Differences between coronary disease and stroke in
incidence, case fatality, and risk factors, but few
differences in risk factors for fatal and non-fatal events
Lars Wilhelmsen
1*
, Max Ko
¨ster
2, Per Harmsen
1, and Georg Lappas
11
Section of Preventive Cardiology, The Cardiovascular Institute, Go
¨teborg University, Drakegatan 6, SE-412 50 Go
¨teborg,
Sweden; and
2Centre for Epidemiology, National Board of Health and Welfare, Stockholm, Sweden
Received 15 February 2005; revised 2 June 2005; accepted 16 June 2005
AimsTo compare incidence and mortality of coronary and stroke events, and risk factors for non-fatal and fatal events, respectively.
Methods and results Incidence and mortality were compared in all coronary (n¼559 341) and stroke (n¼530 689) events in Sweden from 1987 to 2001. Data from 28 years of follow-up of a random sample of 7400 men aged 47–55 and free of disease at baseline were used to compare risk factors. Incidence and 28 days of case fatality were considerably higher for coronary disease than for stroke, especially for men. Incidence of coronary disease decreased, especially for men (P¼0.0001 for both sexes), and mortality declined for both men and women during 1987–2001 (P¼0.0001 for both sexes). Stroke incidence declined slightly (P¼0.0001 for both sexes), and there was a decline of mortality (P¼0.0001 for both sexes). Out-of-hospital mortality during the first 28 days was higher than in-hospital mortality for coronary events, whereas for stroke, in-hospital mortality was higher (in men) or the same (in women) as out-of-hospital mortality. High serum cholesterol was a strong risk factor for coronary events, but not for stroke. High blood pressure was a stronger risk factor for stroke. About 50% of men with both stroke and coronary disease died from coronary disease. ConclusionSeveral differences regarding incidence, mortality, prognosis, and risk factors for stroke and coronary disease point towards different pathologies.
KEYWORDS
Coronary disease; Stroke; Incidence; Mortality; Risk factors; Pathology
Introduction
Myocardial infarction and sudden coronary death (in the
fol-lowing denoted as coronary disease) and stroke are common
causes of disability and death and are often discussed as two
diseases of the same family and caused by atherosclerotic
arterial disease. If there were major similarities between
coronary disease and stroke, declining trends in the
inci-dence of coronary disease would be expected also for
stroke. Alternatively, decreasing incidence of coronary
events could lead to risk of stroke in more people.
1If the
two diseases had similar background and pathology, one
would also expect similar risk factors. Elevated serum
cholesterol is a strong risk factor for coronary disease, but
in most prospective studies, it has not been associated
with increased risk for stroke.
2,3However, lipid-lowering
therapy with statins has reduced the incidence of both
thrombotic stroke and coronary disease.
4,5Owing to the suggested similarities of the two diseases
and their great impact on public health, they were analysed
together
in
the
recently
published
SCORE
project.
6The project was forced to restrict the analysis to fatal
events because of differences in criteria for non-fatal
events in the contributing prospective studies. Against this
background, it would be of interest to study further to
what extent risk factors are similar for stroke and coronary
disease and whether risk factors are the same for non-fatal
and fatal events.
In the present paper, we have analysed mortality and
mor-bidity data from the countrywide Swedish Acute Myocardial
Infarction register, which contains data on incidence and
mortality from 1987 until 2001 with a total of 340 721
male and 218 620 female non-fatal and fatal coronary
events. A similar registration of non-fatal and fatal stroke
events included 261 357 male and 269 332 female events.
In addition, data on 28 years of follow-up of 7400 men,
free of these diseases at baseline, were used to compare
risk factors for non-fatal and fatal coronary and stroke
events.
Methods
Registration of events
A national hospital register of diagnoses at discharge has been in operation since 1972 in Sweden and includes all hospitals in the
&
The European Society of Cardiology 2005. All rights reserved. For Permissions, please e-mail: [email protected]*
Corresponding author. Tel:þ46 31 703 1884; fax:þ46 31 703 1890.E-mail address: [email protected]
doi:10.1093/eurheartj/ehi412
by guest on June 6, 2013
http://eurheartj.oxfordjournals.org/
country since 1987. The quality of the register during the period 1987–95 has been checked and found to be good.7A file of the
men of the population study described subsequently was also checked against this register and it was found that the register had missed only 3% of hospitalizations for myocardial infarction, atrial fibrillation (AF), or heart failure.
