Child abuse: Parental mental illness, learning disability,
substance misuse, and domestic violence
Hedy Cleaver
Ira Unell
C h i l d a b u s e : P a r e n t a l m e n t a l i l l n e s s , l e a r n i n g d i s a b i l i t y,
s u b s t a n c e m i s u s e a n d d o m e s t i c v i o l e n c e
2 n d e d i t i o n
H E DY C L E AV E R , I R A U N E L L A N D J A N E A L D G AT E
UTP
xxx/utptipq/dp/vl
Nbjm-!Ufmfqipof-!Gby!'!F.nbjm
QP!Cpy!3:-!Opsxjdi-!OS4!2HO
Ufmfqipof!psefst0Hfofsbm!forvjsjft;!1981!711!6633 Gby!psefst;!1981!711!6644
F.nbjm;!dvtupnfs/tfswjdftAutp/dp/vl Ufyuqipof;!1981!351!4812
UTPACmbdlxfmm!boe!puifs!Bddsfejufe!Bhfout
PublishedfortheDepartmentforEducationunderlicencefromtheControllerof HerMajesty’sStationeryOffice.
Allrightsreserved. ©CrownCopyright2011
Youmayreusethisinformation(excludinglogos)freeofchargeinanyformator medium,underthetermsoftheOpenGovernmentLicence.Toviewthislicence,visit http://www.nationalarchives.gov.uk/doc/opengovernmentlicence/
oremail:[email protected].
Wherewehaveidentifiedanythirdpartycopyrightinformationyouwillneedtoobtain permissionfromthecopyrightholdersconcerned.
Thispublicationisalsoavailablefordownloadatwww.officialdocuments.gov.uk ISBN:9780117063655
List of figures and tables vi
Preface vii
Acknowledgements viii
Introduction 1
Researchcontext 1
Legalandpolicycontext 8
Limitationsoftheresearchdrawnoninthispublication 16
Structureofthebook 18
PART I: GENERAL ISSUES AFFECTING PARENTING CAPACITY 21
1 Is concern justified? Problems of definition and prevalence 23
Problemswithterminology 23
Prevalenceofparentswithproblemdrinkingordrugmisuse:general
Summaryoftheevidenceforalinkbetweenparentaldisordersand
Prevalence 27
Prevalenceofparentalmentalillness:generalpopulationstudies 28 Prevalenceofparentallearningdisability:generalpopulationstudies 33
populationstudies 36
Prevalenceofdomesticviolence:generalpopulationstudies 43
childabuse 47
Tosumup 48
2 How mental illness, learning disability, substance misuse and domestic
violence affect parenting capacity 49
Impactonparenting 61
Socialconsequences 74
Tosumup 80
3 Which children are most at risk of suffering significant harm? 85
Whatconstitutessignificantharm? 85
Vulnerablechildren 86
Protectivefactors 90
Tosumup 93
Movingontoexploretheimpactonchildrenatdifferentstagesof
development95
PART II: ISSUES AFFECTING CHILDREN OF DIFFERENT AGES 97
4 Child development and parents’ responses – children under 5 years 99
Prebirthto12months 99
Prebirthto12months–theunbornchild 99
Tosumup 108
Prebirthto12months–frombirthto12months 108
Tosumup 115
Childrenaged1–2years 116
Tosumup 124
Childrenaged3–4years 125
Tosumup 134
Identifieddevelopmentalneedsinchildrenunder5years 135
5 Child development and parents’ responses – middle childhood 137
Childrenaged5–10years 137
Tosumup 155
Childrenaged11–15years 159
Tosumup 179
Childrenaged16yearsandover 180
Tosumup 193
Identifiedunmetdevelopmentalneedsinadolescence 195
PART III: CONCLUSIONS AND IMPLICATIONS FOR POLICY AND
PRACTICE 197
7 Conclusions 199
8 Implications for policy and practice 201
Earlyidentificationandassessment 201
Jointworking 204
Flexibletimeframes 205
Informationforchildrenandfamilies 206
Trainingandeducationalrequirements 207
Tosumup 208
Bibliography 211
Figures
Figure1.1 TheAssessmentFramework Tables
Table1.1 Prevalenceofmentalillnessamongadultsinthegeneralpopulation Table1.2 Prevalenceofmentalillnessamongparentsinthegeneralpopulation Table1.3 Relationshipbetweentherateofrecordedparentalproblemsandthe
levelofsocialworkintervention
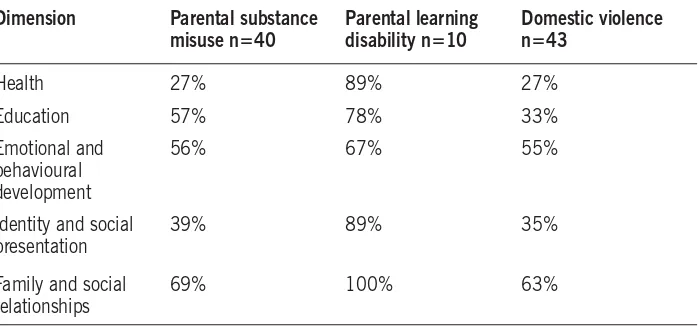
Table4.1 Proportionofchildrenwithidentifiedunmetneeds–childrenunder 5years
Table5.1 Proportionofchildrenwithidentifiedunmetneeds–middle childhood
Itisprobablytruetosaythat,formostpeople,childhoodisamixedexperience whereperiodsofsadnessandlossarebalancedwithmomentsofhappinessand achievement.Suchcomplexity,however,israrelyrepresentedintheliteratureof childhood.Indeed,muchofthewrittenwordinthenineteenthandtwentieth centuriesdepictschildhoodinoneoftwocontrastingways.Forexample,A.A. Milne’spoem‘IntheDark’,firstpublishedin1927,(Milne1971)showschildhood asagoldenerawherechildrenarelovedandnurturedbycaringparents.Itisa timecharacterisedbyinnocence,unqualifiedparentallove,irresponsibility,peer friendshipsandathirstforadventureandknowledge.
I’vehadmysupper, Andhadmysupper,
AndHADmysupperandall; I’veheardthestory
OfCinderella,
Andhowshewenttotheball; I’vecleanedmyteeth,
AndI’vesaidmyprayers,
AndI’vecleanedandsaidthemright; Andthey’veallofthembeen
Andkissedmelots,
They’veallofthemsaid‘Goodnight.’
Butneverfarawayisthealternativeexperience,typifiedbyparentaldesertion, illness,isolationandpoverty.JamesWhitcombRiley(1920),whopenneduplifting poemsofperhapsquestionablequalityforchildrenduringthe1890s,paintsamuch bleakerpictureinhispoem‘TheHappyLittleCripple’.
I’mthistalittlecrippleboy,an’nevergoin’togrow An’getagreatbigmanatall!–‘causeAuntytoldmeso. WhenIwasthistababyonc’t,Ifalledoutofthebed
An’got“TheCurv’tureoftheSpine”–‘at’swhattheDoctorsaid. IneverhadnoMothernen–fermyParunnedaway
Weacknowledgewithsincerethanksthemanypeoplewhogavegenerouslyoftheir timetohelpuswiththiswork.Weparticularlyappreciatetheexpertiseandadvice offeredbyArnonBentovim,RichardVelleman,LornaTempleton,CarolynDavies andSheenaPrentice.TheworkhasbeenfundedbytheDepartmentforEducation andwethankstaffinthedepartment,particularlyJennyGraywhosupportedus throughouttheworkwithherinterestandvaluablecomments.
Theworkwasassistedbyanadvisorygroupwhosemembershipwas:
ThissecondeditionofChildren’sNeeds–ParentingCapacityprovidesanupdate ontheimpactofparentalproblems,suchassubstancemisuse,domesticviolence, learningdisabilityandmentalillness,onchildren’swelfare.Research,andin particularthebiennialoverviewreportsofseriouscasereviews(Brandonetal2008; 2009;2010),havecontinuedtoemphasisetheimportanceofunderstandingand actingonconcernsaboutchildren’ssafetyandwelfarewhenlivinginhouseholds wherethesetypesofparentalproblemsarepresent.
Almostthreequartersofthechildreninboththisandthe200305studyhadbeen livingwithpastorcurrentdomesticviolenceandorparentalmentalillhealth andorsubstancemisuse–oftenincombination.
(Brandonetal2010,p.112)
Theseconcernswereverysimilartothosethatpromptedthefirsteditionofthis book,whichwascommissionedfollowingtheemergenceofthesethemesfromthe DepartmentofHealth’sprogrammeofchildprotectionresearchstudies(Department ofHealth1995a).Thesestudieshaddemonstratedthatahighlevelofparental mentalillness,problemalcoholanddrugabuseanddomesticviolencewerepresent infamiliesofchildrenwhobecomeinvolvedinthechildprotectionsystem.
Research context
andneglectthatitisdrainingtimeandresourceawayfromfamilies’(Munro2010,p.6). Munro’sInterimReport(2011)drawsattentiononceagaintothehighlytraumatic experienceforchildrenandfamilieswhoaredrawnintotheChildProtectionsystem wheremaltreatmentisnotfound,whichleavesthemwithafearofaskingforhelp inthefuture.Afindingwhichwasidentifiedbyearlierresearchonchildprotection (CleaverandFreeman1995).
Evidencefromthe1995childprotectionresearch(DepartmentofHealth1995a) indicatedthatwhenparentshaveproblemsoftheirown,thesemayadverselyaffect theircapacitytorespondtotheneedsoftheirchildren.Forexample,Cleaverand Freeman(1995)foundintheirstudyofsuspectedchildabusethatinmorethan halfofthecases,familieswereexperiencinganumberofproblemsincludingmental illnessorlearningdisability,problemdrinkinganddruguse,ordomesticviolence.A similarpictureofthedifficultiesfacingfamilieswhohavebeenreferredtochildren’s socialcareservicesemergesfrommorerecentresearch(CleaverandWalkerwith Meadows2004).Itisestimatedthatthereare120,000familiesexperiencing multipleproblems,includingpoormentalhealth,alcoholanddrugmisuse,and domesticviolence.‘Overathirdofthesefamilieshavechildrensubjecttochildprotection procedures’(Munro2011,p.30,paragraph2.30).
