84
Parida et aI Med J IndonesThe review
of
the patterns of presentation
and
various prognostic factors
in
male
breast cancer patients
Dillip
Kumar
Parida, Navneet SinghMajhail,
GouraKishore
Rath, PramodKumar Julka
Abstrak
Tujuan srudi ini adalah untuk mempelajari tampilan, gejala, berbagai faktor prognostik dan modalitas terapi dalam penatalal<sanaan kaiker payudara pada
pria.
Tiga puluh kasus kanker payudarapria
telah diobati dengan radioterapidi
bagian knmi anîara tahunlg83-l9gi.
S"^uà penârrita selain pembedahan, mendapat radioterapi (26) dan kemoterapi (12). Mastektomi radikal dilakukan padalg
penderita, sedàngkan6
pendeiita menjalani mastektomi radiknl yang dimodifikasi dan 2 pasien dengan mastektomi biasa' Raàioterapi pascabedah diberikan dengan dosis 50 Gy dalam 25 fraksi selama lima minggu. Kemoterapi diberikan sebagai ajuvan. Selainitu
sàmua pasienjuga
mendapat terapi hormonal Empat pasien hilang dari follow-up. Follow-up dilakukan selama 10-92 bulan dengan*râio,
38 bitan. Angia bebas penyakit 2 dan 5 tahun berturut-turut adalah 87,7 dnn 54,67Vo. Satu pasien mengalami kekambuh-an lokal, sementara 5 poiien mengalami metastasis. (Jsia, status kelenjar limfe dan metastasis merupakan faktor prediktor yang penting. Saatini,
,*u*nyo
kanker payudarapria
diobati seperti kanker payudara wanita sesuai dengan stadium masing-masing. Diperluknn studi acakyang lebih besar untuk optimalisasi pendekatan terapi. (Med J Indones 2001; 10: 84-7)Abstract
This
stu^dy was aimedto
analyze the patternsof
presentation, various prognostic factors and therapeutic modalitiesfor
themanagem,nt of breast cancer in male patients. Thirty cases of male breast cancer were treated with radiotherapy 4t our department betvveen 1983 and 1997. AIt the patients were treated
with
radiotherapy besides surgeryQ6)
and chemotherapy (12). Radical mastectomy was performed in I8 patients, while 6 patients were treated with modified radical mastectomy and 2 patients withsiwle
mastectomy.Thi
post operative radiotherapy was appLied"at the dose of 50 Gy
in
25 fractions over a period offive
weeks.. The chemotheiapy was administered in an adjuvant setting. AII the patients were received hormonal therapy. Four patients were lost tofollow
up. iùe fottow up period rangedfrom
10-92 months with a median of 38 months. The disease-free suwival at 2 and 5 years were 87.7Vo and 54.67Vo, respectively. One patient recurred locally, whereas 5 patients had distant meîastasis. The age, lymph node status at presentation and piesence of distant metastasis were the important prognostic T(tctors. At present, the trend is to treat male breast cancer patientslike
those of females stageper
stage. More randomized studiesare
requiredfor
optimizing therapeutic approach. (MeiI J Indones 2001; 10: 84'7)Keywords: male breast cancer, radiotherapy, chemotherapy, surçery
The incidence
of
male
breastcancer is
less common than thoseof females. It forms
lessthan
lVoof
all the
cases seenat most
of
the centers. The
age
adjustedincidence
rates
are 0.3
per 100,00
population
according
to
1989Delhi
&
Mumbai
cancer registries,while
female breast cancer tops the
list of female
malignancies
in
both
registries.r
The
1995 Delhi
cancerregistry
shows adefinite
increasing trendin
thecrude and age adjusted rate
of
male breast cancer (0.4and
0.7
respectively),
while that
of
female
breastcancer
are 18.3
and 27.7,respectively.