The Swedish Causes of Death Register has been operating since 1961 and found to miss only single events. In the present study, record linkage of the Hospital Discharge Register and the Causes of Death Register was performed. An event (non-fatal or fatal) that occurred within 28 days was considered to be the same event and was counted as one event.
In 1987, there was a change from the eighth to the ninth revision of the International Classification of Diseases (ICD) and in 1997, there was a change to ICD-10. These changes were taken into account in the present analyses. The ICD-8 codes were changed to ICD-9.
For coronary disease, ICD-9 code 410 and ICD-10 codes I21 and 22 were used; for stroke, ICD-9 codes 431, 434, and 436 and ICD-10 codes I61, 63, and 64 were used.
Population study of men
The Multifactor Primary Prevention Study was started in Go¨teborg in 1970 and was intended as an intervention trial against smoking, hypercholesterolaemia, and hypertension at pre-defined levels in an intervention group comprising 10 000 men, a random third of all men in the city (n¼30 000) who were born between 1915 and
1925, but not in 1923.8The remaining two-thirds of the population
constituted two control groups of 10 000 men each. A first screening examination took place between 1970 and 1973 and the data from the examination are used in the present study. After 10 years of follow-up, 20% men surviving and still living in the area, according to the population census from the intervention group and one control group, were re-examined. Out of 1805 invited men in the control group, 1473 participated, and of 1803 invited controls, 1404 participated. After these 10 years of follow-up, risk factor values had decreased in the intervention group, but there were no significant differences in serum cholesterol, smoking, and blood pressure, or outcome between the intervention and control groups.8 Thus, any changes brought about by the intervention
took place in the general population as well, as revealed in the ran-domly selected control group, and the present study group is con-sidered to be representative of the background population.
Those men who responded to a postal questionnaire were invited to a screening examination in hospital, in which 7495 men (75% of the sample) took part. The questionnaire contained questions about history of myocardial infarction and stroke among mothers, fathers, and brothers/sisters, previous myocardial infarction, stroke, diabetes mellitus as well as chest pain and dyspnoea on exertion, smoking habits, psychological stress (defined as feeling tense, irritable or filled with anxiety, or having sleeping difficulties as a result of conditions at work or at home during the preceding 1–5 years), and physical activity at work and during leisure time.
Screening examinations were performed in the afternoon. Blood pressure was measured after 5 min rest to the nearest 2 mmHg, with the subjects seated. These afternoon blood pressures were found to be considerably lower when checked later at a more relaxed situation in a subsample; 175/115 mmHg is comparable with 165/95 at resting conditions. Body height was measured to the nearest centimetre and body weight to the nearest 0.1 kg. Body mass index (BMI) was calculated as weight (kg)/height (m2).
Serum cholesterol concentrations (from a sample taken after fasting for at least 2 h) were determined according to standard labo-ratory procedures. Details of the procedures have been published previously.9
The follow-up extended through the year 1998. The endpoints were registered from several sources. Non-fatal and fatal myocar-dial infarction and stroke up to 65 years of age were recorded
according to specific criteria in special registers.10,11The national
hospital discharge register, which included all ages, was also used. For the present analyses, the following principal or contributory diagnoses at hospitalization or death were used:
(i) Non-fatal myocardial infarction (ICD-9 code 410; ICD-10 code I21).
(ii) Death from coronary disease (ICD-9 codes 410, 411, 412, and 414; ICD-10 code I21).
(iii) Non-fatal and fatal stroke (ICD-9 codes 430–434, 436, and ICD-10 codes I60, 61, 63, and 64. I60 (subarachnoidal bleed-ing) was included in this analysis, but not in the national regis-tration of events.
The study was conducted according to the Declaration of Helsinki rules and was approved by the Ethics Committee of Go¨teborg University.
Statistical methods
Incidence and mortality rates were calculated with the mid-year Swedish population in the respective age groups as denominator. When age-standardization was performed, the Swedish mid-year population of the year 2000 was used as standard. Ages were cate-gorized in 5-year age groups. Differences over time in incidence and mortality were tested with logistic regression. Owing to the large number of events, significant differences are to be expected for some time trends that do not seem impressive. Differences between discrete variables and differences between continuous variables were tested with x2 analysis and t-test, respectively.
Two-sided test withP-values,0.05 are considered as significant.