Children’sserviceshavethetaskofidentifyingchildrenwhomayneedadditional servicesinordertoimprovetheirwellbeingasrelatingtotheir:
(a) physicalandmentalhealthandemotionalwellbeing; (b) protectionfromharmandneglect;
(c) education,trainingandrecreation;
(d) thecontributionmadebythemtosociety;and (e) socialandeconomicwellbeing.
(Section10(2)oftheChildrenAct2004)
TheCommonAssessmentFramework(Children’sWorkforceDevelopment Council2010)andtheAssessmentFramework(DepartmentofHealthetal.2000) enablefrontlineprofessionalsworkingwithchildrentogainanholisticpictureof thechild’sworldandidentifymoreeasilythedifficultieschildrenandfamiliesmay beexperiencing.Althoughresearchsuggeststhatsocialworkers(Cleaveretal.2007) andhealthprofessionalsareequippedtorecogniseandrespondtoindicationsthata childisbeing,orislikelytobe,abusedorneglected,thereislessevidenceinrelation toteachersandthepolice(Danieletal.2009).
Forrester2009).Acallformorehighqualitytrainingonchildprotectionacross socialcare,healthandpolicewasalsomadebyLordLaming(2009).Munro’s reviewofchildprotectioninexploring‘whypreviouswellintentionedreformshave notresultedintheexpectedlevelofimprovements’(p.3)highlightedthe‘unintended consequencesofrestrictiverulesandguidance’,whichhaveleftsocialworkersfeeling that‘theirprofessionaljudgementisnotseenasasignificantaspectofthesocialwork task;itisnolongeranactivitywhichisvalued,developedorrewarded’(Munro2010, p.30,paragraph2.16).
Theexperienceofprofessionalsprovidingspecialistservicesforadultscan supportassessmentsofchildreninneedlivingwithparentalmentalillness,learning disability,substancemisuseordomesticviolence.Research,however,showsthatin suchcasescollaborationbetweenadults’andchildren’sservicesattheassessment stagerarelyhappens(Cleaveretal.2007;CleaverandNicholson2007)andalack ofrelevantinformationmaynegativelyaffectthequalityofdecisionmaking(Bell 2001).Anagreedconsensusofoneanother’srolesandresponsibilitiesisessential foragenciestoworkcollaboratively.TheevidenceprovidedtotheMunroreview (2011)found‘mixedexperiencesandabsenceofconsensusabouthowwellprofessionals areunderstandingoneanother’srolesandworkingtogether’andarguesfor‘thoughtfully designedlocalagreementsbetweenprofessionalsabouthowbesttocommunicatewith eachotherabouttheirworkwithafamily...’(Munro2011,p.28,paragraph2.23). Althoughresearchshowsthatthedevelopmentofjointprotocolsandinformation sharingproceduressupportcollaborativeworkingbetweenchildren’sandadults’ services(Cleaveretal.2007),asurveyof50Englishlocalauthoritiesfoundonly 12%hadclearfamilyfocusedpoliciesorjointprotocols(CommunityCare2009).
Themultiagencyapproach
Inmanyofthecasesthatarereferredtochildren’ssocialcare,nosingleagencywill beabletoprovideallthehelprequiredtosafeguardandpromotethewelfareof thechildandmeettheneedsoftheirparents.Socialworkers,inpartnershipwith familiesandotheragencies,mustjudgewhatservices,fromwhichagencies,are calledfor.Aresearchbasedtypologyoffamilieshasbeendevelopedtohelpsocial workersidentifytherange,typeanddurationofservicesrequiredtomeettheneeds ofthechildandsupportthefamily(CleaverandFreeman1995).Threecategories inthetypologyareparticularlyrelevant:
エ!
Families experiencing multiple problems: thesefamiliesarewellknownto
エ!
Families experiencing a specific problem: thesefamiliesarerarelyknownto statutoryagenciesandcometotheirattentionbecauseofaspecificissue,for exampleacuteparentalmentalillnessoraparentaldrugoverdose.Families arenotconfinedtoanysocialclassand,onthesurfacetheirlivesmayappear quiteordered.エ!
Acutely distressed families: thesefamiliesnormallycope,butanaccumulationofdifficultieshasoverwhelmedthem.Familiestendtobecomposedofsingle orpoorlysupportedandimmatureparents,orparentswhoarephysicallyill ordisabled.
Theabovetypologymakesacleardistinctionbetweenfamilieswhonormallycope wellbuthavebeenrecentlyoverwhelmedbyproblemsandthosewhohavemany chronicproblemswhichrequirelongtermmultiserviceinput.Toensurechildren’s safetyandwelfare,manyofthesefamilieswillrequiresupportfrombothchildren’s andadults’services.Acollaborativeapproachwouldensurethatnotonlyareparents recognisedashavingneedsintheirownright,buttheimpactofthoseneedson theirchildrenbecomespartofamultiagencyresponse.Researchsuggeststhatthe valueofsuchinteragencycollaborationiswidelyacceptedbyprofessionals(Cleaver etal.2007).AreviewoftheliteratureonneglectbyDanielandcolleagues(2009) highlightedtheimportanceofdevelopingmoreeffectiveintegratedapproaches tochildrenwhereallprofessionsregardthemselvesaspartofthechildwellbeing system.However,ensuringthatpracticereflectstheseprinciplesisnotalwayseasy, despitethesupportofnationalpolicyandguidance.
Despiteconsiderableprogressininteragencyworking,oftendrivenbyLocal SafeguardingChildrenBoardsandmultiagencyteamswhostrivetohelpchildren andyoungpeople,thereremainsignificantproblemsinthedaytodayrealityof workingacrossorganisationalboundariesandcultures,sharinginformationto protectchildrenandalackoffeedbackwhenprofessionalsraiseconcernsabouta child.
(LordLaming2009,p.10,paragraph1.6)
Theimportanceofanintegratedprofessionalgroupbeingaccountableforlocal childprotectionratherthanconfiningtheresponsibilitytochildren’ssocialcarewas stressedinMunro’sfirsttworeportsonthechildprotectionsystem(2010,2011).
Reluctancetoadmitproblems
insocialworkerstakingpunitiveaction.Subsequentresearchreinforcesthisfinding (see,forexample,BoothandBooth1996;Cleaveretal.2007;Gorin2004).
Forsimilarreasons,familieswereeagertoconcealdomesticviolence.Farmer andOwen’s(1995)researchsuggests,firstly,thathiddendomesticviolencemay accountformanymothers’seeminglyuncooperativebehaviourand,secondly, thatconfrontingfamilieswithallegationsofabusecouldcompoundthemother’s vulnerableposition.Indeed,childprotectionconferenceswereoftenignorantof whetherornotchildrenlivedinviolentfamiliesbecauseinthe‘faceofallegations ofmistreatmentcouplesoftenformedadefensiveallianceagainsttheoutsideagencies’
(FarmerandOwen1995,p.79).Infact,theauthorsfoundthatthelevelofdomestic violence(52%)discoveredduringtheresearchinterviewswastwicethatdisclosed attheinitialchildprotectionconference.‘Problemswhichparentsthoughtwouldbe discreditingwerenotairedintheearlystages–especiallythosewhichincludeddomestic violenceandalcoholanddrugabuse’(FarmerandOwen1995,p.190).
Thefearthatchildrenwillbetakenintocareandfamiliesbrokenupifparental problemscometolightmaybefeltmoreacutelywhenthemotherisfroma minorityethnicgroup.Difficultiesincommunicationandworriesovercultural normsbeingmisinterpretedincreasewomen’sfears,andofficialagenciesmaybe seenasparticularlythreateningifthemotherisofrefugeestatus(Stevenson2007). Parentsvalueprofessionalswhoarenonjudgementalintheirapproach,who communicatesensitivelyandwhoinvolvetheparentsandkeeptheminformed duringallstagesofthechildprotectionprocess(CleaverandWalkerwithMeadows 2004;KomulainenandHaines2009).Evidencesuggeststhatparentsareableto discusstheirownconcernsabouttheirparentingwhenprofessionalsapproachthem openlyanddirectly(Danieletal.2009).Unfortunately,manyparentsfeeltheyare treatedlesscourteouslybymedicalstaffonceconcernsofnonaccidentalinjuryare raised(KomulainenandHaines2009).
Workinginpartnershipwithchildrenandkeyfamily
members
Statutoryguidance,producedforprofessionalsinvolvedinassessmentsofchildren inneedundertheChildrenAct1989,acknowledgestheimportanceofinvolving childrenandfamiliesandseekstoensurethatallphasesoftheassessmentprocessare carriedoutinpartnershipwithkeyfamilymembers.
Thequalityoftheearlyorinitialcontactwillaffectlaterworkingrelationships andtheabilityofprofessionalstosecureanagreedunderstandingofwhatis happeningandtoprovidehelp.
(DepartmentofHealthetal.2000,p.13,paragraph1.47)
involvementinassessments,plansandreviews.Researchshowsthatmanysocial workersgotoconsiderablelengthstoexplainthingstoparents(particularlythose withlearningdisabilities)andchildren,andtoinvolvethemasmuchaspossiblein allstagesofthechildprotectionprocess(CleaverandWalkerwithMeadows2004). Asecondfindingisthatprofessionalstendtoevadefrighteningconfrontations;a featurewhichcontinuestobeidentifiedinseriouscasereviews(Brandonetal.2009, 2010;DepartmentforEducation2010c;LordLaming2009).Researchsuggests thatwhenprofessionalsfeelunsupportedormustvisitalone,visitingandchild protectionenquiriesmightnotalwaysbeasthoroughastheycouldbe(James1994; Denny2005;Farmer2006).
Gender
Fewofthe1995childprotectionstudiesexploredparentalproblemsintermsof genderandwhetherthegenderoftheparentwiththeprobleminfluencedsocial workintervention.Irrespectiveofwhichparentalfigurewaspresentingtheproblem, professionalsfocusedtheirattentiononworkingwithmothers.Insomecases, despiteprolongeddomesticviolencedirectedfromafatherfiguretothemother andsuspicionsthatthemanwasalsophysicallyabusivetothechildren,fatherswere rarelyinvolvedinthechildprotectionwork.‘Theshiftoffocusfrommentowomen allowedmen’sviolencetotheirwivesorpartnerstodisappearfromsight’(Farmer2006, p.126).However,forsomefamiliesthepossibilityofsocialworkersengagingwith thefatherfigurewasdifficultbecauseherefusedtodiscussthechildwiththeworker, wasalwaysoutduringsocialworkvisitsornolongerlivedinthehousehold(Farmer 2006).
