© World Health Organization 2 0 0 4
All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 2 0 Avenue Appia, 1 2 1 1 Geneva 2 7 , Switzerland (tel: + 4 1 2 2 7 9 1 2 4 7 6 ; fax: + 4 1 2 2 7 9 1 4 8 5 7 ; email: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to Publications, at the above address (fax: + 4 1 2 2 7 9 1 4 8 0 6 ; email: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
Neuroscience of psychoactive substance use and dependence.
1 . Psychotropic drugs - pharmacology 2 . Substancerelated disorders -physiopathology 3 . Psychopharmacology 4 . Brain - drug effects I. World Health Organization.
Foreword ix
Acknowledgements xi
List of background papers and contributors xv
Abbreviations xvii
Chapter 1 . Introduction 1
Structure of the report 1
Psychoactive substances and their sociolegal status 1
Global use of psychoactive substances 4
Tobacco 4
Alcohol 5
Illicit use of controlled substances 9
Adverse effects of psychoactive substances and their mechanisms
of action 1 0
Substance dependence in relation to neuroscience 1 2
The burden of harm to health from psychoactive substance use 1 6
Chapter 2 . Brain Mechanisms: Neurobiology and Neuroanatomy 1 9
Introduction 1 9
Organization of the brain 1 9
The neuron 2 5
Cell body 2 6
Dendrites 2 6
Axon 2 8
Terminal buttons 2 8
Neurotransmission 2 9
Action potential 2 9
Neurotransmitter release 3 0
Receptors 3 1
Neurotransmitters 3 2
Acetylcholine 3 3
Serotonin 3 5
Peptides 3 5
Genes 3 5
Cellular and neuronal effects of psychoactive substances 3 6
Cellular effects 3 6
Neuronal effects 3 8
Conclusion 3 9
Chapter 3 . Biobehavioural Processes Underlying Dependence 4 3
Introduction 4 3
Defining terms 4 4
Classical or Pavlovian conditioning 4 4
Instrumental or operant conditioning 4 6
Reinforcer 4 7
Reward 4 7
Incentive 4 7
Motivation 4 8
Incentive-motivational responding 4 8
Drug reward alone does not explain drug dependence 4 8 Drug dependence as a response to incentive-motivation 4 9 Drug dependence as a response to drug withdrawal 5 0
Dopamine and reinforcement learning 5 0
Dependence-producing drugs as surrogates of conventional
reinforcers 5 1
Dopamine and incentive sensitization 5 2
Psychomotor sensitization 5 3
Sensitization and drug reward 5 3
Sensitization and tolerance 5 4
Individual differences 5 5
Summary 5 8
Chapter 4 . Psychopharmacology of Dependence for Different
Drug Classes 6 7
Introduction 6 7
Alcohol (ethanol) 6 9
Introduction 6 9
Behavioural effects 6 9
Mechanism of action 7 0
Tolerance and withdrawal 7 0
Neurobiological adaptations to prolonged use 7 2
Tolerance and withdrawal 7 4
Neurobiological adaptations to prolonged use 7 5
Tobacco 7 5
Introduction 7 5
Behavioural effects 7 5
Mechanism of action 7 6
Tolerance and withdrawal 7 7
Pharmacological treatment of nicotine dependence 7 8
Opioids 7 9
Introduction 7 9
Behavioural effects 7 9
Mechanism of action 8 0
Tolerance and withdrawal 8 0
Neurobiological adaptations to prolonged use 8 1
Pharmacological treatment of opioid dependence 8 1
Cannabinoids 8 4
Introduction 8 4
Behavioural effects 8 5
Mechanism of action 8 6
Tolerance and withdrawal 8 7
Neurobiological adaptations to prolonged use 8 8
Cocaine (hydrochloride and crack) 8 9
Introduction 8 9
Behavioural effects 8 9
Mechanism of action 8 9
Tolerance and withdrawal 9 1
Neurobiological adaptations to prolonged use 9 1
Pharmacological treatment of cocaine dependence 9 2
Amphetamines 9 3
Introduction 9 3
Behavioural effects 9 4
Mechanism of action 9 5
Tolerance and withdrawal 9 5
Neurobiological adaptations to prolonged use 9 6
Ecstasy 9 6
Introduction 9 6
Behavioural effects 9 9
Mechanism of action 9 9
Tolerance and withdrawal 1 0 0
Neurobiological adaptations to prolonged use 1 0 0
Tolerance and withdrawal 1 0 3
Neurobiological adaptations to prolonged use 1 0 3
Hallucinogens 1 0 4
Introduction 1 0 4
Behavioural effects 1 0 5
Mechanism of action 1 0 5
Tolerance and withdrawal 1 0 5
Neurobiological adaptations to prolonged use 1 0 6
Summary 1 0 6
Chapter 5 . Genetic Basis of Substance Dependence 1 2 5
Introduction 1 2 5
Family, twin and adoption studies: estimations of heritability 1 2 7 Identifying chromosomal locations of interest: linkage studies 1 2 7
Candidate gene approach 1 2 8
Animal studies 1 2 8
Genetics of tobacco dependence 1 3 0
Heritability of tobacco dependence 1 3 0
Tobacco dependence and linkage studies 1 3 1
Candidate genes for tobacco dependence 1 3 1
Genetics of alcohol dependence 1 3 2
Heritability of alcohol dependence 1 3 2
Alcohol dependence and linkage studies 1 3 3
Candidate genes for alcohol dependence 1 3 4
Genetics of opioid dependence 1 3 6
Heritability of opioid dependence 1 3 6
Opioid dependence and linkage studies 1 3 6
Candidate genes for opioid dependence 1 3 6
Genetics of the combined risk of dependence on tobacco, alcohol,
opioids and other psychoactive substances 1 3 8
Heritability of substance dependence 1 3 8
Linkage studies of substance dependence 1 3 9
Candidate genes involved in substance dependence 1 4 0 Confounding issues in linkage and candidate gene studies 1 4 7
Environment 1 4 7
Genetice heterogeneity 1 4 7
Phenotype 1 4 8
Comorbidity 1 4 8
Methodological issues 1 4 8
Chapter 6 . Concurrent Disorders 1 6 9
Introduction 1 6 9
Hypotheses that may explain the observed comorbidity 1 7 0
Schizophrenia 1 7 1
Tobacco smoking and schizophrenia 1 7 1
Psychostimulant (cocaine and amphetamine) dependence and
schizophrenia 1 7 4
Alcohol use and schizophrenia 1 7 6
Neurobiological interactions between schizophrenia and the effects
of psychoactive substances 1 7 6
Depression 1 8 0
Tobacco smoking and depression 1 8 1
Psychostimulant dependence and depression 1 8 2
Alcohol use and depression 1 8 3
Neurobiological interactions between depression and the effects
of psychoactive substances 1 8 4
Discussion and conclusions 1 8 8
Chapter 7 . Ethical Issues in Neuroscience Research on Substance
Dependence Treatment and Prevention 2 0 9
Introduction 2 0 9
Types of research on neuroscience of substance dependence 2 0 9
Animal experiments 2 0 9
Epidemiological research on substance dependence 2 0 9
Experimental studies in humans 2 1 0
Clinical trials of pharmacotherapy for substance dependence 2 1 0 Trials of pharmacotherapies to prevent substance dependence 2 1 1
Approach to ethical analysis 2 1 1
Principles of biomedical ethics 2 1 6
Human rights 2 1 7
Ethics of animal experimentation in neuroscience research 2 1 8
Ethical principles in human biomedical research 2 1 9
Independent ethical review of risks and benefits 2 1 9
Informed consent 2 2 0
Recruitment of subjects 2 2 0
Privacy and confidentiality 2 2 1
Emerging ethical issues in neuroscience research 2 2 2
Research on vulnerable persons 2 2 2
Are substance dependent people vulnerable persons? 2 2 3
Provocation studies 2 2 3
Distributive justice 2 2 6
Conflicts of interest 2 2 6
Trials of preventive pharmacological interventions for substance
dependence 2 2 7
Early intervention studies 2 2 7
Preventive use of drug immunotherapies 2 2 9
Implications of neuroscience research for models of substance
dependence 2 3 1
Implications of neuroscience research for the treatment of substance
dependence 2 3 2
Access to treatment 2 3 2
Legally coerced treatment 2 3 2
Summary and conclusions 2 3 5
Chapter 8 . Conclusion and Implications for Public Health Policy 2 4 1
Introduction 2 4 1
Advances in the neuroscience of psychoactive substance use and
dependence and their implications 2 4 1
Potential advances in policy, prevention and treatment 2 4 3 Ethical issues in the application of neuroscience findings 2 4 4
Implications for public health policy 2 4 7
Conclusion 2 4 8
Substan ce use an d dep en den ce cause a sign ifican t burden to in dividuals an d societies th rou gh ou t th e world. Th e World Health Rep ort 2002 in dicated th at 8.9% of th e total b u rd en of d isease com es from th e u se of p sych oactive su bstan ces. Th e rep ort sh owed th at tobacco accou n ted for 4.1%, alcoh ol 4%, an d illicit dru gs 0.8% of th e bu rden of disease in 2000. Mu ch of th e bu rden attribu table to su bstan ce u se an d dep en den ce is th e resu lt of a wide variety of h ealth an d social p roblem s, in clu din g HIV/ AIDS, wh ich is driven in m an y cou n tries by in jectin g dru g u se.