Results
Incidence, mortality, and case fatality of coronary
disease and stroke in Sweden
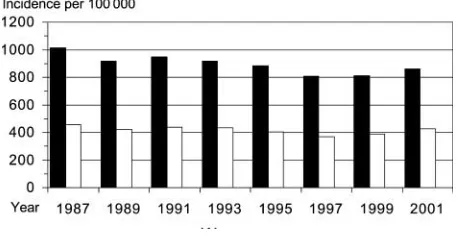
The age-standardized incidence of non-fatal and fatal
myo-cardial infarctions during 1987–2001 among men and women
is shown in
Figure 1.
The incidence was about two times
higher for men compared with women, and there was a
decline in incidence for men from about 1000/100 000 of
the population per year in 1987 to about 800 in 2001
(
P
¼
0.0001); for women, the incidence was around 400/
100 000 and there was a slight decline (
P
¼
0.00021).
There is a slight increase in incidence for 2001, which can
be attributed to change of criteria for myocardial infarction;
elevated levels of plasma troponin T became accepted as
criterion for the diagnosis. The declining incidence among
men was seen for all age groups, except for men aged
.
80. Among men aged
90, the incidence increased (data
Figure 1 Age-standardized incidence of non-fatal and fatal myocardial infarction during 1987–2001 per 100 000 men and women aged between 20 and 90þin Sweden. Decline by time;P¼0.0001 for both sexes.
by guest on June 6, 2013
http://eurheartj.oxfordjournals.org/
not shown). For women, the incidence declined between
ages 60 and 84 years, but it increased in the highest age
groups (data not shown).
Mortality from coronary disease declined during the same
period for both men (
P
¼
0.0001) and women (
P
¼
0.0001)
(
Figure 2).
This was evident for all age groups of both men
and women, except those aged
90. These trends reflected
in declining age-standardized case fatality (including deaths
in hospital and outside hospital within 28 days) from 50.5% in
1987 to 33.8% in 2001 among men (
P
¼
0.0001) and from
46.7% in 1987 to 31.9% in 2001 among women (
P
¼
0.0001).
The number of coronary deaths outside hospital exceeded
that of in-hospital deaths, especially for men (all numbers
for mortality within 28 days) (
Figure 3
). During the entire
period of 1987–2001 and for all ages, there were 145 345
deaths within 28 days among men and 61.5% of these
occurred outside hospital. For women, there were 103 484
deaths and 56.3% of these occurred outside hospital.
Incidence and mortality for stroke are shown in
Figures 4
and
5
. The age-standardized incidence was just above 700/
100 000 for men and just above 500/100 000 for women.
Thus, the sex difference for stroke was smaller than that
for coronary disease. For both sexes, there was a
mode-rately declining incidence over the period (
P
¼
0.0001).
The 28 days of case fatality among men declined slightly
from 180/100 000 to just over 160/100 000 from 1987 to
2001 (
P
¼
0.0001) and declined among women from about
145/100 000 to just over 130/100 000 during the same
period (
P
¼
0.0001).
The number of deaths in hospital and outside-hospital from
stroke appears in
Figure 6.
For men, in-hospital deaths were
higher than out-of-hospital deaths for the entire period of
1987–2001, and was about 1.3 times higher than
out-of-hospital deaths. For women, the numbers were similar for
the two types of death.
Tables 1
and
2
give the number and incidence for coronary
disease and stroke among men and women per 10-year age
groups during the year 2001 (data available for the last
year). Incidence of coronary disease was higher for men
compared with women for all age groups, with the ratio
4.6 for the age group 35–44 years, declining to 1.5 for the
Figure 2 Age-standardized mortality from coronary disease during 1987–2001 per 100 000 men and women aged between 20 and 90þ in Sweden. Decline by time;P¼0.0001 for both sexes.
Figure 3 Number of men and women died in hospital and outside hospital from coronary disease during 1987–2001 in Sweden.
Figure 4 Age-standardized incidence of stroke during 1987–2001 per 100 000 men and women aged between 20 and 90þin Sweden. Decline by time;P¼0.0001 for both sexes.
Figure 5 Age-standardized mortality from stroke during 1987–2001 per 100 000 men and women aged between 20 and 90þin Sweden. Decline by time;P¼0.0001.
Figure 6 Number of men and women died in hospital and outside hospital from stroke during 1987–2001 in Sweden.
by guest on June 6, 2013
http://eurheartj.oxfordjournals.org/
group
.
