COMPARISON OF SUCCESSFUL PREGNANCY RATE BETWEEN
FLEXIBLE AND RIGID CATHETER IN INTRA UTERINE
INSEMINATION
Rusda M, Halim B, Kaban YB, Sahil MF, Efendi IH, Barus RC
Fertility, Endocrinology and Reproductive Division – Departement of Obstetric and Gynecology Medical Faculty – Universitas Sumatera Utara
Medan, Indonesia, October 2013
INTRODUCTION
Background
At present, many couples
presenting with fertility problems seek
advice for subfertility. Some of these
couples will undergo intrauterine
insemination (IUI) or artificial
insemination (AI). In spite of the
success with newer and more
sophisticated assisted reproductive
technique (ART). IUI remains the
recommended treatment for couples
with unexplained subfertility. The
rationale for this is that IUI is a
successful low cost alternative when
compared to the more advanced
fertility treatments such as in-vitro
fertilisation (IVF) and intracytoplasmic
sperm injection ( ICSI ). The costs of
IUI are considerably lower, the
pregnancy rates are similar and the
procedure is less stressful and
invasive compared to IVF and ICSI.
In a systematic review of
embryo transfer ( ET ) catheters, the
softness of the catheters was found to
be a determining factor in the success
of ET procedure. It is still unclear but it
is presumed to be associated with
reduced traumatic effects of flexible
catheter during introduction of the
embryo into the uterine cavity. Number
of cycles in which blood on the
catheter tip is present to examine if
there is a difference in traumatic
effects among flexible and rigid
catheters.
In the other hand, the impact of
the choice of IUI catheter on the
treatment outcome has been poorly
investigated and data comparing
different types of IUI catheters are
limited. The aim of this study is to
evaluate comparison of succesful
pregnancy rate between flexible and
rigid catheter in intra uterine
Methods
The study design was an
analytic observational with cohort
study design to evaluate the
comparison of succesful pregnancy
rate between flexible and rigid catheter
in intra uterine insemination were
performed at the Halim Fertility Centre
and Stella Maris – Women and
Children Hospital in Medan from July
until September 2013. The samples
were all patients seeking treatment
who undergo intra uterine
insemination. All patient than got
ovarian stimulation before intra uterine
insemination was taken. Analysis
between variables was conducted
using chi square to measure
proportion, p- value under 0,05 is
consider as statistically significance
results.
Results
There is no difference between
age group of women who undergo
intra uterine insemination using flexible
or rigid catheters, 30.90 +
Montanaro et al in 2001 through
a retrospective study over 5.5 years
with 273 cycles IIU get women aged
<35 years is a good predictor for the
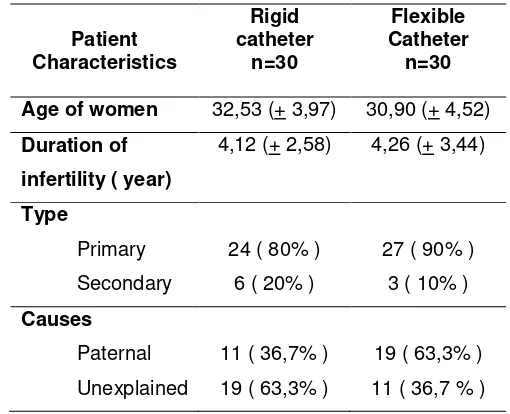
successful rate of the IIU. there was no
difference in duration of infertility
between the two groups. Male factor is
the most cause of infertility in the rigid
catheter group, while unexplained
factor is the most cause in unexplained
factor.
4.52 year
and 32.53 + 3,97 year, respectively.
Table 1. Patient’s Characteristics
Patient
Duration of infertility ( year)
4,12 (+ 2,58) 4,26 (+ 3,44)
The table above also shows
that the type of infertility couples who
get IIU in both groups generally
primary infertility, 24 people (80%) in
the rigid catheter group and 27 people
(90%) in flexible catheter group.
