Knowledge, attitudes, and breast feeding practices of postnatal mothers: A cross sectional survey
Poreddi Vijayalakshmi, (1) Susheela T, (2) Mythili D (3)
RN, RM, BSN, MSN, Clinical instructor, College of Nursing, (1, 2, 3)
National Institute of Mental Health and Neuro Sciences, (Institute of National Importance), Bangalore.
Abstract
Background: Breast feeding has several benefits for both the infants and mothers. However, despite strong evidences in support of breast feeding its prevalence has remained low worldwide. The objective of the present study was to examine the knowledge and attitude towards breast feeding and infant feeding practices among Indian postnatal mothers.
Methodology: A cross sectional descriptive study was carried out among randomly selected postnatal mothers at Pediatric outpatient department at a tertiary care center. Data was collected through face-to-face interview using a structured questionnaire.
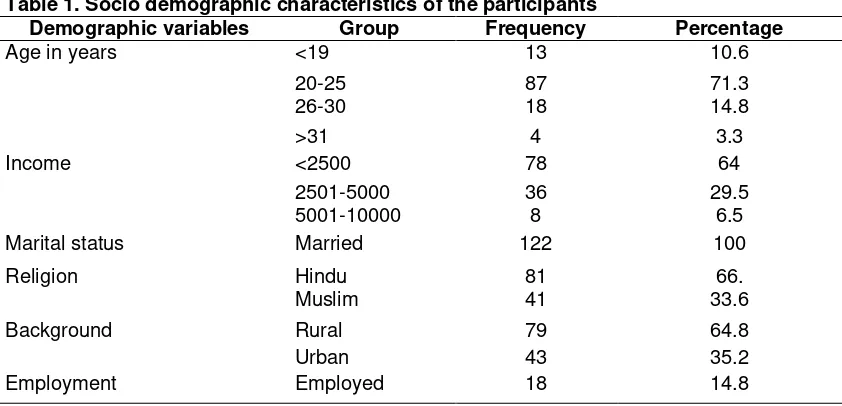
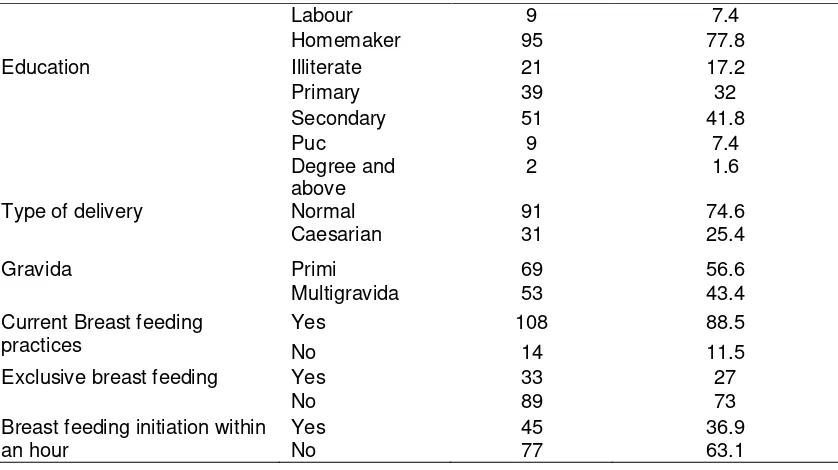
Results: Our findings revealed that a majority (88.5%) of the mothers were breast feeders. However, merely 27% of the mothers were exclusive breast feeders and only 36.9% initiated breast feeding within an hour. While mothers have good knowledge on breast feeding (12.05±1.74, M±SD), the average score of the Iowa Infant Feeding Scale (IIFAS) (58.77±4.74, M ±SD) indicate neutral attitudes toward breast feeding. Mothers those who were currently breast feeding (58.83 ± 4.74) had more positive attitudes than non- breastfeed mothers (45.21±5.22).
Conclusion: Our findings also show that the level of exclusive breast-feeding was low. Thus, it is important to provide prenatal education to mothers and fathers on breast-feeding. We also recommend strengthening the public health education campaigns to promote breast-feeding.
