PRE TES 2
Pendahuluan
Intrauterine Growth Restriction (IUGR)
Kegagalan janin untuk mencapai perkembangan yang sesuai
potensinya
Saat ini, diagnosis berdasarkan EFW (Estimated Fetal Weight) di bawah
persentil 10
Sensitivitas kurang
(gagal terdiagnosis bila ada hambatan perkembangan, namun
EFW janin tidak kurang dari persentil 10)
Luaran perinatal buruk
Penegakan diagnosis merupakan hal yang penting
Mencegah Intrauterine Fetal Death (IUFD), cedera otak perinatal dan fetal distress intrapartum yang berat
Managemen untuk monitoring dan rekomendasi usia saat
persalinan
Fase Pertumbuhan
Hiperplasia
•
0-16 minggu
•
Mitosis cepat
•
Jumlah DNA
Hiperplasia
& Hipertrofi
•
17-32 minggu
•
Mitosis
•
Ukuran sel
Hipertrofi
•
>32 minggu
•
Ukuran sel
,
deposisi lemak,
massa otot dan
jaringan ikat
15 minggu
5 gram/hari
24 minggu
10-20
gram/hari
34 minggu
30- 35
gram/hari
Fase Pertumbuhan
Peningkatan berat
janin (gram/hari)
berdasarkan usia
kehamilan
garis hitam: rata-rata garis biru: ± standar deviasi
Faktor Risiko dan
Etiologi
Faktor Risiko yang
mempengaruhi
pertumbuhan janin
terhambat meliputi
potensi abnormalitas
pada ibu, janin, dan
plasenta
Identifikasi
perkembangan
janin
↓
Sonography
Paling umum dilakukan
Femur Length
Biparietal diameter
Head circumference
Abdominal
circumference
Estimated
Fetal Weight
(EFW)
IUGR vs SGA
Janin Kecil
IUGR
Intrauterine Growth RestrictionSGA
Small for Gestational Age
Janin yang kecil, dengan risiko luaran perinatal lebih buruk
dibandingkan janin yang tumbuh normal
Terdapat redistribusi
hemodinamik sebagai respon adaptasi janin terhadap kondisi
undernutrition, hipoksia atau
gangguan (insufiseiensi) plasenta
Janin yang kecil, dengan luaran perinatal yang sama baik seperti janin yang tumbuh
normal
Tidak terdapat tanda-tanda respon adaptasi janin terhadap perubahan pada lingkungannya juga mempunyai risiko kelainan
perinatal dan neurodevelopmental
1. Which of the following is not true regarding intrauterine growth restriction?
• A. It is associated with premature labour
• B. It may be associated with a low socio-economic status
• C. These babies are at an increased risk of developing respiratory distress syndrome
• D. It may be associated with raised serum AFP at 16 weeks followed by normal scan
at18 weeks
Kehamilan multifetal meningkat sebanyak 3% pada populasi dunia. Persalinan preterm merupakan masalah utama dari kehamilan multifetal, global survey dari WHO menyatakan 35.2 % kehamilan multifetal berakhir
dengan persalinan preterm (Fallis, 2013; Wei, 2016)
PENDAHULUAN
Kehamilan multifetal merupakan hasil dari 2 atau lebih kejadian fertilisasi, fertilisasi tunggal diikuti
pembelahan ”erroneous´ dari zigot, atau kombinasi dari keduanya (Cunningham, 2018)
FAKTOR RISIKO
• 3,5% pada wanita kulit hitam, 3 % pada wanita kulit putih. Wanita Hispanik, Asia dan Amerika kemungkinanya lebih rendah daripada wanita kulit putih.