Becauseof
thelow
incidence
of
male breast cancer and
lack
of
Department of Radiation Oncology, AII India Institute
of
Medical Sciences, New Delhi, India 110029clinical trials there
areno definite guidelines
exist
asto achieve
optimum therapeutic
result. But the
trendworldwide
is to managelike
a female breast cancer.METHODS
Vol 10, No 2,
April-
June 2001overall
and disease-freesurvival
analysis and univariate analysisofprognostic
factors were carried out.RESULTS
Age
range
wasbetween 40-70
yearswith
the
medianof 60
years.The majority
of
patients
(23130)were in
the range of
40-70
years.
The
duration
of
symptoms rangedfrom
1-36months
(averaged 6 months). Breastlump was
present
in
all
patients besides
pain
(17),nipple
discharge
(8), retraction
of
nipple,
ulceration
(6)
and peau
d'orange (3). The
lump
was present in
the upper outer
quadrant
(14), upper inner
quadrant(8)
andcentral
mass(8). The
sizeof
thetumor
variedfrom 0.5
to
8
cm.
Palpable lymphadenopathy at
presentation was
found
in
18patients out
of which 16
had
axillary
nodes and2
with
supraclavicular
as well as axillary nodes.No
patient had any
family
history
of
breast
cancer,previous
exposedto
radiation,
estrogenicdrug
intake, orchidectomyor
Klinefelters
syndrome. Gynaecomastiawas found
on
examination
in 6 of
the 30
patients.Besides
routine
haematological evaluations
all
thesepatients had
fine
needle aspiration
cytology (FNAC)
and
histopathological study
of
the surgicopathologicâl
specimen
for
confirmation
of
diagnosis.
In all
thecases
FNAC
had
shown positive diagnosis
which
later
on
was corroborated
by
the histopathological
findings.
The common surgical
procedure wasradical
mastectomywhich
wasperformed
in
18 cases while 6had
modified radical
mastectomy,
and2
had
simplemastectomy.
Four
patients
did not had any
surgery.Infiltrating duct
carcinoma
was
the
most
commonhistological type
followed
by intralobular variety.
Theover all
TNM
statusis
describedin
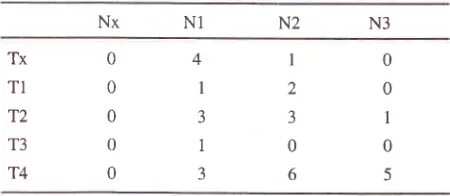
detail in table
l.
Most
of
the
tumors presented
in
advanced stage
(20/30). The
commonest
pattern
of
failure was
thedistant
metasi,asiswhich is
elaboratedin
table 2.
Onepatient recurred
locally.
All
the
patients
receivedadjuvant hormonal treatment. However 12
patientshad combination
chemotherapy.
The
chemotherapyregimens consisted
of
cyclophos-phamide, methotraxate,5FU, epirubicin, paclitaxel,
docetaxel either single
orvaious combinations.
Seven patients reéeivedCMF,
5received
CEF, paclitaxel
in
3
and docetaxel
in
2patients.
The
second
line
chemotherapy
wasadministered
in
l0
out of
12 patientswho failed
to thefirst
line
chemotherapy.Twenty
four
patients receivedradical loco-regional radiation
therapy
while the rest
were treated
palliatively.
The institute protocol of
postoperative radiotherapy
is
to
deliver
50 Gy
in
25Male breast
cancer
85fractions over a period
of five weeks.
The
radiation
planning
is
doneunder
a
simulator
andthe
treatmentis
executed
by
either
a
tele-cobalt
or
high
energylinear
accelerator
after
3
weeks
of
surgery.
Patientshaving symptomatic
metastasis
were
managed
with
palliative radiation
therapy and
combination
chemo-hormonal
therapy.Table
l.
