Apa yang dimaksud Spontaneous Pneumothorax ?
Sumber : buku ajar ilmu bedah karanagn sjamsuhidayat, dejong penerbit buku kedokteran EGC 2010
Pneumotoraks spontan
Secara epidemiologi, pneumothorax spontan cukup sering terjadi. Data dari Amerika Serikat menunjukkan ada sekitar 20.000 pasien per tahun menderita pneumotoraks spontan. Secara umum, pneumotoraks spontan dikelompokkan menjadi dua bentuk, yakni primer dan sekunder. Pneumotoraks spontan primer terjadi pada paru yang sebelumnya tidak memiliki gangguan klinis, sedangkan pneumotoraks spontan sekunder adalah pneumotoraks spontan yang diderita oleh penderita yang sudah memiliki gangguan paru, misalnya pada penderita Penyakit Paru Obstruktif Kronis.
Pneumotoraks spontan terjadi karena lemahnya dinding alveolus dan pleura viseral, sementara pada suatu saat terjadi peninggian tekanan di jalan napas oleh suatu sebab sehingga alveoulus dan pleura yang menutupinya pecah. Hal ini dapat terjadi pada penderita infeksi paru dengan batuk keras, pengguna kortikosteroid kronik, perokok, dan penyakit menahun.
Pneumothoraks spontan adalah keadaan terdapatnya udara atau gas dalam rongga pleura yang dapat menyebabkan paru kolaps baik total maupun sebagian tanpa didahului adanya trauma sebelumnya. Pneumothoraks spontan dibagi
menjadi primer dan sekunder berdasarkan adanya penyakit paru yang mendasari, pneumothoraks spontan primer jika
tidak terdapat latar belakang penyakit paru yang mendasari dan disebut pneumothoraks spontan sekunder bila terdapat latar belakang penyakit paru yang mendasari.
Apa yang dapatmenyebabkan Spontaneous Pneumothorax?
Terdapat beberapa faktor yang mempengaruhi timbulnya pneumothoraks
spontan, diantaranya : usia, jenis kelamin, pneumonia, sarkoidosis, penyakit membran hialin pada neonatus, abses paru, tumor paru, asma, kistik fibrosis, benda asing, dan adanya bleb atau bulla paru.
sampai yang paling berat, tergantung dari masing-masing individu. Penderita mengeluh sesak nafas, nyeri dada, batuk non produktif, bahkan sampai batuk darah. Oleh karena itu diperlukan terapi yang bervariasi, mulai dari observasi sampai tindakan bedah
DAFTAR PUSTAKA
1. Hisyam B, Budiono E. Pneumothoraks spontan. Di dalam : Sudoyo AW, Setiyohadi B, Alwi I, Simadibrata M, Setiati S, editor. Buku ajar ilmu penyakit dalam jilid 2. Edisi IV. Jakarta : Pusat Penerbitan Departemen Ilmu Penyakit Dalam Fakultas Kedokteran Universitas Indonesia, 2006 ; 1073 – 8
Gejala Klinis?
Sesak napas, nyeri dada, batuk, mudah lelah, denyut jantung cepat,
Bagaimana histologi dari daerah yang mengalami Spontaneous Pneumothorax?
Sumber: Jurnal A Unique, Histopathologic Lesion in a Subset of Patients With Spontaneous Pneumothorax
Deborah A. Belchis, MD; Kris Shekitka, MD; Christopher D. Gocke, MD
pleural fibrosis fibrosis of the visceral pleura so that part or all of a lung becomes covered with a plaque or a thick layer of nonexpansible(dak kenyal) fibrous tissue. The more extensive form is called FIBROTHORAX .
Myxoid stroma (cairan mucus dalam membran ganda
Wedge shaped = bentuk irisan
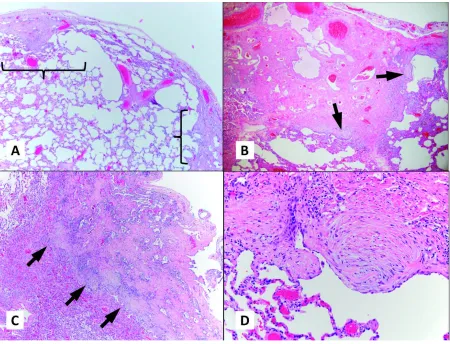
Eleven patients (12% of all patients with SP in the study) were found to have a distinctive pattern of pleural fibrosis with islands of fibroblastic foci within a myxoid stroma at the pleural-parenchymal interface or leading edge. Often, these lesions exhibited a wedge-shaped configuration, with the broad base at the pleural surface and the apex toward the lung parenchyma. In one patient (9%), serial lung biopsies from separate episodes of pneumothorax were available for review (biopsies 2 and 8 in Table 1). The clinical and radiologic findings of our patients are described in Table 1. Almost all were male. Ten of the patients (91%) were younger than 25 years old (range, 16–24); one (9%) was 53. The average age in the larger, 92patient group was 54, and the average in the PAFL subset was 20. In comparison to the main study group, this age difference is statistically significant (P , .05). The 53-yearold patient was a nonsmoker. Of the others, 4 (36%) were nonsmokers, 5 (45%) were smokers, and the smoking status was unknown for 1 patient (9%). Three (27%) had a history of asthma; 3 (27%) did not. The asthma history of the others (5 of 11; 45%) was unknown. In all patients (100%), the upper lobes or apex was involved by the pneumothorax. One (9%) also had lower lobe involvement. On gross examination, 4 of the resected lung specimens (36%) had recognizable blebs or bullae. The largest bulla was in a 16-year-old, nonsmoking patient and measured 9 cm at greatest dimension. Other bullae/blebs measured up to 2 cm in greatest dimension. No masses were identified. Histopathologic review revealed a distinctive lesion with a zonal pattern characterized by dense, collagenous fibrosis at
the subpleural surface and younger, more-active, fibroblastic-like foci at the pleural-parenchymal interface (Figure 1, A through C). The fibroblastic-like foci are key to recognition of the entity. The fibroblastic foci were scattered along the leading edge (Figure 1, D). Less fibrotic, subpleural lesions with a ‘‘stuck-on’’ appearance could be
identified (Figure 2, A). The lesions were multifocal and extended varying lengths along the pleural surface, separated by intervening normal pleura (Figure 1, A). As indicated above, the lesions often assumed a triangular or pyramidal configuration that was quite striking on low power. They sometimes extended down pleural septa but did not seem to disproportionately involve the septa. The amount of subpleural surface involved varied by patient, and
Figure 1. Histopathologic features of pneumothorax-associated fibroblastic lesion (PAFL). A, Wedge-shaped area of zonation demonstrated by
peripheral collagenous fibrosis and intervening normal pleura (brackets indicate 1 PAFL). B and C, Higher-power view illustrating the zonation and
fibroblastic foci (arrowheads) at the leading edge. D, Fibroblastic focus (hematoxylin-eosin, original magnifications