Keywords: Attitudes, Breast feeding, India, Infant feeding practices, Knowledge, Mothers
Corresponding author:
Poreddi Vijayalakshmi
Clinical Instructor, College of Nursing, Department of Nursing,
Introduction exclusively breastfed to achieve optimal growth, development, and health. Thereafter, infants should receive nutritionally adequate
and safe complementary foods, while
continuing to breastfeed for up to two years or
more. (2) Exclusive Breast Feeding (EBF) is
its prevalence has remained low worldwide (5-7)
and it is estimated that only about one-third of infants were exclusively breastfed for the first
six months of life. (3)
In India, breastfeeding appears to be influenced by social, cultural, and economic factors. In 1991, Breastfeeding Promotion Network of India (BPNI) was born to protect,
promote and support breastfeeding. (8)
Further, the Government of India has undertaken National Rural Health Mission,
which intends to implement Integrated
Management of Neonatal and Childhood
Illnesses (IMNCI) through the existing
healthcare delivery system. (9) Poor practices
and attitudes toward exclusive breastfeeding have been reported to be among the major reasons for poor health outcomes among children, particularly in developing countries. Nonetheless, the promotion and acceptance of practices, such as exclusive breastfeeding, are especially important in developing countries with high levels of poverty, and that are characterized by a high burden of disease and low access to clean water and adequate
sanitation. (10)
Breastfeeding has declined worldwide in recent years, as a result of urbanization and maternal employment outside the home. Studies in India have also shown a decline in breastfeeding trends, especially in urban
areas. (11) Early initiation of breastfeeding is
not seen in over 75% of the nation’s children and over 50% of children are not exclusively
breastfed. (12) Hence, the low figures for early
initiation of breastfeeding in India are a matter
of urgent concern. Although, the practice of breast feeding is influenced by various social, cultural and religious beliefs, maternal infant feeding attitude has been shown to be a
stronger independent predictor of
breastfeeding initiation. (13) In addition,
maternal positive attitudes toward
breastfeeding are associated with continuing to be breastfeeding longer and have a greater
chance of success. (14) On contrary, negative
attitudes of women toward breastfeeding is considered to be a major barrier to initiate and
continue to breastfeeding. (15) While, a number
of studies have assessed knowledge, attitude and practice of breastfeeding in different parts of the world; such studies are limited among
Indian mothers. (16-18) However, there were no
reported studies of breastfeeding knowledge and attitudes of mothers using the IIFAS (Iowa Infant Feeding Attitudes Scale) from India, which may be different from other cultures. Further, maternal attitude is also a concept of interest to health professionals who support breastfeeding. Thus the present study was developed to examine the infant feeding practices, knowledge and attitude towards breast feeding among Indian postnatal mothers’ using the IIFAS.
Materials and methods
This was a cross sectional study carried out among post natal mothers who attended immunization clinics and the Pediatric Out Patient Department with their children for vaccination and for the treatment of other minor illnesses at a tertiary care hospital in the month of January 2014.
and lack of time and we could not complete the interviews since mothers could not manage the infants (n=4).
Data collection Instruments
Demographic data survey instrument
The demographic form elicited information on participants’ background: age, marital
status, religion, place of residence,
employment, education, family’s monthly
income, type of delivery, number of deliveries, current breast feeding practices, exclusive breast feeding and initiation of breast feeding within an hour.
Questionnaires Data Collection
A structured questionnaire has been used to assess knowledge and attitudes towards breastfeeding among postnatal mothers.
This questionnaire has two sections;
Section A: This part of questionnaire was developed by the researchers based on the review of literature and past experiences. There were 15 items (3 negatively worded
items) to measure knowledge of the
participants towards breastfeeding. Each item in the knowledge section of the questionnaire had 3 possible responses, namely True, False, and not sure. One mark was awarded for every correct response, zero otherwise. Hence, the total number of marks in the knowledge section ranged from 0 to 15. This part of questionnaire was validated by twelve nursing and obstetrics experts.