85 years. For stroke, the men/women ratio was
lower; 1.4 for the lowest age group decreasing to 1.1 for
those aged
85. Thus, for both diagnoses and in all age
groups, the incidence was higher for men than for women.
However, the absolute number of women with strokes was
higher in the two highest age groups because of the higher
number of women in the population in these ages.
Tables 3
and
4
show the case fatality for men and
women, respectively, who died during the first 28 days
from onset and those who died between 29 days and 5
years. The results are based upon the entire period
1987–2001.
The pattern was very similar for men and women; 28 days
case of fatality was about twice as high for coronary disease
(24–75%) compared with stroke (15–44%), whereas case
fatality for stroke tended to be higher for the long-term
follow-up (6–24% for coronary disease vs. 9–44% for stroke).
Thus, for age groups over 55 years, long-term (29 days to 5
Table 3 Male case fatality within 28 days as well as between 29 days and 5 years, respectively, for coronary disease and stroke during 1987–2001 by age group (Centre for Epidemiology, National Board of Health and Welfare, Sweden)
Age
Table 1 Number of men with coronary disease and stroke, respectively, for hospitalized patients and cases died outside hospital, incidence of these events together per 100 000 and total population by age group in the year 2001 (Centre for Epidemiology, National Board of Health and Welfare, Sweden)
35–44 302 121 65.57 193 11 51.31 645 091
45–54 1415 217 273.42 801 41 141.07 596 878
55–64 2970 556 607.36 2221 85 397.21 580 543
65–74 4453 1048 1558.99 4244 241 1271.05 352 857
75–84 6205 1638 3240.59 6526 748 3005.49 242 024
85 2662 916 5366.73 2370 635 4507.27 66 670
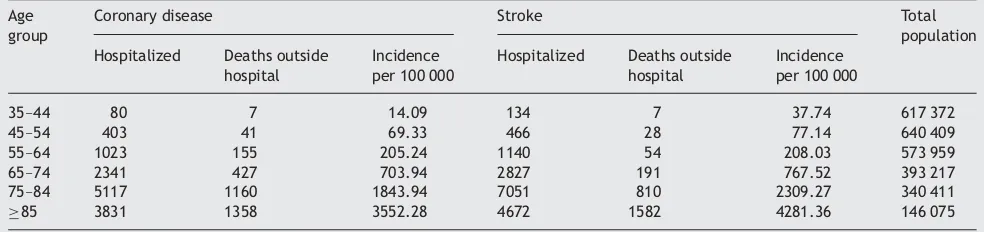
Table 2 Number of women with coronary disease and stroke, respectively, for hospitalized patients and cases died outside hospital, incidence of these events together per 100 000 and total population by age group in the year 2001 (Centre for Epidemiology, National Board of Health and Welfare, Sweden)
Age
45–54 403 41 69.33 466 28 77.14 640 409
55–64 1023 155 205.24 1140 54 208.03 573 959
65–74 2341 427 703.94 2827 191 767.52 393 217
75–84 5117 1160 1843.94 7051 810 2309.27 340 411
85 3831 1358 3552.28 4672 1582 4281.36 146 075
Table 4 Female case fatality within 28 days as well as between 29 days and 5 years, respectively, for coronary disease and stroke during the years 1987–2001 by age group (Centre for Epidemiology, National Board of Health and Welfare, Sweden)
years) case fatality from stroke increased to about twice as
high compared with that for coronary disease.
Risk factors for coronary disease and stroke among
men in Go
¨teborg
The original sample of men included 7495 aged between 47
and 55. Myocardial infarction or stroke had occurred before
baseline in 95 men, and 7400 remained for the present
ana-lyses. During up to 28 years of follow-up, 1150 men suffered
primarily non-fatal myocardial infarction and 554 men fatal
coronary disease. Out of the fatal events, 278 (50%) had
diag-noses for myocardial infarction or coronary atherosclerosis.
Primarily non-fatal strokes occurred in 855 men and fatal
events in 150 men. Out of these, 179 men had a diagnosis
of subarachnoidal bleeding or intracerebral bleeding.