Th is n eu ro scien ce rep o rt is th e first a ttem p t b y WH O to p rovid e a com p reh en sive overview of th e biological factors related to su bstan ce u se an d dep en den ce by su m m arizin g th e vast am ou n t of kn owledge gain ed in th e last 20-30 years. Th e rep ort h igh ligh ts th e cu rren t state of kn owledge of th e m ech an ism s of action of differen t typ es of p sych oactive su bstan ces, an d exp lain s h ow th e u se of th ese su bstan ces can lead to th e develop m en t of dep en den ce syn drom e.
Th o u gh th e fo cu s is o n b ra in m ech a n ism s, th e rep o rt n everth eless addresses th e social an d en viron m en tal factors wh ich in flu en ce su bstan ce use an d dep en den ce. It also deals with n euroscien ce asp ects of in terven tion s an d, in p articu lar, th e eth ical im p lication s of n ew biological in terven tion strategies.
Th e va rio u s h ea lth a n d so cia l p ro b lem s a sso cia ted with u se o f a n d d ep en d en ce on tob a cco, a lcoh ol a n d illicit su b sta n ces req u ire grea ter atten tion by th e p u blic h ealth com m u n ity an d ap p rop riate p olicy resp on ses are n eeded to address these problem s in differen t societies. Man y gaps rem ain to be filled in ou r u n derstan din g of th e issu es related to su bstan ce u se an d dep en den ce bu t th is rep ort sh ows th at we already kn ow a great deal abou t th e n atu re of th ese p roblem s th at can be u sed to sh ap e p olicy resp on ses.
The World Health Organ ization ackn owledges with than ks the m an y authors, reviewers, con su ltan ts an d WHO staff m em bers wh ose exp ertise m ade th is rep ort p ossible. Fran co Vaccarin o of th e Cen tre for Addiction an d Men tal Health an d th e Un iversity of Toron to, Toron to, Can ada, was th e p rin cip al editor for th e rep ort, with th e assistan ce of Su san Rotzin ger from th e Cen tre for Addiction an d Men tal Health . Th e op en in g an d closin g ch ap ters were written by Robin Room of th e Cen tre for Social Research on Alcoh ol an d Drugs, Un iversity of Stockholm , Stockholm , Sweden , with con tribution s from Isidore Obot an d Maristela Mon teiro of th e Dep artm en t of Men tal Health an d Su bstan ce Abu se, WHO.
Sp ecia l a ckn owled gem en t is m a d e to th e followin g in d ivid u a ls wh o con tribu ted reviews th at form ed th e basis for th e fin al rep ort:
Sch ool of Pu blic Health , Boston , MA, USA; An drey Ryabin in , Oregon Health Scie n ce Un ive rsity, Po rtla n d , OR, USA; Alliso n Sm ith , De p a rtm e n t o f Pop u lation an d In tern ation al Health , Harvard Un iversity Sch ool of Pu blic Health , Boston , MA, USA; Rach el Tyn dale, Dep artm en t of Ph arm acology, Un ive rsit y o f To ro n t o, To ro n t o, On t a r io, Ca n a d a ; Cla u d e U e h lin ge r, Psych osocial Cen tre of Fribou rg, Fribou rg, Switzerlan d; Fran co Vaccarin o, Cen tre for Addiction an d Men tal Health , Toron to, On tario, Can ada; Fran k Vocci, Nation al In stitu te on Dru g Abu se, Beth esda, MD, USA; David Walsh , Nation al In stitu te on Media an d th e Fam ily, Min n eap olis, MN, USA.
Th an ks are also d u e to th e in tern ation al scien tific organ ization s th at p rovided docu m en ts reflectin g th eir views on research on an d treatm en t of su bstan ce dep en den ce. Notable am on g th ese are th e College on Problem s of Dru g Dep en d en ce (CPDD) a n d th e In tern a tio n a l So ciety o f Ad d ictio n Medicin e (ISAM).
Man y in dividu als p articip ated in th e variou s con su ltation s h eld to discu ss th e p roject. Th e first su ch con su ltation wh ich took p lace in New Orlean s, LA, USA, in 2000 was atten d ed by exp erts rep resen tin g several in tern ation al organ ization s, in clu din g th e CPDD, th e In tern ation al Society for Biom edical Research on Alcoh olism (ISBRA), th e Nation al In stitu te on Dru g Ab u se (NIDA), th e Nation al In stitu te of Men tal Health (NIMH) an d som e key scien tists in th e field (see list below). Th e secon d con su ltation was h eld in Mexico in Jun e 2002 durin g which a draft rep ort was p resen ted an d discussed exten sively. Th an ks are du e to th e followin g for th eir variou s con tribu tion s to th e rep ort:
Un iversity of Stockh olm , Stockh olm , Swed en ; Ch ristin e A. Rose, Pin n ey Associates, Bethesda, MD, USA; Martin Stafstrom , Malm o Un iversity Hospital, Lu n d Un iversity, Lu n d, Sweden ; Ju lie Staley, Dep artm en t of Psych iarty, Yale Un ive rsit y Sch o o l o f Me d icin e, Ne w Ha ve n , CT, U SA; Howa rd St e a d , Laboratory an d Scien tific Section , Un ited Nation s Office on Drugs an d Crim e, Vien n a, Au stria; Boris Tabakoff, Un iversity of Colorado Sch ool of Medicin e, Boulder, CO, USA; Am bros Uchten hagen , In stitute for Research on Addiction , Zu rich , Switzerla n d ; Geo rge Uh l, Jo h n s Ho p kin s Un iversity Sch o o l o f Me d ic in e, Ba lt im o re , M D, U SA; No ra Vo lkow, Bro o kh a ve n Na t io n a l Laboratory, New York, NY, USA; Helge Waal, Oslo, Norway; Roy Wise, Nation al In stitu te on Dru g Abu se, Beth esda, MD, USA. WHO is also gratefu l to Victor Preed y, Kin g’s College, Un iversity of Lon d on , Lon d on , wh o p rovid ed a tech n ical review of th e fin al draft of th e docu m en t.
Gra t e fu l t h a n ks a re d u e t o t h e U .K. De p a rt m e n t fo r In t e r n a t io n a l De ve lo p m e n t (DFID), t h e Be lgia n Gove r n m e n t , a n d t h e In st it u t e o f Neuroscien ces, Men tal Health an d Addiction of the Can adian In stitutes of Health Research for their fin an cial con tribution s to the project.
Th e p roject leadin g to th is rep ort was in itiated by Maristela Mon teiro, wh o also directed all activities related to its p rep aration , review an d p u blication . Isidore Obot coordin ated th e editin g an d p rodu ction of th e rep ort. Particu lar th a n ks a re d u e to Derek Ya ch a n d Ben ed etto Sa ra cen o wh o p rovid ed lead ersh ip for th e p roject an d con trib u ted com m en ts on variou s d rafts. Th an ks are also due to th e followin g staff of the Dep artm en t of Men tal Health an d Substan ce Abuse for their con tribution s to the project: Vladim ir Pozn yak, José Bertolote, an d Shekhar Saxen a. The report also ben efited from the in puts of th e followin g form er an d cu rren t WHO staff wh o assisted in d ifferen t cap acities: Carolin e Allsop p, Alexan der Cap ron , Joan n Du ffil, Kelvin Kh ow, Tess Narciso, Mylen e Sch reiber, Raqu el Sh aw Moxam , an d Toku o Yosh ida.
Helena M. T. Barros, Th e basic p sych op h arm acology of th e addictive su bstan ces.
David A Collier, Th e gen etics of h eroin abu se.
Michael J. Kuhar, Views of the College on Problem s of Drug Depen den ce regardin g advan ces in research on dru g abu se.
Gaetano Di Chiara, Psych obiology of dru g addiction .
Patricia G Erickson, Resp on din g to su bstan ce dep en den ce from an in tegrated p u blic h ealth p ersp ective.
Wayne Hall and Lucy Carter, Eth ical issu es in trialin g an d u sin g cocain e vaccin es to treat an d p reven t cocain e dep en den ce.
Wayne Hall, Lucy Carter and Katherine Morley, Eth ical issu es in n eu roscien ce research on addiction .
Sofia Gruskin, Karen Plafker & Allison Sm ith, A h u m an righ ts fram ework for p reven tin g p sych oactive su bstan ce u se by you th , in th e con text of u rban ization .
Jack E Henningfield, Neu robiology of tobacco dep en den ce.
Nady El-Gue baly, Views of th e In tern ation al Society of Ad d iction Med icin e (ISAM).
Kathleen M. Kantak, Pre-clin ical an d clin ical stu dies with th e cocain e vaccin e.
Brigitte L. Kieffer, Neu ral basis of addictive beh aviou rs: role of th e en dogen ou s op ioid system .
Harald Klingem ann, Cu ltu ral an d social asp ects of dru g dep en den ce.
Mary Jeanne Kreek, Th e efficacy of m eth adon e an d levom eth adyl acetate.
Sture Liljequist, The n eurochem ical basis of cravin g an d abstin en ce to substan ce abu se.
Rafae l Maldo n ado, Recen t a d va n ces in th e n eu ro b io lo gy o f ca n n a b in o id dep en den ce.
Athina Markou, Com orbidity of dru g abu se with m en tal illn ess p rovides in sigh ts in to th e n eu rob iological ab n orm alities th at m ay m ed iate th ese p sych iatric disorders.
Rachel Tyndale, Gen etics of alcoh ol an d tobacco u se in h u m an s.
Claude Uehlinger, Motivation au x ch an gem en ts de com p ortem en ts addictifs.
Frank J. Vocci, Bu p ren orp h in e as a treatm en t for op iate dep en den ce.