Table 2. Insemination cycle’s
characteristics
Folicle and Endometrium
Number of folicle
folicle
Endometrial thickness
Both groups have the number of
follicles with a diameter of more than
17 mm, each 23 patients (76.7%) in
the rigid group and 22 patients (73.3%)
in the flexible catheter. Farimani et al
in 2007 suggested that from 463
cycles done, the average of the
follicles> 16 mm is a good predictor
associated with increased rate of
pregnancy.
Endometrial thickness in both
groups had a mean consecutive 8.47 ±
1.77 cm at rigid catheter group and
8.63 ± 1.97 cm in flexible catheter
group. Teraporn et al in 2003 got cut
off <7.5 mm of endometrial thickness
is a good predictor for the success of
intrauterine insemination.
Number of sperm used in the
two groups both rigid catheter group
and a flexible catheter are 11.29 x 106
± 8.11 sperms and 12.04 x 106± 8.72
sperms. Based on a retrospective
study in 893 IIU cycle conducted by
Khalil et al in 2001 found that the
number of motile sperm used in IIU
more than 2 x 10 6
Table 3. Factors encountered during
insemination
related with
increasing success rate of IIU.
Factors catheter tip
Yes
The table above shows that
there are no complications found in
catheter failure in both study groups.
This suggests that both types are
relatively easy to perform insertion.
Blood on the catheter when
removed from the uterine cavity are
found more on the rigid catheter group
18 (60%) than flexible catheter, 17
(56.7%). Statistically, the Chi-square
test value is p> 0.05, which indicates
no significant differences between the
two groups in terms of the presence of
blood in the catheter after the
the possibility of injury to the
endometrium at the time of the
procedure.
Cramps / abdominal pain
subjectively assessed in the procedure
occurred in 13 cases (43.3%) with a
rigid catheter, more than on a flexible
catheter which is 9 cases (30%). But,
there is no statistically significant
difference between two groups.
Reflux during insemination
procedure might affect the success of
the IIU. In this study, reflux is more in
rigid catheter group of 8 persons
(26.7%) while 1 in the flexible group
(3.3%). Chi-square test obtained p
value <0.05 indicating there is
significant difference between the two
groups in terms of the occurrence of
reflux after the procedure IIU. This
might be due to rigid catheter has a
smaller diameter than the flexible
catheter, where the larger diameter of
the cervix can accommodate patients
who can prevent reflux.
Table 4. Successful pregnancy
during IIU
Pregnancy
n = 30 total p- value Positive Negative
Types of
** p-value measured with Continuity correction test
Intrauterine insemination
success rates in flexible catheter group
was higher (26.7%) compared with the
rigid catheter group (20%), but from
the statistical test obtained by
Chi-square, p-value = 0.542, showed no
significant difference in terms of the
level of pregnancy success between
the two catheters. Similar with
Teraporn in 2003, of 239 cycles
performed found no statistically
significant difference in the success
rate of insemination both rigid and
flexible catheter with a p value = 0.714.
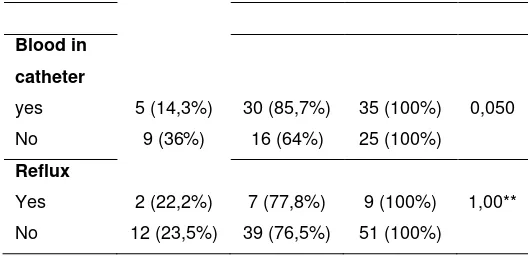
Failure rate in cases with
intrauterine insemination catheter
containing blood is higher (85.7%)
compared with cases that not contain
blood (64%), but from the statistical
test obtained by Chi-square p-value =
0.050, which showed no difference in
terms of the success rate of pregnancy
among catheters that cause bleeding.
The failure rate in the case of
sperm reflux were similar in both
groups with p-value obtained
Correction Continuity test = 1.00,
showed no significant difference in
pregnancy success rates between the
catheter and the incidence of reflux.
We can concluded that the
success rate of intrauterine
insemination in flexible catheter group
was higher (26.7%) compared with the
rigid catheter group (20%), yet the
statistic measured obtained by
Chi-square p value> 0.05, which indicates
no significant difference in pregnancy
success rates between the two
catheters.
Discussion
One aspect on FERT attention
recently is a matter of the use of a
catheter in the insemination process.