Section B: The Iowa Infant Feeding Attitudes Scale (IIFAS) was used to assess mothers’
attitudes toward breastfeeding. (19) The scale
included 17 attitude items to determine level of agreement to each question. A 5-point Likert scale from strongly disagree to strongly agree was applied to all questions. Approximately half of the questions were negatively worded (i.e. 1, 2, 4, 6, 8, 10, 11, 14, and 17). Total IIFAS score ranged from 17 to 85 with higher scores reflecting more positive attitudes on breastfeeding. Total scores were grouped into three groups (1) positive to breastfeeding (70-85), (2) neutral (49-69), and positive to formula feeding (17-48). The Iowa Infant Feeding Attitudes Scale (IIFAS) is a valid and reliable
measure (Cronbach’s alpha scores ranges from (.85-.86) that evaluates breastfeeding knowledge and attitudes in cross-cultural
settings. (20-22)
Data collection procedure
After obtaining the permission from hospital authorities, all mothers were given an explanation of purpose of the study. Written informed consent was obtained from the mothers who were willing to participate in the study. Data were collected by the researchers through face-to-face interview, in a private room at the treatment facilities where the
participants were recruited. It took
approximately 25 minutes to complete the structured questionnaire. Though, it was not part of the study, researchers educated the mothers about the importance of continuing breast feeding up to 2 years.
Ethical consideration
Written consent was obtained from the participants and they were given freedom to quit the study. Participants’ confidentiality was respected.
Statistical analysis
Responses of the negatively worded items were reversed before data analysis. The data were analyzed using statistical software and results were presented in narratives and tables. The relationship between IIFAS scores and socio-demographic variables was tested by using correlation, t-tests, or a one-way analysis of variance. The significance level for all statistical analysis was set at 0.05.
Results
Sample description
exclusive breast feeders and 36.9% initiated breastfeeding within an hour of delivery (Table1).
Table 2 shows the mothers knowledge towards breastfeeding. The majority of the mothers agreed that colostrums is first breast milk (96.7%) and is important to maintain the immunity of the baby (99.2%). While, 85.2% felt that exclusive breast milk to be given during first 6 months, only 68% stated that breastfeeding should be continued up to 2 years. Similarly most of the mothers were aware of the importance of burping after each feed (91.8%), importance of taking healthy food (98.4%) and breast feeding helps in mother and child bonding (97.5%). All the mothers stated that mothers should sit comfortably during breastfeeding. However, 40.2% of the mothers opined that breast feed can affect the beauty of the feeding mothers and 56.6% stated that breastfeeding should be stopped when they start weaning the baby. Nonetheless, the average scores (12.05±1.74, M±SD) indicate that mothers have good knowledge about breastfeeding.
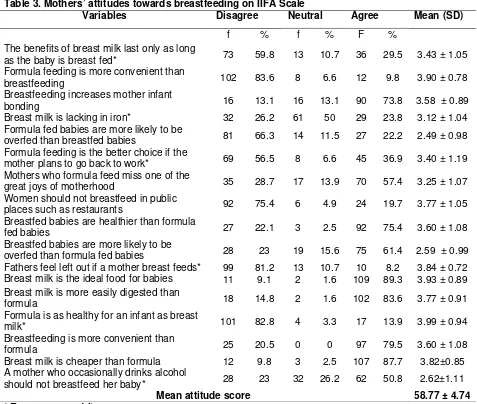
Concerning attitudes of the mothers towards breast-feeding, the majority of the participants agreed that breastfeeding is more convenient than formula feeding (83.6%) and increases mother infant bonding (73.8%). While 26.2% of the mothers disagreed, half (50%) of them were neutral to the statement “breast milk is lacking in iron”. However 36.9% of the participants opined that “formula feeding is the better choice if the mother plans to go
back to work”. Of the mothers, 57.4% agreed that formula feed miss one of the great joys of motherhood and fathers doesn’t feel left out if a mother breastfeeds (81.2%). Nearly three fourths of the participants agreed that the women can breastfeed in public places such as restaurants (75.4%). The majority stated that breast milk is ideal for the babies (89.3%), easily digested (83.6%) and healthy for an infant than formula (82.8%). More than half (50.8%) of the mothers felt that the mother who occasionally drinks alcohol should not breast- feed the baby. However, the average score of the IIFAS (58.77±4.74, M±SD) lay in the range of ‘neutral breastfeeding attitudes’. Most of the individual items had a mean score over 3 and only three items had a mean score less than 3, indicating that most of the mothers had neutral to positive attitude towards breastfeeding (Table 3).