2-DG 2-deoxyglu cose ADH alcoh ol deh ydrogen ase
ADHD atten tion deficit h yp eractivity disorder AIDS Acqu ired Im m u n odeficien cy Syn drom e ALDH2 aldeh yde deh ydrogen ase
AMPA α-am in o3-h ydroxy-5-m eth yl-isoxazole-4-p rop ion ate ASPD an tisocial p erson ality disorder
ATS am p h etam in e-typ e stim u lan ts cAMP cyclic aden osin e m on op h osp h ate CCK ch olecystokin in
COMT catech ol-O-m eth yltran sferase CRA com p arative risk an alysis
CREB cAMP resp on se elem en t bin din g p rotein CRF corticotrop in -releasin g factor (CRF) CYP26 Cytoch rom e P-450 RA1
CYP2D6 Cytoch rom e P-450 2D6 CYP2E1 Cytoch rom e P-450 2E1 DALY disability-adju sted life years DBH dop am in e beta h ydroxylase DMT dim eth yltryp tam in e DNA deoxyribon u cleic acid
DOM dim eth oxy-4-m eth ylam p h etam in e DRD1 dop am in e recep tor D1
EMCDDA Eu rop ean Mon itorin g Cen tre for Dru gs an d Dru g Addiction ESPAD Eu rop ean Sch ool Su rvey Project on Alcoh ol an d Oth er Dru gs EEG electroen cep h alograp h y
FDA Un ited States Food an d Dru g Adm in istration FDG flu orodeoxyglu cose
fMRI fu n ction al m agn etic reson an ce im agin g GABA γ-am in obu tyric acid
GBD Global Bu rden of Disease HIV Hu m an Im m u n odeficien cy Viru s
ICD-10 Ten th Revision of th e In tern ation al Statistical Classification of Diseases an d Related Health Problem s
IDU in jectin g dru g u se
LAAM Levo-alp h a-acetyl-m eth adol LSA d-lysergic acid am in e LSD lysergic acid dieth ylam ide MAO m on oam in e oxidase
MAOI m on oam in e oxidase in h ibitor MDA m eth ylen edioxyam p h etam in e
MDMA 3,4-m eth ylen edioxym eth am p h etam in e MET m otivation al en h an cem en t th erapy MRI m agn etic reson an ce im agin g m RNA m essen ger ribon u cleic acid n ACh R n icotin ic acetylch olin e recep tor
NHSDA Nation al Hou seh old Su rvey on Dru g Abu se NIDA Nation al In stitu te on Dru g Abu se
NMDA N-m eth yl-D-asp artate NPY n eu rop ep tide Y PCP p h en cyclidin e
PET p ositron em ission tom ograp h y PMA p aram eth oxyam p h etam in e QTL qu an titative trait loci
TH tyrosin e h ydroxylase THC tetrah ydrocan n abin ol TMA trim eth oxyam p h etam in e TPH tryp top h an h ydroxylase
UDHR Un iversal Declaration of Hu m an Righ ts
UNDCP Un ited Nation s In tern ation al Dru g Con trol Program m e UNODC Un ited Nation s Office on Dru gs an d Crim e
UNODCCP Un ited Nation s Office for Dru g Con trol an d Crim e Preven tion USDHHS Un ited States Dep artm en t of Health an d Hu m an Services VTA ven tral tegm en tal area
CHAPTER 1
Introduction
Th is rep ort d escrib es ou r cu rren t u n d erstan d in g of th e n eu roscien ce of psychoactive substan ce use an d depen den ce. It draws on the explosive growth in kn owled ge in th is area in recen t d ecad es, wh ich h as tran sform ed ou r u n derstan din g of th e bioch em ical action of p sych oactive su bstan ces, an d con tribu ted n ew in sigh ts in to wh y m an y p eop le u se th em , an d wh y som e u se th em to th e exten t of cau sin g h arm or of becom in g dep en den t on th em .
Structure of the report
con sciou sn ess, m ood or th in kin g p rocesses. As later ch ap ters will exp lain , advan ces in n eu roscien ce h ave given u s a m u ch better u n derstan din g of th e p h ysical p rocesses by wh ich th ese su bstan ces act. Psych oactive su bstan ces act in th e brain on m ech an ism s th at exist n orm ally to regu late th e fu n ction s of m ood, th ou gh ts, an d m otivation s. In th is rep ort, ou r em p h asis will be on alcoh ol an d oth er h yp n otics an d sed atives, n icotin e, op ioid s, can n ab is, c o c a in e , a m p h e t a m in e s a n d o t h e r st im u la n t s, h a llu c in o ge n s, a n d p sych oactive in h alan ts.
Use of th ese su bstan ces is defin ed in to th ree categories accordin g to th eir sociolegal statu s. First, m an y of th e su bstan ces are u sed as m edication s. Western an d oth er system s of m edicin e h ave lon g recogn ized th e u sefu ln ess of th ese su bstan ces as m edication s in relievin g p ain , p rom otin g eith er sleep or wakefu ln ess, an d relievin g m ood disorders. Cu rren tly, m ost p sych oactive m e d ica t io n s a re re st rict e d t o u se u n d e r a d o ct o r’s o rd e rs, t h ro u gh a p re scr ip t io n syst e m . In m a n y co u n t rie s, a s m u ch a s o n e -t h ird o f a ll p rescrip tion s written are for su ch m edication s. An exam p le of th is is th e u se o f th e stim u la n t m eth ylp h en id a te to trea t ch ild h o o d a tten tio n d eficit h yp eractivity d isord er (ADHD), wh ich will b e d iscu ssed in Ch ap ter 4. As described in Ch ap ter 6, som e of th e su bstan ces are also often u sed as “self-m ed ication s” to relieve d istress fro“self-m “self-m en tal or p h ysical d isord ers, or to alleviate th e side-effects of oth er m edication s.
A secon d category of u se is illegal, or illicit, u se. Un der th ree in tern ation al con ven tion s (see Box 1.1), m ost n ation s h ave bou n d th em selves to ou tlaw trade in an d n on -m edical u se of op iates, can n abis, h allu cin ogen s, cocain e an d m an y oth er stim u lan ts, an d m an y h yp n otics an d sedatives. In addition to th is list, cou n tries or local ju risdiction s often add th eir own p roh ibited su bstan ces, e.g. alcoh olic beverages an d variou s in h alan ts.
Desp ite th ese p roh ibition s, illicit u se of p sych oactive su bstan ces is fairly widesp read in m an y societies, p articu larly am on g you n g adu lts, th e u su al p u rp ose bein g to en joy or ben efit from th e p sych oactive p rop erties of th e su bstan ce. Th e fact th at it is illegal m ay also add an attractive frisson , an d th u s stren gth en th e iden tification of u sers with an alien ated su bcu ltu re.
Th e th ird category of u se is legal, or licit, con su m p tion , for wh atever p u rp ose th e con su m er ch ooses. Th ese p u rp oses m ay be qu ite varied, an d are n ot n ecessarily con n ected with th e p sych oactive p rop erties of th e su bstan ce. For in stan ce, an alcoh olic beverage can be a sou rce of n u trition , of h eatin g or coolin g th e b od y, or of th irst-qu en ch in g; or it m ay serve a sym bolic purpose in a roun d of toastin g or as a sacram en t. However, whatever th e p u rp ose of u se, th e p sych oactive p rop erties of th e su bstan ce in evitably accom p an y its u se.
BOX 1 .1
United Nations drug control conventions
The three major international drug control treaties are mutually supportive and complementary. An impor tant purpose of the first two treaties is to codify internationally applicable control measures in order to ensure the availability of narcotic drugs and psychotropic substances for medical and scientific purposes, and to prevent their diversion into illicit channels. They also include general provisions on illicit trafficking and drug abuse.
Single Convention on Narcotic Drugs, 1 9 6 1
This Convention recognizes that effective measures against abuse of narcotic drugs require coordinated and international action. There are two forms of intervention and control that work together. First, it seeks to limit the possession, use, trade in, distribution, impor t, expor t, manufacture and production of drugs exc lusively t o m edic al and sc ient ific pur poses. Sec ond, it c om bat s dr ug traffic king through international c ooperation to deter and disc ourage drug traffickers.
Convention on Psychotropic Substances, 1 9 7 1
The Convention noted with concern the public health and social problems resulting from the abuse of certain psychotropic substances and was determined to prevent and combat abuse of such substances and the illicit traffic which it gives rise to. The Convention establishes an international control system for psychotropic substances by responding to the diversification and expansion of the spectrum of drugs of abuse, and introduced controls over a number of synthetic drugs according to their abuse potential on the one hand and their therapeutic value on the other.
United Nations Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances, 1 9 8 8
This Convention sets out a comprehensive, effective and operative international treaty that was directed specifically against illicit traffic and that considered various aspects of the problem as a whole, in par ticular those aspects not envisaged in the existing treaties in the field of narcotic drugs and psychotropic substances. The Convention provides comprehensive measures against drug trafficking, including provisions against money laundering and the diversion of prec ursor c hemic als. It provides for international c ooperation through, for example, extradition of drug traffickers, controlled deliveries and transfer of proceedings.
an d distilled sp irits. Becau se th e u se of caffein ated su bstan ces is relatively u n p roblem atic, it is n ot fu rth er con sidered in th is rep ort. Wh ile in h alan ts are also widely available, they are m ostly used for psychoactive purposes by those b elow th e age of easy access to alcoh ol, tob acco an d oth er p sych oactive su bstan ces.