Using Cox regression analyses, independent risk factors
for the combination of non-fatal and fatal events have
been published previously
2,12(Harmsen
et al.
has submitted
for publication). Independently significant risk factors for
coronary disease (non-fatal and fatal) during 28 years of
follow-up were age, myocardial infarction in mothers,
fathers, and siblings, chest pain on exercise, diabetes
melli-tus, smoking, low social class, psychological stress, high
serum cholesterol, and high blood pressure (in spite of
treat-ment), but not low physical activity during leisure time or
high BMI.
For stroke (non-fatal and fatal), independent risk factors
were age, previous transient ischaemic attacks, AF, diabetes
mellitus, psychological stress, smoking, high blood pressure,
and high BMI, but not high serum cholesterol or low physical
activity during leisure.
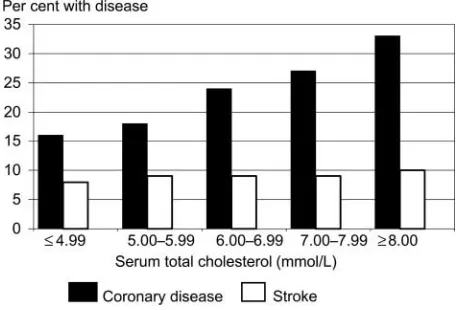
Table 5
lists risk factors that differed
between coronary disease and stroke. Coronary disease and
stroke events during 28 years of follow-up by serum total
cholesterol are shown in
Figure 7.
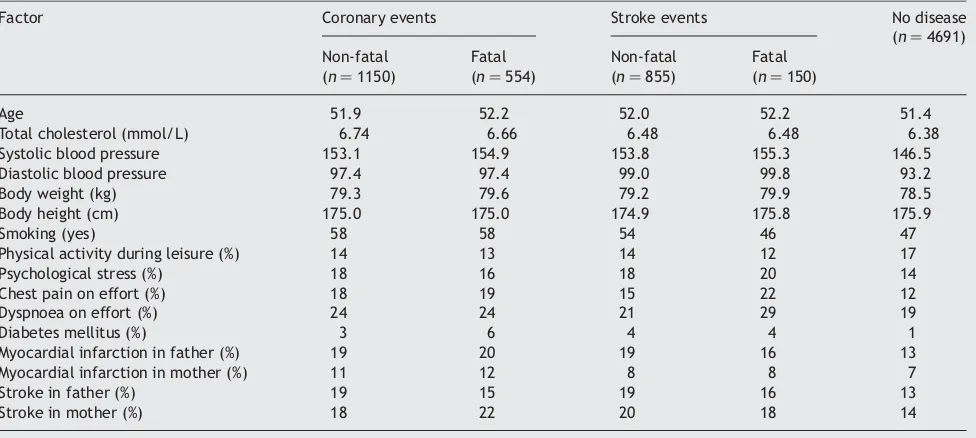
Table 6
gives baseline data for primarily non-fatal and
fatal events within 28 days among those who suffered
coro-nary events and stroke events, respectively, as well as for
those who did not suffer any of these diseases during the
following 28 years. Taking into consideration that multiple
tests were performed, only
P
-values less than 0.01 may
be considered important. Only few differences were
found. Men with fatal coronary events tended to be older
(
P
¼
0.013) and had diabetes more often (
P
¼
0.006). They
tended to have a family history of stroke more often
among mothers (
P
¼
0.036) compared with men who
suf-fered non-fatal events. Men who sufsuf-fered fatal strokes
tended to report chest pain (
P
¼
0.011) and dyspnoea on
effort (
P
¼
0.027) more often than men with non-fatal
strokes, but the baseline age did not differ. None of the
other baseline factors as mentioned in Methods differed
between non-fatal and fatal events for either coronary
disease or stroke.
Out of the 1150 primarily surviving men with coronary
disease, 676 (59%) died during 12 483 person-years of
follow-up. Of these men, 68% died from coronary disease,
5% from stroke, and 27% from other diseases (
Figure 8
).
Out of the 855 surviving men with stroke, 478 (56%) died
during 8315 person-years of follow up. Causes of death
were coronary disease (52%), stroke (13%), and other
causes (35%) (
Figure 8
). Thus, a considerable proportion of
the men with stroke died from coronary disease.