Ras
• Kejadian kembar dizigot meningkat pada usia 15-37 tahun
Usia saat kehamilan
• Kemungkinan meningkat 8x lipat saat paritas ≤4 dan 20x lipat saat paritas ≥5 (Olusanya,2012)
Jumlah paritas
• Riwayat kembar dari ibu lebih berpengaruh daripada riwayat kembar dari ayah
Hereditas
• Beberapa penelitian menunjukkan wanita yang mendapat asam folat memiliki prevalensi yang lebih tinggi. Pada World
War II di eropa saat pemenuhan nutrisi bagi wanita hamil
lebih sulit tercatat penurunan angka kehamilan kembar
Nutrisi
• Peningkatan kelahiran kembar berkaitan dengan pelepasan FSH hipofisis yang berlebihan sebagai respons terhadap penurunan umpan balik negatif dari kegagalan impending ovarium
Gonadotropin Pituari
• Induksi ovulasi dengan FSH plus human chorionic
gonadotropin (hCG) atau klomifen sitrat meningkatkan
kemungkinan ovulasi bersamaan.
Terapi Infertilitas
DIZIGOTIK VS
MONOZIGOTIK
Dizigotik
Lebih sering Dipengaruhi kadar FSH (geografi, ras, multipara, usia, kontrasepsi) Selalu dikorionikMonozigotik
Jarang (3.5-4/1000 kelahiran) Paling dipengaruhi genetik Korionisitas tergantung kapan membelah (Cunningham et al, 2018) (Basiri et al, 2019)KLASIFIKASI
DICHORIO
N
19
DIAGNOSIS MULTIFETAL
Evaluasi Klinis
Sonograf
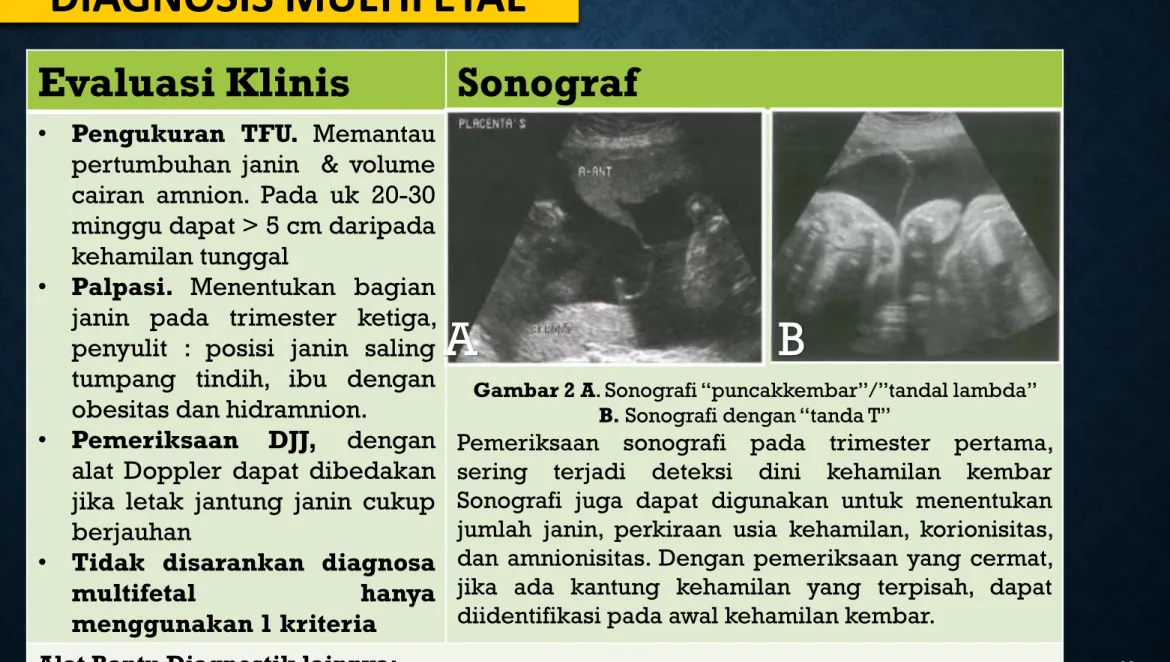
• Pengukuran TFU. Memantau
pertumbuhan janin & volume cairan amnion. Pada uk 20-30 minggu dapat > 5 cm daripada kehamilan tunggal
• Palpasi. Menentukan bagian
janin pada trimester ketiga, penyulit : posisi janin saling tumpang tindih, ibu dengan obesitas dan hidramnion.
