VoL7, No 3, July - September 1998
Endoscopic management of bile leaks
after
L.A.
LesmanaEndoscopic managementfor biliary
leaks
l6l
laparoscopic cholecystectomy
Abstrak
Kebocoran empedu didapatkan pada sebelas clari 16
Kebocoran terjadi di duktus sistikus pada 9 pasien dan di duktus
metode endoskopi. Terapi endoskopik meLiputi pemasangan stent
P
obilier untuk drainase pada 3 pasien.k
4 prosedur tersebut. Endoskopi terapep
Abstract
c t inj urie s fo I low in g raparo s c op ic c ho re cy s te c to my. Le ak o c c ur re d by various endoscopic methods. nts, and insertion of nasobiliary significant compLications of the
Keywords : Endoscopic therapy - biliary reaks - Iaparoscopic chorecystectomy
INTRODUCTION
return to
work.
However,
biliary
complications after LC,
noticeable
bile duct
leaks,
is reported from
O.3Voto
3.0Vo com_Several studies have
shown
theeffectiveness
of
endo_scopic sphincterotomy
alone
or
in
combination with
stent placement
or
insertion
of
nasobiliarv
tube drainagein
healing
biliary
leaks.8-14, Department of Medicine, Faculty
of
Indonesia, Dr. Cipto Mangunkusumo nesiaWe report herein
ourexperience
in
dealing
with
endo_scopic
managementof
biliary
leaksfollowing LC.
PATIENTS AND METHODS
From January
1993 toDecember
I99l
dataof
sixteenERCP
wasperformed
technique
underintravenous
sedation
cope
(Olympus,
Japan)
type JFIT
20,
meinrerval
from
lC
,g
the
ERCP
procedure,
clinical
symptoms,
andliver
functions
were noted.Diagnosis of bile
Ieaks was made at ERCP demonsrrat_ing
contrastextravasation
from
thebiliary
tract.
Endo_scopic techniques to
resolve
thebiliary
lèaksincluded
stent placement alone
or
in
combination
with
endo_or insertion of nasobiliary
162 Lesmana
tain
criteria
in
selecting the method
of
endoscopicinterventions.
A
7Fr
endoprosthesis was placed above the siteof
leak
in all
stented patients.In
general,
the stent was removed after
four
to
six
weeks
of
placement without control
cholangiogram
except
in
onepatient
with big
leak
at thecommon
bile
duct.
A
tubecholangiography
wasperformed
aftertwo
weeks
of
insertion
in
patients
with NBT
drainage.Ultrasound
using real
time
scanner
(Toshiba
SSA-2701'
Japan)
and spiral CT-Scan
of
the
abdomen(Siemens Somatom+4, Germany) were carried out
in
five
and one patients respectively
to
evaluate
the presenceof
biloma.
RESULTS
Over the study period,
bile
leaks were
detected in
eleven
of l6
patientswith biliary
complications
relatedto
LC. In
the otherfive
patientsstricture
of thecommon
hepatic duct was obtained in
two
andtotal
ductobstruc-tion
in
theremaining
three patients.Diagnostic
ERCPfindings of
these
16patients were shown
in
table
l.
Table
l.
Diagnostic ERCP findingsin l6
patients with biliary complications related to LCBile duct injury
[image:2.595.200.538.104.693.2]Med J Indones
Table 2. Therapeutic ERCP interventions
in
11 patientsEndoscopic procedure N Vn
Stenting alone
Stent placement and sphincterotomy Insertion of nasobiliary tube
5
J
3
46 27 27
Total
The group study
consisted
of
eleven
patients;
eight
males and
three
females
with
an
average
age of 46 years (range 26to
10 years).The
meaninterval of LC
to
the ERCP procedure
was 6.3
days (range
3
to
12days). The most common presenting symptom
wasabdominal pain found
in
10of
II
patients(9lVo),fever
in
7patients
andjaundice in
2 patients.During
ERCP,
biliary
leaks were
demonstratedin
all
patients.
Cystic duct leak
was detected
in
9
patients whereasleak at
the common
bile duct
in
the other
2patients.
Therapeutic ERCP interventions were
suc-cessful
in
all
these
II
patients (table
2).