Wh ile th ere is a clear ration ale for a sep arate legal statu s for m edication s, t h e ra t io n a le fo r t h e d ist in ct io n b e t we e n su b st a n ce s t h a t a re u n d e r in tern ation al con trol an d th ose th at are n ot is m ore p rob lem atic. Th e su b stan ces wh ich are in clu d ed in th e in tern ation al con ven tion s reflect h istorical u n derstan din gs in p articu lar cu ltu ral settin gs abou t wh at sh ou ld be viewed as u n iqu ely dan gerou s or alien . Som e p sych op h arm acologists or ep idem iologists today, for in stan ce, wou ld argu e th at alcoh ol is in h eren tly n o less dan gerou s or h arm fu l th an th e dru gs in clu ded in th e in tern ation al con ven tion s. Moreover, as d iscu ssed b elow, d ep en d en ce on n icotin e in tobacco is associated with m ore death an d ill-h ealth th an dep en den ce on oth er p sych oactive su bstan ces. As will be seen in th e ch ap ters wh ich follow, th e growin g kn owledge of th e n eu roscien ce of p sych oactive su bstan ce u se h as em p h asized th e com m on alities in action wh ich sp an th e th ree sociolegal statu ses in to wh ich th e su bstan ces are divided.
Global use of psychoactive substances
Tob a cco
Man y typ es of tobacco p rodu cts are con su m ed th rou gh ou t th e world bu t th e m o st p o p u la r fo rm o f n ico tin e u se is ciga rette sm o kin g. Sm o kin g is a u b iqu itou s activity: m ore th an 5500 b illion cigarettes are m an u factu red an n u ally an d th ere are 1.2 b illion sm okers in th e world . Th is n u m b er is expected to in crease to 2 billion by 2030 (Mackay & Eriksen , 2002; World Ban k, 1999). Sm okin g is sp read in g rap id ly in d evelop in g cou n tries an d am on g wom en . Cu rren tly, 50% of m en an d 9% of wom en in develop in g cou n tries sm oke, as com p ared with 35% of m en an d 22% of wom en in d evelop ed cou n tries. Ch in a, in p articu lar, con tribu tes sign ifican tly to th e ep idem ic in develop in g cou n tries. In deed, th e p er cap ita con su m p tion of cigarettes in Asia an d th e Far East is h igh er th an in oth er p arts of th e world, with th e Am ericas an d eastern Eu rop e followin g closely beh in d (Mackay & Eriksen , 2002).
alth ou gh sm okin g is in creasin g in th is region . It h as been sh own th at an n u al per capita con sum ption of cigarettes there is less than 100 (Corrao et al., 2000). There is widespread use of other tobacco products (such as sn uff an d chewin g tobacco) in som e cou n tries, bu t th e exten t of adverse h ealth con sequ en ces of u se of th ese form s of tobacco is still n ot clear.
In Stage 2 of th e ep idem ic, abou t 50% of th e m en sm oke an d th ere is an in creasin g percen tage of wom en sm okers. This is the case in Chin a an d Japan , an d in som e coun tries in n orthern Africa an d Latin Am erica. In con trast, Stage 3 describes a situ ation in wh ich th ere is a n oticeable decrease in sm okin g am on g m en an d wom en b u t th ere is in creased m ortality from sm okin g-related diseases. Som e cou n tries in Latin Am erica an d eastern an d sou th ern Eu rop e fall in to th is category. A fin al stage is m arked by decreasin g sm okin g p revalen ce, a p eakin g of death s from tobacco-related disease am on g m en (accou n tin g for abou t on e-th ird of th e total), an d a con tin u ed in crease in deaths from tobacco-related disease am on g wom en . This is curren tly the case in Au stralia, Can ada, th e USA, an d western Eu rop e. Table 1.1 sh ows th e rates of sm okin g for m ales an d fem ales an d p er cap ita con su m p tion of cigarettes in selected cou n tries with data from all categories of sm okers.
Table 1 .1 Prevalence of smoking among adults and youths in selected countries
Annual Prevalence of smoking (%) per capita
Adults Youths consumption
Country of cigarettes Males Females Males Females
Argentina 1 4 9 5 4 6 .8 3 4 .4 2 5 .7 3 0 .0
Bolivia 2 7 4 4 2 .7 1 8 .1 3 1 .0 2 2 .0
Chile 1 2 0 2 2 6 .0 1 8 .3 3 4 .0 4 3 .4
China 1 7 9 1 6 6 .9 4 .2 1 4 .0 7 .0
Ghana 1 6 1 2 8 .4 3 .5 1 6 .2 1 7 .3
Indonesia 1 7 4 2 5 9 .0 3 .7 3 8 .0 5 .3
Jordan 1 8 3 2 4 8 .0 1 0 .0 2 7 .0 1 3 .4
Kenya 2 0 0 6 6 .8 3 1 .9 1 6 .0 1 0 .0
Malawi 1 2 3 2 0 .0 9 .0 1 8 .0 1 5 .0
Mexico 7 5 4 5 1 .2 1 8 .4 2 7 .9 1 6 .0
Nepal 6 1 9 4 8 .0 2 9 .0 1 2 .0 6 .0
Peru 1 8 4 9 4 1 .5 1 5 .7 2 2 .0 1 5 .0
Poland 2 0 6 1 4 4 .0 2 5 .0 2 9 .0 2 0 .0
Singapore 1 2 3 0 2 6 .9 3 .1 1 0 .5 7 .5
Sri Lanka 3 7 4 2 5 .7 1 .7 1 3 .7 5 .8
USA 2 2 5 5 2 5 .7 2 1 .5 2 7 .5 2 4 .2
aggressively by tran sn ation al corp oration s th at target you n g p eop le in advertisin g an d p rom otion cam p aign s. Accordin g to th e Global statu s rep ort o n a lco h o l ( WH O, 1999) a n d a s sh own in Fig. 1.1 b e low, th e le ve l o f con su m p tion of alcoh ol h as declin ed in th e p ast twen ty years in develop ed cou n tries bu t is in creasin g in develop in g cou n tries, esp ecially in th e Western Pacific Region where the an n ual per capita con sum ption am on g adults ran ges from 5 to 9 litres of p u re alcoh ol, an d also in cou n tries of th e form er Soviet Un io n ( WH O, 1999). To a gre a t e xt e n t t h e rise in t h e ra t e o f a lco h o l con su m p tion in develop in g cou n tries is driven by rates in Asian cou n tries. Th e level of con su m p tion of alcoh ol is m u ch lower in th e African , Eastern Mediterran ean , an d Sou th -East Asia Region s.
Th ere is a lon g tradition of research on th e ep idem iology of alcoh ol u se in develop ed cou n tries an d we h ave learn t m u ch abou t th e distribu tion an d d e t e r m in a n t s o f d r in kin g in d iffe re n t p o p u la t io n s. Fo r m a n y ye a rs, re se a rch e r s fo cu se d o n a ve ra ge vo lu m e o f a lco h o l co n su m p t io n in determ in in g th e level of drin kin g in a p articu lar cou n try. Usin g p rodu ction or sales data from official records has ten ded to un derestim ate con sum ption , especially in developin g coun tries, where un recorded con sum ption of locally brewed beverages is sign ifican t. In order to im p rove th e m easu rem en t of p er
cap ita con su m p tion , WHO h as sp on sored research p rojects in fou r cou n tries (Brazil, Ch in a, In d ia an d Nigeria) to d eterm in e th e level of u n record ed con su m p tion in th ese cou n tries.
It is exp ected th at m ore p recise estim ates of alcoh ol u se will lead to better u n derstan din g of th e association between u se an d p roblem s. In th is regard th e com p arative risk an alysis (CRA) p roject of WHO is n oteworth y. Th e CRA u ses p er cap ita con su m p tion data togeth er with p attern s of drin kin g to lin k u se to disease bu rden (Reh m et al., 2002). A p attern s ap p roach to alcoh ol con su m p tion assu m es th at th e way in wh ich alcoh ol is con su m ed is closely lin ked to disease ou tcom e. Drin kin g du rin g m eals, for exam p le, is associated with less risk of p roblem s th an drin kin g du rin g fiestas or drin kin g in p u blic p laces. In th e CRA an alysis, fou r p attern valu es h ave been develop ed, with 1 as th e least h azardou s an d 4 as th e m ost detrim en tal. At p attern valu e 1 th ere are few occasion s of h eavy drin kin g, an d drin kin g is often don e with m eals, wh ile p attern valu e 4 is ch aracterized by m an y h eavy drin kin g occasion s an d drin kin g ou tside m eals. Table 1.2 sh ows th e p attern valu es for differen t WHO region s, with each region divided in to at least two subregion s. Values for som e region s are based on lim ited aggregate data an d are on ly in dicative of th e p attern of drin kin g in th ese region s.
In th e African Region , th ere was a stead y rise in p er cap ita con su m p tion in th e 1970s an d a d eclin e b egin n in g from th e early 1980s. However, th e p attern of d rin kin g h as ten d ed toward s th e h igh er levels with m en in m ost cou n tries d rin kin g at p attern valu e 3 of th e CRA estim ates. Th is is th e case for Gab on , Gh an a, Ken ya, Lesoth o, Sen egal, an d Sou th Africa, for exam p le. However, it is on ly in very few cou n tries (e.g. Zam b ia an d Zim b abwe) th at th e p attern valu e is 4. Th e d etrim en tal p attern of d rin kin g in m an y su b -Sah aran cou n tries h as been sh own in several su rveys (e.g. Mu ston en , Beu kes & Du Preez, 2001; Ob ot, 2001). In m ost cou n tries wom en d rin k m u ch less th an m en an d in som e of th ese cou n tries th e ab sten tion rate for old er wom en is very h igh .