• Pemeriksaan DJJ, dengan
alat Doppler dapat dibedakan jika letak jantung janin cukup berjauhan
• Tidak disarankan diagnosa
multifetal hanya
menggunakan 1 kriteria
Gambar 2 A. Sonografi “puncakkembar”/”tandal lambda” B. Sonografi dengan “tanda T”
Pemeriksaan sonografi pada trimester pertama, sering terjadi deteksi dini kehamilan kembar Sonografi juga dapat digunakan untuk menentukan jumlah janin, perkiraan usia kehamilan, korionisitas, dan amnionisitas. Dengan pemeriksaan yang cermat, jika ada kantung kehamilan yang terpisah, dapat diidentifikasi pada awal kehamilan kembar.
Alat Bantu Diagnostik lainnya:
• Radiografi abdominal sulit saat janin bergerak dan uk <18minggu • Magnetic Resonannce Imaging patologi kembar yang lebih detail
• Kadar β-hCG dan maternal serum levels of alpha-fetoprotein (MSAFP) meningkat
• Evaluasi USG perkiraan usia kehamilan, menentukan korionisitas dan screening Down’s syndrome
Menentukan usia kehamilan dan korionisitas
• Lebih beresiko anemia rutin evaluasi as folat/zat besi
Diet and Nutrisi
Perawatan spesialistik
• Skrining down syndrome saat CRL : 45 mm - 84 mm (pada usia kehamilan : 11 – 13+6 minggu)
• Screening kombinasi : nuchal translucency, β hCG , pregnancy
associated plasma protein A)
• Monitoring untuk IUGR
SKRINING
