Rekomendasi B) Amnioreduction bertahan sebelum usia
kehamilan 26 minggu (Rekomedasi A) (Khalil et al., 2016)
MANAGEMENT
KOMPLIKASI
Twin Anemia – Polycyteamia Sequence (TAPS)
Mempengaruhi 2% dari kehamilan multifetal dan 13% setelah mendapatkan terapi ablasi laser
FETAL
Pilihan terapi pada TAPS bergantung kasus per kasus. Terapi paling umum adalah konservatif, early delivery, ablasi laser, transfusi intrauterine, partial exchange transfusion (Evidence Level 3) (Khalil et al., 2016).
MANAGEMENT
KOMPLIKASI
Twin Reversed Arterial PerfusionSequence (TRAPS) FETAL
Terapi utama dari TRAPS adalah discontinuation transfusion dari janin acardiac, dengan cara ligasi tali pusat dari janin acardiac (Evidence Level 3).
(Khalil et al., 2016)
Twin Reverse Arterial Perfussion (TRAP) terjadi pada 1% kehamilan multifetal dengan janin kedua acardiac.
MANAGEMENT
KOMPLIKASI
Selective Intra Uterine Growth Restriction FETAL
Terminasi merupakan pilihan utama dimana bila termasuk dalam tipe I direkomendasikan pada usia kehamilan 34-36 minggu, sedangkan pada tipe II dan III disarankan dilakukan terminasi pada usia kehamilan 32 minggu
MANAGEMENT
• sFGR, secara konvensional, didefinisikan sebagai suatu kondisi di mana satu janin memiliki EFW <10 percentile dan diskrepansi EFW dengan kembarannya > 25%
• Terjadi pada 10-15% kehamilan multifetal
• Tipe I, waveform doppler arteri umbilikalis terdapat positive end-diastolic flow
• Tipe II, terdapat absent or reversed end-diastolic flow (AREDF).
• Tipe III, terdapat pola AREDF yang memebntuk siklus/intermittent
1. All except which of the following complications are increased in multifetal gestations?
a. Preeclampsia b. Hysterectomy c. Maternal death d. Postterm delivery
2. Which of the following mechanisms may result in monozygotic twins being discordant for malformations or traits?
a. Prezygotic mutation
b. Variable expression of the same genetic disease c. Skewed lyonization in male fetuses with differential expression of X-linked traits or diseases
d. All of the above
3. A 37-year-old G1 comes to establish prenatal care with you after being
discharged from her reproductive endocrinologist. This pregnancy was conceived via single embryo transfer in vitro fertilization. Which one of the following is true regarding her situation?
a. Assisted reproductive technology increases the incidence of monozygotic twins two- to fivefold.
b. If a single zygote splits 8 days post fertilization, a monochorionic diamnionic twin gestation results.
c. Because this pregnancy is known to have begun with one embryo, you can be certain that she will have monochorionic twins, but amnionicity depends on timing of split.
d. All of the above
4. A 29-year-old G1P1 conceived dichorionic twins via gonadotropin stimulation and intrauterine insemination (IUI) with her husband’s semen.
Her blood type is O-negative, so prior to receiving
anti-D immune globulin the neonates’ blood type is assessed. One neonate is A-positive and the other is O-negative. Her husband is A-positive. This finding can be explained to the parents by describing which
of the following phenomena?
a. Superfetation
b. Superfecundation
c. This is not atypical for dichorionic twins
d. This cannot be explained without alleging infidelity or poor technique by her reproductive endocrinologist’s office.
5. Which of the following factors increases the risk for monozygotic twinning?
a. Maternal age b. Increased parity
c. Race and family history d. None of the above
6. Which hormone is the most likely underlying cause of increased twinning seen in some racial and ethnic groups?
a. Estrogen
b. Progesterone
c. Luteinizing hormone
d. Follicle-stimulating hormone
7. Which of the following statements regarding atypical twinning is not true?
a. Monochorionic twins are never dizygotic.
b. Twins of opposite sex are not always dizygotic.
c. Monochorionic twins are not always the same sex.
d. None of the above is true
Pendahuluan
Intrauterine Growth Restriction (IUGR)
Kegagalan janin untuk mencapai perkembangan yang sesuai potensinya
Saat ini, diagnosis berdasarkan EFW (Estimated Fetal Weight) di bawah persentil
10
Sensitivitas kurang
(gagal terdiagnosis bila ada hambatan perkembangan, namun EFW janin tidak
kurang dari persentil 10) Luaran perinatal buruk
Penegakan diagnosis merupakan hal yang penting
Mencegah Intrauterine Fetal Death (IUFD), cedera otak perinatal dan fetal distress
intrapartum yang berat
Managemen untuk monitoring dan rekomendasi usia saat persalinan
Fase Pertumbuhan
Hiperplasia
• 0-16 minggu
• Mitosis cepat
• Jumlah DNA
Hiperplasia &
Hipertrofi
• 17-32 minggu
• Mitosis
• Ukuran sel
Hipertrofi
• >32 minggu
• Ukuran sel , deposisi lemak, massa otot dan jaringan ikat
15 minggu 5 gram/hari
24 minggu 10-20 gram/hari
34 minggu 30- 35 gram/hari
Fase Pertumbuhan
Peningkatan berat janin (gram/hari) berdasarkan
usia kehamilan
garis hitam: rata-rata garis biru: ± standar deviasi
Faktor Risiko dan Etiologi
Faktor Risiko yang
mempengaruhi pertumbuhan janin terhambat meliputi potensi abnormalitas pada
ibu, janin, dan plasenta
Identifikasi
perkembangan janin
↓
Sonography
Paling umum dilakukan
Femur Length
Biparietal diameter
Head circumference
Abdominal circumference
Estimated Fetal
Weight (EFW)
IUGR vs SGA
Janin Kecil
IUGR
Intrauterine Growth Restriction
SGA
Small for Gestational Age Janin yang kecil, dengan risiko luaran
perinatal lebih buruk dibandingkan janin yang tumbuh normal Terdapat redistribusi hemodinamik
sebagai respon adaptasi janin terhadap kondisi undernutrition,
hipoksia atau gangguan (insufiseiensi) plasenta
Janin yang kecil, dengan luaran perinatal yang sama baik seperti
janin yang tumbuh normal Tidak terdapat tanda-tanda respon adaptasi janin terhadap perubahan