TNM stage distribution of the patientsTx T1 T2 T3 T4 N3 N2 NI Nx 0 0 0 0 0 4 I J 1 3 I 2 3 0 6 0 0 I 0 5
Table 2. Patient prohle
Total no patients analysed : 30
Age distribution :
< 40 years
40-50 years 50-60 years
50-60 years
>70 years
Symptoms: Painless lump Nipple discharge Retracted nipple Retracted nipple Ulceration Pe-u-de orange
Surgery:
Simple
mastectomy
:2
Modified radical
mastectomy
: 6Radical
mastectomy
: 18Radiotherapy (post-op):
Chest wall
only
: 6Chest wall + SCF +
Axilla
: 3Chest wall + SCF + Axilla + IMC : 15
Failure pattem :
Locally
: 1 Locally + Distant :2 Distantonly
'.3IMC : Internal mammary chain, SCF : Supraclavicular fossa
The
follow
up period
rangedfrom l0-92
months
with
a median
of
38 months. Four patients were lost
tofollow
up.The
axillary
lymph
node status, presenceof
distant
metastasis at presentation
and age were
the [image:2.612.305.530.197.295.2]86
Parida et alimportant prognostic factors
found
to
affect
theactuarial
diseasefree survival.
DISCUSSION
The
oldest
patient
in
our
serieswas
of
79
years old.The
mean age atpresentation
in
men
has beenfound
to
be 6-11
yearsmore than women. The
mean ageof
the
female patients suffering
from
breast
cancercoming
to
our
centre was 46.8years
with
the rangeof
22-'70
years.
Scheike
et
al"
have
reported
that gynaecomastia,either
clinical or
microscopic
is
often associatedwith
male breast cancer.
But
till
today
nodefinite
correlation
has
been established
betweenthem. Olsson
&
Ranstamu
haue
tried
to
corelatehistory
of
head
injury
and
development
of
breastcancer
in
male.
We
have
recorded
this
history
in
eleven (36Vo) patients.
The higher
incidencein
theleft
breast
than
right is usually
observedbut
the
cause isvery
difficult
to
establish.
We
had 14
left
breastcancers cases
vs
16right
breasttumors
in
our
series.Many
studies
report that
painless breast
lump is
theusual presenting feature
which was
observed
in
our analysis.a'sMost
of
the
patients
(14)
presentedwith
T4
lesions showing
that
the
tumor
in
male
very
quickly
involves
theskin
evenif
theT
sizeis
small.It
is
already
documented
that
males present
in
a
late stagethan
females.
Borgen
et
al6 have reported
theincidence
of
early
breastin
male patients cango
up to the tuneof
'77Vo.Surgery remains
the
mainstay
modality
of
treatment.Radical
mastectomy
(RM)
is
the
cornmonestprocedure
at
our
institution. However
modified
radical mastectomy
(MRM)
is commonly practiced in
western countries.
Radiation
therapy
is
the
principal
adjuvant
modality
besides
chemo
and
hormonal
therapy.
Post
operative
radiation therapy
hasdefinitely improved the
loco-regional recurrence
rateand
ultimately
diseasefree survival.o't
[n
our
seriesall
the
patients received radiation therapy
(24-posrop,
6-Palliative). Crichlow
&
Galta have recommended thatthe internal
mammary
chain
should
be
treated
in
all
cases,
as
the
tumors
are
mostly centrally
locatedresulting
a
high
chance
of
their involvement.
Only
one
patient
recurredlocally in
our
series.Chemo
andhormone therapy
is
usedin
nodepositive
cases.
In our
seriesall
the patientsreceived hormonal
therapy
in
the form
of
tamoxifen. However
therelative
role
of
tamoxifen have
not
been
defined.Ribeiro
&
Swindell8
have shown asignificant survival
Med J Indones
advantage
in
the
patients treated
with
tamoxifen"
Many
studies havealso shown
abenefit
in
over
all
aswell
as diseasefree survival
in
the
patients
receivedadjuvant
chemotherapy.6'eReceptor status
is
also
animportant predictor
of
hormonal
therapy,which play
agreater
role in
caseof
nodepositive
patients.As
in
our
center,
majority
of
patients
presentsin
anadvanced stage,
neo adjuvant therapy may have
asignificant
role
in
the
management.