Interpretingbehaviour
Afinalfactoridentifiedbytheoriginalchildprotectionstudies,andstillpertinent today,isthatsocialworkersmaymisinterpretparents’behaviour(Departmentfor Education2010c;HMGovernment2010a;C4EO2010).Forexample,research hasshownthatsocialworkerswerelikelytoassumethatguiltyorevasivebehaviour ofparentswasrelatedtochildabuse.Butsuchbehaviourwas,onoccasions,found tobetheresultofparentswantingtokeepsecretahistoryofmentalillness,learning disability,illicitdruguseorotherfamilyproblems(CleaverandFreeman1995).
2010c).Professionals’sympathyforparentscanleadtoexpectationsforchildren beingsettoolow.LordLamingstresses,‘Itisnotacceptabletodonothingwhenachild maybeinneedofhelp.Itisimportantthatthesocialworkrelationship,inparticular,isnot misunderstoodasbeingarelationshipforthebenefitoftheparents,orfortherelationship itself,ratherthanafocusedinterventiontoprotectthechildandpromotetheirwelfare’
(LordLaming2009,p.24,paragraph3.2).Practitionersupportwhichbenefits theparentsbutdoesnotpromotethewelfareofthechildrenwasalsoaconcern highlightedinMunro’sfirstreportofthechildprotectionsystem.Sheidentified‘a reluctanceamongmanypractitionerstomakenegativeprofessionaljudgmentsabouta parent....Incaseswhereadultfocusedworkersperceivedtheirprimaryroleasworking withintheirownsector,failuretotakeaccountofchildreninthehouseholdcouldfollow’
(Munro2010,p.17,paragraph1.27).Akeyfindingfromareviewofevidenceon whatworksinprotectingchildrenlivingwithhighlyresistantfamilieswastheneed forauthoritativechildprotectionpractice.
Families’lackofengagementorhostilityhamperedpractitioners’decisionmaking capabilitiesandfollowthroughwithassessmentsandplans...practitioners becameoverlyoptimistic,focusingtoomuchonsmallimprovementsmadeby familiesratherthankeepingfamilies’fullhistoriesinmind.
(C4EO2010,p.2)
Alackofknowledgeaboutdifferentcultureswithinminoritycommunities canalsobeabarriertounderstandingwhatishappeningtothechildren.Inquiry reportsandresearchhavehighlightedthatstereotypingoffamiliesfromdifferent backgrounds,linkedwithdifficultiesinattributingthecorrectmeaningtowhat parentssay,mayhaveanegativeimpactonsocialworkassessmentsandjudgements (DuttandPhillips2000).Forexample,inthecaseofVictoriaClimbié,achildwho cametoEnglandfromtheIvoryCoastofAfrica,professionalsassumedtheunusual, exceptionallyrespectfulandfrequentlyfrozenresponsetoher‘mother’wasnormal inthefamily’sculture,wheninfactitwasasignthatVictoriawasafraidofher abusivecarer(Cm57302003;ArmitageandWalker2009).Communicationand understandingcanbeeasedwhenparentshavetheopportunitytousethelanguage oftheirchoice(GardnerandCleaver2009).Thefollowingconclusion,drawnfrom analysingchilddeathsandseriousinjury,isrelevanttoallthoseprofessionalswho haveconcernsaboutthewelfareandsafetyofachild.
Inordertohaveabetterchanceofunderstandinghowdifficultiesinteract, practitionersmustbeencouragedtobecurious,andtothinkcriticallyand systematically.
Legal and policy context
Safeguardingandpromotingchildren’swelfare
TheChildrenAct1989placesadutyonlocalauthoritiestoprovidearangeof appropriateservicesforchildrentoensurethatthose‘inneed’aresafeguardedand theirwelfareispromoted.Childrenaredefinedas‘inneed’whentheyareunlikely toreachormaintainasatisfactorylevelofhealthordevelopment,ortheirhealth anddevelopmentwillbesignificantlyimpairedwithouttheprovisionofservices (s17(10)oftheChildrenAct1989).
Althoughmanyfamiliescopeadequatelywiththedifficultiestheyface,others needtheassistanceofservicesandsupportfromoutsidethefamilyto‘safeguardand promotethewelfareofthechildren’,whichisdefinedas:
エ!
protectingchildrenfrommaltreatment;
エ!
preventingimpairmentofchildren’shealthordevelopment;
エ!
ensuringthatchildrenaregrowingupincircumstancesconsistentwiththe provisionofsafeandeffectivecare;
andundertakingthatrolesoastoenablethosechildrentohaveoptimumlife chancesandtoenteradulthoodsuccessfully.
(HMGovernment2010a,p.34,paragraph1.20)
TheDepartmentofHealth‘regardssafeguardingvulnerablechildrenasahigh priorityandissupportingtheNHStoimprovesafeguardingarrangements’(Department ofHealth2010a,p.6).Providingsupporttoparentsinordertoimproveoutcomesfor childrenispartoftheGovernment’sstrategytoimprovepublichealth.IntheWhite PaperHealthyLives,HealthyPeople(Cm79852010)theGovernmentseekstogive
evidence‘tosuggestthatthefirstthreeyearsoflifecreatethefoundationinlearninghow toexpressemotionandtounderstandandrespondtotheemotionsofothers’(Allen2011, p.5,paragraph15).Thereisanemphasisonearlyinterventionpackageswhich haveaproventrackrecord,andarecommendationthatanew,EarlyIntervention Foundationiscreated.
Pastgovernmentshavealsosoughttorespondtotheneedsofvulnerablefamilies withtheaimofimprovingthewellbeingofchildren.TheChildrenAct1989 recognisedthattopromotechildren’swelfare,servicesmayneedtoaddressthe difficultiesthatparentsexperience.
Parentsareindividualswithneedsoftheirown.Eventhoughservicesmaybe offeredprimarilyonbehalfoftheirchildren,parentsareentitledtohelpand considerationintheirownright...Theirparentingcapacitymaybelimited temporarilyorpermanentlybypoverty,racism,poorhousingorunemploymentor bypersonalormaritalproblems,sensoryorphysicaldisability,mentalillnessor pastlifeexperiences...
(DepartmentofHealth1991,p.8)
UndertheChildrenAct2004‘achildren’sservicesauthorityinEnglandmusthave regardtotheimportanceofparentsandotherpersonscaringforchildreninimproving thewellbeingofchildren’(Section10(3)oftheChildrenAct2004).
TheNationalFrameworkforChildren,YoungPeopleandMaternityServices stressedtheimportanceofprovidingsupporttoparentsandtheneedforcollaboration betweenadults’andchildren’sservices.
Inadditiontomeetingthegeneralneedsofparentsfromdisadvantaged backgrounds,itisimportanttoconsiderthemorespecialisedformsofsupport requiredbyfamiliesinspecificcircumstances,suchassupportforparentswith mentalhealthdifficultiesordisabilities,orwithsubstancemisuseproblems.Good collaborativearrangementsarerequiredbetweenservicesforadults,wherethe adultisaparent,andchildren’sservices,inparticular,wherechildrenmaybe especiallyvulnerable.
(DepartmentofHealthandDepartmentforEducationandSkills2004, p.69,paragraph3.4).
TheneedsofvulnerablechildrenwereaddressedintheDepartmentofHealth’s revisedcodeofpracticewhichprovidesguidancetodoctors,relevanthospitalstaff andmentalhealthprofessionalsonhowtheyshouldproceedwhenundertaking theirdutiesundertheMentalHealthAct1983.Thecodeofpracticenotesthat practitionersshouldensurethat:
エ!
appropriatearrangementsareinplacefortheimmediatecareofdependent children;
エ!
thebestinterestsandsafetyofchildrenarealwaysconsideredin arrangementsforchildrentovisitpatientsinhospital;and
エ!
thesafetyandwelfareofdependentchildrenaretakenintoaccountwhen cliniciansconsidergrantingleaveofabsenceforparentswithamental disorder.
(DepartmentofHealth2008)
Improvingchildprotectionandreformingfrontlinesocialworkpracticeis apriorityfortheGovernment.Althoughpastgovernmentswerecommittedto protectingchildren,statisticalreturnsonthenumbersofchildrensubjecttoachild protectionplancontinuetoincreasesuggestingmoreneedstobedone(Department forEducation2009and2010a).AtMarch201039,100childrenweresubjecttoa childprotectionplan,anincreaseof5,000(15%)fromthe200809figures(Munro 2011,p.25).Threeprinciplesunderpinnedtherecentreviewofchildprotection whichtheGovernmentaskedProfessorMunrotoundertake:‘earlyintervention; trustingprofessionalsandremovingbureaucracysotheycanspendmoreoftheirtimeon thefrontline;andgreatertransparencyandaccountability’(Munro2010,p.44).
TheChildrenAct2004placedstatutorydutiesonlocalagenciestomake arrangementstosafeguardandpromotethewelfareofchildreninthecourseof dischargingtheirnormalfunctions.Ensuringeffectiveinteragencyworkingisa keyresponsibilityofLocalSafeguardingChildrenBoards(LSCBs).LSCBsshould ensurethatagenciesdemonstrategoodcollaborationandcoordinationincases whichrequireinputfrombothchildren’sandadults’services.Servicesforadults includeGPsandhospitals,learningdisabilityandmentalhealthteams,drugaction teamsanddomesticviolenceforums.
Asurveyoftheorganisationsresponsibleforsafeguardingandpromotingthe welfareofchildrenundersection11oftheChildrenAct2004suggestedthat althoughsignificantprogresshasbeenmade,twothirdsoforganisationsdidnotyet haveallthekeyarrangementsinplace(MORI2009).TheGovernment’sstatutory guidanceWorkingTogethertoSafeguardChildrenmakesclearthatsafeguardingand promotingthewelfareofchildren‘dependsoneffectivejointworkingbetweenagencies andprofessionalsthathavedifferentrolesandexpertise’(HMGovernment2010a, p.31,paragraph1.12).
Adultmentalhealthservices–includingthoseprovidinggeneraladultand community,forensic,psychotherapy,alcoholandsubstancemisuseandlearning disabilityservices–havearesponsibilityinsafeguardingchildrenwhenthey becomeawareof,oridentify,achildatriskofharm.