pada lingkungannya
juga mempunyai risiko kelainan perinatal dan neurodevelopmental
8. In which chromosomal aneuploidy is fetal-growth restriction virtually always present?
a. 45,X
b. Trisomy 13 c. Trisomy 18 d. Trisomy 21
9. Which of the following drugs and chemicals is capable of limiting fetal growth?
a. Alcohol b. Cocaine c. Cigarettes
d. All of the above
10. Which of the following practices may prevent or limit fetal growth restriction?
a. Smoking cessation
b. Increase caloric requirements for women with a growth restricted infant.
c. Even with normal fundal height and presumed growth, it is reasonable to
perform Doppler velocimetry and fetal surveillance on the current pregnancy if the woman had an infant with growth restriction previously.
d. All of the above
11. Ms. Smith is a 37-year-old multigravida who presents to your office at 32 weeks’ gestation as calculated by her last menstrual period. Her hematocrit is 29%, and she has sickle-cell trait. During sonographic evaluation, the fetus has biometric values that correlate with a 28-week fetus. What is the most likely explanation?
a. Aneuploidy
b. Chronic hypoxia
c. Poor pregnancy dating
d. First-trimester cytomegalovirus infection
12. For the patient in number 11, when will you reevaluate fetal growth?
a. 1 week b. 2 weeks c. 3 weeks d. 6 weeks
13. What is the major risk factor for fetal overgrowth?
a. Genetics b. Multiparity
c. Maternal obesity
d. Gestational diabetes
14. For the prediction of macrosomia, how does clinical estimation of fetal weight compare with sonographic estimation?
a. Less accurate b. Similar accuracy
c. Modestly more accurate d. Significantly more accurate
5. Routine membrane sweeping on cervical exam at 38–40 weeks’ gestation has been shown to be
associated with which of the following?
a. Increased pain
b. Increased bleeding
c. Lower rate of postterm pregnancies d. All of the above
16. In primigravidas undergoing induction of labor at 41 weeks’ gestation,
what beginning fetal station was associated with the highest rate of caesarean section?
a. 0 b. –1 c. –2 d. –4
17. Which of the following is predictive of a successful induction of labor?
a. Cervical length <3 cm b. Cervical length <2.5 cm
c. Cervical dilation prior to induction d. All of the above
18. Comparing induction of labor at 41 weeks’ gestation to prolonging pregnancies with fetal testing, research supports which of the following statements?
a. Induction increases the rate of cesarean delivery.
b. Induction increases the rate of postpartum hemorrhage.
c. Induction increases the rate of anesthesia complications.
d. Induction decreases the rate of meconium aspiration syndrome.
19. What are considerations when considering amniotomy during a postterm induction?
a. Increase risk for cord compression
b. Allows more precise fetal heart rate monitoring
c. Aids in identification of thick meconium in amnionic fluid d. All of the above
20. When used during labor, amnioinfusion does which of the following?
a. Prevents placental abruption
b. Decreases the occurrence of variable decelerations
c. Decreases the incidence of meconium aspiration syndrome d. None of the above
21. With thick meconium early in the labor process, which of the following is true?
a. Cesarean delivery is likely
b. Chances for vaginal delivery are diminished
c. If delivery is remote, some obstetricians elect to perform cesarean delivery d. All of the above
22. The American College of Obstetricians and Gynecologists recommends which of the following in the setting of meconium-stained amnionic fluid?
a. Intubation if the baby is depressed b. Amnioinfusion only during active labor
c. The pediatrician should immediately perform bulb suction on the warmer.
d. The obstetrician should perform bulb suction after delivery of the baby.
23. A 44-year-old primigravida presents to clinic at 40 weeks’ gestation. She wants to go into labor naturally, and therefore wants to wait as long as possible to be induced.
Based on the American College of Obstetricians and Gynecologists, when should she be induced?
a. 40 weeks’ gestation b. 41 weeks’ gestation c. 42 weeks’ gestation
d. When the patient is ready
24. The patient in Question 23 inquires about the risks of going past 41 weeks’
gestation. What are the risks she is concerned about?
a. Macrosomia
b. Cesarean delivery
c. Postmaturity syndrome d. Anesthesia complications
25. The patient in Question 23 agrees to induction of labor at 41 weeks’ gestation. How will you manage her pregnancy during this week?
a. Fetal surveillance b. Anesthesia consult
c. Weekly prenatal care visit only, as usual
d. Cancel her clinic visit and see her on the day of her induction