Mothers from urban background
(60.23±4.11, p < .012) and monthly income above Rs 2500/- had higher IIFAS scores, indicating more favorable attitudes towards breastfeeding. There was also significant difference with regard to current breast feeding practices (p< .000). Mothers those who were currently breastfeeding (58.83 ± 4.74) had more positive attitudes than non- breastfeeding mothers (45.21±5.22) did. Although there were no significant differences found, older aged mothers (60.00±5.40) and homemakers (59.13 ± 4.72) had more positive attitudes towards breastfeeding than the other participants (Table 4).
Table 1. Socio demographic characteristics of the participants
Demographic variables Group Frequency Percentage
Age in years <19 13 10.6
20-25 87 71.3
26-30 18 14.8
>31 4 3.3
Income <2500 78 64
2501-5000 36 29.5
5001-10000 8 6.5
Marital status Married 122 100
Religion Hindu 81 66.
Muslim 41 33.6
Background Rural 79 64.8
Urban 43 35.2
Labour 9 7.4
Homemaker 95 77.8
Education Illiterate 21 17.2
Primary 39 32
Secondary 51 41.8
Puc 9 7.4
Degree and above
2 1.6
Type of delivery Normal 91 74.6
Caesarian 31 25.4
Gravida Primi 69 56.6
Multigravida 53 43.4
Current Breast feeding practices
Yes 108 88.5
No 14 11.5
Exclusive breast feeding Yes 33 27
No 89 73
Breast feeding initiation within an hour
Yes No
45 77
36.9 63.1
Table 2. Mothers’knowledge regarding breastfeeding
Variables True
False
Mean ± SD
f % F %
Colostrum is first breast milk 118 96.7 4 3.3 0.96 ± 0.17
Colostrum is important for the baby to maintain immunity 121 99.2 1 0.8 0.99 ± 0.09
Burping should be done after each feed 112 91.8 10 8.2 0.93 ± 0.30
Breast feeding should be continued Up to 2 years 83 68 39 32 0.68 ± 0.46
Exclusive breast milk can be given during first 6 months 104 85.2 18 14.8 0.85 ±0.35
Lactating mother should take healthy food to improve secretion of milk
120 98.4 2 1.6 0.98 ± 0.12
During breastfeeding the mother should sit comfortably 122 100 0 0 1.00 ± 0.00
During breastfeeding the mother should maintain eye to eye contact and talk with the baby
113 92.6 9 7.4 0.92 ± 0.26
Wash each breast with warm water before breast feeding 105 86.1 17 13.9 0.86 ±0.34
Awakening the baby while breastfeeding 74 60.7 48 39.3 0.60 ±0.49
Breast feeding helps in mother and child bonding 119 97.5 3 2.5 0.97 ±0.15
Breast feeding can prevent diseases affecting breast 116 95.1 6 4.9 0.95 ±0.21
Breastfeed affect the beauty of feeding mothers 49 40.2 73 59.8 0.40 ±0.49
Mother should not feed the child when she has diarrhea 44 36.1 78 63.9 0.36 ±0.48
Stop breastfeeding when you start weaning 69 56.6 53 43.4 0.56 ±0.49
Mean Knowledge score 12.05±1.74
Table 3. Mothers’attitudes towards breastfeeding on IIFA Scale
Variables Disagree Neutral Agree Mean (SD)
f % f % F %
The benefits of breast milk last only as long
as the baby is breast fed* 73 59.8 13 10.7 36 29.5 3.43 ± 1.05
Formula feeding is more convenient than
breastfeeding 102 83.6 8 6.6 12 9.8 3.90 ± 0.78
Breastfeeding increases mother infant
bonding 16 13.1 16 13.1 90 73.8 3.58 ± 0.89
Breast milk is lacking in iron* 32 26.2 61 50 29 23.8 3.12 ± 1.04
Formula fed babies are more likely to be
overfed than breastfed babies 81 66.3 14 11.5 27 22.2 2.49 ± 0.98
Formula feeding is the better choice if the
mother plans to go back to work* 69 56.5 8 6.6 45 36.9 3.40 ± 1.19
Mothers who formula feed miss one of the
great joys of motherhood 35 28.7 17 13.9 70 57.4 3.25 ± 1.07
Women should not breastfeed in public
places such as restaurants 92 75.4 6 4.9 24 19.7 3.77 ± 1.05
Breastfed babies are healthier than formula
fed babies 27 22.1 3 2.5 92 75.4 3.60 ± 1.08
Breastfed babies are more likely to be
overfed than formula fed babies 28 23 19 15.6 75 61.4 2.59 ± 0.99
Fathers feel left out if a mother breast feeds* 99 81.2 13 10.7 10 8.2 3.84 ± 0.72