Discussion
When comparing coronary disease and stroke, we found that
incidence and short-term case fatality of coronary disease
were considerably higher than that of stroke, especially
for men. Incidence of coronary disease decreased especially
for men, and mortality declined for both men and women
during 1987–2001. For stroke, there was a less marked
decline regarding incidence and there were slight declines
in mortality. Out-of-hospital mortality during the first 28
days from occurrence was higher than in-hospital mortality
for coronary events, whereas for stroke, in-hospital
mor-tality was higher (in men) or the same (in women) as
out-of-hospital mortality. The 28 days of case fatality from
coronary disease was nearly three times higher for men
and at least two times higher for women compared with
case fatality of stroke during that period. It is known that
a substantial proportion of these early coronary deaths are
instantaneous and are caused by fatal cardiac arrhythmias.
Longer-term (29 days to 5 years) case fatality was higher
for stroke than for coronary disease.
There were well-known differences in risk factors between
coronary disease and stroke: serum cholesterol being a strong
risk factor for coronary events, but not for stroke, not even
Table 5 Differences between coronary disease and stroke forindependent risk factors among men
Factor Coronary disease Stroke
Previous TIA n.s. 1.80 1.19–2.74
AF n.s. 2.55 1.20 – 5.41
A 28 years of follow-up of 7400 men aged 47–55 at baseline. TIA, transitory ischaemic attack; n.s., not significant.
Figure 7 Coronary and stroke events by serum total cholesterol at baseline during 28 years of follow-up of 7322 men free of any of these diseases at baseline.
by guest on June 6, 2013
http://eurheartj.oxfordjournals.org/
when only pure thrombotic strokes are analysed, a finding
that is contrary to what was published by Lawlor
et al.
13High blood pressure and high BMI were more important risk
factors for stroke than for coronary events. However,
50%
of both stroke and coronary disease men died from coronary
disease, suggesting similar background pathology for the
two diseases.
The changing incidences for stroke and coronary disease
are of interest. It has been hypothesized that decreasing
coronary incidence might lead to increased stroke incidence
because of the higher number of surviving coronary patients
at risk for stroke. However, death from stroke was not
common among the post-infarct men of the present study.
On the basis of statistical calculations, Peeters
et al.
1denied that increased coronary survival could lead to
increased stroke incidence. The declining coronary
mor-tality is, to some extent, due to the better hospital
treat-ment, but it is noteworthy that out-of-hospital coronary
mortality also declined. The autopsy rate was previously
high, especially among out-of-hospital deaths, and it was
earlier shown that this mortality was mainly caused by
coro-nary disease.
14It has been shown that the declining
coron-ary incidence is primarily due to primcoron-ary preventive
achievements regarding smoking, serum cholesterol, and
blood pressure.
14The previous decline in mean blood
pressure in the population seems to have halted recently,
15and that may be part of the reason for the inconsiderable
decline of stroke incidence. Increased body weight, which
is not of strong importance for coronary disease (yet)
according to our studies,
12but is important for stroke,
16is
another factor that may have played a part. The different
stroke subtypes have different pathological background—
athero-thrombosis vs. haemorrhages. Since 1983, at least
90% of stroke diagnoses were based upon CT scan,
2and
only 18% of the strokes were due to any type of
haemor-rhage. When we analysed risk factors for
thrombotic/occlu-sive strokes separately, we came to the same risk factor
pattern. Thus, athero-thrombotic pathology is the main
background for most stroke events, and the risk factor
difference against coronary disease seems to be due to
differences in pathology for different vascular beds. In
another study, we found increased fibrinogen levels to be
strongly associated with both stroke and coronary disease,
whereas coronary disease, but not stroke, was associated
with high total plasma cholesterol in that study.
17We
studied only men in the present study because comparable
long-term results on risk factors from the same population
and with a great number of events were available. In an
earlier study of women, we found risk factors for coronary
disease to be high serum cholesterol and triglycerides,
smoking, diabetes, as well as high blood pressure, and for
stroke, triglycerides and high blood pressure, but the
number of endpoints was limited to 67 and 66 events.
18Puddu
et al.
19discussed the possible different pathologies
between stroke and coronary disease and concluded that
they are two aspects of the same disease, but that the
Figure 8 Cause of death during follow-up among primarily surviving menwith coronary disease (n¼1150) and stroke (n¼855).