Stent place-ment alone wasperformed in
five of
1I
patients(figure
l), ES
with
bilio-endoprostheses
in
threepatients,
andinsertion
of
NBT
drainage
in
the remaining
threepatients
(figure 2). In
onepatient
with big
leak
at thecommon
bile
duct
(CBD)
the stent placement
wasextended
up
to
8
weeks
becausecontrol
cholangiog-raphy after 4 weeks
still
shqwed extravazationof small
amount
of
contrast.Total
Figure
l.
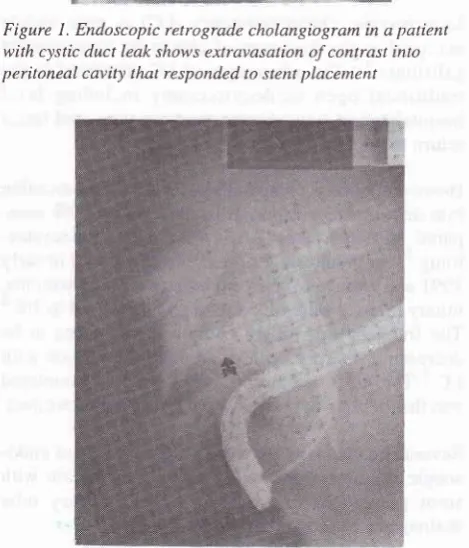
Endoscopic retograde cholangiogram in apatientwith cystic duct leak shows extravasation of contrast into peritoneal cavity that responded to stent placement
F i gure 2. Cho lan g io gram afte r lap aro s c opic c ho Ie cy s t ec t omy
demonstrates biliary leak (arrow) that successfully teated by
insertion of nasobiliary tube drainage
t00 1l
q
Biliary leaks
Stricture of common hepatic duct
Total duct obstruction
11
2 J
69 12
l9
[image:2.595.51.285.399.482.2] [image:2.595.312.547.419.693.2]Endos c op ic nlana g e nrc nt fo r b i Lia ry leaks r63 Vol 7, No 3, JulS, - Septenùer 1998
Additional duct fïndings
at ERCP were
stonesin
theCBD
in
five
parients which being extracted wrth
adormia
basket
at
the
same session
of
stent
or
NBT
removal. Complications
of
endoscopic therapy
oc_curred
in
threepatients. Bleeding after
ES occurreclin
two patients
with CBD
stoneswhich could
be managedconservatively
and stentmigration into
thecolon
wasdetected
in
theremaining
onepatient. The
stent cameouI spontaneously
with
the stool.C
performed
in
ie
the presencela
vity
andsub-DISCUSSION
The
reasonsfor ductal injury
atLC include
variation
anatomy,
technically difficult
dissection
dueto
severeoccurs when loose clips dislodge
or
the
cystic
duct
remnant necroses.
Our
studyconfirms
that mostof
thePain,
which
was
detectedinglVo
of
patients, was
themôst
common symptom
atclinical
presentation consis_tent
with biliary peritonitis.
The
meaninrerval of LC
dure
in
our
erthan that
t.e'13
Thi, d
hr beparrly
elack
of
the
facilities
in
our country.
Some
hat
chouseful
safterl
a
nega
le out a
While
is not
institution, ERCP
demonstrated the
presenceof
bile
leaks
in
l)OVo
patientsin
our
series.Therefore,
we
on to
perform
ERCPdirectly to
the
specteàbile
leaks
fol_Iowing LC,
as
e.r.l
l'18Our
results also
support
the other findings
that
therapeutic ERCP
procedures, such as stentplacement
and
NBT
decompression,
are
effective methods
tbr
healing
postLC
biliary
leaks.8-laThe
presumed
beneflt
of
endoscopic therapy
is
tlrereduction
of
sphinter
Oddi
pressure.
The
clecreaseresistance across
the ampula
therefbre
cliverts bilc
flow
into
the
duodenum
and away
fiom
the site
ol'injured
bile
duct. Although reducrion
of
ampLrllarypressure
is widely
accepted as animpor[ant
factr_rr inresolving
biliary
leaks,the
bestendoscopic
nrethocl toachieve
this
hasnot
beenwell
studied.Some
experts have claimed that
NBT
clrainagc
hassome
potential
advantagescompared
to
stenting.l3.l9
First, NBT
provides maximal and
direct bile
cluctpatients). Stent placement
is
more convenient for
patients and enable them
to
return
to
their
activity
faster
compared to
thosewho
arereceiving
NBT.