Usia kehamilan 16-17, 19-20, dan 21-22 minggu
untuk skrining TTTS dan TAPS serta skrining jantung sebagai bagian dari skrining anatomi
lengkap pada minggu ke 18-19 minggu atau pada minggu ke 21-22.
USG pada usia kehamilan 11+0 minggu
hingga 13+6 minggu (CRL 45-84 mm)
berfungsi untuk menilai viabilitas janin, usia kehamilan dan korionisitas, serta melihat
adanya malformasi kongenital mayor
Jika tidak terdapat kelainan dilanjutkan pemeriksaan pertumbuhan pada
PILIHAN PERSALINAN
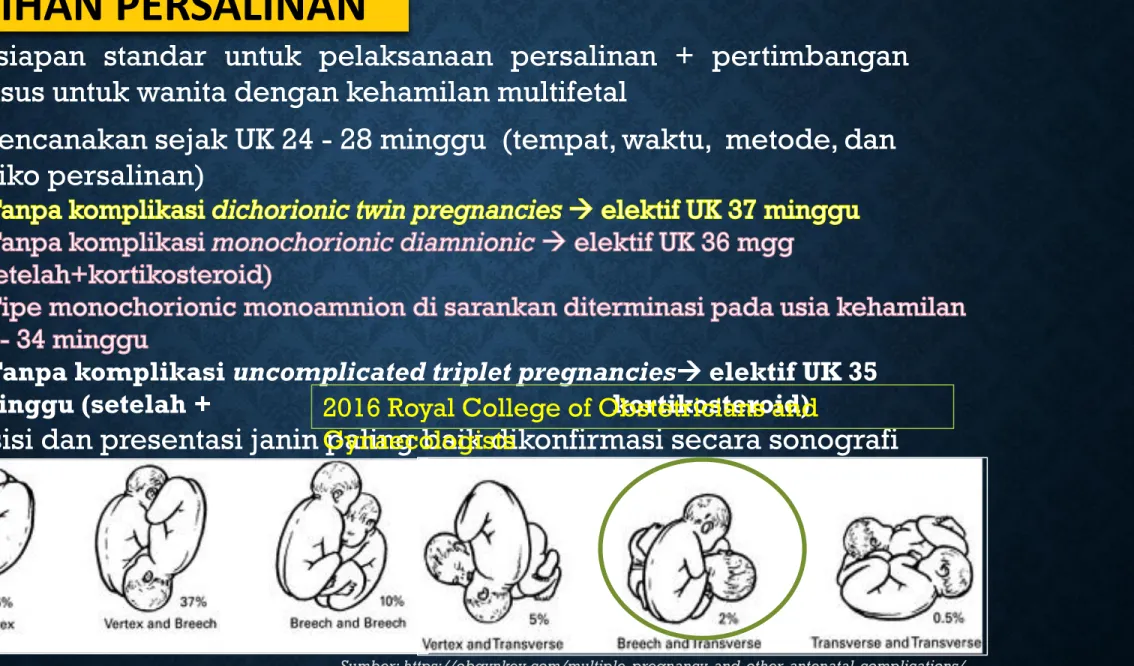
Direncanakan sejak UK 24 - 28 minggu (tempat, waktu, metode, dan
resiko persalinan)
- Tanpa komplikasi uncomplicated triplet pregnancies elektif UK 35 minggu (setelah + kortikosteroid)
Persiapan standar untuk pelaksanaan persalinan + pertimbangan
khusus untuk wanita dengan kehamilan multifetal
Posisi dan presentasi janin paling baik dikonfirmasi secara sonografi
Gambar 3. Macam-macam presentasi janin pada kehamilan
kembar
Sumber: https://obgynkey.com/multiple-pregnancy-and-other-antenatal-complications/
2016 Royal College of Obstetricians and Gynaecologists
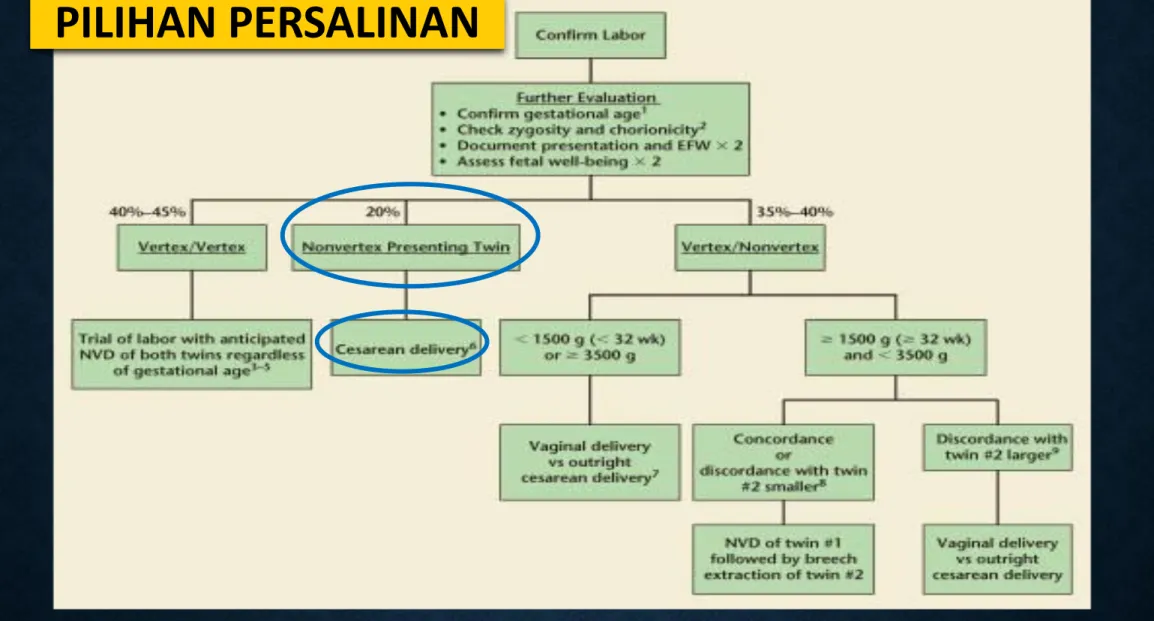
Christopher D, Robinson BK, Peaceman AM. An evidence-based approach to determining route of delivery for twin gestations. Rev Obstet Gynecol. 2011;4(3-4):109-116.