Several previous studies on flexible
catheter for embryo transfer can
improve the success of the embryo
transfer. It is still unclear why, but
theoretically associated with the
incidence of trauma to the endometrial
lining, which flexible catheter may
reduce trauma at the entry time of the
embryo into the uterine cavity
compared with a rigid catheter.
In the other hand, there is no
significant difference of the success
rate of pregnancy among two
catheters, not only in terms of there is
bleeding or reflux happened during
procedures. Perhaps this because
after the IIU, sperm is known reached
the peritoneal cavity rapidly, but the
implantation of the embryo in the
uterus occurs about 7 days after
fertilization. In contrast of embryo
transfer, embryo before implantation
will float or stick to the wall with
endometrial adhesions are not strong
in a few days (embryo transfer second
or third day) or within 1 day of
implantation (day 5 embryo transfer or
6). Therefore, the average will
decrease if embryo transfer catheter
directly damage the embryo and / or
endometrium or if the embryo get out
through the cervix or fallopian tubes.
However, we expected the
clinician to consider uncomfortable
aspects of a rigid catheter although
there was no difference of successful
pregnancies.
REFERENCE
1. Stephen, E.H. and A. Chandra.
Use of infertility services in the
United States. Family Planning
Perspective, l32: 132-137:2000
2. Abou Setta AM, Al Inany HG,
Mansour RT, Serour GI,
embryo transfer catheters for
assisted reproduction: a
systematic review and
meta-analysis.Human Reproduction
2005;20(11):3114–21.
3. Voorhis, V., A.F. Sparks and
B.D. Allen. Cost effectiveness of
infertility treatment. Fertile.
Steril., 67: 830-860. ISBN:
1749-6632; 1997.
4. Abdelkader, A.M. and J. Yen.
The potential use of intrauterine
insemination as a basic option
for infertility. Rev. Technol. Int.
11: 609-622; 2009.
5. Andersen, A.N., V. Goossens
and A.P. Ferraritti,. Assisted
reproductive technology in
Europe hum. Report, 23:
756-771. 2008.
6. Pandian Z, Bhattacharya S,
Vale L, Templeton A. In vitro
fertilisation for unexplained
subfertility. Cochrane Database
of Systematic Reviews 2005,
Issue 2.
7. Steures P, van der Steeg JW,
Hompes PG, Habbema JD, et
al. Intrauterine insemination
with controlled ovarian
hyperstimulation versus
expectant management for
couples with unexplained
subfertility and an intermediate
prognosis: a randomised clinical
trial. Lancet:2006;368:216–221.
8. TerapornV., Sreshthaputra,O et
al.Comparison of Tom Cat
and PIVET Catheter for
Intrauterine Insemination:Thai
Journal of Obstetrics and
Gynaecology December 2003,
Vol. 15, pp. 223-229.
9. Karen L, Smith, R. Daniel.Does
Catheter Type Effect Pregnancy
Rate in Intrauterine
Insemination Cycles?:Journal of
Assisted Reproduction and
Genetics, Vol. 19, No. 2,
February 2002.
10. Kamil.N, Mohammed B.Efficacy
of Intra Uterine Insemination in
the Treatment of
Infertility:American Medical
Journal 2 (1): 47-50, 2011.
11. Cohen MR. Intrauterine
insemination.Int J Fertil
1962;7:235–240.
12. Zegers-Hochschild F, Nygren
KG, Adamson GD, et al.On
behalf of The International
Committee Monitoring Assisted
Reproductive Technologies.
The ICMART glossary on ART
terminology.Hum Reprod
2006a;21:1968–1970.
13. Andersen AN, Gianaroli L,
reproductive technology in
Europe, 2001. Results
generated from European
registers by ESHRE. Hum
Reprod2005;20:1158–1176.
14. Bensdorp AJ, Cohlen BJ,
Heineman MJ,et al. Intra
Uterine Insemination for male
subfertility. Cochrane Database
Syst Rev;2007.
15. Andersen AN, Gianaroli L,
Felberbaum R, de Mouzon J,
Nygren KG.Assisted
reproductive technology in
Europe, 2001. Results
generatedfrom European
registers by ESHRE. Hum
Reprod2005;20:1158–1176.