Parentalmentalillness
TheGovernmentiscommittedto
‘protectingthepopulationfromserioushealththreats;helpingpeoplelivelonger, healthierandmorefulfillinglives;andimprovingthehealthofthepoorest,fastest; andliftingfamiliesoutofpoverty.’
(Cm79852010,p.4(1))
Poormentalhealthisakeycomponentoftheoverallburdenoflongstanding illnesswithinthegeneralpopulationandisresponsibleforthegreatestproportionof workingdayslost(HealthandSafetyExecutive2010).Initsstrategyforimproving publichealthinEngland,theGovernmenthasidentifiedtheneedtotargetarange ofissuesincludingmentalillness,heavydrinkinganddrugmisuse(Cm79852010). Itrecognisesthatnosingleagencycandothisalone.‘Responsibilityneedstobeshared rightacrosssociety–betweenindividual,families,communities,localgovernment, business,theNHS,voluntaryandcommunityorganisations,thewiderpublicsectorand centralgovernment’(Cm79852010,p.24,paragraph2.5).TheCrossGovernment mentalhealthoutcomesstrategysetsoutplanstoensurementalhealthawareness andtreatment(forchildrenaswellasadults)aregiventhesameprominenceas physicalhealth.Sixobjectivesarehighlighted:
(i) Morepeoplewillhavegoodmentalhealth
(ii) Morepeoplewithmentalhealthproblemswillrecover
(iii) Morepeoplewithmentalhealthproblemswillhavegoodphysicalheath (iv) Morepeoplewillhaveapositiveexperienceofcareandsupport
(v) Fewerpeoplewillsufferavoidableharm
(vi) Fewerpeoplewillexperiencestigmaanddiscrimination
(HMGovernment2011,p.6,paragraph1.5)
Childrenareattheheartofthisstrategy.Itacknowledgesthatsomeparents‘will requireadditionalsupporttomanageanxietyanddepressionduringpregnancyandthe child’searlyyears...’(HMGovernment2011,p.39,paragraph5.5).Theaimisto interveneearlywith‘vulnerablechildrenandyoungpeopleinordertoimprovelifetime healthandwellbeing,preventmentalillnessandreducecostsincurredbyillhealth, unemploymentandcrime’(p.9,paragraph1.15).Itisanticipatedearlyintervention willbringbenefitsnotonlytotheindividualduringchildhoodandintoadulthood, butalsoimprovehisorhercapacitytoparent.
‘Goodpartnershipworkingbetweenhealthandsocialcareisvitalforhelpingthemtomanage theirconditionandliveindependently’(DepartmentofHealth2010b,p.13,paragraph 3.13).
Parentswithalearningdisability
TheEqualityAct2010prohibitsserviceprovidersdiscriminatingonanumberof criteriaincludingdisability.Disabilityisdefinedinthefollowingway.
(1)Aperson(P)hasadisabilityif—
(a)Phasaphysicalormentalimpairment,and
(b)theimpairmenthasasubstantialandlongtermadverseeffectonP’s
abilitytocarryoutnormaldaytodayactivities.
(Section6(1)oftheEqualityAct2010)
Section47(1)oftheNationalHealthServicesandCommunityCareAct1990 placesadutyonlocalauthoritiestoconsidertheneedsofdisabledpersons,including thosewithlearningdisabilities.Thisissupportedbypracticeguidance.
Ingeneral,councilsmayprovidecommunitycareservicestoindividualadults withneedsarisingfromphysical,sensory,learningorcognitivedisabilities,or frommentalhealthneeds.
(DepartmentofHealth2010b,p.18,paragraph43)
Supportingdisabledadultsintheirroleasparentsishighlightedinthispractice guidance.Forexample,indeterminingeligibility,allfourlevelsincludethesituation inwhich‘familyandothersocialrolesandresponsibilitiescannotorwillnotbe undertaken’(DepartmentofHealth2010b,p.20,paragraph54).Localauthorities areenjoinedtoconsidertheadditionalhelpthoseadultswith,forexample, mentalhealthdifficultiesorlearningdisabilitiesmayneediftheyhaveparenting responsibilities.Thisincludesidentifyingwhetherachildoryoungpersonisacting inacaringroleandtheeffectthisishavingonthemandexploringwhetherthereis aneedtosafeguardandpromotethewelfareofthechild.
Parentalsubstancemisuse
IntheGovernment’sdrugstrategy,theimpactofdrugsandalcoholmisuseonsociety isrecognised.
Fromthecrimeinlocalneighbourhoods,throughfamiliesforcedapartby dependency,tothecorruptingeffectofinternationalorganisedcrime,drugshave aprofoundandnegativeeffectoncommunities,familiesandindividuals.
(HMGovernment2010b,p.3)
interveningearlyandsupportingpeopletorecover.Relevantagenciesareexpectedto worktogethertoaddresstheneedsofthewholeperson.Topreventsubstancemisuse amongstchildrenandyoungpeople(someofwhomwillhaveparentswhomisuse drugsandalcohol)thestrategyadvocatestheuseoffamilyfocusedinterventions (HMGovernment2010b,p.11).
Ithasbeenestimatedthattherearebetween250,000and350,000childrenof problemdrugusersintheUK(AdvisoryCouncilontheMisuseofDrugs2003) andathirdofadultsintreatmenthavechildcareresponsibilities(HMGovernment 2010b).TheGovernment’sdrugstrategyplacesaparticularfocusonthechildrenof parentswithdrugandalcoholproblems.Theneedtobeawareoftheharm,abuse andneglect,aswellastheinappropriatecaringroles,somechildrenmayexperience isstressed.Thestrategyisclearthat‘wherethereareconcernsaboutthesafetyand welfareofchildren,professionalsfrombothadultandchildren’sservices,alongside thevoluntarysector,shouldworktogethertoprotectchildren,inaccordancewiththe statutoryguidanceWorkingTogethertoSafeguardChildren(2010)’(HMGovernment 2010b,p.21).
Arangeofrelevantpracticeguidanceisavailabletolocalauthorities.Forexample, theDepartmentofHealthhasproducedguidancewhichfocusesonpeoplewith severementalhealthproblemsandproblematicsubstancemisuse.
Substancemisuseisusualratherthanexceptionalamongstpeoplewithsevere mentalhealthproblemsandtherelationshipbetweenthetwoiscomplex.
(DepartmentofHealth2002,p.4)
Theguidancesupportedjointworkingandimprovedcoordinatedcarebetween mentalhealthservicesandspecialistsubstancemisuseservices(Departmentof Health2002).
ModelsofCareforAlcoholMisusers(DepartmentofHealthandNational TreatmentAgencyforSubstanceMisuse2006)providedpracticeguidancefor localhealthorganisationsandtheirpartnersinthecommissioningandprovisionof assessments,interventionsandtreatmentofadultswhomisusealcohol.Theguidance acknowledgedtheimpactofparentalalcoholmisuseonchildren.Thisisclearly statedintheforewordbythethenchiefmedicalofficer,SirLiamDonaldson:
Thereisnodoubtthatalcoholmisuseisassociatedwithawiderangeofproblems, includingphysicalhealthproblemssuchascancerandheartdisease;offending behaviours,notleastdomesticviolence;suicideanddeliberateselfharm;child abuseandchildneglect;mentalhealthproblemswhichcoexistwithalcohol misuse;andsocialproblemssuchashomelessness.
However,therecommendationsrelatingtoscreeningandearlyassessmentsdid notincludethechildrenofparentswhomisusealcohol,althoughtheguidancedid recommendthatcomprehensiveriskassessmentsshouldbetargetedat,amongothers, userswithcomplexneedsincludingwomenwhoarepregnantorhavechildren‘at risk’.TheDepartmentofHealthhasrecentlytrialledarangeofalcoholscreening andbriefinterventionapproachestoevaluatetheirdelivery,effectivenessandcost effectiveness(ScreeningandInterventionProgrammeforSensibleDrinking(SIPS) seewww.hubcap.org.uk/F25W.)
Domesticviolence
TheGovernmentisalsoconcernedaboutviolenceagainstwomenandchildren andiscommittedtoimprovingthestandardsofcareandsupport.
Aswellasthegovernment’scommitmenttosupportexistingrapecrisiscentre provisiononastablebasisandtoestablishnewcentres,theHomeOfficehas allocatedaflatcashsettlementofover£28moverthenextfouryearsforworkto tackleviolenceagainstwomenandgirls.
(HMGovernment2010c,p.15,paragraph2.1)
TheDepartmentofHealth’sactionplanImprovingservicesforwomenandchild victimsofviolence(HMGovernment2010c,p.15,paragraph2.1)ispartofthe crossGovernmentapproachtotacklingsuchviolence.Theplanacknowledgesthat
‘violenceandabusecanalsobeariskfactorinfamilieswithmultipleproblems....the SpendingReviewmakesacommitmentforanationalcampaigntosupportandhelpturn aroundthelivesoffamilieswithmultipleproblems,improvingoutcomesandreducing coststowelfareandpublicservices’(p.10).
Withtheaimofimprovingtheresponsetothevictimsofviolence,theGovernment’s actionplanproposesto:
エ!
raiseawareness:amongsthealthprofessionaloftheirroleinaddressingthe issues,andthroughprovidingpatientswithinformationthathelpsthem accessrelevantservicesquicklyandsafely;
エ!
improvethecompetencyandskillsofNHSstaffthroughdevelopinga trainingmatrix;
エ!
improvethequalityofservicestovictimsofviolence;and
エ!
improvethedatacollectiononviolenceandsupporthealthprofessionalsto appropriatelyshareinformation.
FamilyLawAct1996andtheProtectionfromHarassmentAct1997.The2004 Actextendedthepowersofthecourtinprotectingthepartnersinarelationship. Furthermore,itcreatedanewcriminaloffenceof‘causingorallowingthedeathofa childorvulnerableadult’(Section4oftheDomesticViolence,CrimeandVictims Act2004).
Section24oftheCrimeandSecurityAct2010alsoseekstoprotectwomen andchildrenwhoarethevictimsofdomesticviolence.Seniorpoliceofficershave beengiventhepowertoissuedomesticviolenceprotectionnotices(DVPN).Such anoticecanbeusedtobanviolentmenfromthefamilyhome,initiallyfor24 hours,topreventwomenfromfutureviolenceorthethreatofviolence.Thesafety ofthechildmustalsobetakenintoconsideration.BeforeissuingaDVPNthe officermustconsider‘thewelfareofanypersonundertheageof18whoseintereststhe officerconsidersrelevanttotheissuingoftheDVPN(whetherornotthatpersonisan associatedperson)’(Section24(3)oftheCrimeandSecurityAct2010).Theissuing ofaDVPNtriggerstheapplicationtothemagistratescourtforadomesticviolence protectionorder.Thisisanorder,lastingbetween14and18days,whichprohibits theperpetratorfrommolestinghisvictim.