Gambar 4. Alur pemilihan persalinan pada kehamilan kembar
(Christoper, 2011)
MATERNAL
Persalinan preterm (35.2%) ( Jun Wei, 2016) Hipertensi dalam kehamilan 2.5 -2.8 kali (Devine and Malone, 2004) Diabetes dalam kehamilan 2.2 kali (Rauh-Hain et al., 2009). AFLP 7.1% hingga 28.6% (Minakami et al., 2014). Anemia (multifetal triplet, 70%)(Devine and Malone, 2004). Cholelitiasis 0.4% - 5.5% (Rissanen et al., 2019)
KOMPLIKASI
(ACOG, 2016)
KOMPLIKASI
Preterm Delivery
Deteksi
• Pada pasien asimptomatik tidak dianjurkan melakukan tindakan intervensi yang bertujuan untuk skrining risiko preterm
• Pada pasien simtomatik dapat dilakukan pengukuran panjang serviks dan skrining fetal fibronectin sebagai bantuan untuk prediksi risiko kelahiran preterm. Panjang serviks 25mm adalah cut-off paling sering digunakan pada trimester kedua
Pencegahan
• Belum ada Tindakan intervensi yang direkomendasikan untuk memprolong masa kehamilanManajemen
• Tokolitik dapat diberikan untuk memperpanjang masa kehamilan jangka pendek
• Pemberian kortikosteroid antenatal untuk wanita hamil usia 24-34 minggu mengurangi insiden kematian neonatal karena distres pernapasan
• Pemberian magnesium sulfat prenatal dapat dilakukan untuk mengurangi terjadinya cerebral palsy
FETAL
Gambar 2. Overview insidensi komplikasi kehamilan ganda (Cunningham, 2014)
KOMPLIKASI
Dichorion
Diamnion Monochorion Diamnion Monochorion Monoamnion
TTTS Rare 15% 2-6%
TAPS - Up to 5 % -
TRAP - 1% 1%
sIUGR 11.6% 12% -
Tabel 1. Insidensi komplikasi fetal pada kehamilan Multifetal (Rauh-Hain et al., 2009; Anca et al.,
2015; Buyukkaya, Tekbas and Buyukkaya, 2015; Johnson, 2015; K.Behavkova, 2016; Lanna et al., 2019; Antonakopoulos et al., 2020; Gleeson et al., 2020)
KOMPLIKASI
Twin to Twin Trnasfussion syndrome
Mempengaruhi 15% dari kehamilan multifetal monochorionic.
FETAL
• Treament of choice adalah ablasi laser
pada quintero stage II
(Rekomendasi: A)
• Konservatif management dilakukan
pada quintero stage I (Rekomendasi B)
• Amnioreduction bertahan sebelum
usia kehamilan 26 minggu
(Rekomedasi A) (Khalil et al., 2016)
KOMPLIKASI
Twin Anemia – Polycyteamia Sequence (TAPS)
Mempengaruhi 2% dari kehamilan multifetal dan 13% setelah mendapatkan terapi ablasi laser
FETAL
Pilihan terapi pada TAPS bergantung kasus per kasus. Terapi paling umum adalah konservatif, early delivery, ablasi
laser, transfusi intrauterine, partial
exchange transfusion (Evidence Level 3)
(Khalil et al., 2016).
KOMPLIKASI
Twin Reversed Arterial PerfusionSequence (TRAPS)
FETAL
Terapi utama dari TRAPS
adalah discontinuation
transfusion dari janin
acardiac, dengan cara
ligasi tali pusat dari janin acardiac (Evidence Level 3).