Table 6 Baseline factors for men who suffered primarily non-fatal and fatal coronary disease and stroke, respectively, as well as for men who did not suffer any of these diseases during 28 years of follow-up (Primary Prevention Study, Go¨teborg)
Factor Coronary events Stroke events No disease (n¼4691) Non-fatal
(n¼1150)
Fatal (n¼554)
Non-fatal (n¼855)
Fatal (n¼150)
Age 51.9 52.2 52.0 52.2 51.4
Total cholesterol (mmol/L) 6.74 6.66 6.48 6.48 6.38 Systolic blood pressure 153.1 154.9 153.8 155.3 146.5 Diastolic blood pressure 97.4 97.4 99.0 99.8 93.2 Body weight (kg) 79.3 79.6 79.2 79.9 78.5 Body height (cm) 175.0 175.0 174.9 175.8 175.9
Smoking (yes) 58 58 54 46 47
Physical activity during leisure (%) 14 13 14 12 17
Psychological stress (%) 18 16 18 20 14
Chest pain on effort (%) 18 19 15 22 12
Dyspnoea on effort (%) 24 24 21 29 19
Diabetes mellitus (%) 3 6 4 4 1
Myocardial infarction in father (%) 19 20 19 16 13 Myocardial infarction in mother (%) 11 12 8 8 7
Stroke in father (%) 19 15 19 16 13
Stroke in mother (%) 18 22 20 18 14
P-values for difference between non-fatal and fatal events are given in the text.
by guest on June 6, 2013
http://eurheartj.oxfordjournals.org/
reactivity of the coronary and cerebral arteries is different.
Falk
20proposed that the ulceration of atherosclerotic
plaques is important in coronary occlusion, but not in
intra-cranial cerebral arteries. It is also known that individuals
with familial hypercholesterolaemia develop myocardial
infarction at a young age, but they do not develop
stroke.
21The coronary atherosclerotic plaque had higher
lipid content, whereas the cerebral plaque had higher
content of fibrous tissue, which in turn is more strongly
affected by high blood pressure.
22An important practical question is whether the
predic-tions in the SCORE project,
6which was based upon fatal
coro-nary and stroke events, can also be used for non-fatal
disease. In the present analyses, diabetes was a stronger
risk factor for fatal events when compared with non-fatal
events, but diabetes was not included in the SCORE
diagram. Thus, it would not make a difference. A problem
is, however, that out of the three risk factors used in
SCORE, serum cholesterol, blood pressure, and smoking,
there are quantitative differences regarding cholesterol
and blood pressure. In the present study, the relative risk
for coronary events with 1 mmol/L increase of total serum
cholesterol was 1.220, but was insignificant for stroke. The
risks associated with increase of blood pressure were more
similar. Risk for stroke increased with 1.026 and for coronary
with 1.020 for 1 mmHg increase of diastolic blood pressure.
The results regarding coronary events agree with other
pro-spective studies summarized by Dobson
et al.
23When using
SCORE, risk of coronary events are somewhat overestimated
by blood pressure values, but underestimated by serum
cholesterol values, and vice versa for stroke events.
References
1. Peeters A, Bonneux L, Barendregt JJ, Mackenbach JP; Netherlands Epidemiology and Demography Compression of Morbidity Research Group. Improvements in treatment of coronary heart disease and cessa-tion of stroke mortality rate decline.Stroke2003;34:1610–1616. 2. Harmsen P, Rosengren A, Tsipogianni A, Wilhelmsen L. Risk factors for
stroke in a cohort of middle-aged men in Go¨teborg, Sweden. Stroke 1990;21:223–229.
3. Prospective Studies Collaboration. Cholesterol, diastolic blood pressure, and stroke: 13 000 strokes in 450 000 people in 45 prospective cohorts. Lancet1995;346:1647–1653.
4. The Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344: 1383–1389.
5. Collins R, Armitage J, Parish S, Sleight P, Peto R; Heart Protection Study Collaborative Group. Effects of cholesterol-lowering with simvastatin on stroke and other major vascular events in 20 536 people with cerebrovas-cular disease or other high-risk conditions.Lancet2004;363:757–767.
6. Conroy RM, Pyo¨ra¨la¨ K, Fitzgerald AP, Sans S, Menotti A, deBacker G, De Bacquer D, Ducimitiere P, Jousilahti P, Keil U, Njo¨lstad I, Oganov RG, Thomsen T, Tunstall-Pedoe H, Tverdal A, Wedel H, Whincup P, Wilhelmsen L, Graham IM. On behalf of the SCORE project group. Estimation of ten-year risk of fatal cardiovascular risk in Europe: the SCORE project.Eur Heart J2003;24:987–1003.