Thereisalsostatutoryandpracticeguidanceavailabletosupportprofessionalsin safeguardingwomenandchildrenfromdomesticviolence.Forexample,Working TogethertoSafeguardChildrenreinforcedtheroleofthepoliceinidentifyingand safeguardingchildrenlivingwithdomesticviolence;‘patrolofficersattendingdomestic violenceincidents,forexample,shouldbeawareoftheeffectofsuchviolenceonany childrennormallyresidentwithinthehousehold’(HMGovernment2010a,p.71, paragraph2.126).Toensurepoliceofficersworkinginchildprotectionatalllevels haveaccesstospecialisttrainingondomesticviolence,anupdatedtrainingmodule hasbeenmadeavailabletopoliceforcessinceDecember2009(Cm7589).
The2009HomeOfficeguidanceandpracticeadviceandWorkingTogetherto SafeguardChildren(HMGovernment2010a)bothadvocatetheuseofmulti agencyriskassessmentconferences(MARAC)asaprocessfor‘helpingtoaddress anissueofdomesticviolence;formanagingPPOs,includingthosewhoareproblematic drugusers;orforidentifyingchildrenatrisk’(HomeOffice2009a,p.1415,paragraph 2.3.3).(PPOsrefertoProlificandotherPriorityOffenders).MARACmeetingsare expectedtoinvolverepresentativesofkeystatutoryandvoluntaryagencies,who mightbeinvolvedinsupportingavictimofdomesticabuse.
Anotherexampleofmultiagencyworkingincasesofdomesticviolenceisthe SpecialistDomesticViolenceCourt(SDVC)programme.Thesespecialcourts, withintheCriminalJusticeSystem,bringtogetherasimilarrangeofbodiesto MARAC.
Agenciesworktogethertoidentify,trackandriskassessdomesticviolencecases, supportvictimsofdomesticviolenceandshareinformationbettersothatmore offendersarebroughttojustice.
Limitations of the research drawn on in this
publication
Differentlawsandcultures
Muchoftheresearchonmentalillness,learningdisability,domesticviolenceand substancemisusecomesfromtheUS,whichhasdifferentlaws,traditions,andsocial institutionsfromtheUnitedKingdom.Forexample,amajordifferencewhich existsinrelationtosubstancemisuseisthecommitmenttoharmminimisation intheUnitedKingdom.ThisapproachisnotuniversallysharedintheUS,which hasfollowedanabstinenceonlypolicyforthelast30years.Asaresultthereare uniqueservicesintheUnitedKingdom,suchasconsistentlyavailablemethadone treatmentandneedleandsyringeexchangeschemesforproblemdrugusers,and controlleddrinkingprogrammesforproblemalcoholusers.IntheUS,abstinence basedprogrammes,especiallyinalcoholservices,aremoreavailablethancontrolled drinking,andmethadonemaintenanceprogrammesaremorerestrictiveintheUS comparedtotheUnitedKingdom.Thishasimplicationsforservicesforwomenin theUS,wheremanytreatmentprogrammesforpregnantdrugandalcoholusers requirewomentobeabstinentinordertotakepartintheprogramme.Inmany Americanstates,pregnantmotherswhousedrugsoralcoholriskprisonsentences whilepregnantonthegroundsofphysicalchildabuse.
Focusingonaspecificissue
Mostresearchiscentredonaspecificissuesuchasdomesticviolence,depression, learningdisabilityorheroinuse.However,inpractice,manyproblemdruguserswill useavarietyofdrugsandalcohol(polydruguse).Similarly,manyofthoseexperiencing domesticviolencealsosufferdepressionandmayusealcoholordrugsasawayof coping;orthosewhoareperpetratingtheviolencemaybeundertheinfluenceof alcoholordrugs.Moreover,alearningdisabilitydoesnotinureanindividualto drugmisuse,domesticviolenceormentalillness.Inthispublication,althougheach issueistakenindividuallywhendescribingthepsychologicalandphysicalsymptoms, whendiscussingthefindingsfromresearchinrelationtotheimpactonparenting capacityamorepragmaticandinclusiveapproachhasbeentaken.
Timelimitedresearch
Samplingbias
Thesamplesusedinmanyresearchstudiesaretakenfromspecificgroupssuch asparentalcocaineoralcoholusersintreatment,mentallyillparentsinhospital, parentsinreceiptofservicesforlearningdisability,ormothersinrefuges.Farlessis knownaboutparentsinthegeneralpopulationwhoexperiencetheseproblemsbut donotseekhelp;itwouldbedangeroustoassumethatthepopulationsstudiedare representative.
Researchontheimpactofparentalproblemsonchildrentendstobebiased towardswomenascarers.Therearemorestudiesonmaternalparentingcapacity thanpaternalcapacity,andoftentheinfluenceofotherfamilyfactors,suchas theroleofgrandparentsorsiblings,ortheimpactofdivorceorseparation,isnot considered.
Manyofthestudiesfocusonspecificproblems,suchaschildren’sdrugandalcohol use,violence,mentalhealth,education,offendingandbehaviouralproblems,rather thanamoreholisticapproachortheidentificationofsignsofresilienceorcoping strategies.
Itisoftennotpossibletoaccuratelymeasurethequantitiesofdrugsandalcohol beingusedbyparents,thedegreeofviolenceexperienced,ortheextentofmental illnessorlearningdisability.Forexample,someparentsmayfeelthreatenedby serviceswhichcantakeactiononthecareoftheirchildrenandunderestimate theirdifficulties.Inothersituationsparentsmayoverestimatetheirproblems.For example,drugusemaybeexaggeratedandpresentedasmitigatingcircumstancesin criminalcourtcasesorinanattempttomaximiseamethadoneprescription.
Afurtherlimitationoftheresearchisthedependenceonclientrecall.Drugs andalcohol,domesticviolence,mentalillnessandlearningdisabilitiesalladversely affectthecapacitytoremember,andmanystudiesrelynotonlyonrecentmemory butmemoryovermanymonthsoryears.Itisquestionablehowaccuratethese measurementsare.Finally,itisessentialtorememberthatthemajorityofparents whoexperiencetheseissues,especiallythosewhopresentforservices,areusually alsosufferingfrommultipleformsofdeprivationandsocialexclusion.Thesefactors shouldnotbeunderestimatedintheirneteffectonparentingcapacity.
CHILD’S DE VEL
OPMENT AL NEEDS
PARENTING CAP
ACIT
Y CHILD
Safeguarding & promoting
welfare
Health BasicCare
EnsuringSafety
EmotionalWarmth
Stimulation Education
BehaviouralDevelopment
FAMILY & ENVIRONMENTAL FACTORS
Emotional&
Identity
Family&Social Guidance&
Relationships Boundaries
SocialPresentation
Stability
SelfcareSkills
Community R
esour
ces
Family
’sS ocial Integration Income
Emplo
yment H
ousing WiderF
amily FamilyH
istor y &F
unctioning
Structure of the book
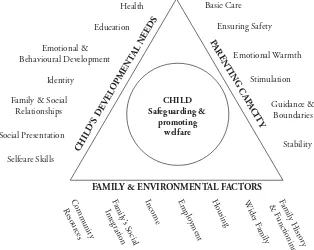
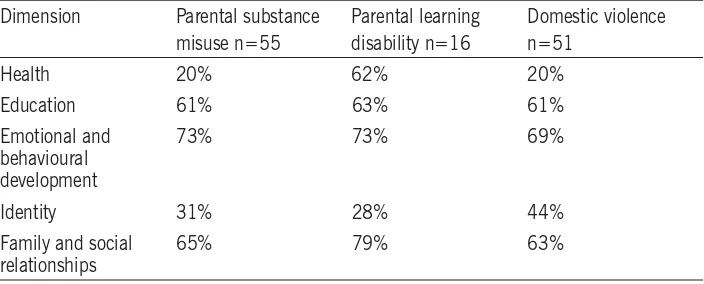
Inconsideringhowparentalmentalillness,learningdisability,problemdrinking, drugmisuseordomesticviolencemayaffectthechild,aholisticanddevelopmental modelisapplied.Researchfindingsaredisaggregatedthroughapplyingthe conceptualframeworkdesignedtoassessandmeasureoutcomesforchildreninneed (DepartmentofHealthetal2000).Thethreedomainsofthechild’sdevelopmental needs,parentingcapacityandfamilyandenvironmentalfactorsconstitutethe framework.Thethreeinterrelateddomainsincorporateanumberofimportant dimensions(seeFigure1.1).
Figure1.1�eAssessmentFramework
particularemphasisonhowparentalmentalillness,learningdisabilities,substance misuseanddomesticviolencehaveanimpactonchildren’shealthanddevelopment, andwhetherthereisevidencethatchildrenaresuffering,orlikelytosuffer,significant harm.Becausetheimpactonthechildwilldependonavarietyoffactorsincluding ageanddevelopmentalstage,theagebandsfirstusedintheIntegratedChildren’s System(DepartmentforChildren,SchoolsandFamilies2010)havebeenapplied. Forexample,withregardtotheeducationaldevelopmentofchildrenaged3–4years, itisimportanttoidentifywhenparents’problemssubstantiallyrestrictthechild’s accesstostimulatingtoysandbooks,orpreventparentsspendingsufficienttime talking,readingorplayingwiththeirchildren.Alternatively,assessingtheimpactof thesesameparentalissuesontheeducationofadolescentsaged11–15yearsneeds tofocusondifferentthemes–forexample,schoolattendanceandinvolvementin otherlearningactivitiessuchassport,musicorhobbies.
Withineachdimensionandforeachagegroup,evidenceisusedtohighlight boththeadverseimpactonchildrenandthefactorswhichactasprotectors,suchas thestrategieschildrenusetocopewithstressfulfamilysituationsandthesupport andinfluenceofthewiderfamilyandcommunity.
Thebookisdividedintothreeparts,PartsI,IIandIII.