(Khalil et al., 2016)
Twin Reverse Arterial Perfussion (TRAP) terjadi pada 1% kehamilan multifetal dengan
janin kedua acardiac.
KOMPLIKASI
Selective Intra Uterine Growth Restriction
FETAL
Terminasi merupakan pilihan utama dimana bila termasuk dalam tipe I direkomendasikan pada usia kehamilan 34-36 minggu, sedangkan pada tipe II dan III disarankan dilakukan terminasi pada usia kehamilan 32 minggu
MANAGEMENT
• sFGR, secara konvensional, didefinisikan sebagai suatu kondisi di mana satu janin memiliki EFW <10 percentile dan diskrepansi EFW dengan kembarannya > 25%
• Terjadi pada 10-15% kehamilan multifetal
• Tipe I, waveform doppler arteri umbilikalis terdapat positive end-diastolic flow
• Tipe II, terdapat absent or reversed end-diastolic flow (AREDF).
• Tipe III, terdapat pola AREDF yang memebntuk siklus/intermittent
2. Which of the following is true regarding the monozygotic twins?
• A. Are more common than dizygotic twins
• B. Are commonly familial
• C. May be reliably distinguished from dizygotic twins by the naked-eye examination
of the foetal membranes and placentae
• D. Have a higher incidence of placenta praevia than singleton pregnancies
3. Which of the following complication is associated with multiple births?
• A. Increased incidence of congenital abnormalities
• B. Increased incidence of growth retardation
• C. Increased incidence of postpartum haemorrhage
• D. Increased incidence of preterm labour
4. Second trimester bleeding may be due to which of the following cause? • A. Missed abortion • B. Premature labour • C. Erythroblastosis fetalis • D. Threatened abortion • E. Monilial infection
5. Which of the following is not true regarding ABO blood group incompatibility between mother and foetus?
• A. It is associated with a strongly positive direct Coombs’ test
• B. Its severity does not vary between the first and subsequent pregnancies
• C. It is usually detected in the antenatal period
• D. Manifests itself on the first or second day of life
6. Which of the following is not true regarding preimplantation genetic diagnosis?
• A. Disorders caused by a single gene defect can be detected
• B. It should be used to exclude Down syndrome in a couple undergoing IVF using a
donor ovum from a 23-year-old, into a 46-year-old recipient
• C. Foetal sex can be determined
• D. HLA status can be determined
7. Which of the following is true regarding a 37 yearold-woman at 16 weeks’ gestation?
• A. Has a risk of Down syndrome of 1:100
• B. Should be advised to have screening for Down syndrome
• C. Should be advised to have amniocentesis, not the ‘triple’ test
• D. Is at increased risk of Edward’s syndrome
8. Regarding ‘HELLP’ syndrome which of the following statement is not true?
• A. It is related to preeclampsia
• B. It may occur in non-pregnant patients
• C. Upper abdominal quadrant pain is a characteristic feature
• D. Patients may have low platelets
9. Which of the following statement is correct regarding the foetal scalp ph?
• A. A result of 7.28 is normal
• B. Accurately determines the condition of the baby
• C. Carries no risk
• D. Cannot be performed in cases of breech presentation
• E. Increases the Caesarean section rate in patients having continuous electronic
10. Which of the following is not true regarding the epidural space?
• A. Commences at the foramen magnum
• B. Contains Batson’s plexus
• C. Ends at the level of S2 in the adult
• D. Negative pressure within the space is greatest in the lumbar and sacral regions
11. Which of the following is true regarding classical caesarean section?
• A. Is Caesarean section performed through a mid-line abdominal incision
• B. Is never done nowadays
• C. Carries an increased risk of dehiscence of the abdominal wound
• D. Is a ground for elective repeat caesarean section
12. Which of the following is not true regarding the ventouse method of delivery?
• A. May employ a metal cup
• B. Has increased in popularity with electronic pumps
• C. Can be used safely in the absence of criteria necessary for a forceps delivery
• D. Requires the patient to be in the lithotomy position
13. Which of the following steps must be taken at the time of massive post-partum haemorrhage?
• A. An anaesthetist is essential to assist in the management of the patient
• B. Initial cross-matching of three units of blood is sufficient
• C. Bimanual uterine compression has no role in these cases
• D. Uncross-matched O rhesus-positive blood may be given in an emergency
14. Which of the following is true regarding breastfeeding?
• A. Human milk contains more protein than cow milk.