Breast milk is the ideal food for babies 11 9.1 2 1.6 109 89.3 3.93 ± 0.89
Breast milk is more easily digested than
formula 18 14.8 2 1.6 102 83.6 3.77 ± 0.91
Formula is as healthy for an infant as breast
milk* 101 82.8 4 3.3 17 13.9 3.99 ± 0.94
Breastfeeding is more convenient than
formula 25 20.5 0 0 97 79.5 3.60 ± 1.08
Breast milk is cheaper than formula 12 9.8 3 2.5 107 87.7 3.82±0.85
A mother who occasionally drinks alcohol
should not breastfeed her baby* 28 23 32 26.2 62 50.8 2.62±1.11
Mean attitude score 58.77 ± 4.74
* Reverse scored items
Table 4. Differences in demographic factors and total attitude scores
Demographic variables Group (N=122) Mean (SD) P-value
Age in years <25 (n=100) 58.51(4.57) 0.184
>25 (n=22) 60.00(5.40)
Religion Hindu (n=81) 58.83(4.90) 0.839
Muslim (n=41) 58.65(4.48)
Background Rural (n=79) 57.98(4.90) 0.012*
Urban (n=43) 60.23(4.11)
Income <2500 (n=78) 57.91(4.45) 0.007*
>2500(n=44) 60.31(4.90)
Employment Employed (n=28) 57.57(4.70) 0.126
Education Illiterate (n=60) 59.50(4.94) 0.099
Literate (n=62) 58.08(4.47)
Type of delivery Normal (n=91) 58.40(4.54) 0.139
Caeserian (n=31) 59.87(5.22)
Exclusive breast feeding Yes (n=33)
No (n=89)
* Significance at p <0.05
Discussion
To our best knowledge, this was the first study that examined knowledge and attitudes
towards breastfeeding among postnatal
mothers using an internationally standardized tool (IIFAS) in India. Although, the present study demonstrated good knowledge among Indian mothers, they hold neutral attitudes
toward breastfeed indicating room for
improvement.
In the present study, majority (88.5%) of the mothers were breast feeding their infants. While, 85.2% of the mothers were aware of was substantially lower than previous studies
(25) but higher than a recent studies from India
(7.8% and 16.5%) (26, 27) New Guinea (17%),
(28) and Nigeria. (29) Further, studies indicate the
prevalence of exclusive breastfeeding at six months is generally low in low resource
countries and varies from 9% (30) to 40%. (16)
The majority of the mothers started supplementary feed at 4-6 months of age and the reasons given by them were; insufficient milk, to calm down the baby and believed that breast milk alone is insufficient for a growing
baby. Published reports indicate that
insufficient milk supply was the most common reason cited by the women for weaning. This finding was similar to those found in other
studies. (14,31) In a recent evaluation of the
Millennium Development Goals (MDGs),
exclusive breastfeeding (EBF) for six months was considered as one of the most effective
interventions to achieve Millennium
Development Goals (MDG-4). (30) However,
breastfeeding promotion interventions in
developing countries have been shown to result in a six fold increase in exclusive
breastfeeding rates at six months. (32)
According to Infant and Young Child Feeding (IYCF, 2006) guidelines, Government of India recommends that initiation of breastfeeding should begin immediately after
birth, preferably within one hour. (33) Though,
majority of the mothers delivered normally and in the hospital, only 36.9% of the mothers stated that they had initiated breastfeeding within an hour. Most common reasons for delay in initiation of breastfeeding as cited by the mothers were; delay in shifting the mothers from labor room, babies were in neonatal ICU, Caesarean section and family restriction. This is higher than the studies conducted from different parts of the world ranging from 6.3%
to 31%. (17, 25, 34, 35) On the contrary, few studies
demonstrated higher rate of breastfeeding
initiation 38% (36) 53% (37) and 72.2%. (25)
However, the data in various studies in India shows that initiation rates vary from 16 to
54.5%. (38) These findings indicate health
professionals to be made aware about the importance of initiating early breastfeeding is an urgent concern.