Part IincludesChapters1–3andexploresthefollowinggeneralissues:
Chapter 1:questionswhetherconcernisjustified,andexplorestheproblemsof definitionandprevalence.
Chapter 2:exploresthewaysinwhichmentalillness,learningdisability,problem druguse(includingalcohol)anddomesticviolenceaffectparentingcapacity. Chapter 3:identifieswhichchildrenaremostvulnerable.
Part IIincludesChapters4–6,withaspecificfocusonchildrenofdifferentages andstagesofdevelopment:
Chapter 4:discussestheimpactofparentalproblemsforchildrenunder5 years.
Chapter 5:focusesontheissuesforchildrenaged5to10years. Chapter 6:focusesonyoungpeopleaged11yearsandover.
Part IIIincludesChapters7and8whichdrawtogetherthefindingsand implicationforpolicyandpractice:
Chapter 7:discussestheconclusionsfromthestudy.
1
definition and prevalence
Tounderstandwhetherthepresentconcernsoverparentalmentalillness,learning disability,problemalcoholanddruguseordomesticviolencearejustified,this chapterexaminestheproblemswithterminologyandtheprevalenceoftheseissues. Generalpopulationstudiesprovideevidenceoftheirprevalenceandtherelevance ofgender,cultureandclass.Findingsfromchildprotectionresearchareusedto identifyassociationsbetweentheseparentalproblemsandchildren’shealthand development,includingtheextenttowhichtheymayposeariskofsignificant harmtothechild.
Problems with terminology
Understandingthedegreeoftheseparentalproblemsisdifficultbecausedifferent researchstudiesusedifferenttermsandtherearefewdefinitionsprovided. Forexample,intheDepartmentofHealth’s1995studiesonchildprotection (DepartmentofHealth1995a)itisunclearwhetherSharlandetal.’s(1996)parents whohave‘relationshipproblems’areasimilargrouptoThoburnetal.’s(1995) parentswhoarein‘maritalconflict’,orFarmerandOwen’s(1995)familieswhoare experiencing‘domesticviolence’.Difficultiesalsoarisebecause,forexample,different countriesusedifferentwaysofmeasuringdrugandalcoholuse.Forinstance,the ‘unitofalcohol’intheUnitedKingdomhaslittlemeaningintheUSwheredifferent measuresofalcoholareusedinpeerreviewedjournalsandresearch.Inaddition,the purityofdrugsusedindifferentcountriesmaydiffer.Forexample,agramofheroin inNewYorkmaybemoreorlesspurethanagramofheroininLondon.
Whenscrutinisingtheliteratureonmentalillness,learningdisability,problem alcoholanddruguse,anddomesticviolencetheauthorshavebeenguidedintheuse oftermsbythefollowingpolicyandpracticedocuments.
Mentalillness
ClinicalstudiesofadultsgenerallydefinementalillnesseitherbyusingtheEuropean system:TheICD10ClassificationofMentalIllnessandBehaviouralDisorders(World HealthOrganisation1992)ortheUSclassification:DiagnosticandStatistical ManualofMentalDisorders(AmericanPsychiatricAssociation2000).Unfortunately, thequalityofinformationfromcommunitybasedrecordsmayprecludesuch aprecisediagnosis.Inaddition,therecontinuestobeconsiderabledisputeover whether‘personalitydisorder’isapsychiatricillnessassuchormerelyadescription ofextremesofnormalvariation(seeKendell2002foradiscussionofthisissue). Moreover,because‘personalitydysfunctionhasbeenrepeatedlydescribedinanecdotal casereports,clinicalstudiesandsurveysoftheparentsofmaltreatedchildren’(Falkov 1997,p.42)itwasthoughtthattoomititinastudyoftheimpactonchildrenof parentalproblemswouldberemiss.Insomeways,therecentamendmentstothe MentalHealthAct2007simplifytheissueinclinicaltermswiththeuseofanew expression–‘mentaldisorder’–whichisdefinedas‘anydisorderordisabilityof themind’butexcludesbothalcoholanddrugdependenceand‘learningdisabilities unlesswithabnormallyaggressiveorseriouslyirresponsiblebehaviour’.
Learningdisability
TheDepartmentofHealth’sdefinitionoflearningdisabilityencompassespeople withabroadrangeofdisabilities.Learningdisabilityincludesthepresenceof:
エ!
asignificantlyreducedabilitytounderstandneworcomplexinformation,to learnnewskills(impairedintelligence);withエ!
areducedabilitytocopeindependently(impairedsocialfunctioning);エ!
whichstartedbeforeadulthood,withalastingeffectondevelopment.(HMGovernment2010a,p.279,paragraph9.56) Mencapalsoprovidesacleardescriptionoflearningdisability.
Alearningdisabilityiscausedbythewaythebraindevelops.Therearemany differenttypesandmostdevelopbeforeababyisborn,duringbirthorbecauseof aseriousillnessinearlychildhood.Alearningdisabilitycanbemild,moderate, severeorprofound,butallarelifelong.Manypeoplewithalearningdisability, however,liveindependentlives.
birth,braininjuryatbirth,braininfectionsorbraindamageafterbirth.Examples includeDown’ssyndrome,FragileXsyndromeandcerebralpalsy(RoyalCollegeof Psychiatrists2004a).
Problemdrinking
TheNationalInstituteforHealthandClinicalExcellence(2010)intheirpublic healthguidanceonalcoholusedisordersprovidesthefollowingdefinitions: Hazardous drinking Apatternofalcoholconsumptionthatincreasessomeone’s riskofharm.
Harmful drinking Apatternofalcoholconsumptionthatiscausingmentalor physicaldamage.
Higher-risk drinking Regularlyconsumingover50alcoholunitsperweek(adult men)orover35unitsperweek(adultwomen).
IntheUnitedKingdomoneunitisequivalenttohalfapintofordinarystrength lagerorbeeroroneshot(25ml)ofspirits,whileasmall(125ml)glassofwineis equalto1.5units.Theunitmeasurehaslostsomeofitsvalueandsimplicitybecause fewpubsorrestaurantsserve125mlglassesofwine(theyarenoweither175ml or250ml).Also,whentheunitwasdevisedwinewascalculatedashavingon average9%alcohol,whilemostwinesthesedaysare12–15%.Similarly,thealcohol contentofmanybeersandlagersisnowmorethanitwaswhentheunitsystem wasestablished.Previously,thealcoholcontentofbeerandlagerwasestimatedat 3.5–4.0%.Nowmostbeersarestronger,3.5–9.0%,withmanypopularbeersat5%. Thepub‘measure’ofspiritshas,insomepubs,beenreplacedbya35mlmeasure. Recently,thenumberofunitsofalcoholinabottleofwinehasbeenprintedonthe label.
TheGovernmentstrategyforpublichealth(Cm79852010)acknowledgesthe deleteriousimpactofheavydrinkingonhealthandthenegativeeffectonothers.
‘Drunkennessisassociatedwithalmosthalfofassaultandmorethanaquarterofdomestic violenceincidents’(p.20,paragraph1.31).
Problemdruguse
Researchintoproblemdruguseemploysabewilderingrangeoftermsinits descriptionsincludingdruguse,drugmisuse,drugdependence,addiction,drug abuseandproblemdruguse.Thesetermsarenotalwaysdefined,whichmakesit difficulttocomparethefindingsfromonestudywithanother.Forinstance,someone canbeaproblemdruguser(havingproblemsasaresultofdruguse)butnotsuffer fromaddiction(suggestingphysicalandpsychologicaldependence).
Byproblemdrugusewemeandrugusewithseriousnegativeconsequencesof aphysical,psychological,socialandinterpersonal,financialorlegalnaturefor usersandthosearoundthem.Suchdrugusewillusuallybeheavy,withfeatures ofdependence.
(AdvisoryCouncilontheMisuseofDrugs2003,p.7)
Domesticviolence
Whenconsideringdomesticviolence,the2009definitionusedbytheHomeOffice wasfoundtobehelpful.
Domesticviolenceis‘Anyincidentofthreateningbehaviour,violenceorabuse (psychological,physical,sexual,financialoremotional)betweenadultswhoareor havebeenintimatepartnersorfamilymembers,regardlessofgenderorsexuality.’ Thisincludesissuesofconcerntoblackandminorityethnic(BME)communities suchassocalled‘honourbasedviolence’,femalegenitalmutilation(FGM)and forcedmarriage.
(HomeOffice2009b)
Thisdefinitionofdomesticviolencedoesnotconfineitselftophysicalorsexual assaultsbutincludesarangeofabusivebehaviourswhicharenotinthemselves inherentlyviolent.Asaconsequence,someauthorsprefertousetheterm‘domestic abuse’.Itshouldalsobenotedthatdomesticviolencerecognisesfewsocial boundaries.Forexample,researchonfemalevictimsofdomesticviolencereports that‘violenceagainstwomenisthemostdemocraticofallcrimes,itcrossesallreligious, classandracebarriers’(Women’sAid1995).
Childabuseandneglect
Childabuseandneglectareformsofchildmaltreatmentandresultfromanyone (butmorecommonlyaparentorcarer)inflictingharmorfailingtoacttoprevent harm.Statutoryguidanceprovidesthefollowingdescriptionsofabuseandneglect.
Physicalabusemayinvolvehitting,shaking,throwing,poisoning,burningor scalding,drowning,suffocating,orotherwisecausingphysicalharmtoachild. Physicalharmmayalsobecausedwhenaparentorcarerfabricatesthesymptoms of,ordeliberatelyinduces,illnessinachild.
overprotectionandlimitationofexplorationandlearning,orpreventingthechild participatinginnormalsocialinteraction.Itmayinvolveseeingorhearingtheill treatmentofanother.Itmayinvolveseriousbullying(includingcyberbullying), causingchildrenfrequentlytofeelfrightenedorindanger,ortheexploitationor corruptionofchildren.Somelevelofemotionalabuseisinvolvedinalltypesof maltreatmentofachild,thoughitmayoccuralone.
Sexualabuseinvolvesforcingorenticingachildoryoungpersontotakepart insexualactivities,notnecessarilyinvolvingahighlevelofviolence,whetheror notthechildisawareofwhatishappening.Theactivitiesmayinvolvephysical contact,includingassaultbypenetration(forexample,rapeororalsex)ornon penetrativeactssuchasmasturbation,kissing,rubbingandtouchingoutsideof clothing.Theymayalsoincludenoncontactactivities,suchasinvolvingchildren inlookingat,orintheproductionof,sexualimages,watchingsexualactivities, encouragingchildrentobehaveinsexuallyinappropriateways,orgroominga childinpreparationforabuse(includingviatheinternet).Sexualabuseisnot solelyperpetratedbyadultmales.Womencanalsocommitactsofsexualabuse,as canotherchildren.