16. ESHRE Capri Workshop Group.
Intrauterine Insemination.
Human Reproduction Update,
Vol.15, No.3 pp. 265–277,
2009.
17. Andersen AN, Goossens V,
Ferraretti AP, et al, The
European IVF monitoring
(EIM)Consortium, for the
European Society of Human
ReproductionEmbryology
(ESHRE). Assisted reproductive
technology in Europe,2004:
results generated from
European registers by ESHRE.
HumReprod2008;23:756–771.
18. Aboubakr M.Insemination
intrauterine:Middle East Fertility
Society Journal;Vol. 9, No. 2,
2004.
19. Boomsma, C.M., M.J.
Heineman and B.J. Cohlen.
Semen preparation techniques
for intrauterine insemination.
Cochrane Database Syst. Rev.
nm7: 1223-1235; 2007.
20. Van Voorhis BJ, Barnett MR,
Sparks AE, et al. Effect of the
total motile sperm count on the
efficacy and cost effectiveness
of intrauterine insemination
andin vitro fertilization. Fertil
Steril2001;75:661–668.
21. Duran HE, Morshedi M, Kruger
T, Oehninger S. Intrauterine
insemination: a systematic
review on determinants of
success. Human Reproduction
Update 2002;8(4):373–84.
22. Van Weering HGI, Schats R,
McDonnell J, et al. The impact
of the embryo transfer catheter
on the pregnancy rate in IVF.
Hum Reprod 17,666–670; 2002.
23. McDonald JA and Norman RJ.
A randomized controlled trial of
a soft double lumen embryo
transfer catheter versus a firm
single lumen catheter:
pregnancy rates. Hum Reprod:
2002;17,1502–1506.
24. Lavie O, Margalioth EJ,
Geva-Eldar T, et al. Ultrasonographic
endometrial changes after
intrauterine insemination:
Technical aspects of
intrauterine insemination
catheters :The Cochrane
Collaboration. parison of two
catheters. Fertility and Sterility
1997;68:731–4.
25. Smith KL, Grow DR, Wiczyk
HP, et al. Does catheter type
effect pregnancy rate in
intrauterine insemination
cycles? J Assist Reprod Genet
19,49–52; 2002.
26. Miller PB, Acres ML, Proctor
JG, et al. Flexible versus rigid
intrauterine insemination
catheters: a prospective,
randomised, controlled study.
Fertil Steril 83,1544–1546;
2005.
27. Ragni G, Alagna F, Brigante C
et al. GnRH antagonists and
mild ovarian stimulation for
intrauterine insemination: a
randomized study comparing
different gonado-trophin
dosages. Hum Reprod 19,54–
58. 2004.
28. Fancovits et al, Catheter type
does not effect the outcome of
intrauterine insemination
treatment: prospective
randomized study. Fertil Steril
83,699-704: 2005.
29. Cantineau AEP, Heineman MJ,
Cohlen BJ. Single versus
double intrauterine insemination
(IUI) in stimulated cycles for
subfertile couples. Cochrane
Database Syst Rev 2003.
30. WHO.Examination and
processing of human semen,
WHO laboratory manual 5th
31. “Intrauterine Insemination.” In
Vitro Fertilization IVF,Web.21
Mar 2011. edition:164-165; 2010.
32. Reproductive Medicine and
Infertility Associates,
“Intrauterine Insemination
Section”: 3-5; 2010.
insemination
.html>.
33. Farimani M, Amiri I. Analysis of
Prognostic Factors for
Successful Outcome in Patients
Undergoing Intrauterine
Insemination. Acta Medica
34. van der Poel N, Farquhar C,
Abou-Setta AM. Soft versus firm
catheters for intrauterine
insemination. Cochrane review:
2010
35. Schoolcraft WB, Surrey ES and
Gardner DK. Embryo transfer:
techniques and variabels
affecting success. Fertil. Steril
76,863–870:2001.
36. NICE guideline Fertility:
assessment and treatment for
people with fertility problems.
Clinical guideline 11. National
Institute for Clinical Excellence,