In th e Region of th e Am ericas, h eavy drin kin g (i.e. drin kin g five or m ore drin ks on at least on e occasion in th e p ast m on th ) is a com m on drin kin g b eh aviou r am on g you n g p eop le. Both alcoh ol con su m p tion an d h eavy drin kin g are rep orted m u ch m ore often am on g m ales th an fem ales in both Mexico an d th e USA (WHO, 1999; Medin a-Mora et al., 2001). Th ou gh Mexico h as a relatively low p er cap ita con su m p tion of alcoh ol, th e p attern valu e for th at cou n try is 4. Th is is becau se th ere is h igh frequ en cy of h eavy drin kin g, esp ecially by you n g p eop le, on fiesta occasion s.
N
Illicit use of controlled sub sta nces
Data from th e Un ited Nation s Office on Dru gs an d Crim e (ODC) sh ow large-scale seizures of cocain e, heroin , can n abis an d am phetam in e-type stim ulan ts in differen t p arts of th e world. Availability of cocain e, h eroin an d can n abis dep en ds on th e level of cu ltivation in sou rce cou n tries an d on th e su ccess or failu re of traffickin g organ ization s. However, even with in creased levels of law en forcem en t activities, th ere always seem s to be en ou gh dru gs available to u sers.
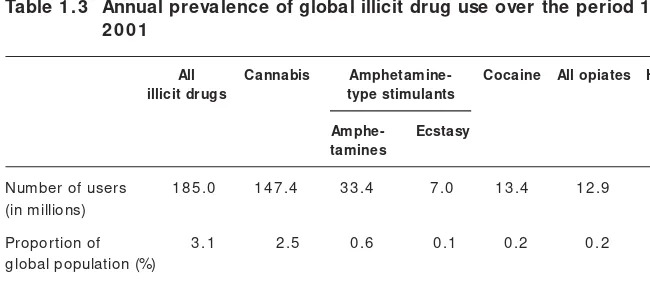
Accordin g to ODC estim ates (UNODCCP, 2002), abou t 185 m illion p eop le m ake illicit u se of on e typ e of illicit su bstan ce or an oth er. Table 1.3 sh ows that can n abis is con sum ed by the largest n um ber of illicit drug users, followed by am p h etam in es, cocain e an d th e op iates.
Illicit d ru g u se is a p red om in an tly m ale activity, m u ch m ore so th an cigarette sm okin g an d alcoh ol con sum p tion . Drug use is also m ore p revalen t am on g you n g p eop le th an in older age grou p s. Several n ation al an d m u lti-n atiolti-n al su rveys h ave p rovided data olti-n dru g u se ilti-n differelti-n t grou p s. For exam ple, in the USA, the Nation al Household Survey on Drug Abuse (NHSDA) h as served as a sou rce of u sefu l in form ation on d ru g u se in th e gen eral p op u lation , an d th e Mon itorin g th e Fu tu re p roject p rovides data on dru g u se by you n g p eop le in secon dary sch ools. Th e Eu rop ean Sch ool Su rvey Project on Alcoh ol an d Oth er Dru gs (ESPAD), an in itiative of th e Cou n cil of Eu rop e, h as becom e a data sou rce on you th dru g u se for m an y Eu rop ean cou n tries. Th e Eu rop ean Mon itorin g Cen tre for Dru gs an d Dru g Addiction (EMCDDA) also p rovides regu lar data on dru g u se (in clu din g h azardou s m eth ods of u se, su ch as in jectin g d ru g u se (IDU)) in Eu rop ean cou n tries. Wh ile n ation al su rveys of you th an d adu lts are h eld on a regu lar basis in som e cou n tries, reliable data on dru g u se is gen erally lackin g in m ost develop in g cou n tries.
Table 1 .3 Annual prevalence of global illicit drug use over the period 1 9 9 8 – 2 0 0 1
All Cannabis Amphetamine- Cocaine All opiates Heroin illicit drugs type stimulants
Amphe- Ecstasy tamines
Number of users 1 8 5 .0 1 4 7 .4 3 3 .4 7 .0 1 3 .4 1 2 .9 9 .2 0 (in millions)
Proportion of 3 .1 2 .5 0 .6 0 .1 0 .2 0 .2 0 .1 5 global population (%)
Projects su ch as th e Sou th African Com m u n ity Ep idem iology Network on Dru g Use (SACENDU) an d its related region al n etwork h ave been started to address th is lack of in form ation .
Th e data in Table 1.3 sh ow th at 2.5% of th e total global p op u lation an d 3.5% of p eop le 15 years an d above h ad u sed can n abis at least on ce in a year between 1998 an d 2001. In m an y develop ed cou n tries, for exam p le Can ada, th e USA an d Eu rop ean cou n tries, m ore th an 2% of you th s rep orted h eroin u se an d alm ost 5% rep orted sm okin g cocain e in th eir lifetim e. In deed, 8% of you th s in western Eu rop e an d m ore th an 20% of th ose in th e USA h ave reported usin g at least on e type of illicit drug other than can n abis (UNODCCP, 2002). Th ere is eviden ce of rap id in creases in th e u se of am p h etam in e-typ e stim u lan ts am on g teen agers in Asia an d Eu rop e. In jectin g dru g u se is also a growin g p h en om en on , with im p lication s for th e sp read of HIV in fection s in an in creasin g n u m ber of cou n tries.
Th e n on m edical u se of m edication s (e.g. ben zodiazep in es, p ain killers, am p h etam in es, etc.) is kn own to be fairly com m on bu t global statistics are lackin g.
Adverse effects of psychoactive substances and
their m echanism s of action
In th e m ajority of cases, p eop le u se p sych oactive su bstan ces becau se th ey exp ect to ben efit from th eir u se, wh eth er th rou gh th e exp erien ce of p leasu re or th e avoidan ce of p ain . Th e ben efit is n ot n ecessarily gain ed directly from th e p sych oactive action of th e su b stan ce. Som eon e d rin kin g b eer with colleagu es m ay be m ore m otivated by th e feelin g of fellowsh ip th is brin gs th an by th e p sych oactive effect of th e eth an ol.
However, th e p sych oactive effect is n everth eless p resen t, an d is u su ally at least p erip h erally in volved in th e decision to u se.
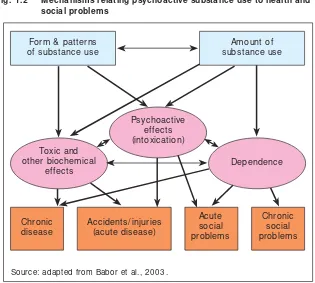
th is in clu des liver cirrh osis an d a h ost of oth er ch ron ic illn esses; for n icotin e taken in cigarette form , th is in clu des lu n g can cer, em p h ysem a an d oth er ch ron ic illn esses. Th rou gh th e sh arin g of n eedles, h eroin u se by in jection is a m ain vector for tran sm ission of in fectiou s agen ts su ch as HIV an d h ep atitis C viru s. Secon d th ere are th e acu te or sh ort-term biological h ealth effects of th e su bstan ce. Notably, for dru gs su ch as op ioids an d alcoh ol, th ese in clu de overdose. Also classed in this category are the casualties due to the substan ce’s e ffe ct s o n p h ysica l co o rd in a t io n , co n ce n t ra t io n a n d ju d ge m e n t , in circum stan ces where these qualities are dem an ded. Casualties resultin g from drivin g after drin kin g alcoh ol or after oth er dru g u se featu re p rom in en tly in th is category, bu t oth er acciden ts, su icide an d (at least for alcoh ol) assau lts are also in cluded. The third an d fourth categories of harm ful effects com prise the adverse social con sequen ces of the substan ce use: acute social p roblem s, su ch as a break in a relation sh ip or an arrest, an d ch ron ic social p roblem s, su ch as defau lts in workin g life or in fam ily roles. Th ese last categories are im p ortan t in relation to alcoh ol an d m an y illicit d ru gs, b u t are p oorly m easu red an d m ostly exclu ded from m easu rem en ts of h ealth effects su ch as in th e Global Bu rden of Disease (GBD).
Fig. 1 .2 Mechanisms relating psychoactive substance use to health and social problems
Form & patterns of substance use
Amount of substance use
Dependence Psychoactive
effects (intoxication) Toxic and
other biochemical effects
Chronic social problems Acute
social problems Accidents/ injuries
(acute disease) Chronic
As earlier n oted, th e p robability of th e occu rren ce of th ese categories of h arm fu l effects also dep en ds on h ow m u ch of th e su bstan ce is u sed, in wh at form s, an d with wh at p attern s of u se. Th ese asp ects of u se m ay be th ou gh t of as lin ked to th e differen t kin ds of h ealth an d social p roblem s by th ree m ain m echan ism s of action (see Fig. 1.2). On e m echan ism con cern s the direct toxic effects of the substan ce, either im m ediate (e.g. poison in g) or cum ulative over tim e (e.g. cirrh osis). A secon d m ech an ism con cern s th e in toxicatin g or oth er p sych oactive effects of th e su b stan ce. A traffic accid en t m ay resu lt, for in stan ce, from th e fact th at a car driver is u n der th e in flu en ce of sedatives. A retail store em p loyee m ay be in toxicated at work after u sin g can n abis, an d becau se of th is, m ay be fired by th e m an ager.
Th e th ird m ech an ism con cern s dep en den ce on th e su bstan ce. Su bstan ce depen den ce – or depen den ce syn drom e – is the curren t techn ical term in ology for th e con cep t of “addiction”. At th e h eart of th is con cep t is th e idea th at th e u ser’s con trol over an d volition ab ou t u se of th e d ru g h as b een lost or im p aired . Th e u ser is n o lon ger ch oosin g to u se sim p ly b ecau se of th e ap p aren t ben efits; th e u se h as becom e h abitu al, an d cravin gs to reu se m ean th at th e u ser feels th at th e h ab it is n o lon ger u n d er con trol. Th e u ser’s d e p e n d e n ce is t h u s se e n a s p ro p e llin g fu r t h e r u se d e sp it e a d ve r se con sequen ces which m ight have deterred others who are n ot depen den t, from fu rth er u se.