Neglectisthepersistentfailuretomeetachild’sbasicphysicaland/orpsychological needs,likelytoresultintheseriousimpairmentofthechild’shealthordevelopment. Neglectmayoccurduringpregnancyasaresultofmaternalsubstanceabuse.Once achildisborn,neglectmayinvolveaparentorcarerfailingto:
エ!
Provideadequatefood,clothingandshelter(includingexclusionfromhome orabandonment);
エ!
Protectachildfromphysicalandemotionalharmordanger;
エ!
Ensureadequatesupervision(includingtheuseofinadequatecaregivers); or
エ!
Ensureaccesstoappropriatemedicalcareortreatment.
エ!
Itmayalsoincludeneglectof,orunresponsivenessto,achild’sbasicemotional needs.
(HMGovernment2010a,p.3839,paragraphs1.331.36)
Prevalence
relationshipbetweenintelligence–untilitfallsbelowacertainlevel,usuallytaken tobeanIQof60orless–andparenting(BoothandBooth2004;Tymchuck1992). Itistheextremityorcombinationofthesesituations,particularlytheassociation withviolence,whichmayimpairparents’capacitytomeettheirchildren’sneeds and,insomesituations,resultinchildabuseandneglect.
Unfortunately,theabilitytoaccuratelygaugetheextentofparentalmentalillness, learningdisability,problemalcoholordruguse,anddomesticviolenceishampered notonlybyproblemsofterminologybutalsobecauseprevalencedependsupon thepopulationgroupbeingstudied.Forexample,communitybasedsamplessuch asthehouseholdsurveycarriedoutbytheOfficeforNationalStatisticswillbe morerepresentativethanresearchwhichfocusesonspecificgroups,suchashospital patients,womenandchildreninrefuges,orthosewhoattendclinicsorcourts. Moreover,theseverityoftheconditionunderstudyislikelytobemuchgreaterin specificsamplegroupsasisthecoexistenceofavarietyofadditionalproblems.But regardlessofthetypeofsamplegroupunderconsideration,anygeneralisationsto samplesbeyondthatbeingstudiedshouldbemadewithconsiderablecaution.
Thefollowingsectionsexplore,inturn,theexistingevidenceontheprevalence of:
エ!
parentalmentalillnessエ!
learningdisabilityエ!
problemdrinkinganddruguseエ!
domesticviolence.Twosourcesareexaminedforeachcategory:
エ!
generalpopulationstudiesエ!
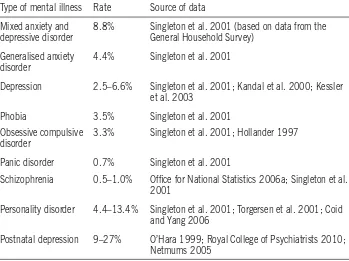
childprotectionresearch.Prevalence of parental mental illness: general
population studies
Type of mental illness Rate Source of data Mixed anxiety and
depressive disorder
8.8% Singleton et al. 2001 (based on data from the General Household Survey)
Generalised anxiety disorder
4.4% Singleton et al. 2001
Depression 2.5–6.6% Singleton et al. 2001; Kandal et al. 2000; Kessler et al. 2003
Phobia 3.5% Singleton et al. 2001 Obsessive compulsive
disorder
3.3% Singleton et al. 2001; Hollander 1997
Panic disorder 0.7% Singleton et al. 2001
Schizophrenia 0.5–1.0% Office for National Statistics 2006a; Singleton et al. 2001
Personality disorder 4.4–13.4% Singleton et al. 2001; Torgersen et al. 2001; Coid and Yang 2006
Postnatal depression 9–27% O’Hara 1999; Royal College of Psychiatrists 2010; Netmums 2005
Itisencouragingtonotethattheproportionofpeoplereceivingtreatmentfor mentalhealthdifficultieshasincreasedfrom14%in1993to24%in2000.In themainthiswastheresultofadoublingintheproportionofthosereceiving medication,whereasaccesstopsychologicaltreatmenthasremainedconstant(Office forNationalStatistics2005).
Thepictureiscomplicatedbecausementalillnessfrequentlyexistsalongsideother disorders.Forexample,USresearchindicatesthathalfofthosewithadiagnosis ofschizophrenia(Swoffordetal.2000)andnearlyathirdofthosewithamood disorderalsomisusedorweredependentuponalcoholordrugs(Regieretal.1990). TheworkofRosenthalandWestreich(1999)intheUSalsosuggeststhathalfof individualswhoexperiencealcoholordrugproblemsormentalhealthdisorders willhavetwoormoreofthesedisordersovertheirlifetime.WorkintheUnited Kingdomwhichfocusedonthoseattendingmentalhealthservicesfound44%of patientsselfreportedproblemuseofdrugsand/orwereassessedtohaveusedalcohol athazardousorharmfullevelsinthepreviousyear(Weaveretal.2002).
thedatabythetypeoffamilyunit,showedpsychiatricmorbiditytobeassociated withfamilycharacteristics.Coupleslivingwithchildrenhaveagreatermorbidity forbothneuroticdisorder(155perthousand)andfunctionalpsychoses(4per thousand)thancoupleswithoutchildren(134perthousandforneuroticdisorder andtwoperthousandforfunctionalpsychoses).Thedataalsoshowahigherrateof mentalillnessforloneparentsthanforadultslivingasacouplewithchildren(see Table1.2).Thesefindingssuggestthatchildrenmaybemorevulnerabletoharm andneglectwhenlivingwithaloneparentwhosuffersfrommentalillness,because whentheparentisexperiencingthedisorderthereislikelytobenoothercaring adultlivinginthehometotakeontheparentingrole.
Table 1.2: Prevalenceofmentalillnessamongparentsinthegeneralpopulation
Type of mental illness Couple and child(ren) Lone parent and child(ren) Neurotic disorders 15.5% 28%
Functional psychoses 0.4% 1.1%
Parentalmentalillness:issuesofgender,
cultureandclass
Researchonfathersormalecarerswithmentalhealthproblemsissparse.What isclearisthatmenwholiveeitherasacouplewithchildrenorinaloneparent situationhavealowerrateofneuroticdisorderandfunctionalpsychosesthando womeninsimilarsituations(Singletonetal.2001;CoidandYang2006).
Incontrast,thereisaconsiderablebodyofworkwhichrecordstherateofmental illnessinmothers.Somewhatsurprisingisthattheprevalenceofmaternalmental illnessappearstovaryfromcountrytocountry.Forexample,anAmericanstudy suggestsasmanyas25–39%ofwomensufferdepressionfollowingchildbirth (CentreforDiseaseControlandPrevention2004),whereasBritishstudieshave traditionallyplacedthefigureataround10%(O’HaraandSwain1996).However, amorerecentonlinesurveysuggestsdepressionfollowingchildbirthhasincreased significantlyoverthepast50yearsinBritain,upfrom8%inthe1950sto27% today(Netmums2005).Onemightquestionwhetherthevarianceinreported ratesofmentalillnessisduetorealdifferencesinprevalence,inhowmentalillness manifestsitself,orinthemethodsofassessmentandrecording.Forexample,the USstudy(CentreforDiseaseControlandPrevention2004)of453,186women recordeddepressionintermsofitsseverityandfound7.1%ofmothersreported experiencingseveredepression,andjustmorethanhalfreportedexperiencinglow tomoderatedepressionfollowingchildbirth.
qualificationsandtocomefromsocialclassV(unskilled,manualoccupations)and beeconomicallyinactive.Adultswithmentalhealthproblemshavethehighest unemploymentratesforanyofthemaingroupsofdisabledpeople;only21%are employed(OfficeforNationalStatistics2006b).Theimpactofclassandpovertyare exacerbatedwhenadultsareparentscaringforchildren.‘...amongthosewithchildren athome,workingclasswomenwerefourtimesmorelikelytosufferfromadefinite psychiatricdisorder’thancomparablemiddleclasswomen(BrownandHarris1978, p.278).
Vulnerabilitytomentaldisordersmaybetheresultofadverselifeeventssuchas poverty,poorenvironment,sexismorracismandotherformsofsocialdisadvantage (CentreforDiseaseControlandPrevention2004;GhateandHazel2002;Propper etal.2004).Forexample,researchbasedin15electoralwardsinLondonfoundthe incidenceofschizophreniainnonwhiteminoritieswasrelatedtotheproportion oftheethnicminoritylivinginthearea;thesmallertheminoritygroupthegreater theincidenceofschizophrenia(Boydelletal.2001).Ofsignificanceareindividual experiences,particularlythoseinvolvinglongtermthreat(BrownandHarris1978; Sheppard1993).
Thepictureisfurthercloudedbecausementalillnessisperceiveddifferently bydifferentculturalgroups(NSPCC1997a;Anglinetal2006).Forexample, theliteratureseemstosuggestthatinsomesouthAsianculturesmentalillnessis expressedintermsofphysiologicalailments.Asaresult,symptomsmaybereported asproblemsrequiringmedicalratherthanpsychiatricservices.Likewise,insome culturesoutsidetheWesternworldschizophreniaisinterpretedasapossessionof thesuffererbymalevolentspirits,andtheservicesofpriestsratherthandoctorsare sought(LittlewoodandLipsedge1997).
Thiscumulativebodyofevidence,althoughillustratingsomeofthedifficulties inassessingprevalence,suggeststhataconsiderablenumberofchildrenarelivingin familieswhereatleastoneparentissufferingfromamentalillness.
Prevalenceofparentalmentalillness:
childprotectionstudies
Themajorityofparentswhoexperiencementalillnessdonotneglectorharmtheir childrensimplyasaconsequenceofthedisorder(Tunnard2004).Childrenbecome morevulnerabletoabuseandneglectwhenparentalmentalillnesscoexistswith otherproblemssuchassubstancemisuse,domesticviolenceorchildhoodabuse (Cleaveretal.2007).