Ste
have also
beenreported
asthe
t2'I
f
choice
in
other
series.lo-recent
studles,dJ?,r.n,.on
be
for
4 to 6 weeksin
mostof
the patients.On
nt in our
seriesrequired stenting
fbr
gwe
of big
leak
ar rheCBD.
In
conclusion, both
stent placement
anclnasobiliary
tube
drainage
are
safe and
effective
encloscopic
therapy
for bile
leaksfollowing
Iaparoscopic cholecys_tectomy.
REFERENCES
l.
Schirmer BD, Edge SB, Dix J, Hyser MJ, Hanks JB, Jones RC. Laparoscopic cholecystectomy, treatment of choicc fbr symptomatic choleli tiasi s. Ann Surg 1 99 I :2 I 3 :665 _7 . 2. Southern Surgeons Club.A
prospective analysisol
l-5 l8laparoscopic cholecystectomies.
N
Eng
J Mctl
l99l:324:1073-8.
3. Peter JH, Cibbons GD, lnnes JT. Complications of laparo_
scopic cholecystectomy. Surgery l99l
;l
l0:769_7g. 4. Rossi RL, Schirmer WJ, Braasch JW. Laparoscopic bile ductinjuries. Arch Surg I 992 1 2j :569 _602.
5. Deziel DJ, Millikan KW, Economou SG, Doolas A, Tao Ko Sung,
Airan
scopic cholecys_tectomy:
a
ospitals ancl ananalysis of
7
165:9-14.164 Lesmana
7. Woods MS, Traverso LW, Kozarek RA, Tsao J, Rossi RL, Gough
D, et al.
Characteristicof
biliary
complications during laparoscopic cholecystectomy.A
multi institutional study. Am J Surg 1994;167:27-33.8. Foutch PG, Harlan JR, Hoefer
M.
Endoscopic therapy forpatients with a post-operative biliary leak. Gastrointest En-dosc 1992;39:416-21.
9. Brooks
DC,
BeckerJN,
ConnorspJ,
Carr-Locke DL.Management of bile leaks following Iaparoscopic choleiys-tectomy. Surg Endosc 19931,7 :292-5.
10. Kozarek
KA,
Ball TJ, Patterson DJ, Brandabur JJ, Raltz S,Traverso LW. Endoscopic treatment of biliary injury in the era
of
laparoscopic cholecystectomy. Gastrointest Endosc 1994;40:10-16.ll.
RaijmanI, Catalano
MF,
Hirsch GS,Mac
Fadyen B, BroughanTA,
Chung RS, et al. Endoscopic treatment of biliary leakage after laparoscopic cholecystectomy.Endos-copy 19941'26:741-4.
12. Himal HS. The role of ERCP in laparoscopic
cholecystec-tomy-related
cystic duct
stump leaks.
Surg EndoscI 996: l0:653-5.
Med J Indones
13. Chou S, Bosco JJ, Heiss FW. Successful treatment of post-cholecystectomy bile leaks using nasobiliary tube drainage and sphincterotomy. Am J Gasrroenterol
l99j;92
1839-43. 14. Ryan ME, Geenen JE, Lehman GA,Aliperti
G, FreemanML,
SilvermanWB, et al.
Endoscopic intervention for biliary leaks aftei laparoscopic cholecystectomy: amulti-center revi ew. Gastrointest Endosc 1998 ;4j :261 -6. 15. Davidoff
AM,
PappasTN,
MurrayEA.
Mechanismsof
maj or biliary injury duri n g I aparoscopi c cholecystectomy.
Ann Surg 1992;21 5 : 19 6-202.
16. Asbun HJ, Rossi RL, Lowell JA, Munson JL. Bileducrinjury
during laparoscopic cholecystectomy: mechanism of injury, prevention and management. World J Surg 1993;17:547 -52. 17. Brugge WR, Rosenberg DJ,
Alawi
A.
Diagnosisof
pos-toperative bile leaks. Am J Gastroenterol 1994;89:2178-83. 18. Prat F, Pelletier G, Ponchan T, Fritsch J, Meduri B, Boyer J, et al. What role can endoscopy playin
the managementof
biliary complications after laparoscopic cholecystectomy ?
Endoscopy 1997 ;29 :341 -8.