Th e lin k between su bstan ce u se an d h arm in a p articu lar case m ay, of cou rse, in volve m ore th an on e of th e th ree m ech an ism s. Ben zodiazep in es m ay be in volved in a case of su icide, for in stan ce, both th rou gh th e u ser’s desp air over th e disru p tion brou gh t to h is or h er life by dep en den ce on th e dru gs, an d as th e actu al m ean s of su icide th rou gh overdose. However, th e m echan ism s can also operate alon e. It is im portan t to keep in m in d, m oreover, th at dep en den ce is n ot th e on ly m ech an ism p oten tially lin kin g su bstan ce u se to h ealth an d social h arm .
Substance dependence in relation to neuroscience
positive on at least three of these is diagn osable as “depen den t”. Som e of the criteria are m easurable in biological term s, while others are not. The two criteria m ost easily m easured biologically are the third an d fourth in Box 1.2: with-drawal – the occurren ce of un pleasan t physical an d psychological sym ptom s when use of the substan ce is reduced or discon tin ued, an d toleran ce – the idea that increased am ounts of the drug are required to achieve the sam e effect, or th at th e sam e am ou n t p rodu ces less effect. Th e oth er fou r criteria for d ep en d en ce in clu d e elem en ts of cogn ition , wh ich are less accessib le to b iological m easu rem en t, b u t are b ecom in g m easu rab le u sin g im p roved n euroim agin g techn iques (see Chapter 3). In the sixth criterion , for in stan ce, th e u ser’s kn owled ge of sp ecific cau sal con n ection s is to b e ascertain ed , som ethin g n ot accessible to direct biological m easurem en t or to an an im al m odel. The first criterion , “stron g desire or sen se of com pulsion”, requires in quiry in to the user’s self-perception s, an d relates to the idea of cravin g for the substan ce. It has proved difficult to agree on a defin ition of the con cept of
BOX 1 .2
Criteria for substance dependence in ICD-1 0
Three or more of the following must have been experienced or exhibited together at some time during the previous year:
1 . a strong desire or sense of compulsion to take the substance;
2 . difficulties in controlling substance-taking behaviour in terms of its onset, termination, or levels of use;
3 . a physiological withdrawal state when substance use has ceased or been reduced, as evidenced by: the characteristic withdrawal syndrome for the substance; or use of the same (or a closely related) substance with the intention of relieving or avoiding withdrawal symptoms;
4 . evidence of tolerance, such that increased doses of the psychoactive substance are required in order to achieve effects originally produced by lower doses;
5 . pro g ressive neg lec t o f alt er nat ive pleasures o r int erest s bec ause o f psychoactive substance use, increased amount of time necessary to obtain or take the substance or to recover from its effects;
6. persisting with substance use despite clear evidence of over tly harmful consequences, such as harm to the liver through excessive drinking, depressive mood states consequent to heavy substance use, or drug-related impairment of cognitive functioning. Efforts should be made to determine that the user was actually, or could be expected to be, aware of the nature and extent of the harm.
Am erican Psychiatric Association (1994) are sim ilar to those of ICD-10 (Box 1.3), as well as those in m an y research studies. Other term s used in relation to the use of psychoactive substan ces are presen ted in Box 1.4.
A further difficulty is that the diagn ostic defin ition of depen den ce, as n oted
BOX 1 .3
Criteria for substance dependence in DSM-IV
According to the DSM-IV, substance dependence is:
a maladaptive pattern of substance use, leading to clinically significant impairment or distress, as manifested by three (or more) of the following, occurring at any time in the same 1 2 -month period:
1 . tolerance, as defined by either of the following:
(a) a need for markedly increased amounts of the substance to achieve intoxication or desired effect
(b) markedly diminished effect with continued use of the same amount of the substance
2 . withdrawal, as manifested by either of the following:
(a) the characteristic withdrawal syndrome for the substance
(b) the same (or a closely related) substance is taken to relieve or avoid withdrawal symptoms
3 . the substance is often taken in larger amounts or over a longer period than was intended
4 . there is a persistent desire or unsuccessful efforts to cut down or control substance use
5 . a great deal of time is spent in activities necessary to obtain the substance (e.g. visiting multiple doctors or driving long distances), use the substance (e.g. chain-smoking), or recover from its effects
6 . important social, occupational, or recreational activities are given up or reduced because of substance use
7 . the substance use is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance (e.g. current cocaine use despite recognition of cocaine-induced depression, or continued drinking despite recognition that an ulcer was made worse by alcohol consumption)
qu alifyin g as dep en den t m u st be p ositive on at least on e criterion wh ich is n ot fu lly biologically m easu rable.
Th u s a co n t in u in g d ifficu lt y in t h e n e u ro scie n ce o f p sych o a ct ive su bstan ces is th at, wh ile m ost of th eir effects sh own in Fig. 1.2 are directly m easurable, drug depen den ce is n ot, both as it is curren tly techn ically defin ed an d as it is gen erally u n derstood in th e wider society.
However, as will be discussed later in the report, n euroscien tists have m ade a n u m b er of ad van ces in u n d erstan d in g wh y h u m an s fin d u sin g th ese
BOX 1 .4
Definitions of terms related to use of psychoactive substances
Harmful use
A pattern of psychoactive substance use that is causing damage to health. The damage may be physical or mental.
Hazardous use
A pattern of psychoactive substance use that increases the risk of harmful consequences for the user.
Intoxication
A condition that follows the administration of a psychoactive substance and results in disturbances in the level of consciousness, cognition, perception, affect, or b ehavio ur, o r o t her p s yc ho p hys io lo g ic al f unc t io ns and res p o ns es . The disturbances are related to the acute pharmacological effects of, and learned responses to, the substance and resolve with time, with complete recovery, except where tissue damage or other complications have arisen. Complications may include trauma, inhalation of vomitus, delirium, coma and convulsions, and other medical complications. The nature of these complications depends on the pharmacological class of substance and mode of administration.
Substance abuse
Persistent or sporadic drug use inconsistent with or unrelated to acceptable medical practice. A maladaptive pattern of substance use leading to clinically significant impairment or distress, as manifested by one (or more) of the following: failure to fulfil major role obligations at home, school or work; substance use in situations in which it is physically hazardous; recurrent substance-related legal problems; continued substance use despite having persistent or recurrent social or interpersonal problems exacerbated by the effects of the substance.
The burden of harm to health from psychoactive substance use
No global assessm en ts are available for social h arm from su bstan ce u se (as sh own in Fig. 1.2). However, th ere is n ow a develop in g tradition of estim atin g th e con tribu tion of alcoh ol, tobacco an d illicit dru g u se to th e global bu rden of disease. Th e first sign ifican t attem p t at th is was in th e earlier WHO p roject on global bu rden of disease an d in ju ry (Mu rray & Lop ez, 1996). Based on a stan dard of m easu rem en t kn own as disability-adju sted life years (DALYs), estim ates of the burden im posed on society due to prem ature death an d years lived with disability were assessed. The global burden of disease (GBD) project showed that tobacco an d alcohol were m ajor causes of m ortality an d disability in develop ed cou n tries, with th e im p act of tobacco exp ected to in crease in oth er p arts of th e world.
Th e reliab ility of th e GBD an d oth er estim ates of d eath s an d d isease dep en ds on th e qu ality of th e data th ey are based u p on . Data u sed in th ese a n a lyses were m o stly fro m stu d ies co n d u cted in d evelo p ed co u n tries (e sp e cia lly t h e U SA a n d Eu ro p e a n co u n t r ie s) a n d a fe w, o ft e n n o n -rep resen tative, su rveys in develop in g cou n tries. Th e in h eren t difficu lty of assessin g th e p revalen ce of su bstan ce u se an d th e association between u se an d problem s also m ean s that the burden estim ates were highly approxim ate. However, the GBD provided for the first tim e a set of global data on the burden of alcoh ol an d oth er dru g u se/ dep en den ce an d th ere are con tin u in g efforts to com e u p with m ore p recise estim a tes of d ea th a n d d isea se b u rd en associated with licit an d illicit su bstan ces.
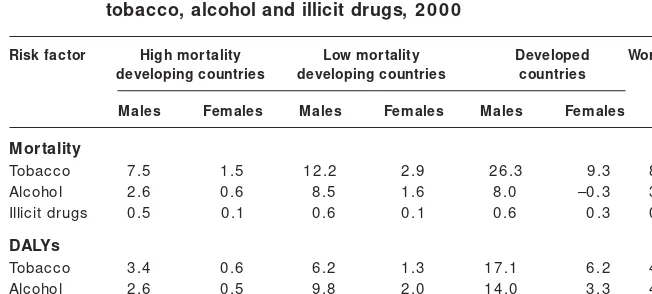
Th e 2002 World h ealth report (WHO, 2002) in clu des a n ew set of estim ates for th e year 2000 of th e b u rd en attrib u tab le to tob acco, alcoh ol an d oth er d ru gs. Th e se e stim a te s a re b a se d o n d a ta th a t a re sign ifica n tly m o re com p lete an d on m ore d efen sib le m eth od ologies, an d th ere is n o d ou b t th at th ey will be im p roved fu rth er in fu tu re years. Table 1.4 sh ows th e resu lts from th e estim ates for 2000, in term s of th e m ortality attrib u tab le to each class of su b stan ces, as well as a m easu re of th e years of life lost or im p aired d u e to d isab ility (DALYs). Note th at estim ated p rotective effects for h eart d isease from m od erate d rin kin g h ave b een su b tracted to yield th e n et n egative b u rd en for alcoh ol (th is accou n ts for th e n egative n u m b er in th e tab le).