• B. Human milk has a higher energy content and more fat than cow milk
• C. Breast feeding does not protect against infection in the baby.
• D. Breast milk is of uniform composition throughout a feed.
15. Hydramnios is not associated with which of the following conditions?
• A. Twin-twin transfusion syndrome
• B. Diabetes
• C. Potter’s syndrome
• D. Hydrops fetalis
16. Which of the following is not true regarding the routine ultrasound scan at 18– 20+6
weeks?
• A. The National Screening Committee has recommended 6 basic measurements that should be taken
• B. The National Screening Committee has identified 11 foetal anomalies to be looked for • C. Screening for placenta praevia is at the top of the list
• D. Choroid plexus cysts no longer need any response • E. Presence of echogenic bowel requires a response
17. Epidural bupivacaine administered during labour may cause which of the following?
• A. An increased rate of caesarean delivery
• B. Decreased uterine contractility
• C. Pruritus
• D. Tinnitus
18. Which of the following statement is not correct regarding external cephalic version?
• A. Anti-D should be given to rhesus negative mothers.
• B. Is best done at 32 weeks
• C. Reduces the incidence of breech presentation at term
• D. Is more successful if a beta-sympathomimetic is used
19. Which of the following is not true regarding a newborn term infant?
• A. Anaemia may be caused by a cephalhaematoma
• B. Ballotable kidneys may not always be abnormal
• C. Oedema of the feet and hands suggest Turner’s syndrome
• D. The Apgar score at 5 minutes is more predictive of later neurodevelopment
prognosis than Apgar score at 1 minute
• E. The findings of bilateral single palmar creases in an otherwise normal-appearing
20. Which of the following is true regarding haemoglobin values of less 10g/dl during pregnancy?
• A. Is a recognised side-effect of anti-convulsant therapy
• B. Is associated with urinary tract infection
• C. Is a complication of multiple pregnancy
• D. Increases the risk of post-partum haemorrhage
21. Which of the following is true regarding thyrotoxicosis in pregnancy?
• A. It is usually due to a solitary adenoma
• B. The major maternal risk is congestive cardiac failure
• C. Beta-blocking drugs are contra-indicated
• D. May be treated with radioactive iodine as the drug does not cross the placenta
22. Which of the following is true regarding hypertension in pregnancy?
• A. It is of little significance unless accompanied by proteinuria
• B. It causes foetal growth restriction in more than half of affected women
• C. It is not associated with an increased incidence of bleeding from placental
praevia
• D. It should be assessed by admission to hospital
23. Which of the following is not true concerning the blood pressure regulation?
• A. Adrenaline acts primarily upon the vasomotor centre
• B. Angiotensinogen is inactive without modification
• C. Bradykinin decreases blood pressure
• D. Prostacyclin lowers blood pressure
24. Which of the following is not true regarding placental abruption?
• A. May have no associated vaginal bleeding
• B. Is an indication for delivery
• C. Has a higher incidence with maternal cocaine abuse
• D. May be identified using ultrasound to demonstrate retroplacental clot
• E. The diagnosis of concealed abruption can be easily confused with that of acute
25. Which of the following is true regarding the Kleihauer test?
• A. It may be used to confirm the presence of Rhesus antibodies
• B. It should be performed routinely at 28 and 36 weeks in the woman who is rhesus
negative
• C. It is no longer required after delivery in the Rhesus negative woman
• D. It is based on the relative resistance of foetal haemoglobin to denaturation using
an acid solution