Emergency Prenatal Telemonitoring System in Wireless Mesh Network
Teks penuh
Gambar

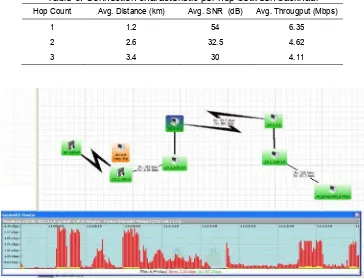
![Table 2. Result of Average output data rate [16]](https://thumb-ap.123doks.com/thumbv2/123dok/243609.503253/4.595.130.466.670.746/table-result-average-output-data-rate.webp)
Dokumen terkait
Penelitian ini dilakukan untuk mengetahui Kadar Hambat Minimum (KHM) dan Kadar Bunuh Minimum (KBM) ekstrak etanol kulit kayu akway serta golongan senyawa kimianya yang
Indikator rendahnya aktivitas belajar siswa dapat dilihat dari (1) Siswa yang bekerja sama dengan siswa lainnya: rendah sebanyak 9 siswa, pada kategori sedang 7 siswa
[r]
Dalam penelitian tindakan kelas guru dapat meneliti sendiri praktik pembelajaran yang dilaksanakan di kelas, baik dilihat dari interaksi peserta didik dalam proses
[r]
Jadi hasil analisis kinerja keuangan koperasi Murakabi DPU dari rasio likuiditas, rasio solvabilitas, rasio profitabilitas, rasio aktivitas, rasio rentabilitas secara
Siswa yang Mengikuti EkstrakLrrikLrlcr Bola Basket di. SMPN 50
merencanakan kegiatan tindak lanjut dalam bentuk pembelajaran remedi, program pengayaan, layanan konseling dan/atau memberikan tugas baik tugas individual maupun kelompok