In the present study, 85.2% of the mothers were aware of EBF. This finding is consistent with previous results that lactating mothers
knowledge of EBF. (25, 39) Similarly, 68% mothers in the current study felt that they should continue breastfeeding till the age of 2 years. This finding is consistent with a recent study that found 75% mothers were aware that they should continue breastfeeding till the
age of 2 years. (35) Mothers who breastfed at 6
months had a higher average score (58.83 ± 4.74) on the IIFAS than their non-breastfeeding counterparts (45.21±5.22) and significant difference was observed (p< .000). Previous studies also have shown that mothers who do not breastfeed have negative attitudes towards
breastfeeding. (40) Most mothers had low
attitude scores towards “Breast milk is lacking in iron”, “Formula fed babies are more likely to be overfed than breastfed babies” and “A mother who occasionally drinks alcohol should not breastfeed her baby” and indicated future promotion program should improve these knowledge and attitudes. On the other hand, consonance with previous reports about breastfeeding, most of the mothers in this study agrees that breastfeeding promotes
mother-baby bonding. (41)
A number of studies also enlightened that there are psychological benefits for both mother and infant as the act of breastfeeding is a time of physical contact and closeness which
nurtures the bond between the two. (42, 43) In
line with previous research, mothers from urban background had higher score on IIFAS and indicate more positive attitudes toward
breastfeeding. (23) Maternal education has
been described as one of the strongest
determinants of the practice of EBF. (44)
Though, no difference was found between education and attitudes score, surprisingly, in our study illiterate mothers (59.50 ± 4.94) than literate mothers (58.08 ±4.47) hold better positive attitudes toward breast feeding. This finding is similar to results from Jordan where less educated women were more likely to breastfeed than women of higher education
level. (45) Studies indicate that mothers with
higher family income had better attitudes towards breastfeeding and similar finding was
observed in the study sample. (46, 47) Mothers
with income higher than 2500 Rs/-
(57.91±4.45) had better attitudes than mothers with low income (60.31± 4.90) and significant difference was found (p< .007).
Though, statistically significant difference was not found between attitude scores and
age, employment. Mothers older than 25 years and homemakers had more positive attitudes toward breast feeding. This finding is consistent with previous reports that showed high rates of awareness of EBF among older
groups (47) and homemakers. (41) These
findings can be attributed to homemakers who can focus on motherhood than working women. Studies have found a direct correlation between positive attitude to breastfeeding and
optimal EBF practice. (15, 48, 49) The mothers in
the present study had adequate knowledge and neutral attitudes toward breast feeding. These findings were supported by a recent study that found most mothers had neutral
knowledge and attitude on breastfeeding. (47)
Limitations
The present study has certain limitations such as cross sectional in nature, all the participants were at 6 months postpartum and small sample size that made difficult to generalize the findings. Future research should be focused on larger sample and qualitative studies such as focus group interviews to identify barriers to promote breast feeding among Indian mothers. Further, perceptions of health care providers towards breast feeding may provide greater understanding of the social and cultural beliefs in maternal and child health care practices postpartum. However, despite of these limitations, the present study findings may be helpful to the clinicians and
nursing professionals in designing the
interventions to promote breast feeding practices.
Conclusions
The present study concludes that the mothers have a very good knowledge and neutral attitudes toward breast feeding. Our findings also show that the level of exclusive breast feeding was low among Indian mothers. Thus, it is important to provide prenatal education to mothers and fathers on breast feeding. We also recommend strengthening the public health education campaigns to promote breast feeding.