Table 1.4 offers am p le eviden ce th at th e bu rden of ill-h ealth from u se of p sych oactive su b stan ces, taken togeth er, is su b stan tial: 8.9% in term s of DALYs. However, GBD fin din gs re-em p h asize th at th e m ain global h ealth bu rden is du e to licit rath er th an illicit su bstan ces.
Th e p rim ary em p h asis in th is rep ort, h owever, is n ot on th e h arm fu l con sequen ces which can result from substan ce use (except as they occur in the body’s n ervous system ) an d n either is it prim arily on the toxic qualities of the substan ces. Rather the em phasis is on pattern s of substan ce use, an d on the m echan ism s of psychoactivity an d of depen den ce (as in dicated in Fig. 1.2). Sin ce depen den ce refers to m echan ism s by which use is sustain ed over tim e – thereby m ultiplyin g the probabilities of harm ful con sequen ces of use – special atten tion is given in this report to the n euroscien ce of depen den ce.
References
Am erican Psych iatric Association (1994) Diagn ostic an d statistical m an u al of m en tal d isord ers, 4th ed . (DSM -IV ). Wash in gton , DC, Am erican Psych iatric Association .
Babor T et al. (forth com in g) No ordin ary com m odity: alcoh ol an d pu blic policy. Oxford, Oxford Un iversity Press.
Corrao MA et al., eds. (2000) Tobacco con trol: cou n try profiles. Atlan ta, GA, Th e Am erican Can cer Society.
Degen h ardt L et al. (2002) Com parative risk assessm en t: illicit dru g u se. Gen eva,
Table 1 .4 Percentage of total global mortality and DALYs attributable to tobacco, alcohol and illicit drugs, 2 0 0 0
Risk factor High mortality Low mortality Developed Worldwide developing countries developing countries countries
Males Females Males Females Males Females
Mortality
Tobacco 7 .5 1 .5 1 2 .2 2 .9 2 6 .3 9 .3 8 .8
Alcohol 2 .6 0 .6 8 .5 1 .6 8 .0 –0 .3 3 .2
Illicit drugs 0 .5 0 .1 0 .6 0 .1 0 .6 0 .3 0 .4 DALYs
Tobacco 3 .4 0 .6 6 .2 1 .3 1 7 .1 6 .2 4 .1
Alcohol 2 .6 0 .5 9 .8 2 .0 1 4 .0 3 .3 4 .0
Feren tzy P (2001) From sin to disease: differen ces an d sim ilarities between p ast an d cu rren t con cep tion s of ch ron ic dru n ken n ess. Con tem porary Dru g Problem s, 28:363–390.
Lop ez AD, Collish aw NE, Pih a T (1994) A d escrip tive m od el of th e cigarette ep idem ic in develop ed cou n tries. Tobacco Con trol, 3:242–247.
Mackay J, Eriksen M (2002) Th e tobacco atlas. Gen eva, World Health Organ ization . Med in a -Mora E et a l. (2001) Pa ttern s of a lcoh ol con su m p tion a n d rela ted p roblem s in Mexico: resu lts from two gen eral p op u lation su rveys. In : Dem ers A, Room R, Bou rgau lt C, eds. Su rveys of drin k in g pattern s an d problem s in seven developin g cou n tries. Gen eva, World Health Organ ization :13-32.
Mu rray CJ, Lop ez AD (1996) Global h ealth statistics. Global bu rden of disease an d in ju ry series. Vol. 2. Gen eva, World Health Organ ization .
Muston en H, Beukes L, Du Preez V (2001) Alcohol drin kin g in Nam ibia. In : Dem ers A, Room R, Bou rgau lt C, eds. Su rveys of drin k in g pattern s an d problem s in seven developin g cou n tries. Gen eva, World Health Organ ization :45-62.
Obot IS (2001) Hou seh old su rvey of alcoh ol u se in Nigeria: th e Middlebelt Stu dy. In : Dem ers A, Room R, Bourgault C, eds. Su rveys of drin kin g pattern s an d problem s in seven developin g cou n tries. Gen eva, World Health Organ ization : 63-76. Reh m J et al. (2002) Alcoh ol as a risk factor for bu rden of disease. Gen eva, World Health Organ ization , u n p u blish ed m an u scrip t.
Room R (2001) Govern in g im ages in public discourse about problem atic drin kin g. In : Heath er N, Peters TJ, Stockwell T, eds. Han dbook of alcoh ol depen den ce an d alcoh ol-related problem s. Ch ich ester, Wiley:33–45.
Room R et al. (1996) WHO cross-cu ltu ral ap p licability research on diagn osis an d assessm en t of su bstan ce u se disorders: an overview of m eth ods an d selected resu lts. Addiction, 91:199–220.
Room R et al. (2002) Alcoh ol an d th e developin g w orld: a pu blic h ealth perspective. Helsin ki, Fin n ish Fou n dation for Alcoh ol Stu dies.
UNODCCP (2002) Global illicit dru g tren ds 2002. New York, NY, Un ited Nation s Office for Dru g Con trol an d Crim e Preven tion .
World Ban k (1999) Cu rbin g th e ep id em ic: govern m en ts an d th e econ om ics of tobacco con trol. Wash in gton , DC, World Ban k.
WHO (1992) Th e ICD-10 classification of m en tal an d beh aviou ral d isord ers: cli n i ca l d escri p t i on s a n d d i a gn ost i c gu i d eli n es. Ge n e va , Wo r ld H e a lt h Organ ization .
WHO (1999) Global statu s report on alcoh ol. Gen eva, World Health Organ ization . WHO (1994) Lexicon of alcoh ol an d dru g term s. Gen eva, World Health Organ i-zation .
CHAPTER 2
Brain Mechanism s: Neurobiology
and Neuroanatom y
Introduction
Su bstan ce dep en den ce is a disorder th at in volves th e m otivation al system s of th e brain . As with an y disorder sp ecific to an organ or system , on e m u st first u n derstan d th e n orm al fu n ction of th at organ or system to u n derstan d its dysfu n ction . Becau se th e ou tp u t of th e brain is beh aviou r an d th ou gh ts, disorders of th e brain can resu lt in h igh ly com p lex beh aviou ral sym p tom s. Th e brain can su ffer m an y typ es of disease an d trau m as, from n eu rological con dition s su ch as stroke an d ep ilep sy, to n eu rodegen erative diseases su ch as Parkin son disease an d Alzh eim er disease, to in fection s or trau m atic brain in ju ries. In each of th ese cases, th e beh aviou ral ou tp u t is recogn ized as bein g p art of th e disorder.
Sim ilarly, with d ep en d en ce, th e b eh aviou ral ou tp u t is com p lex, b u t is m ostly related to th e effects of dru gs on th e brain . Th e trem ors of Parkin son disease, the seizures of epilepsy, even the m elan choly of depression are widely recogn ized an d accep ted as sym p tom s of an u n derlyin g brain p ath ology. Dep en den ce h as n ot p reviou sly been recogn ized as a disorder of th e brain , in th e sam e way th at p sych iatric an d m en tal illn esses were n ot p reviou sly viewed as bein g a resu lt of a disorder of th e brain . However, with recen t advan ces in n eu roscien ce, it is clear th at dep en den ce is as m u ch a disorder of the brain as an y other n eurological or psychiatric illn ess. New techn ologies an d research p rovide a m ean s to visu alize an d m easu re ch an ges in brain fu n ction from th e m olecu lar an d cellu lar levels to ch an ges in com p lex cogn itive processes, that occur with short-term an d lon g-term substan ce use. Th is ch ap ter reviews basic p rin cip les of brain an atom y an d fu n ction to p rovide a fram ework with in wh ich th e n eu roscien ce of dep en den ce can be discu ssed.
Organization of the brain
Th e region of th e b rain wh ere it m eets th e sp in al cord is called th e rh om ben cep h alon or h in dbrain , an d is com p osed of th e m yelen cep h alon (m edu lla) an d m eten cep h alon (p on s an d cerebellu m ) (Fig. 2.1). Th e m edu lla is vital to su stain in g life, an d con trols p rocesses su ch as breath in g, h eartbeat an d blood flow. Th e m edu lla also con tain s recep tors for th e op ioid dru gs, such as heroin an d m orphin e, which is why these drugs can cause respiratory dep ression an d death . Th e p on sis a relay station for sign als bein g carried from th e cortex to th e cerebellu m , wh ich is in volved inbody m ovem en ts an d coordin ation .