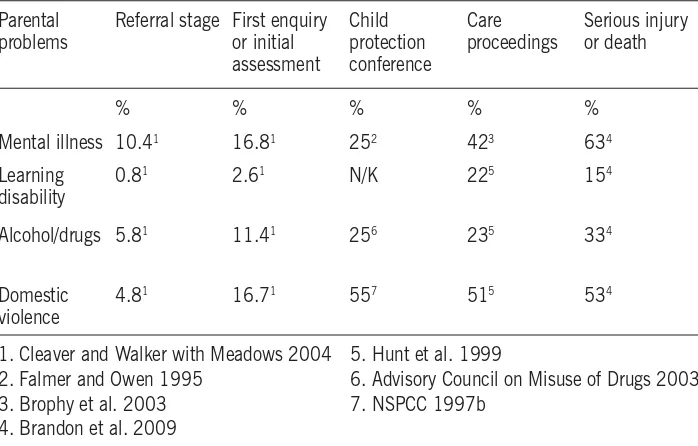
WalkerwithMeadows’(2004)studyof2,248referralstochildren’ssocialcarefound, onreanalysingtheirdata,thatparentalmentalillnesswasrecordedin10.4%of referrals,afindingsimilartothe13%identifiedbyGibbonsetal.(1995).However, prevalenceincreaseswithgreaterknowledgeofthefamilycircumstances.Following aninitialassessment,socialworkersrecordedparentalmentalillnessin16.9%of cases(CleaverandWalkerwithMeadows2004).Whencasescomeundergreater scrutinyandachildprotectionconferenceisheld,prevalenceincreasesonceagain. Parentalmentalillnesswasidentifiedinaquarterofcasescomingtoconference (FarmerandOwen1995).Thereisafurtherriseinprevalenceforchildreninvolved incareproceedings.Parentalmentalillnesshadbeennotedinsome43%ofcases wherechildrenarethesubjectofcareproceedings(42%inHuntetal.1999;and 43%inBrophyetal.2003).
Earlyresearchonchildmurderrecordedparticularlyhighratesofmaternalmental illness.Resnich’s(1969)reviewof131casesofparentalchildmurderidentified71% ofmothersasbeingdepressedandGibson’s(1975)studyofmaternalfilicidenoted 90%ofthemothershadapsychiatricdisorder.Morerecentresearchintoextreme casesofchildabusetempersthesefindings,althoughthereremainsconsiderable variation.Falkov’s(1996)studyoffatalchildabusefound32%ofparentshada psychiatricdisorder,afindingsimilartotherate(28%)identifiedinfamiliessubject toseriouscasereviewsduring2007–8(Ofstedetal.2008).However,thisislikelyto beanunderestimate.Theanalysisofanintensivesampleof40seriouscasereviews foundalmosttwothirds(63%)ofchildrenlivedinahouseholdwithaparentor carerwithcurrentorpastmentalillness(Brandonetal.2009and2010),afigure ratherhigherthanthe43%foundinRederandDuncan’s1999studyoffatalchild abuse.
Thefocusonmothers,commoninmuchofthechildprotectionresearch,might suggestthattheyaremorepronetokillingtheirchildren.However,filicideisnot theprerogativeofmothers.Exceptforneonates,fathersandfatherfiguresaremore likelytomurderachildintheircarethanaremothers(MarksandKumar1996; Stroud1997;Cavanaghetal.2007).
Fatheradmittedshakingthebaby...Bothparentshaveahistoryofmentalillness. Littleknownaboutfamily,buttheyhavehadfrequenthousemovesandchanges ofname.
(Brandonetal.2008,p.46)
Parentalmentalillnessandtypeofchildabuse
parentalmentalillnesswasrecordedin31%ofcases(GlaserandPrior1997). Researchonchildsexualabusealsosuggestsagreaterassociationwithparental mentalillness.Sharlandandcolleagues’(1996)studyofchildsexualabusefound 71%offamilies,wherethereweresuspicionsofabuse,wereina‘poorpsychological state’usingtheGeneralHealthQuestionnaire(GoldbergandWilliams1988)and therewasafurtherincreasewhensuspicionswereconfirmed.Thesefindingsarein linewithMoncketal.’s(1995)studyoffamiliesattendingaspecialisedtreatmentand assessmentdayclinicforchildsexualabuse.Theyfound86%ofmothers(assessed usingtheGeneralHealthQuestionnaire)showedsymptomsofdepressionoranxiety and,foraconsiderableproportion,thesymptomshadbeenoflongduration.
Caution,however,mustbeexercisedinrelationtothesefindingsbecausestudies ofphysicalabuseandneglecthavetendednottousestandardisedmeasuresofmental healthanditisnotpossibletocomparelikewithlike.
Prevalence of parental learning disability:
general population studies
Theprevalenceoflearningdisabilityamongthegeneralpopulationisdifficultto establishbecausenoinformationiskeptnationally.EmersonandHatton(2008), usingdatafrom24localauthoritiesestimatedthattherewere985,000peoplein Englandwithalearningdisability,equivalenttoanoverallprevalencerateof2%of theadultpopulation.
However,McGawandNewman(2005)raiseanoteofcaution,pointingout howdifferencesinclassificationresultinconfusionandinconsistency.Traditionally, scoresonstandardisedintelligencetestshavebeenusedtodefinelearningdisability; approximatelytwothirdsofpeople(69%)fallwithinthenormalrangeof85to115 (averageIQbeing100).Individualswhoseresultsaretwostandarddeviationsbelow themean,i.e.anIQof70orbelow,areclassifiedas‘learningdisabled’(Dowdney andSkuse1993).Onedifficultyinestablishingtheprevalenceoflearningdisability relatestohowthosewithborderlineIQs(70to85)areclassified.Inaddition, individualsmayexhibitdifferentabilitylevelsacrossthecomponentsofIQand othertestsused.‘...inrealitythereisnocleardemarcationbetweenparentswhohave learningdisabilitiesandthosewhodonot’(McGawandNewman2005,p.8).
parentswithlearningdisabilitiesincontactwithservices’(DepartmentofHealthand DepartmentforEducationandSkills2007,p.36).
Peoplewithalearningdisabilityhavegreaterphysicalandmentalhealthneeds andaremorelikelytohaveexperiencedchildhoodabuseorneglectthantherestof thepopulation(McGawetal.2007).Forexample,intheUnitedKingdomresearch indicates25–40%ofadultswithalearningdisabilitywillexperienceamentalhealth problematsomepointintheirlives(MIND2007).Inparticular,ratesofschizophrenia arethreetimeshigherthaninthegeneralpopulation,althoughtherearefewdataon theprevalenceofothertypesofmentalillness(Hassiotisetal.2000).
Parentallearningdisability:issuesofgender,culture
andclass
Mostreportsandstudiesinvolvingpeoplewithlearningdisabilitiesdonot differentiatebetweenmenandwomen.AsMcCarthy(1999)explains‘Itisasif havingalearningdisabilityoverridesallotheridentitiesanditis,somewhatbizarrely,as ifitispoliticallyincorrecttodrawattentiontogenderdifferences.’Literaturethatdoes differentiatebetweenmenandwomenwithlearningdisabilitiestendstofocuson sexualityandsexualabuse.Studiesfocusingonmenwithalearningdisabilityare almostexclusivelyabouttheirsexualbehaviour,andthosewhichfocusonwomen highlighttheirsexualvulnerability(McCarthy1999).
Incontrast,muchresearchhasdrawnattentiontothevulnerabilityoffamilies whereoneormoreparenthasalearningdisability.Parentswithlearningdisabilities havebeenfoundtobeamongstthemostsociallyandeconomicallydisadvantaged groups.Thefinancialdifficultiesfacedbythesefamiliesareillustratedinthefigures drawntogetherbyMencap.Thedatashowthatlessthanoneinfivepeoplewith learningdisabilitiesareinwork(comparedwithoneintwodisabledpeoplegenerally) andthatthosewhoareworkingaremostlyonlyworkingparttimeandarelow paid.Justoneinthreepeoplewithlearningdisabilitiestakepartinsomeformof educationortraining(Mencap2008).
Prevalenceofparentallearningdisability:child
protectionstudies
disability.Parentallearningdisabilityisfrequentlyidentifiedasoneofthemany cocurrentproblemsthatimpactonparents’capacitytosafeguardandpromotethe welfareoftheirchildren(CleaverandFreeman1995;CleaverandNicholson2007). Finally,inanintensivestudyof40seriouscasereviews15%ofchildrenwereliving withaparentwithalearningdisability(Brandonetal.2009).
Areviewofresearchsuggeststhatbetween40%and60%ofparentswithlearning disabilitieshavetheirchildrentakenintocareasaresultofcourtproceedings (McConnellandLlewellyn2002).Amorerecentsurveyof2,893peoplewith learningdisabilitiesinEnglandfoundofthosewhowereparents,justunderhalf (48%)werenotlookingaftertheirchildren(Emersonetal.2005).However, thisfigureincludedchildrenwhohadlefthomebecausetheyhadgrownupand, therefore,itmustnotbeassumedthat48%ofparentswithalearningdisabilityhad hadtheirchildrentakenintocare.Thesefigurescontrastgreatlywiththefindings fromanindepthfollowupstudyof64casesreferredtochildren’ssocialcarewhere oneorbothparentshadalearningdisability(CleaverandNicholson2007).In thisstudymostchildrencontinuedtolivewiththeirparentsfollowingareferralto children’ssocialcare.Threeyearsaftertheinitialreferralonly12children(18.8%) hadbeenremovedfromtheirparents’care,includingtwochildrenwhohadbeen placedforadoption.
Parentallearningdisabilityandtypeofchildabuse
Learningdisabilityisnotcorrelatedwithdeliberateabuseofchildren‘...IQbyitself, isnotapredictoreitheroftheoccurrenceorofthenonoccurrenceofpurposefulchild abuse...’(Tymchuck1992,p.169).Infact,thereisconsiderableevidencetoshow thatanaccumulationofthestressorsrelevanttoallparentsaremorepredictive ofpoorparentingthanIQscores.Theseinclude,forexample,poverty,inadequate housing,maritaldisharmonyandviolence,poormentalhealth,childhoodabuse, substancemisuseandalackofsocialsupports(Craft1993;BoothandBooth 1996;CleaverandNicholson2007).Inaddition,parentsmayhavethechallenge ofcaringforadisabledchild.Childrenborntoparentswithalearningdisability areatincreasedriskofinheritedlearningdisabilitiesandpsychologicalandphysical disorders(McGawandNewman2005).