Acknowledgement
References:
1. In fact Canada. Breastfeeding: a human
right. Human and legal rights of
breastfeeding women and children
1997(Cited 2014 July 25). Available from: https://www.infactcanada.ca/humright. 2. WHO. Exclusive breastfeeding for six
months best for babies everywhere’, World Health Organization 2011(Cited 2014 July 21). Available from: http://www.who.int. 3. WHO. The WHO Global Data Bank on
Infant and Young Child Feeding. WHO Nutrition for Health and Development, 2009 (Cited 2014 July 21) Available from: Grummer-Strawn LM. Breastfeeding rates in the United States by characteristics of the child, mother or family: the 2002 National Immunization Survey. Pediatrics, 2005; 115:31-7. trends in exclusive breastfeeding. Int Breastfeed J, 2012; 28:12.
8. Gupta A. BPNI: 10 years of its work. J Indian Med Assoc, 2002; 100:512-5. 9. NRHM. National Rural Health Mission
(2005-2012) Mission document, 2006.New Delhi: MOHFW, Government of India, New Delhi; Ministry of Health and Family Welfare (MoHFW).
10. Magawa R. Knowledge, attitudes and
practices regarding exclusive
breastfeeding in Southern Africa-Part 2. 2012 (Cited 2014 July 21). Available from : http://www.consultancyafrica.com
11. Rasania SK, Singh SK, Pathi S, Bhalla S, Sachdev TR. Breast-Feeding Practices In A Maternal And Child Health Centre In Delhi. Health Popul Perspect Issues. 2003; 26:110-5.
12. NFHS. National Family Health Survey-III 2005-06 (Cited 2014 July 21). Available from: http://www.nfhsindia.org
13. Scott JA, Shaker I, Reid M. Parental
attitudes toward breastfeeding: their
association with feeding outcome at hospital discharge. Birth, 2004; 31:125-31. 14. Chen CH, Chi CS. Maternal intention and
actual behavior in infant feeding at one month postpartum. Acta Paediatr Taiwan. 2003; 44:140-4.
15. Dungy CI, McInnes RJ, Tappin DM, Wallis AB, Oprescu F. Infant feeding attitudes and knowledge among socioeconomically disadvantaged women in Glasgow. Matern Child Health J, 2008; 12:313-22.
16. Madhu K, Sriram C, Ramesh M. Breast Feeding Practices and Newborn Care in Rural Areas: A Descriptive Cross-Sectional Study. Indian J Community Med, 2009; 34:243-6.
17. Dongre AR, Deshmukh PR, Rawool AP, Garg BS. Where and How Breastfeeding Promotion Initiatives Should Focus Its Attention? A Study from Rural Wardha. Indian J Community Med. 2010; 35:226-9. 18. Kishore MSS, Praveen K, Arun KA.
Breastfeeding Knowledge and Practices amongst Mothers in a Rural Population of North India: A Community-based Study. J Trop Pediatr, 2009; 55:183-8.
19. De la Mora A, Russell DW, Dungy CI, Losch M, Dusdieker L. The Iowa Infant Feeding Attitude Scale: analysis of reliability and validity. J Appl Psychol, 1999; 29:2362-80.
20. Al-Madani M, Vydelingum V, Lawrence J. Saudi mothers’ expected intentions and attitudes toward breast-feeding. Infant Child Adolesc Nutr, 2010; 2:187-98. 21. Sittlington J, Stewart-Knox B, Wright M,
Bradbury I, Scott JA. Infant-feeding attitudes of expectant mothers in Northern Ireland. Health Educ Res, 2007; 22:561-70.
22. Wallis AB, Brînzaniuc A, Chereches R, Oprescu F, Sirlincan E, David I. Reliability and validity of the Romanian version of a scale to measure infant feeding attitudes and knowledge. Acta Paediatr, 2008; 97:1194-9.
24. Simard I, O'Brien HT, Beaudoin A, Turcotte D, Damant D, Ferland S, et al. Factors influencing the initiation and duration of breastfeeding among low-income women followed by the Canada prenatal nutrition program in 4 regions of quebec. J Hum Lact, 2005; 21:327-37.
25. Oche MO, Umar AS, Ahmed H.
Knowledge and practice of exclusive breastfeeding in Kware, Nigeria. Afr Health Sci, 2011; 11:518-23.
26. Tiwari R, Mahajan PC, Lahariya C. The determinants of exclusive breastfeeding in urban slums: a community based study. J Trop Pediatr, 2009; 55:49-54.