7. Hammar N, Alfredsson L, Rose´n M, Spetz C-L, Kahan T, Ysberg A-S. A national record linkage to study acute myocardial infarction incidence and case fatality in Sweden.Int J Epidemiol2001;30(Suppl. 1):S30–S33. 8. Wilhelmsen L, Berglund G, Elmfeldt D, Tibblin G, Wedel H, Pennert K, Vedin A, Wilhelmsson C, Werko¨ L. The multifactor primary prevention trial in Go¨teborg, Sweden.Eur Heart J1986;7:279–288.
9. Wilhelmsen L, Rosengren A, Eriksson H, Lappas G. Heart failure in the general population of men—morbidity, risk factors and prognosis. J Intern Med2001;249:253–261.
10. Elmfeldt D, Wilhelmsen L, Tibblin G, Vedin JA, Wilhelmsson C, Bengtsson C. Registration of myocardial infarction in the city of Go¨teborg, Sweden. J Chron Dis1975;28:173–186.
11. Harmsen P, Tibblin G. A stroke register in Go¨teborg, Sweden.Acta Med Scand1972;191:463–470.
12. Wilhelmsen L, Lappas G, Rosengren A. Risk of coronary events by baseline factors during 28 years follow-up and three periods in a random popu-lation sample of men.J Intern Med2004;256:298–307.
13. Lawlor DA, Davey Smith G, Leon DA, Sterne JAC, Ebrahim S. Secular trends in mortality by stroke subtype in the 20th century: a retrospective analysis.Lancet2002;360:1818–1823.
14. Wilhelmsen L, Rosengren A, Johansson S, Lappas G. Coronary heart disease attack rate, incidence and mortality 1975–1994 in Go¨teborg, Sweden.Eur Heart J1997;18:572–581.
15. Wilhjelmsen L. Cardiovascular monitoring of a city during 30 years.Eur Heart J1997;18:1220–1230.
16. Jood K, Jern C, Wilhelmsen L, Rosengren A. Body mass index in mid-life is associated with a first stroke in men: a prospective population study over 28 years.Stroke2004;35:2764–2769.
17. Eriksson H, Wilhelmsen L, Welin L, Sva¨rdsudd K, Tibblin G. 21-year follow-up of CVD and total mortality among men born in 1913. In: Ernst E, Koenig W, Lowe GDO, Meade TW, eds. Fibrinogen: A ‘New’ Cardiovascular Risk Factor.Blackwell-MZV; 1992. p115–119.
18. Rosengren A, Wilhelmsen L, Lappas G, Johansson S. Body mass index, cor-onary heart disease and stroke in Swedish women. A prospective 19-year follow-up in the BEDA study. Eur J Cardiovasc Prev Rehabil 2003; 10:443–450.
19. Puddu P, Puddu GM, Bastagli L, Massarelli G, Muscari A. Coronary and cer-ebrovascular atherosclerosis: two aspects of the same disease or two different pathologies?Arch Gerontol Geriatr1995;20:15–22.
20. Falk E. Plaque rupture with severe pre-existing stenosis precipitating cor-onary thrombosis: characteristics of corcor-onary atherosclerotic plaques underlying fatal occlusive thrombi.Br Heart J1983;50:127–134. 21. Postiglione A, Nappi A, Brunetti A, Soricelli A, Rubba P, Gnasso A,
Cammisa M, Frusciante V, Cortese C, Salvatore M. Relative protection from cerebral atherosclerosis of young patients with homozygous familial hypercholesteroemia.Atherosclerosis1991;90:23–30.
22. Tanaka K, Masuda J, Imamura T, Sueishi K, Nakashima T, Sakurai I, Shozava T, Hosoda Y, Yoshida Y, Nishiyama Y, Yutani C, Hatano S. A nation-wide study of atherosclerosis in infants, children and young adults in Japan.Atherosclerosis1988;72:143–156.
23. Dobson AJ, Evans A, Ferrario M, Kuulasmaa KA, Moltchanov VA, Sans S, Tunstall-Pedoe H, Tuomilehto JO, Wedel H, Yarnell J. Changes in esti-mated coronary risk in the 1980s: data from 3 populations in the WHO MONICA Project. World Health Organization. Monitoring trends and deter-minants in cardiovascular diseases.Ann Med1998;30:199–205.
by guest on June 6, 2013
http://eurheartj.oxfordjournals.org/