Eight
patients received neoadjuvant
chemotherapy.The
disease freesurvival
rates
at
2
yearsand
5
years
were
87.7Vo&
54.6Vo.Borgen et
aloreported
5 yearsover
all
&
DFSof
85Vo
&.
68Vo
respectively. Whereas
Engin
andUnsallo reported a 5 year
overall
&
DFS
of
37 &.27Vorespectiveiy.
In a
collective review, Crichlows
hasreported
a
5
year overall survival rate
of
49Va.The
outcome
of
male
breast cancer
is
improving over
aperiod
of
time
with
availability
of
newer chemotherapeutic agents,quicker
diagnosis and aboveall,
increased
sense
of
awareness
on
the part
of
patients.
On univariate analysis,
the
age
atpresentation,
axillary
lymphnode
statusand
presenceof
distant
metastasis
at
presentation
were found
toinfluence the DFS significantly
in
our
series. Many
literatures show
axillary
nodes as
the
single
mostimportant
prog
breastcanc"r.t'"
A
re
ositive
nodes
DFS
has
et
al.r2In
our
study the node negative patientsfaired better
asregards
to the survival
(med
DFS 57 mo)
than
nodepoiitiu"
patients (med DFS
48
mo). Adami
et
alrr have reportedthe
adverseeffect
of
ageon the overall
outcome.
Engin
&
Unsalro have alsofound
that
when thepatient
is
more than60
yearsof
age the prognosisis
badwhen compared to the patients
of
lessthan
60 years.In
our
series,patients below 50 years
of
agehad a shorter DFS.
In
India, unlike female
patients
with
breast
cancer,male patients usually
present
in
an
advanced
stagewhich
influence tha
treatmentpolicies. The
mean agefor
these patients
is
about
10
years
less than
thepatients
in
west.
Stage
for
stage,
the
current
management
of
male
breast cancer
in
generally
similar
to
that
of
female breast cancer except
breast cancer conservatlon.REFERENCES
8
9
10
ll
3
VoI 10, No 2, April
-
June 20012.
Scheike O, Visfeld J. Male breast cancer; Gynaecomastiain
patientswith
breast cancer. Acta pathol MicrobiolScand 1973;81:359-65.
Olsson
H,
RanstamJ.
Head trauma and exposure toprolactin elevating drugs as risk factors for male breast cancer. J Natl Cancer Inst 1988; 80:679-83.
Crichow RW,
Galt
SW. Male breast cancer. Surg ClinNorth Am, 1990:70: 1165-77.
5.
Crichow
RW.
Carcinomaof the
male
breast. SurgGynecol Obstet 1972; 134:1019.
Borgen PI, Wong GY, Vlamis V et al. Current
mar.ragement
lZ.of male breast cancer.
A
reviewof
104 cases. Ann Surg1992';215:451-9.
Patel HZ, Buzdar
AU, Hortobagyi GN. Role
of adjuvant therapy in male breast cancer. Cancer 1989; 64:1583-5.Male breast
cancer
87Ribeiro
G,
SwindellR.
Adjuvant tamoxifenfor
malebreast cancer (MBC). Br J Cancer 1992;65:252-4.
Bagley
CS,
WesleMN,
Young
RC,
Lippman ME.
Adjuvant chemotherapy
in
maleswith
cancerof
thebreast. Am J Clin Oncol 1987; l0:55-60.
Engin K, Unsal M. Cancer of the male breast. The Turkish
experience. J surg Oncol 1993;53:128-32.
Adami HO, Hakulinen
T, Ewertz
M
et al. The survivalpattern in male breast cancer. An analysis of 1429 patients
from the Nordic countries. Cancer 1989; 64:1171- -82. Guinee VF, Olsson H, Moller
T
et al. The prognosis ofbreast cancer
in
males.A
reportof
335 cases. Cancer1993;7 l:154-61 .
6