Fig. 2 .1 Central nervous system
Forebrain
Mid brain
Hindbrain Basal ganglia
Postcentral gyrus Central sulcus
Parietal lobe Frontal lobe
Temporal lobe Cerebral hemisphere
Diencephalon
Cerebellum Pons Medulla
Spinal cord
Cervical
Thoracic
Lumbar Sacral Precentral gyrus
Midbrain
Occipital lobe
Above th e h in dbrain is th e m esen cep h alon or m idbrain (Fig. 2.1), wh ich con tain s two areas th at are very im p ortan t in su bstan ce dep en den ce. Th e ven tral tegm en tal area (VTA) is rich in dop am in e cell bodies, an d p rojects to th e lim bic system an d forebrain region s. Th e VTA is in volved in sign allin g th e im p ortan ce of stim u li th at are critical to su rvival su ch as th ose associated with feedin g an d rep roduction . However, m an y p sychoactive drugs also have p owerfu l effects on th is brain area, wh ich con tribu tes to th e develop m en t of dep en den ce by sign allin g to th e brain th at p sych oactive su bstan ces are very im p ortan t from a m otivation al p ersp ective. Th e dop am in ergic p rojection from th e VTA to th e n u cleu s accu m ben s (discu ssed below) is kn own as th e m esolim bic dop am in e system , an d is th e n eu rotran sm itter system th at is m o st st ro n gly im p lica t e d in t h e d e p e n d e n ce -p ro d u cin g p o t e n t ia l o f p sych oactive dru gs (Wise, 1998). Th is key con cep t will be discu ssed in m ore d etail in Ch ap ters 3 an d 4. An oth er im p ortan t m id b rain stru ctu re is th e su bstan tia n igra, wh ich also h as dop am in ergic p rojection s to th e forebrain , bu t th ese p ath ways are in volved in coordin atin g an d execu tin g m ovem en ts of th e body. Degen eration of n eu ron s in th e su bstan tia n igra leads to th e ch aracteristic sym p tom s of Parkin son disease.
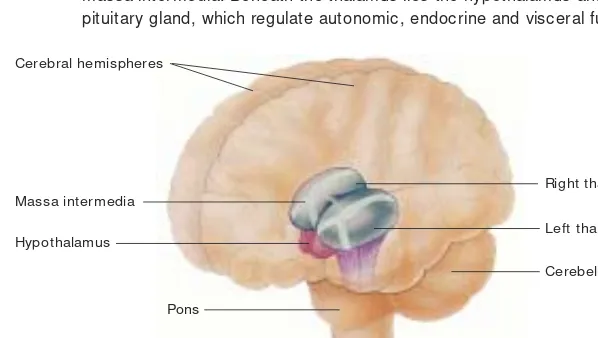
Fin ally, th ere is th e p rosen cep h alon or forebrain , wh ich is com p osed of th e dien cep h alon an d th e telen cep h alon (cerebral h em isp h eres) (Fig. 2.1). Im p o rta n t a re a s o f th e d ie n ce p h a lo n (Fig. 2.2) a re th e th a la m u s, th e h yp o t h a la m u s, a n d t h e p o st e r io r lo b e o f t h e p it u it a r y gla n d . Th e h yp oth alam u s is critical for regu latin g h orm on al sign als an d basic bodily
Fig. 2 .2 Diencephalon
The figure shows the location of the two lobes of the thalamus, joined by the massa intermedia. Beneath the thalamus lies the hypothalamus and posterior pituitary gland, which regulate autonomic, endocrine and visceral functions.
Massa intermedia
Right thalamus
Left thalamus Hypothalamus
Cerebellum
Pons
fu n ction s – con cern in g, for exam p le, water balan ce, body tem p eratu re an d rep rod u ctive h orm on es – as well as for resp on d in g to ch an ges in th ese fun ction s. The hypothalam us also secretes horm on es that travel to the n earby posterior lobe of the pituitary glan d. The thalam us fun ction s as a relay station for sen sory an d m otor in form ation goin g to an d from the cortex to other areas of th e brain an d body.
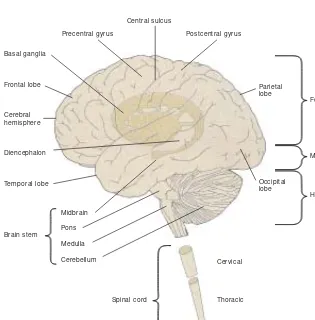
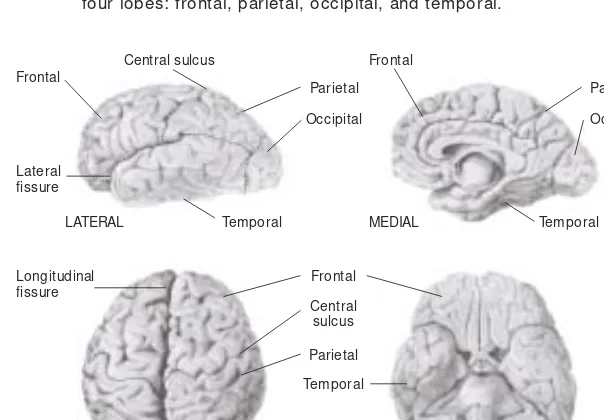
Th e telen cep h alon of th e forebrain is th e m ost h igh ly develop ed area of th e brain , an d is com p osed of two cerebral h em isp h eres sep arated by th e lon gitu din al fissu re (Fig. 2.3). Th e ou term ost layer of th e brain is th e cortex, wh ich is m ade u p of layers of n erve cells or n eu ron s, an d h as a h igh ly folded organ ization th at in creases its su rface area an d th e n u m ber of n eu ron s th at it con tain s. Ben eath th e cortex ru n m illion s of axon sth at in tercon n ect th e n eu ron s an d allow th e differen t areas of th e brain to com m u n icate an d to coordin ate beh aviou r.
Each h em isp h ere of th e brain is divided in to fou r lobes: fron tal, p arietal, tem p oral, an d occip ital (Fig. 2.3). Differen t areas of th e cortex are sp ecialized for differen t fu n ction s (Fig. 2.4). Th e m otor association cortex, for exam p le, is in volved in coordin atin g m ovem en ts of th e body, an d th e p rim ary m otor
Fig. 2 .3 Cerebral hemispheres
The telencephalon is composed of two cerebral hemisphere separated by the medial longitudinal fissure. Each hemisphere is subdivided into four lobes: frontal, parietal, occipital, and temporal.
Frontal
Central sulcus
Parietal Occipital
Lateral fissure
LATERAL
Longitudinal fissure
MEDIAL
Parietal
Parietal Occipital
Frontal
Temporal
Temporal Frontal
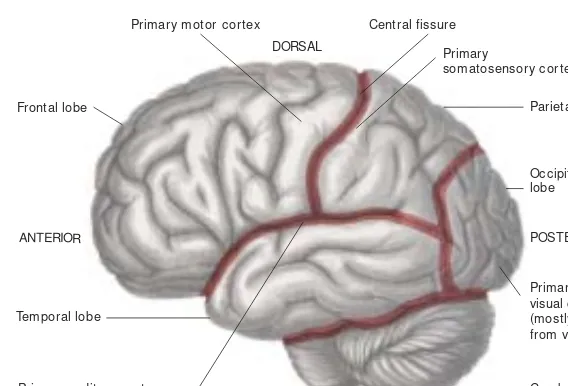
cortex is in volved in execu tin g th is fu n ction . Sim ilarly, th ere is a p rim ary sen sory cortex th at receives in form ation from each of th ese sen se organ s. In form ation from the prim ary sen sory areas goes to sen sory association areas of th e cortex, wh ich are in volved in p ercep tion an d m em ory con n ected with th e sen se o rga n s. Here in fo rm a tio n fro m severa l sen se o rga n s ca n b e com bin ed to form com p lex p ercep tion s (Fig. 2.5). Th e cortex is in volved in m a n y a sp e ct s o f su b st a n ce d e p e n d e n ce, fro m t h e p rim a r y e ffe ct s o f psychoactive drugs on sen sation s an d perception s, to the com plex behaviours an d th ou gh ts in volved in d ru g cravin g an d u n con trolled su b stan ce u se. Neuroim agin g techn iques such as positron em ission tom ography (PET) have sh own ch an ges in areas of th e cortex followin g both sh ort-term an d lon g-term su bstan ce u se (see Box 2.1 an d Ch ap ter 4 for details).
Ben eath the cortex are several other im portan t structures. The basal gan glia (Fig. 2.6) are stru ctu res in volved in volu n tary m otor beh aviou r an d con sist of th e caudate, p utam en , globus p allidus an d am ygdala (th e am ygdala is also p art of th e lim bic system , an d will be discu ssed in th e n ext section ). Th e cau date an d p u tam en togeth er are kn own as th e striatu m . Ju st below th e striatu m is a key area for su bstan ce dep en den ce an d m otivation , kn own as
Fig. 2 .4 Structural and functional regions of the cerebral cortex
The cerebral cortex is structurally differentiated into four lobes. The cerebral cortex can also be differentiated into functionally specialized areas.
Source: Reproduced from Carlson, 1 9 8 8 , with permission from the publishers.
Central fissure
DORSAL Primary
somatosensory cortex
POSTERIOR
Primary visual cortex (mostly hidden from view) Frontal lobe
Temporal lobe ANTERIOR
Cerebellum Primary auditory cortex
(mostly hidden from view)
Primary motor cortex
accu m b en s is a very im p ortan t b rain area in volved in m otivation an d learn in g, an d sign allin g th e m otivation al valu e of stim u li (Robbin s & Everitt, 1996; Cardin al et al., 2002). Psych oactive su bstan ces in crease th e p rodu ction
Fig. 2 .5 The relation between different functional brain regions
Information received from primary sensory cortices is integrated in sensory association areas, which are involved in perception and memories.
Source: Reproduced from Carlson, 1 9 8 8 , with permission from the publishers.
Fig. 2 .6 Basal ganglia
The basal ganglia are shown, comprised of a number of structures involved in the performance of voluntary motor responses.
Source: Reproduced from Pinel, 1 9 9 0 , with permission from the publishers. Frontal lobe
Primary motor cortex
Execution of movement
Parietal lobe
Perception of space location of limits
Auditory information and memories Plane for
movement
Visual perception Occipital lobe
Temporal lobe
Right globus pallidus
Head of caudate
Left globus pallidus
Left putamen
Left amygdala Two lobes of thalamus