27. Bandyopadhyay M. Impact of ritual pollution on lactation and breastfeeding practices in rural West Bengal, India. Int Breastfeed J, 2009 (Cited 2014 July
20)4:2. Available from:
http://wwwinternationalbreastfeedingjourna lcom/content/4/1/2.
28. Kuzma J. Knowledge, attitude and practice related to infant feeding among women in Survey. National Population Commission. Federal Republic of Nigeria 2008 (Cited sectional, health facility based survey. Int Breastfeed J, 2012; 10:1.
31. Otsuka K, Dennis CL, Tatsuoka H, Jimba M. The relationship between breastfeeding self-efficacy and perceived insufficient milk among Japanese mothers. J Obstet Gynecol Neonatal Nurs, 2008; 37:546-55. 32. Imdad A, Yakoob MY, Bhutta ZA. Effect of
breastfeeding promotion interventions on breastfeeding rates, with special focus on developing countries. BMC Public Health, 2011; 13:3.
33. IYCF. National guideline on Infant and Yong Child Feeding, 2nd edition. 2006
34. Oche MO, Umar AS. Breastfeeding Practices of Mothers in a Rural Community of Sokoto, Nigeria. Niger Postgrad Med J, 2008; 15:101-4.
35. Chaudhary RN, Shah T, Raja S.
Knowledge and practice of mothers regarding breast feeding: a hospital based study. Health Renaissance, 2011; 9:194-200.
36. Raval D, Jankar DV, Singh MP. A study of breast feeding practices among infants living in slums of Bhavnagar city, Gujarat, India Health line, 2011;2:78-83. 37. Chandrashekhar TS, Joshi HS, Binu V,
Shankar PR, Rana MS, Ramachandran U. Breastfeeding initiation and determinants of exclusive breastfeeding-a questionnaire survey in an urban population of western Nepal. Public Health Nutr, 2007; 10:192-7. 38. Agarwal S, Srivastava K, Sethi V. Maternal
and New-born Care Practices Among the Urban Poor in Indore, India: Gaps, Reasons and Possible Program Options. Urban Health Resource Center, New Delhi, 2007.
39. Ekanem IA, Ekanem AP, Asuquo A, Eyo VO. Attitude of working mothers to
exclusive breastfeeding in Calabar
municipality, cross river State, Nigeria. Journal of Food Research, 2012; 1:71-75. 40. Holbrook EK, Mary CW, Melvin BH, Janet
MW. Maternal sociodemographic
characteristics and the use of the Iowa Infant Attitude Feeding Scale to describe breastfeeding initiation and duration in a population of urban, Latina mothers: a prospective cohort study. Int Breastfeed J, 2013 (Cited 2014 July 20) 8:7. Available
Knowledge, attitude and techniques of breastfeeding among Nigerian mothers from a semi-urban community. BMC Research Notes, 2013;6:552
42. Hale R. Infant nutrition and the benefits of breastfeeding. Br J Midwifery, 2007; 15:368-71.
44. Dubois L, Girard M. Social determinants of initiation, duration and exclusivity of breastfeeding at the population level. The results of a longitudinal study of child development in Quebec (ELDEQ 1998-2002). Can J Public Health. 2003; 94:300-5.
45. Khassawneh M YK, Zouhair A, Ahmad A. Knowledge, attitude and practice of breastfeeding in the north of Jordan: a cross-sectional study 2006. Int Breastfeed J, (Cited 2014 June 17) 1:17. Available from:
http://wwwinternationalbreastfeedingjourna lcom/content/1/1/17.
46. Shi L ZJ, Wang Y, Guyer B. Breastfeeding in rural China: association between knowledge, attitudes, and practices. J Hum Lact, 2008; 24:377-85.
47. Weiqi C. Breastfeeding knowledge,
attitude, practice and related determinants among mothers in Guangzhou, China.
West cluster: University of Hong
Kong.2010.
48. Hurley KM, Black MM, Papas MA, Quigg AM. Variation in breastfeeding behaviours,
perceptions, and experiences by
race/ethnicity among a low-income
statewide sample of special supplemental nutrition program for women, infants and children (WIC) participants in the United States. Matern Child Nutr, 2008; 4:95-105. 49. Persad MD, Mensinger JL. Maternal
breastfeeding attitudes: association with
breastfeeding intent and